-
8/3/2019 Health Economics- Lecture Ch14
1/54
Hospitals and Long Term Care
Dr. Katherine Sauer
Metropolitan State College of Denver
Health Economics
-
8/3/2019 Health Economics- Lecture Ch14
2/54
Chapter Outline:
I. Hospital BackgroundII. Hospital Utilization and Costs
III. Nursing Homes
IV. Hospice, Home Health, and Informal Care
-
8/3/2019 Health Economics- Lecture Ch14
3/54
In 2005, there were 5,756 hospitals with close to 1million beds
in the United States.
Of the 14.4 million persons employed at all health
service sites in 2006, 5.7 million were employed
athospitals.
At the same time, the aging of the population has created
a major challenge for the adequate provision of long-term
care.
-
8/3/2019 Health Economics- Lecture Ch14
4/54
-
8/3/2019 Health Economics- Lecture Ch14
5/54
I. Background on Hospitals
A. 4 criteria for categorizing hospitals:
1. length of stay
short stay (less than 30 days)
long stay (more than 30 days)
2. type
community
teaching
mental
respiratory diseases
other specialties (ex: maternity)
-
8/3/2019 Health Economics- Lecture Ch14
6/54
3. ownership
privatenon-profit
proprietary (for-profit)
publicfederal
state
county
local
4. size (number of beds)
[most short-stay facilities have
-
8/3/2019 Health Economics- Lecture Ch14
7/54
primary care: preventative and non-hospitalized curative
secondary care: common surgical and medical procedures
in hospitals
tertiary care: most complex procedures(ex: open heart surgery,
organ transplant)
Most community hospitals provide secondary care.
-
8/3/2019 Health Economics- Lecture Ch14
8/54
B. History
Hospitals date back to ancient Egypt and Greece
In many countries, hospitals were organized by religious
groups.- illness associated with lack of faith
In the US, early hospitals were for the poor , mental
patients, and infectious diseases.- medicine practiced at
home
-
8/3/2019 Health Economics- Lecture Ch14
9/54
The modern US hospital came about at the turn of the
20th century.
- advances in antisepsis (help fight off infections)
improved surgical success
- advances in anesthesia, anatomy, physiology,
and invention of the X-ray machine
- rapid urbanization
- rising wealth, private insurance, workers comp
- Johns Hopkins (Baltimore, MD) 1885
-
8/3/2019 Health Economics- Lecture Ch14
10/54
C. Organization
Nonprofit community hospitals are usually governed by
a board of trustees.- strong business background
Decision making power rests with the medical staff, not
the administrators or board.- the medical staff is made up of
physicians who
are not hospital employees
- direct hospital resources
- not held directly accountable for resources- bill
separately
- have admitting privileges at several
hospitals (attract patients)
-
8/3/2019 Health Economics- Lecture Ch14
11/54
Increasingly, hospitals are moving to permanent physician-
employees.
- use HMOs to attract patients
- advertise
Many smaller hospitals have closed, or merged,
orreorganized.
- deal with lower inpatient utilization
There is pressure to join networks of providers.
Many are focusing on outpatient care.
-
8/3/2019 Health Economics- Lecture Ch14
12/54
D. Regulation and Accreditation
Hospitals are subject to state and federal regulations.
- quality
- costs
- reimbursement
They are licensed at the state level.
They have their own quality assurance programs.- 1971 PSROs
(professional standards review orgs)
- 1984 PROs (peer review orgs)
- case-by-case reviews
-2002 QIOs (quality improvement orgs)
-
8/3/2019 Health Economics- Lecture Ch14
13/54
-
8/3/2019 Health Economics- Lecture Ch14
14/54
II. Hospital Utilization and Costs
Hospital costs account for about 1/3 of NHE.
- increasing at a rate of about 10% per year
-
8/3/2019 Health Economics- Lecture Ch14
15/54
A. Data
-
8/3/2019 Health Economics- Lecture Ch14
16/54
-
8/3/2019 Health Economics- Lecture Ch14
17/54
Competition and Costs:
Usually, competition results in lower costs.
Some argue that hospitals may be an exception.
