Embed Size (px)
Citation preview

Stephen L. G. Rothman, MD #{149}Neil Chaftez, MD #{149}Michael L. Rhodes, PhD#{149}Melvyn S. Schwartz, DDS, MscD
CT in the Preoperative Assessmentof the Mandible and Maxilla for
Endosseous Implant Surgery
Work in Progress’
171
Head and Neck Radiology
A new computer software programthat generates panoramic andoblique computed tomographyscans was used to examine 205 pa-
tients who were being consideredfor endosseous dental implants inthe mandibular or maxillary arches.This technique allowed recognition
of the course of the inferior alveolarnerve canal and measurement of thealveolar ridge, which facilitated thedesign and placement of an optimaldental prosthesis.
Index terms: Computed tomography (CT),
computer programs #{149}Computed tomography
(CT), preoperative #{149}Computed tomography
(CT), technology #{149}Jaws, CT, 24.1211
Radiology 1988; 168:171-175
I From MPDI, Inc. 2730 Pacific Coast High-way, Torrance, CA 90505 (S.L.G.R., NC.,
M.L.R.); Department of Radiology (NC.), Uni-versity of California at San Francisco; and Per-madent Center (M.S.S.), Torrance, Calif. From
the 1987 RSNA annual meeting. Received De-
cember 11, 1987; revision requested January 28,1988; revision received March 7; acceptedMarch 23. Address reprint requests to S.L.G.R.
C RSNA, 1988
T HIN section, high-resolution corn-puted tomography (CT) is a
well-established diagnostic tool forexamining patients with serious max-illofacia! pathologic conditions. Itsuse in the realm of routine oral sun-gcry has been much slower in dcvc!-oping. Recently, CT scanning hasbeen shown to be useful for the pre-operative modeling of custom sub-peniosteal implants (1-4) as well asfor the preoperative planning of en-dosseous dental implants (5,6). Themodern technique for the implanta-tion of titanium fixtures into the jawwas described by Branemark et almore than 20 years ago; they pub-lished a 10-year follow-up study onthe original series in 1977 (7). Theprocedure is more than 90% success-ful when in the hands of an expeni-enced surgeon. Mandibular implan-tation has been more successful thanmaxillary implantation because ofthe greater thickness of the alveolarbone of the mandible and the pneu-matization of the maxillary sinus.Optima! positioning of the titaniumfixtures requires a detailed know!-edge of the cross-sectional anatomyof the alveolar ridges of the edentu-bus region along the entire curva-tune of the bone. However, previoustechniques have failed to providetrue cross sections through the de-sired location in the jaw. Only cross-sectiona! scans perpendicular to thelong axis of the body can be obtainedwith ease. Direct, corona! CT scansrequire tilting both the patient’shead and the scanner to obtain near-ly cross-sectional images. Theseviews, although useful, are especiallydifficult to obtain from an older,edentulous patient. Furthermore, thescans are not truly cross sectionsalong the curvature of the bone.They are only approximations of thetrue cross sections and are slightly
distorted due to the curvature.Artifacts from metallic dental rcs-
torations compromise the visualiza-
tion of that portion of alveolar bonethat is included in the same coronalscan. An additional drawback to co-monal scanning is the inclusion ofboth the eye and the thyroid in theprimary radiation beam.
Direct CT examination of the man-dible in an oblique plane also mc-quires difficult placement of thebody of the mandible perpendicularto the gantry. To provide true cross-sectional scans of both the mandibleand maxilla from an easy-to-obtainaxial CT scan, we developed special-ized reformatting computer software.This new software is designed to as-sist the oral surgeon in optimizingplacement of the endosseous im-plants. It is the purpose of this studyto describe the technique and prclim-mary clinical results of CT scanningwith multiplanar reformations in thepreoperative examination of patientsbeing considered for implant surgeryin the mandibular or maxillary arch-es.
PATIENTS AND METHODS
Two hundred five consecutive patients
referred for mandibular on maxillary CT
for oral surgery between August 1986 and
August 1987 were included in this study.
