Embed Size (px)
Citation preview
Health Information Exchange Ad Hoc WorkgroupKickoff Meeting
March 30, 2010
2
Agenda
Introductions
Health Information Technology Plan Summary
Health Information Exchange (HIE) Ad Hoc Workgroup Charge and
Approach
Selection of Co-Chairs
HIE Overview – Health IT Plan
Review of Health Information Exchange Planning Requirements
Next Steps
Appendix: HIE Section of Review of Health IT Plan - Deloitte
November 2009
3
Health Information Technology Plan Summary
4
Massachusetts e-Health Institute Establishedwith Vision of EHR and HIE Adoption by 2015
Massachusetts e-Health Institute (MeHI) established within the Massachusetts Technology Collaborative through Chapter 305 of the Acts of 2008– Mission to promote implementation of Electronic Health Records in all
provider settings as part of an interoperable Health Information Exchange
State appropriated $15M for 2009: annual funding subject to appropriation through 2014
Development of six-year Plan for statewide deployment of electronic health records and health information exchange
Use of Implementing Organizations to assist in the execution of the plan through community engagement, technology selection, project management, training etc.
Health IT efforts in Commonwealth support healthcare reform
Leveraging state-wide efforts including Massachusetts e-Health Collaborative, Massachusetts Health Data Consortium, NEHEN, Masspro, Eastern MA H/C Initiative, CHAPS, SafeHealth, etc.
5
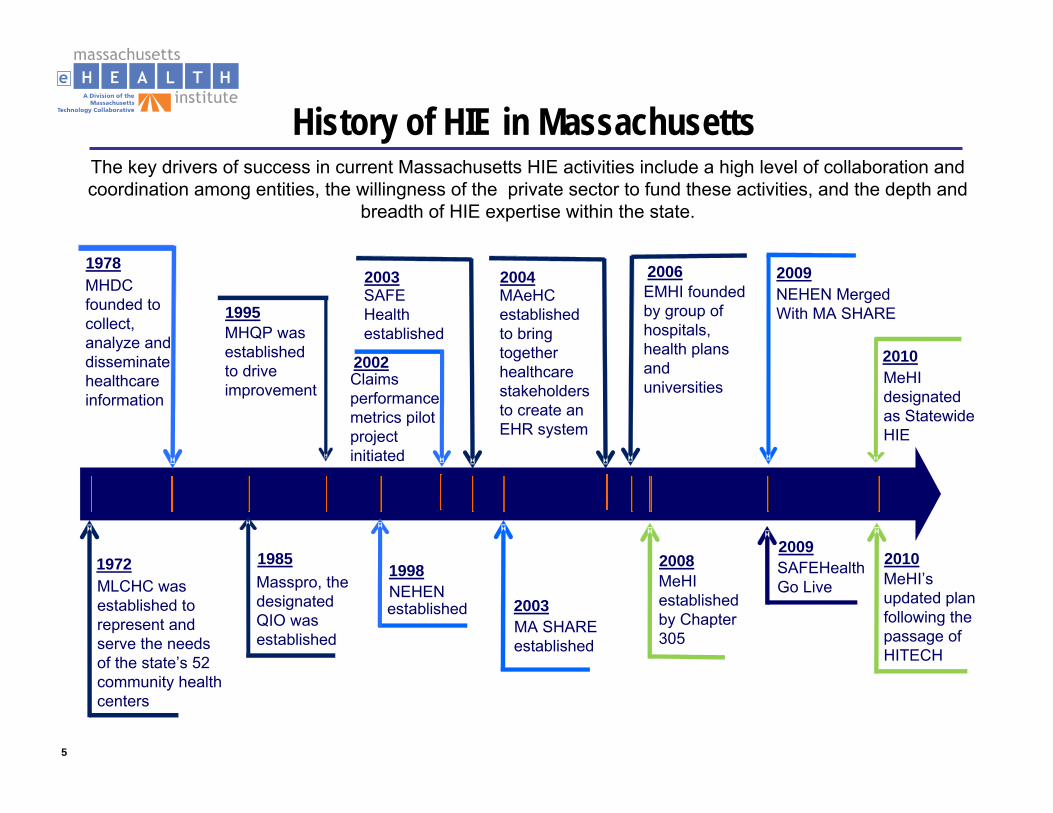
The key drivers of success in current Massachusetts HIE activities include a high level of collaboration and coordination among entities, the willingness of the private sector to fund these activities, and the depth and
breadth of HIE expertise within the state.