- medical arms race (MAR)
-
8/3/2019 Health Economics- Lecture Ch14
18/54
game theory example:
Suppose there are two hospitals, each considering
adding a heart transplant unit.
Hospital B
Add unit Do not add unit
HospitalA
Add
unit
100
100
-50
200
Do
not
add
unit
200
-50
150
150
-
8/3/2019 Health Economics- Lecture Ch14
19/54
Why doesnt competition drive down prices?
- reimbursement mechanisms
- retrospective
In recent years, hospitals have become more competitive.
Hospitals as well as insurance companies must compete
for their managed care business through price and quality.
Hospitals also are now reimbursed by many major third-party
payers on a prospective basis at rates that are
independent of their actual costs.
-
8/3/2019 Health Economics- Lecture Ch14
20/54
B. Empirical Evidence
Kessler and McClellan (2000)
Examined the effects of hospital competition on the
costs and outcomes for Medicare beneficiaries who
incurred heart attacks.Prior to 1991, competition improved
outcomes
in some cases, but also raised costs.
After 1990, there were substantial decreases incosts and
substantial improvements in outcomes.
-
8/3/2019 Health Economics- Lecture Ch14
21/54
Zwanziger and Mooney (2005)
Studied HMOs in New York State which until 1996regulated the
rates (determined largely by historical costs)
private insurers were required to pay for inpatient care.
After the 1996 reforms, HMOs were able to negotiatelower prices
with hospitals that were located in more
competitive markets.
-
8/3/2019 Health Economics- Lecture Ch14
22/54
Dranove and colleagues (2002)
Found that for the average market, the consolidation
between 1981 and 1994 attributable to managed carerepresented
the equivalent of a decrease to 6.5 equal-
sized hospitals from 10.4 such hospitals.
Summary:
-
8/3/2019 Health Economics- Lecture Ch14
23/54
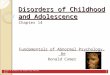
C. Hospital Cost Shifting
For legal and ethical reasons, hospitals often
provideuncompensated care.
- uninsured
- insured but dont pay their portion of bill
- restriction on reimbursement rates
- Medicare and Medicaid dont pay full bills
So, in reality are the costs shifted to the paying
customers?
-
8/3/2019 Health Economics- Lecture Ch14
24/54
Private Patients Medicare Patients
PP
QQ*priv
P*priv
MC = AVC MC = AVC
R1
DMR
Qmed
R2
R = reimbursement
-
8/3/2019 Health Economics- Lecture Ch14
25/54
In the short run, even if reimbursement falls, the hospital
wont raise prices for the private patients.
However, the hospitals profits are lower.- merge?
- close?
- pay less to employees?
-
8/3/2019 Health Economics- Lecture Ch14
26/54
Empirical Evidence?
Morrisey (1995)Indicates that cost shifting through higher
prices has
taken place but that it is far from complete.
One study included in his review shows that Californiahospitals
reduced the amount of uncompensated care by
53 cents for every $1 decrease in their discounts to third
parties.
This would have been unnecessary if the hospitals could
have shifted the costs to others.
-
8/3/2019 Health Economics- Lecture Ch14
27/54
Cleverly (1993)
Examined 160 community hospitals that closed between
1989 and 1991.
The analysis shows that high prices and lack of
investment in technology drive patients away.
With lower utilization, costs per patient increase and
cash flows become negative.
The deteriorating liquidity ultimately leads to closure.
-
8/3/2019 Health Economics- Lecture Ch14
28/54
Succi and colleagues (1997)
Found that rural hospitals gain an advantage and reduce
the threat of competition by differentiating their services.
Those that offer more basic services and high-tech
services compared to the market average are less likely to
close.
-
8/3/2019 Health Economics- Lecture Ch14
29/54
Jantzen and Loubeau (2000)
Found that price and hospital participation in networksare very
important to managed care organizations in
awarding contracts.
Second, hospitals and hospital systems, through their sizeand
partnerships, seek to counter the pricing pressure and
other demands that have been placed on them by
managed care organizations.
-
8/3/2019 Health Economics- Lecture Ch14
30/54
Sprang et al. (2001)
There is some evidence that restructuring lowers costs.
Krishnan (2001)Evidence indicating that merged hospitals charge
higher
fees than otherwise, especially when the merging
hospitals gain substantial market shares.