There were 74 men and 131 women. 5ev-
en patients were examined before and af-
ten implantation of a titanium fixture.
Prior to surgery, all patients in this
study underwent CT scanning on a 9800
high-resolution scanner (General Electric,
Milwaukee). Overlapping 1 .5-mm axial
cross-sectional sections were obtained
through the maxilla or mandible at 1-mm
intervals. Correct angulation of the jaw
was determined with a digital radio-
graph. The CT data were reconstructed
with a bone algorithm (General Electric).
The axial cross-sectional data were refor-
matted into corona! and sagittal planes of
view in the first 97 patients. Oblique
planes of view were reformatted perpen-
dicular and parallel to a curved line de-
marcating the curvature of the alveolar
ridge. These oblique views represent true
cross-sectional scans of the curvature of

c.
a. b.
172 #{149}Radiology July 1988
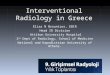
Figure 1. (a) Composite group of axial CT scans of the mandi-ble with appended millimeter scale. The curve through the
central image is drawn by the technologist to define the plane
of the panoramic and oblique neformations. (b) Cross-sectional
oblique refonmations computed from the scans in a. (c) Pan-
oramic CT reformations on the same patient derived from the
same data. Tick marks correspond to the position of the
oblique scans.
the bone. The CT scans were photo-graphed in alignment with a measuring
scale, which allowed precise measure-ments to be made from the radiographic
film. The remaining 108 patients in the
study had the data reformatted with a
modification of the computer program
that greatly simplified the procedure. On
an axial scan through the roots of the
teeth, the curvature of the alveolar ridgeis drawn on the computer screen. The
new program then produces sequential
oblique cross sections every 2 or 3 mmaround the entire curvature of the alveo-lar ridge. Each of these cross sections issequentially numbered and matched to
tick marks on the axial views. Finally,five panoramic CT tomognaphic sectionsare produced, and the oblique views arekeyed to the panoramic scans as well (Fig
1). It generally requires approximately 15
minutes to obtain the scan with the dy-
namic scanning mode. The computer pro-
cessing requires approximately 30-45
minutes depending on the number of
oblique scans that must be made. The lo-cation, axial inclination, and length of the
titanium implants were planned by the
surgeon with the aid of the cross-section-
a! scans.
DISCUSSION
In all, 114 maxillae and 117 mandi-
bles were studied with CT with scansproduced throughout the edentulousregions. The mandibles and maxilla of
26 patients were studied.
The preoperative analysis of themandible or maxilla for implant sur-gery requires special attention to ana-tomic detail unique to each bone.
Mandible
The two anatomic features of the
mandible that arc most important tothe surgeon are the contour of the a!ve-olar ridge and the location of the infc-
nor alveolar nerve.
The application of commonly usedimplant systems to the partially eden-
tulous patient underscores the impor-tance of the inferior alveolar nerve as avita! structure to be avoided during
surgery. Compression of the nerve bythe fixture may result in sensory dys-function of the lower lip and teeth. Al-
though the nerve can often be visual-
ized in two dimensions on standard in-traona! and panoramic scans, the two-
dimensional scan does not demonstratethe position of the nerve in a buccal-lingua! direction. The bucca!-!ingua!
position of the nerve can only be seenin either axial or cross-sectional views
of the mandibular ridges. With noknowledge of the buccal-lingual posi-tion of the nerve, the surgical result isoften compromised. Under these cm-cumstances, the surgeon must keep the
fixture length short of the nerve asseen in a two-dimensional lateral view
or on the panoramic view. This notonly results in the use of a short fixturebut precludes anchoring the apical endof the fixture in cortical bone. Both ofthese factors decrease the probability of
solid, permanent osseous integration.The inferior alveolar neurovascular
bundle can be seen in cross-sectional
scans of the body of the mandible. Themandibular canal may lie in the middleof the mandible (Fig 2), which pre-cludes successful implantation. Alter-natively, the canal may lie either alongthe bucca! or lingua! wall of the bodyof the bone. In these cases, it is possibleto implant the fixture adjacent to thenerve either on its medial or lateral
side (Fig 3). The nerve courses diago-na!!y from the lingua! region in theposterior area to the bucca! region inthe area of the mental foramen (Fig 4).It is therefore possible to straddle thenerve with one fixture medial and one
lateral. The walls of the mandibular ca-na! arc visible because of the adjacentbone. Most often there is a thin, densecortical bone rim around the nerve. Oc-
casionally, no bone can be distin-guished surrounding the nerve on thecross-sectional views.