History of HIE in Massachusetts
1978MHDC founded to collect, analyze and disseminate healthcare information
2003MA SHARE established
1995MHQP was established to drive improvement
1972MLCHC was established to represent and serve the needs of the state’s 52 community health centers
1985Masspro, the designated QIO was established
2004MAeHC established to bring together healthcare stakeholders to create an EHR system
2006EMHI founded by group of hospitals, health plans and universities
2008MeHI established by Chapter 305
2010MeHI’s updated plan following the passage of HITECH
1998NEHENestablished
2009NEHEN Merged With MA SHARE
2010MeHI designated as Statewide HIE
SAFEHealth Go Live
2009
2003SAFE Health established
2002Claims performance metrics pilot project initiated
6
ARRA/HITECH OpportunitiesHITECH Statewide HIE with collaborative governance and sustainable funding model: funded for $10.6M for Massachusetts (MEHI)HITECH Regional Extension Center to support implementation of electronic health record systems in physician offices: funded for $13.4M for Massachusetts (MeHI) for two years with additional $1MAdditional opportunities for Massachusetts include:– ARRA: HIT Community College/Education Grant with 13 Mid-
Atlantic States: $10-$15M– ARRA: Beacon Community Cooperative Agreement grant: $10-
20M– ARRA: Strategic Health IT Advanced Research Project (SHARP):
$18M

7
HITECH – Total Provider Adoption ValueAssumes all eligible entities receive maximum incentives
Medicare IncentivesMedicaid Incentives
Hospitals: $ 412 M
Physicians: $ 755 M CHCs: $ 29.46 M
Total Incentives for Meaningful Use: $1.20 Billion (2-3 years)
8
MA Health IT Plan Overview: Goals1. Improve access to comprehensive, coordinated, person-focused health
care through widespread provider adoption and meaningful use of certified EHRs
2. Demonstrably improve the quality and safety of health care across all providers through Health IT that enables better coordinated care, provides useful evidence-based decision support applications, and can report data elements to support quality measurement.
3. Slow the growth of health care spending through efficiencies realized from the use of Health IT.
4. Improve the health of the Commonwealth’s population through public health programs, research, and quality improvement efforts, enabled through an efficient, reliable and secure health information exchange processes.
9
MA Health IT Plan Overview: Strategies
Strategy 1: Establish Multi-Stakeholder Governance.
Strategy 2: Establish a Privacy Framework to Guide the Development of a Secure Health IT Environment.
Strategy 3: Implement Interoperable Health Records in all Clinical Settings and Assure They Are Used to Optimize Care.
Strategy 4: Develop and Implement a Statewide Health InformationExchange (HIE) Infrastructure to Support Care Coordination, Patient Engagement and Population Health.
Strategy 5: Create a Local Workforce to Support Health IT Related Initiatives.
Strategy 6: Monitor Success.
10
Health Information Exchange (HIE) Ad Hoc Workgroup Charge and Approach
11
Governance
While developing a governance approach to ensure public-private collaboration, MeHI must consider the following:
Support the ability to utilize existing public and private sector technologies where appropriate Leverage the wealth of knowledge residing in both sectors Ensure that appropriate conflict of interest controls are in place to protect both public and private stakeholders participating in the collaborative approach Promote transparency in the efficient utilization of funds to support prioritized programsPromote teaming of resources across both the private and public sectors where appropriateEnsure sustainability
12
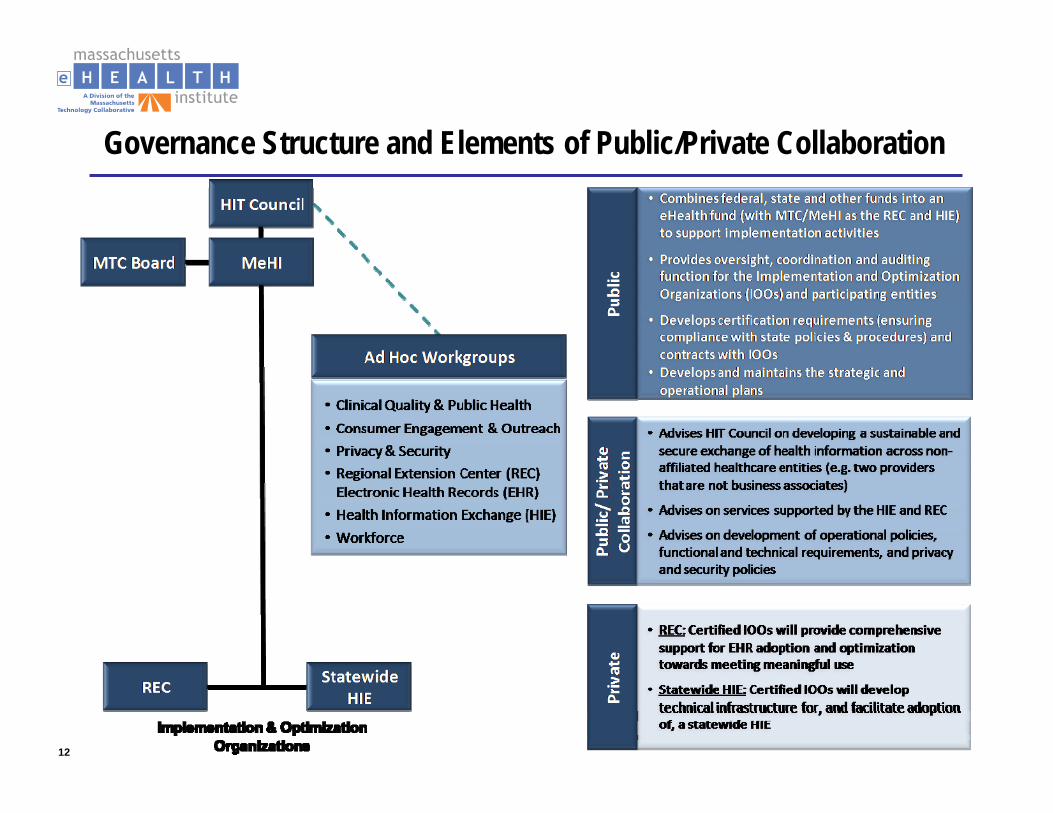
Governance Structure and Elements of Public/Private Collaboration
13
HIE Ad Hoc Workgroup Charge and ApproachPrimary Focus– In the context of development of the HIE Operational Plan, advise
on how to develop and maintain functional and technical requirements for the Health Information Exchange (intra and inter-state).