-
8/3/2019 Health Economics- Lecture Ch14
31/54
Harrison (2007)
Using comprehensive national data covering the period
19811998 found that increased market power, rather
than improved efficiency, is the principal driving force
for consolidations.
Melnick and Keeler (2007)
Found that hospitals that were members of multihospital
systems increased their prices between 1999 and 2003 at
much higher rates than nonmembers.
Summary:
-
8/3/2019 Health Economics- Lecture Ch14
32/54
D. Quality of Care
The public cares about quality!
Hospital quality is often understood in two ways.
The availability of high tech units and services is one
way to think about quality.
Quality can also be understood in terms of hospital
mortality and error rates, readmission rates, and the
rates at which a hospital meets established treatment
processes and protocols.
-
8/3/2019 Health Economics- Lecture Ch14
33/54
Areas of Health Econ research:
1. relationship between size and quality
2. quality and cost (do you get what you pay for?)
3. type of ownership and quality
4. quality and Medicaid patients
-
8/3/2019 Health Economics- Lecture Ch14
34/54
Empirical Evidence:
Williams et al., 2005Analysis of quarterly data for heart
attacks, congestive
heart failure, and pneumonia
substantial gains in 15 of the 18 measures over the two-year
study period.
The gains were greatest for hospitals that had been the
worst performers at the start of the evaluation period.
-
8/3/2019 Health Economics- Lecture Ch14
35/54
Jha et al., 2005
examined 10 quality indicators and found mean
performance scores (representing proportions of patients
who satisfied the criteria) were89 percent for heart attacks
81 percent for congestive heart failure
71 percent for pneumonia
Summary:
-
8/3/2019 Health Economics- Lecture Ch14
36/54
III. Nursing Homes
A. Background and Costs
The increase in the elderly populations has increased
interest in long-term care problems.
Traditionally, the elderly have been cared for until
death by families.
The first nursing homes in the US were the county
poorhouses established for those without families
(18th/19th century)
-
8/3/2019 Health Economics- Lecture Ch14
37/54
Other state and local facilities evolved.
- some were sponsored by religious and fraternal
groups
Social Security Act of 1935 provided funds for patients in
private nursing homes.
Medicare and Medicaid we passed in 1965 and increasedboth the
funding and the nursing industry.
-
8/3/2019 Health Economics- Lecture Ch14
38/54
The growing nursing home population and the growing cost
of nursing homes is linked with Medicare and Medicaid.
Medicare covers those who are discharged from hospitals,
but require skilled nursing care to recover.
- historically Medicare reimbursed on a cost basis- Balanced
Budget Act of 1997 mandated a shift to
prospective reimbursement [fixed per diem
payments determined by the category a person is
in]- shift the financial risk to the nursing home
-
8/3/2019 Health Economics- Lecture Ch14
39/54
Medicaid pays for the long-term care of the poor (elderlyand
non-elderly).
- covers skilled nursing care
- covers intermediate care
Medicare is administered by the state, but subject to
federal requirements.
- state eligibility requirements can vary
- state payment methods can vary
-
8/3/2019 Health Economics- Lecture Ch14
40/54
B. Quality of Care
One would expect a positive association between size and
quality as a result of economies of scale and scope.
Daviss (1991)
Review of a large number of studies, suggests that no
clear relationship exists.
-
8/3/2019 Health Economics- Lecture Ch14
41/54
C. Relationship Between Type of Ownership and Quality
Analysts have not been able to detect an unambiguous
positive relationship between quality and costs.
- so, expect that they would have difficulty in
detecting any relationship between type of
ownership and process or outcome measures of
quality.
Daviss review confirms this conclusion.
-
8/3/2019 Health Economics- Lecture Ch14
42/54
D. Medicaid Patients and Quality of Care
Expenditures per resident are lower in homes with
higher proportions of Medicaid patients.
- negative relationship between quality and the
proportion of Medicaid residents in a nursing
home
Troyer (2004)
found that Medicaid resident mortality rates were 4.2
percent and 7.8 percent higher than those for private-
pay residents after one and two years, respectively.