2. 3.
Volume 168 Number 1 Radiology #{149}173
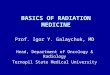
Figures 2, 3. (2) Three sequential cross-sectional oblique CT reformations demonstrating an edentulous portion of densely ossified mandi-
ble. The alveolar ridge is concave rather than convex due to a previous dental extraction. Note that the inferior alveolar neurovasculan chan-
nd lies centrally within the bone at this location (arrowhead). (3) Three sequential cross-sectional oblique CT nefonmations from a patient
who has had a titanium fixture (arrow) implanted into the mandible just lingual to the inferior alveolar nerve canal (arrowheads). The base
of the fixture is anchored into cortical bone.
Figure 4. Axial CT scan from a patient with
unilateral fibrous dysplasia. Note that the
inferior alveolar nerve canal crosses from
the lingual to buccal side of the bone (an-
rowheads). Because the nerve also slopes
from superior to inferior, its entire length
can never be seen on a single axial scan.
In many patients, the neurovascular
bundle loops downward, forward, and
medially before exiting from the men-
ta! foramen. The entire trunk of the
nerve may course anterior to the men-
tal foramen making a backward loop
(Fig 5). In most patients this loop is lessthan 3 mm but occasionally it may be
very long as in the specimen in Figure
5b. The extent of this anterior loopingcan be seen on the cross-sectional scansand the panoramic scans. This aspect is
exceedingly important to define prior
to surgery. Standard surgical doctrine
suggests not placing any fixtures with-
in 3 mm of the mental foramen. It is ob-
vious from Figure 5 that implants wellin front of this 3-mm limit stand a sig-
nificant chance of damaging a forward
projecting nerve.
The totally edentulous mandible usu-ally undergoes profound alveolar ridge
atrophy. In badly resorbed mandibles,
the nerve may lie on the crest of theridge (Fig 6), making endosseous im-
plant placement impossible with stan-
dard surgical techniques. These pa-ticnts have great difficulties maintain-ing regular dentures because of paindue to neural irritation. Occasionally,when endosseous implantation is im-
possible, the CT data may facilitate the
fabrication and positioning of satisfac-tory snug-fitting subpeniostea! appli-ances.
The mental fomamen usually exitsnearly halfway between the superior
and inferior borders of the mandible innonresorbed ridges but sometimes exitsclose to or on top of the ridge of re-sorbed mandible. While the fonamcnmay be seen in axial views, it is opti-mally visualized in oblique cross sec-
tions and panoramic views (Fig 7).
Routine radiographic studies in thoseresorbed mandibles in which bucca!
and lingual heights differ may actually
mislead the surgeon. Severely resorbed
mandibles frequently present adequate
bone height either buccal or lingual to
the nerve although the absolute height
may be dramatically reduced. The stan-
dard radiographic technique for plan-
ning fixture length in the edentulous
mandible utilizes a lateral skull radio-
graph, which demonstrates the greatest
height of bone present at any cross-sec-
tional level but fails to indicate the
shape or the contour of the ridge. It is
impossible (with previous techniques)
to delineate the contour of the ridge.