Purpose– The purpose of the HIE Workgroup is to provide guidance, advice
and recommendations to the Health IT Council on matters related to the development and sustainability of an HIE.
– This Workgroup will be comprised of subject matter experts and advisors across different workgroup domains.
– It is intended that this Workgroup will provide outside viewpoints and recommendations to the Health IT Council on functional and technical requirements for the HIE.
14
Additional ResponsibilitiesReceive and respond to periodic Project Management Office (PMO) reports.Provide recommendations on a common privacy and security framework or certification program.Advise on maintaining the IOOs approach to implementing nationally recognized interoperability and terminology requirements and standards.Advise on the technical architecture, including the architecture for the proposed National Health Information Network (NHIN).Advise on options for long-term sustainability.
15
Additional Responsibilities (cont’d)Provide recommendations on how to address long-term financial sustainability of HIE and REC services.Interpret national and Commonwealth legislation, as it relates to operation of the HIE, and provide recommendationsAdvise on activities of the Implementation and Optimization Organization (IOO) related to the secondary use of data flowing through the HIE.Make recommendations on the types and sequence of capabilities to support adoption of the HIE by all stakeholders, including providers and patients.
16
Selection of Co-Chairs
17
HIE Overview – Health IT Plan
18
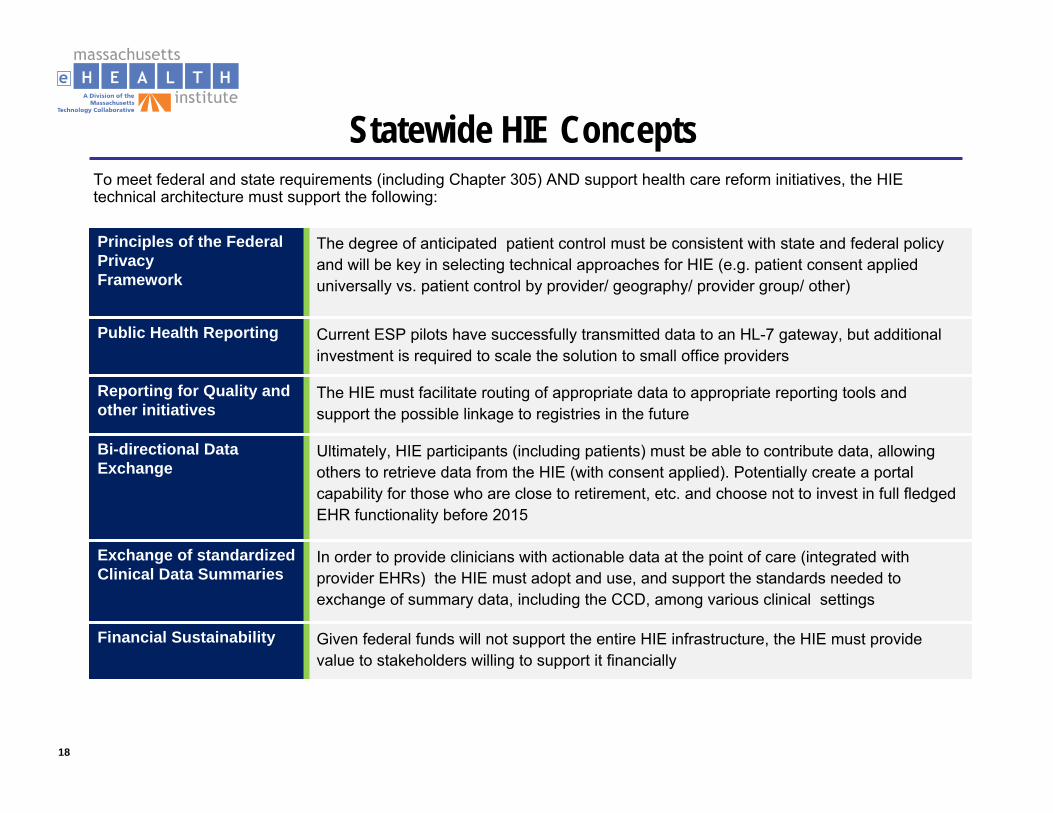
Principles of the Federal Privacy Framework
The degree of anticipated patient control must be consistent with state and federal policy and will be key in selecting technical approaches for HIE (e.g. patient consent applied universally vs. patient control by provider/ geography/ provider group/ other)
Public Health Reporting Current ESP pilots have successfully transmitted data to an HL-7 gateway, but additional investment is required to scale the solution to small office providers
Reporting for Quality and other initiatives
The HIE must facilitate routing of appropriate data to appropriate reporting tools and support the possible linkage to registries in the future
Bi-directional Data Exchange
Ultimately, HIE participants (including patients) must be able to contribute data, allowing others to retrieve data from the HIE (with consent applied). Potentially create a portal capability for those who are close to retirement, etc. and choose not to invest in full fledged EHR functionality before 2015
Exchange of standardized Clinical Data Summaries
In order to provide clinicians with actionable data at the point of care (integrated with provider EHRs) the HIE must adopt and use, and support the standards needed to exchange of summary data, including the CCD, among various clinical settings