-
8/3/2019 Health Economics- Lecture Ch14
43/54
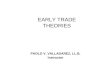
E. Excess Demand
For years the industry has been characterized as having
excess demand.
Economists are intrigued/skeptical of persistent shortages
of any commodity.
-
8/3/2019 Health Economics- Lecture Ch14
44/54
A nursing home admits private (self-paying or
insurance) patients and Medicaid patients.
P
P1
R1
MC = AVC
DMR
Q1 Qcapicity Q
Admit private patientswhere MR exceeds R.
(Q1)
They will pay p1.
Suppose there are Qm
Medicare patients
wanting admission.
A number of them
wont get in.
Qm
-
8/3/2019 Health Economics- Lecture Ch14
45/54
Medicare raises the reimbursement rate:
P
P2
P1
R2
R1
MC = AVC
DMR
Q2Q1 Qcapicity Q
Find where R2 > MR .
Admit Q2 privatepatients.
They will pay p2.
There are still Qm
Medicare patients
wanting admission.
A smaller number of
them wont get in.
Qm
-
8/3/2019 Health Economics- Lecture Ch14
46/54
F. Financing Long-Term Care
Patients must meet income and asset requirements to beeligible
for Medicaid nursing home benefits.
- spend a lifetime paying into taxes and then
must spend down to qualify for Medicaid
There are a variety of proposals to allow individuals to
have higher incomes and still be eligible for care.
Federal policy centers on two strategies:- encourage home
care
- encourage private LTC coverage
-
8/3/2019 Health Economics- Lecture Ch14
47/54
IV. Hospice, Home Health, and Informal Care
The budgetary pressure of caring for the growing
elderlypopulation in hospitals and nursing homes has promoted
interest in other less costly arrangements.
Hospice and home health programs are perceived to becost
effective and are heavily funded at the federal level.
Hospice care:
- for the terminally ill- care in their own homes
- improved quality of life in final days
- death with dignity
-
8/3/2019 Health Economics- Lecture Ch14
48/54
Most hospice patients receive care in their own homes,
but the use of special facilities is becoming more
prevalent.
In hospice, an interdisciplinary team of health
professionals provides individualized care.
- emphasizes patients physical and emotional
comfort (i.e., palliative as opposed to curative
care)
- support for family members
Medicare introduced hospice benefits in 1983.
-
8/3/2019 Health Economics- Lecture Ch14
49/54
Home health care (larger and more important program)
provides care to patients with acute and long-term needs.
disabilities
recuperating from a hospital stay
the terminally ill
The rationale for public funding for home health care rests
on the premise that it is much less expensive than either
hospital or nursing home care.
-
8/3/2019 Health Economics- Lecture Ch14
50/54
Benefit was included in initial Medicare legislation in1965.
- 1973 extended to certain disabled people under 65
HHC is one of the fastest growing components of
totalspending.
BBA legislation in 1997 moved reimbursement from cost-
based to prospective.
-
8/3/2019 Health Economics- Lecture Ch14
51/54
Concluding Thoughts:
Common perceptions of complete cost shifting do not
accurately represent how hospital markets function.
There are significant deficiencies in the quality of
hospital care, and improving quality is one of this
nations most important goals.
-
8/3/2019 Health Economics- Lecture Ch14
52/54
In the long-term care sector, we focused on nursinghomes,
emphasizing three issues:
quality, especially for Medicaid patients
shortages
financing nursing home care
Home health care is a less costly alternative to nursing
home care and represents one of the fastest-growing
components of health care spending.
-
8/3/2019 Health Economics- Lecture Ch14
53/54
Discussion Questions:
1. Explain why it is often claimed that hospitals competefor
doctors rather than patients.What are some of the
implications of this phenomenon, assuming that it is
true?
2. Explain why only about 5% of adults buy long-term
care coverage.
3. Explain how excess demand for nursing home bedsmay persist
over long periods. How can the hypothesis
be tested?
-
8/3/2019 Health Economics- Lecture Ch14
54/54
4. Informal care provided by children and other familymembers
are good substitutes for Long Term Care for
parents. Describe some potential social and
demographic changes that may reduce the availability of
such informal care. Develop policies that may help takeadvantage
of the substitutability to delay entry of the
elderly into Long Term Facilities.