Figure 8 demonstrates a patient whosealveolar ridge appears to be of adequateheight. The oblique reformations dem-
onstnatc that because of the tapered,knife-like shape of the ridge, successful
implantation is not possible. Closely
spaced reformatted cross-sectionalscans perpendicular to the curvature of
the arch solve this problem by allow-
ing the surgeon to plan the position
and lengths of the mandibular im-
plants when surgery is deemed possi-
blc and to withhold surgery when it isnot (Fig 7).
Maxilla
Implantation into the maxilla pre-
sents a significant challenge to the sun-
geon who is charged with the responsi-bility of placing fixtures in the optimal
position. The surgeon is limited by his
ignorance of the precise size and con-
tour of the alveolar process of the max-
i!!a, as we!! as the location of both the
cortical bone and anatomic structures
that are to be avoided during surgery.
Preoperative planning with CT withmultiplanar reformation is preferable
to having to make strategic decisions
after the mucoperiosteal flaps have
been reflected to permit direct visual-ization of the osseous structures. Directintraoperative observation does not
provide the surgeon with the knowl-edge of the internal anatomic features
that CT does. The optima! placement of
the fixtures can usually be attained
when a dental surgeon and prosth-
odontist work together. As a rule, how-
ever, the prosthodontist is absent from
the operative suite. The use of CT with
multiplanar reconstruction provides an
opportunity for both members of the
team to confer in the best interests of
the patient.
Assessment of the shape and contour
of the alveolar ridges is best done with
oblique cross-sectional reformations. In
these scans, one can appreciate the en-
tire thickness as we!! as the shape and
height of the alveolar ridge and the lo-
cation and availability of cortical bone
(Fig 9).The difference between the anterior
inferior curving contour of the native
teeth that emanate from the alveolar
process and the noncurving fixtures
pose problems unique to maxillary im-plantation. The cheek and lip will be
displaced anteriorly by the distal aspect
of the fixture if it is implanted in the
same position as the normal teeth in
this region. Therefore, a different site

a. b.
174 #{149}Radiology July 1988
Figure 5. (a) Panoramic CT reformation scans demonstrate the entire length of the right inferior alveolar canal in a partially edentulous pa-
tient (arrowheads). Note that a portion of the nerve projects in front of the mental foramen (arrow). (b) Radiograph of a mandible specimen
with a flexible wire in the inferior alveolar canal. The mental foramen is outlined by a loop of wire. Note that the nerve projects well in
front of the mental foramen.
6. 7.
Figures 6, 7. (6) Three sequential oblique reformations from an edentulous patient with severe atrophy of the alveolar process. The mental
foramen points upward to the alveolar crest. Note that the nerve sits within the superior cortical bone (arrowhead). (7) Panoramic CT refor-
mation scans from an edentulous patient demonstrate the mental foramen lying superiorly on the alveolar crest (arrowheads).
8. 9.
Figures 8, 9. (8) Oblique reformations demonstrate a smooth but asymmetric contour of the alveolar ridge due to irregular atrophy. Because
the top half of the ridge is thin and pointed, it is impossible to implant a 3.5-mm fixture within the bone. Note also that there is no visible
cortical bone surrounding the inferior alveolar nerve canal and that it is nearly impossible to identify it with certainty. (9) Three oblique ref-ormations through the anterior portion of the maxilla. Note the downward projection of the residual tooth in a direction different from the
alveolar ridge. A fixture implanted into the long axis of the alveolar process would project forward toward the lip with unacceptable cosmet-
ic results (arrowhead).
and angulation for fixture implantation
must be sought to achieve both articu-
lation with the lower teeth and an ac-
ceptable cosmetic result. Furthermore,
in selecting a suitable site for implanta-
tion, the buccal fossae must be avoided.
The oblique CT scans provide an op-
portunity to fulfill these prerequisites
for an optima! dental prosthesis in the
alveolar process of the maxilla.
Another difficulty in placing im-
plants in the maxilla is the paucity of
cortical bone to provide firm anchorage
for the apical end of fixtures. Cross-sec-
tiona! scans assist the surgeon in locat-
ing cortical bone in the floor of the na-sal cavity and/or sinuses and in prede-termining the optimal fixture lengths

a. b.