Financial Sustainability Given federal funds will not support the entire HIE infrastructure, the HIE must provide value to stakeholders willing to support it financially
Statewide HIE ConceptsTo meet federal and state requirements (including Chapter 305) AND support health care reform initiatives, the HIE technical architecture must support the following:
19
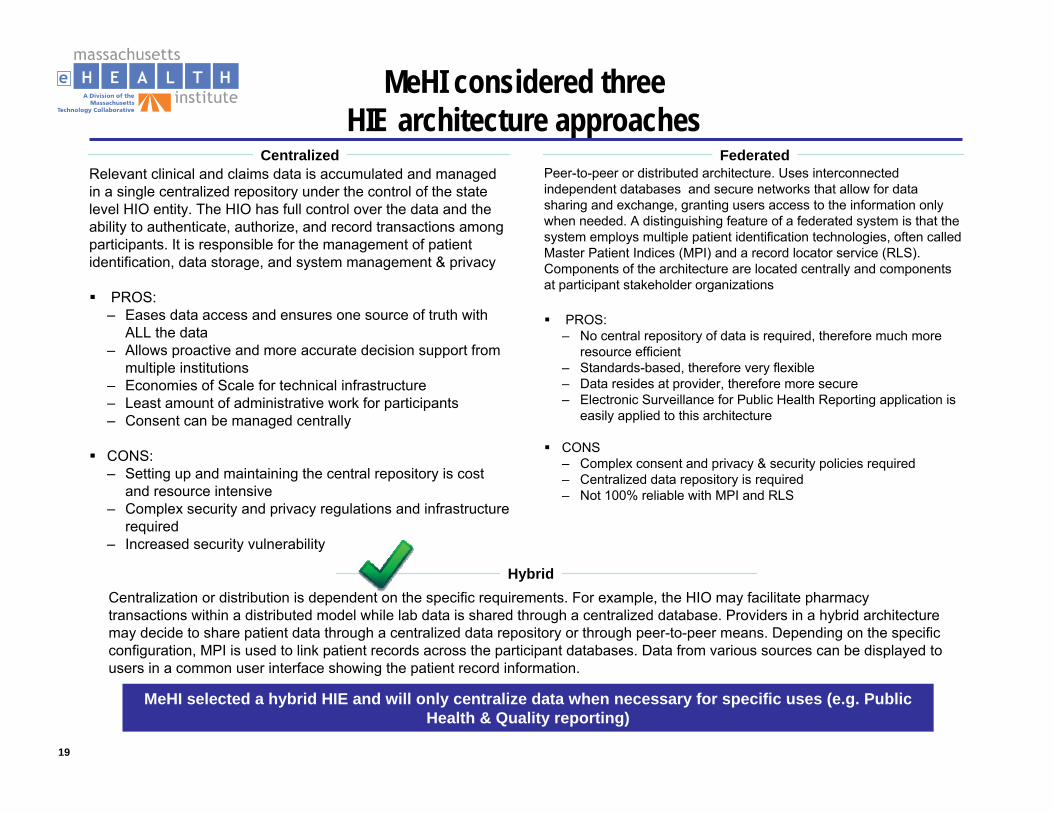
MeHI considered three HIE architecture approaches
Centralized FederatedRelevant clinical and claims data is accumulated and managed in a single centralized repository under the control of the state level HIO entity. The HIO has full control over the data and theability to authenticate, authorize, and record transactions among participants. It is responsible for the management of patient identification, data storage, and system management & privacy
PROS:– Eases data access and ensures one source of truth with
ALL the data– Allows proactive and more accurate decision support from
multiple institutions– Economies of Scale for technical infrastructure– Least amount of administrative work for participants– Consent can be managed centrally
CONS:– Setting up and maintaining the central repository is cost
and resource intensive– Complex security and privacy regulations and infrastructure
required– Increased security vulnerability
Peer-to-peer or distributed architecture. Uses interconnected independent databases and secure networks that allow for data sharing and exchange, granting users access to the information only when needed. A distinguishing feature of a federated system is that the system employs multiple patient identification technologies, often called Master Patient Indices (MPI) and a record locator service (RLS).Components of the architecture are located centrally and components at participant stakeholder organizations
PROS:– No central repository of data is required, therefore much more
resource efficient– Standards-based, therefore very flexible– Data resides at provider, therefore more secure– Electronic Surveillance for Public Health Reporting application is
easily applied to this architecture
CONS– Complex consent and privacy & security policies required– Centralized data repository is required– Not 100% reliable with MPI and RLS
HybridCentralization or distribution is dependent on the specific requirements. For example, the HIO may facilitate pharmacy transactions within a distributed model while lab data is shared through a centralized database. Providers in a hybrid architecture may decide to share patient data through a centralized data repository or through peer-to-peer means. Depending on the specific configuration, MPI is used to link patient records across the participant databases. Data from various sources can be displayed to users in a common user interface showing the patient record information.
MeHI selected a hybrid HIE and will only centralize data when necessary for specific uses (e.g. Public Health & Quality reporting)
20
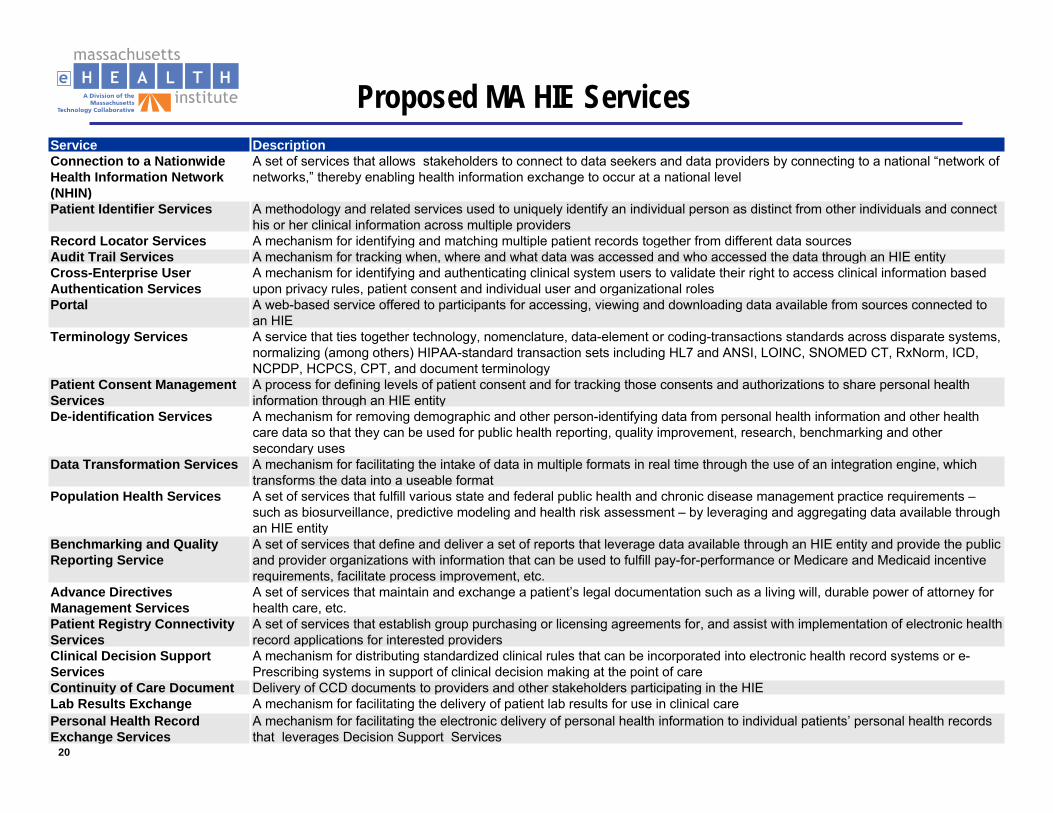
Proposed MA HIE ServicesService DescriptionConnection to a Nationwide Health Information Network (NHIN)
A set of services that allows stakeholders to connect to data seekers and data providers by connecting to a national “network of networks,” thereby enabling health information exchange to occur at a national level
Patient Identifier Services A methodology and related services used to uniquely identify an individual person as distinct from other individuals and connecthis or her clinical information across multiple providers
Record Locator Services A mechanism for identifying and matching multiple patient records together from different data sourcesAudit Trail Services A mechanism for tracking when, where and what data was accessed and who accessed the data through an HIE entityCross-Enterprise User Authentication Services
A mechanism for identifying and authenticating clinical system users to validate their right to access clinical information based upon privacy rules, patient consent and individual user and organizational roles
Portal A web-based service offered to participants for accessing, viewing and downloading data available from sources connected to an HIE
Terminology Services A service that ties together technology, nomenclature, data-element or coding-transactions standards across disparate systems, normalizing (among others) HIPAA-standard transaction sets including HL7 and ANSI, LOINC, SNOMED CT, RxNorm, ICD, NCPDP, HCPCS, CPT, and document terminology
Patient Consent Management Services
A process for defining levels of patient consent and for tracking those consents and authorizations to share personal health information through an HIE entity
De-identification Services A mechanism for removing demographic and other person-identifying data from personal health information and other health care data so that they can be used for public health reporting, quality improvement, research, benchmarking and other secondary uses
Data Transformation Services A mechanism for facilitating the intake of data in multiple formats in real time through the use of an integration engine, whichtransforms the data into a useable format
Population Health Services A set of services that fulfill various state and federal public health and chronic disease management practice requirements –such as biosurveillance, predictive modeling and health risk assessment – by leveraging and aggregating data available through an HIE entity
Benchmarking and Quality Reporting Service
A set of services that define and deliver a set of reports that leverage data available through an HIE entity and provide the public and provider organizations with information that can be used to fulfill pay-for-performance or Medicare and Medicaid incentive requirements, facilitate process improvement, etc.
Advance Directives Management Services
A set of services that maintain and exchange a patient’s legal documentation such as a living will, durable power of attorney for health care, etc.