Volume 168 Number I Radiology #{149}175
Figure 10. (a) Three oblique reformations through the posterior portion of the left maxilla demonstrate profound atrophy of the entire al-
veolar process. The sinus is well pneumatized, but only a thin cortical line of bone is present infeniorly. (b) Three oblique reformations
through the anterior portion of the maxilla. The alveolar process is profoundly narrowed in the buccolingual dimension. It is very thin and
pointed. This type of anatomy may preclude successful implantation.
a. b.
Figure 11. (a) Panoramic CT reformations demonstrate severe periodontal disease with the inflammatory process eroding the maxillary si-
nus (arrowheads). Note the swelling of the sinus mucosa (arrow). (b) Oblique reformations on the same patient. There is no normal bone
surrounding the root of the visualized tooth. This is due to inflammation and chronic infection. Between the root of the tooth and the floor
of the soft-tissue-filled sinus, there is destruction of bone (arrowhead). The presence of active infection will require vigorous therapy prior
to any surgery.
required to engage the cortical bone
(Fig 10). Anatomic features such as the
incisive canal can be visualized and
thus avoided during surgery. The avail-
ability of bone can be predetermined
with cross-sectional scanning as both
the height and width of the alveolar
processes can be measured preoper-
atively. It is very important to evaluate
the maxillary sinuses. Periodontal dis-
ease is an inflammatory, erosive pro-
cess that contains bacteria. Often the
inflammatory process destroys the al-
veolar bone between the root of the
tooth and the mucosa of the sinus. In-
fection of the sinus can occur. Since it
is best not to implant into an infected
sinus, one must establish this diagnosis
with certainty. On the cross-sectional
oblique and panoramic scans (Fig 11), it
is possible to define the extent of pen-
odontal erosion as well as the extension
of the inflammatory process into the si-
nus.
Not only can developmental defects,
foreign bodies, and osseous disease be
recognized preoperatively and thus
avoided at the time of surgery, but fix-tune placement also can be planned fordesign of the optimal prosthesis.
CONCLUSION
Although virtually all CT scanners
are capable of producing appropriate
reformations, the technique described
herei n provides cross-sectional refor-
mations parallel and perpendicular to a
curved line demarcating the curvatureof the mandibular and maxillary arch-es. These oblique scans represent true
cross-sectional views of the curving
bone. The technique described also a!-
lows direct measurement from the ra-
diographs regardless of film size or
magnification. Al! of the planes of the
reformatted scans are related to each
other by a series of tick marks, which
allow the observer to rapidly correlate
the different views. U
References
1. Rhodes ML, Kuo YM, Rothman SLG, Woz-
nick C. An application of computer graph-ics and networks to anatomic model andprosthesis manufacturing. IEEE Comput
Graphics Applications 1987; 7:12-25.
2. Truitt HP, James R, Boyne P. Non-inva-sive technique for mandibular subpenioste-al implants: preliminary report. J Prosthet
Dent 1986; 55:494-497.3. James R. Tissue response to dental im-
plant device. Clin Dent 1983; 4:1-21.4. Golec TS. CAD-CAM multiplanar imaging
for subpeniosteal implants. Dent ClinNorth Am 1986; 30:85-95.
5. Schwarz MS, Rothman SLG, Rhodes ML,Chafetz N. Computed tomography. I. Pre-operative assessment of the mandible for
endosseous implant surgery. mt J OralMaxillofac Implant 1987; 2:137-141.
6. Schwarz MS. Rothman SLG, Rhodes ML,Chafetz N. Computed tomography. II.Preoperative assessment of the maxilla for
endosseous implant surgery. mt J OralMaxillofac Implant 1987; 2:143-148.
7. Branemark Pt, Hansson BO, Adell R, et al.Osseointegrated implants in the treatment
of edentulous jaw: experience from a 10-year period. Scand J Plast Reconstr Sung(suppi 16) 1977.