Patient Registry Connectivity Services
A set of services that establish group purchasing or licensing agreements for, and assist with implementation of electronic health record applications for interested providers
Clinical Decision Support Services
A mechanism for distributing standardized clinical rules that can be incorporated into electronic health record systems or e-Prescribing systems in support of clinical decision making at the point of care
Continuity of Care Document Delivery of CCD documents to providers and other stakeholders participating in the HIELab Results Exchange A mechanism for facilitating the delivery of patient lab results for use in clinical carePersonal Health Record Exchange Services
A mechanism for facilitating the electronic delivery of personal health information to individual patients’ personal health records that leverages Decision Support Services
21
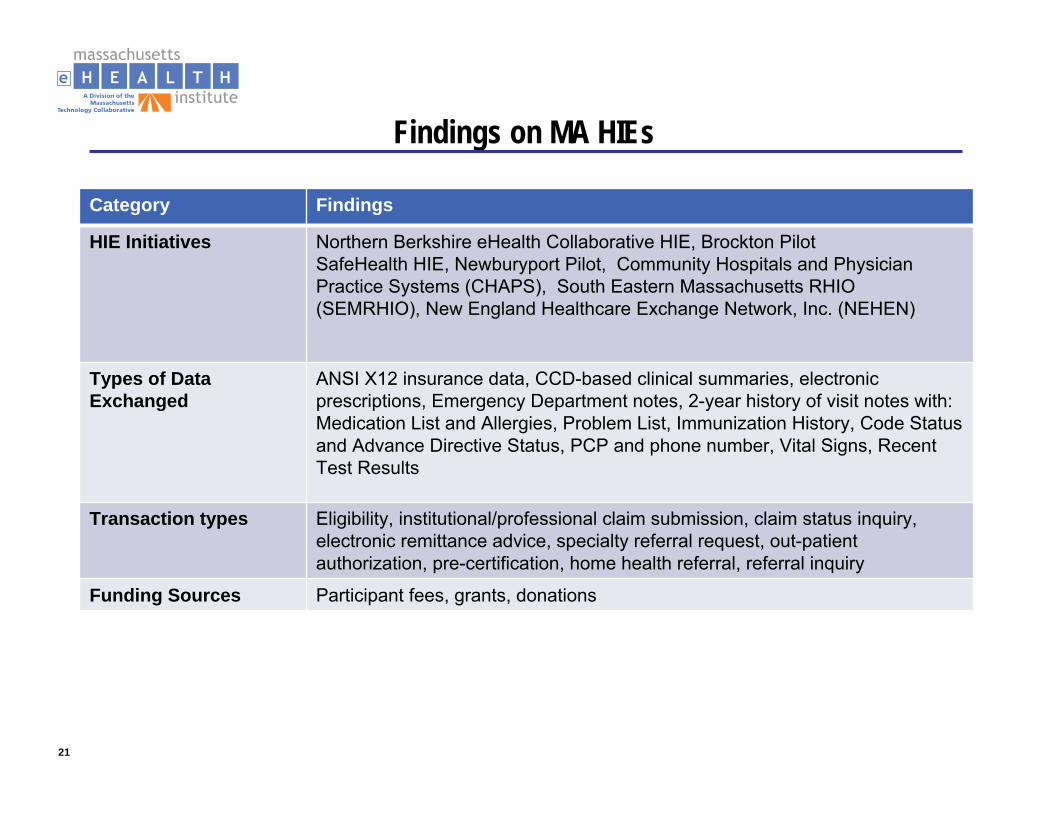
Findings on MA HIEs
Category Findings
HIE Initiatives Northern Berkshire eHealth Collaborative HIE, Brockton PilotSafeHealth HIE, Newburyport Pilot, Community Hospitals and Physician Practice Systems (CHAPS), South Eastern Massachusetts RHIO (SEMRHIO), New England Healthcare Exchange Network, Inc. (NEHEN)
Types of Data Exchanged
ANSI X12 insurance data, CCD-based clinical summaries, electronic prescriptions, Emergency Department notes, 2-year history of visit notes with: Medication List and Allergies, Problem List, Immunization History, Code Status and Advance Directive Status, PCP and phone number, Vital Signs, Recent Test Results
Transaction types Eligibility, institutional/professional claim submission, claim status inquiry, electronic remittance advice, specialty referral request, out-patient authorization, pre-certification, home health referral, referral inquiry
Funding Sources Participant fees, grants, donations

22
Review of Health Information Exchange Planning Requirements
23
Review of HIE Operational Planning RequirementsGeneral PlanningFive Domains– Governance– Finance– Technical Infrastructure– Business and Technical Operations– Legal/Policy
Nationwide Health Information Network (NHIN)Coordination with other States
http://statehieresources.org/

24
General Planning
No one size fits all in a Strategic or Operational Plan. However, there are important factors that must be taken into account to ensure that Plans can serve as effective statewide roadmaps for HIE development that serves the broad public benefit.
Regardless of previous planning efforts, all states under the State HIE Program must revisit their efforts and align current levels of HIE planning with the requirements and opportunities presented under the State HIE Program.
The Strategic Plan and Operational Plan provide a critical blueprint for a state’s progress toward key milestones for Interoperability, as calledfor by HITECH and federal rulemaking, and advanced through the State HIE Program and other related efforts.
http://statehieresources.org/the-toolkit/general-planning/
25
GovernanceGovernance convenes healthcare stakeholders to:
– create trust and consensus on an approach for statewide HIE
– provide oversight and accountability of HIE to protect the public interest. 1
One of the primary purposes of a governance entity is to develop and maintain a multi-stakeholder process, to ensure HIE among providers is in compliance with applicable policies and laws.1
The Operational Plan should describe any ongoing development of the governance model, including alignment with NHIN. It should also identify the following:
– Milestones, interdependencies and timelines that are relevant to any developmental steps that are outlined in the Strategic Plan related to establishing an agreed upon governance structure
– Actions, timeline and milestones for achieving operational status as an NHIO2
1. American Recovery and Reinvestment Act of 2009: State Health Information Exchange Cooperative Agreement Program2. http://statehieresources.org/the-toolkit/general-planning/planning-overview/operational-plan-guidelines/
26
Finance
This domain encompasses the identification and management of financial resources necessary to fund HIE.
It includes public and private financing for building HIE capacity and sustainability. This also includes but is not limited to the following:
– Pricing strategies
– Market research
– Public and private financing strategies
– Financial reporting
– Business planning
– Audits and controls
American Recovery and Reinvestment Act of 2009: State Health Information Exchange Cooperative Agreement Program
27
Finance (cont’d)
The Operational plan should provide detailed cost estimates, timelines and plans for obtaining financing and implementing a sustainable business plan aligned with the Strategic Plan.
It should also include the following:
– High level budget
– Staffing plan
– Processes, timelines, milestones for achieving operational status related to financial management
– Timeline, milestones, activities related to developing and implementing a financing plan and business model
http://statehieresources.org/the-toolkit/general-planning/planning-overview/operational-plan-guidelines/

28
Technical InfrastructureThis domain includes the architecture, hardware, software, applications, network configurations and other technological aspects that physically enable the technical services for HIE in a secure and appropriate manner.1
The Operational Plan should provide detailed timelines, milestones, interdependencies, etc. for implementing the technical infrastructure dimensions outlined in the Strategic Plan. It should also address the following:
– Decision points and decision making contingencies, action steps, etc.
– Processes and timelines for developing alignment with NHIN core services and specifications, standards, NHIO requirements and interconnectivity
– Processes, timelines, etc. for obtaining certification of relevant HIE components and services
– Processes to respond to evolving Meaningful Use criteria2
1. American Recovery and Reinvestment Act of 2009: State Health Information Exchange Cooperative Agreement Program2. http://statehieresources.org/the-toolkit/general-planning/planning-overview/operational-plan-guidelines/
29
Business and Technical Operations The activities in this domain include but are not limited to:– Procurement– Identifying requirements– Process design– Functionality development– Project management– Help desk– Systems maintenance– Change control– Program evaluation– Reporting
Some of these activities and processes are the responsibility of the entity or entities that are implementing the technical services needed for health information exchange; there may be different models for distributing operational responsibilities.
American Recovery and Reinvestment Act of 2009: State Health Information Exchange Cooperative Agreement Program
30
Business and Technical Operations The Operational Plan should include details for how and when the state will implement governance and technical operations, in line with the approaches described in the Strategic Plan
It should include the following:
– Staffing
– Use of consultants
– Procurement processes and timeline
– Contracting processes and timelines
– Development and implementation policies, and standard operating procedures and participation processes
http://statehieresources.org/the-toolkit/general-planning/planning-overview/operational-plan-guidelines/
31
Legal / Policy
The mechanisms and structures in this domain address legal and policy barriers and enablers related to the electronic use and exchange of health information. These mechanisms and structuresinclude but are not limited to policy frameworks, privacy and security requirements for system development and use, data sharing agreements, laws, regulations, and multi-state policy harmonization activities.
The primary purpose of the legal/policy domain is to create a common set of rules to enable inter-organizational and eventually interstate health information exchange, while protecting consumer interests.
American Recovery and Reinvestment Act of 2009: State Health Information Exchange Cooperative Agreement Program
32
Legal / Policy (cont’d)
The Operational Plan needs to describe the steps to be taken, timeline, interdependencies, etc. for developing and implementing the organizational and technical approaches outlined in the Strategic Plan, including the following:
– Steps to implement the appropriate structure for the legal entity that will provide governance
– Steps to implement policies and protocols for how the statewide HIE will foster compliance with applicable federal and state legal and policy requirements, including addressing interdependencies between policy requirements, HIE governance and oversight mechanisms.
– Processes, timelines, etc. for ongoing development, in response to applicable federal requirements for utilization and protection of health data, aligning with the state’s strategy for HIE with federal care delivery organizations (VA, DoD, HIS, etc.).
http://statehieresources.org/the-toolkit/general-planning/planning-overview/operational-plan-guidelines/
33
Nationwide Health Information Network (NHIN)
The Nationwide Health Information Network (NHIN) is a collection of standards, protocols, legal agreements, specifications and services that enable the secure exchange of health information over the internet.
NHIN is a key component of the nationwide health information technology strategy and will provide a common platform for health information exchange across diverse entities, within communities and across the country.
As a critical part of the national health IT agenda, it will enable health information to follow the consumer, be available for clinical decision making, and support appropriate use of health care information beyond direct patient care, so as to improve public health.
http://statehieresources.org/the-toolkit/nationwide-health-information-network/nhin-overview/
34
Coordination with Other StatesAligned with the Strategic Plan, the Operational Plan should describe the specific timeline and multi-state coordinated activities, milestones, dependencies among states relative to establishing an interstate approach for secure HIE.The scope of these activities may include the following:– Plans for bringing up HIE services – Policy development/determination – Legislative action, if required
http://statehieresources.org/the-toolkit/general-planning/planning-overview/operational-plan-guidelines/
35
Inter-state Collaboration Critical for HIEMassachusetts helped form a New England coalition focused on collaborating on issues pertinent to eHealth activity in this region including state agencies, quasi-public agencies, non-profits and other organizations in the following states:– Connecticut – New York is interested in working with Massachusetts– Maine – Massachusetts– New Hampshire– Rhode Island– Vermont
Group meets monthly to share, learn and identify priorities for focus among the New England states in Health IT.– Share best practices, manage overlapping patients– Work jointly on issues pertinent across our states– Optimize opportunities relevant to health information technology
Initial opportunities for collaboration have been identified including the following:– Develop necessary interfaces and touch points and address overlaps in the development of the
various Health Information Exchange systems in region– Agree on full education curriculum for providers and future workforce – Create centers of excellence for the various EHR systems that meet HHS Certification, with
resources available to others in the region who need specific help – Privacy policy harmonization: the states have adopted, and are adopting, different privacy policies
that will need to be harmonized, or at least dealt with, as patients cross state lines– Sharing of best practices and lessons learned in various state-wide deployments of EHR and HIE
36
Next StepsHow do we get work done?How do we coordinate with other groups?Schedule next meeting at location of choice
Rick Shoup, Ph.D., Director of [email protected]@maehi.org
37
Appendix A: HIE Section of Review of Health IT Plan
Deloitte November 2009
38
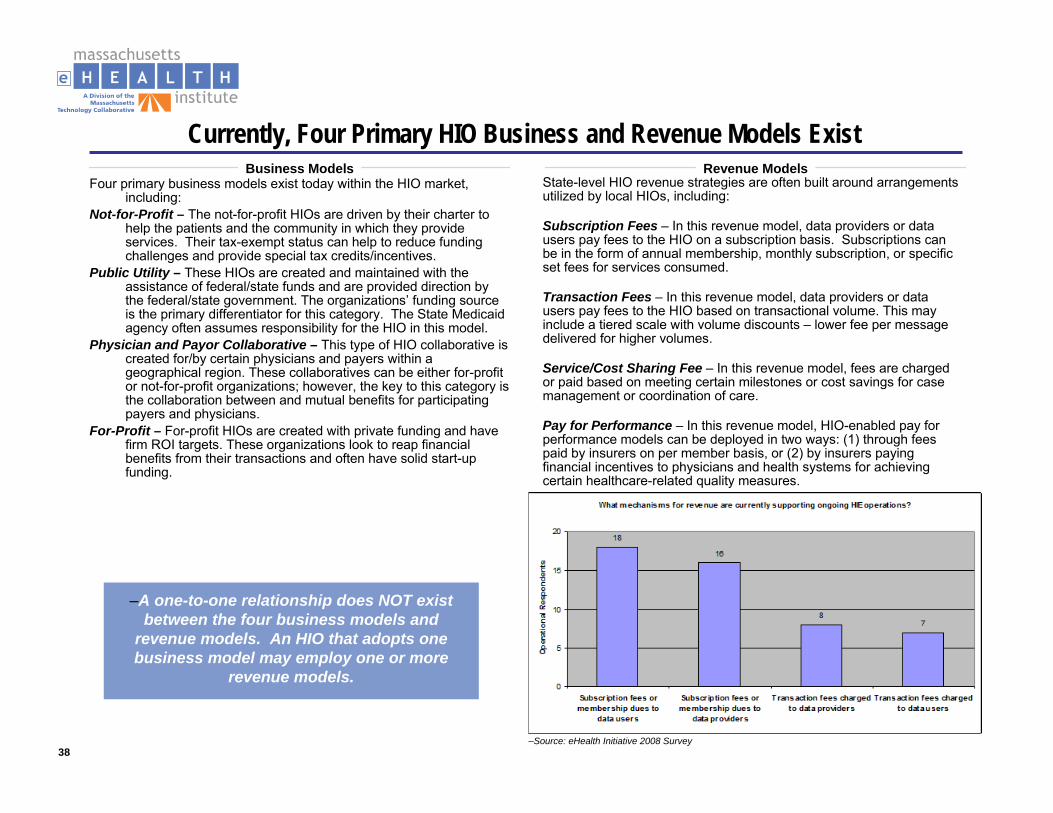
Currently, Four Primary HIO Business and Revenue Models ExistBusiness Models Revenue Models
Four primary business models exist today within the HIO market, including:
Not-for-Profit – The not-for-profit HIOs are driven by their charter to help the patients and the community in which they provide services. Their tax-exempt status can help to reduce funding challenges and provide special tax credits/incentives.
Public Utility – These HIOs are created and maintained with the assistance of federal/state funds and are provided direction by the federal/state government. The organizations’ funding source is the primary differentiator for this category. The State Medicaid agency often assumes responsibility for the HIO in this model.
Physician and Payor Collaborative – This type of HIO collaborative is created for/by certain physicians and payers within a geographical region. These collaboratives can be either for-profit or not-for-profit organizations; however, the key to this category is the collaboration between and mutual benefits for participating payers and physicians.
For-Profit – For-profit HIOs are created with private funding and have firm ROI targets. These organizations look to reap financial benefits from their transactions and often have solid start-up funding.
State-level HIO revenue strategies are often built around arrangementsutilized by local HIOs, including:
Subscription Fees – In this revenue model, data providers or data users pay fees to the HIO on a subscription basis. Subscriptions can be in the form of annual membership, monthly subscription, or specific set fees for services consumed.
Transaction Fees – In this revenue model, data providers or data users pay fees to the HIO based on transactional volume. This may include a tiered scale with volume discounts – lower fee per message delivered for higher volumes.
Service/Cost Sharing Fee – In this revenue model, fees are charged or paid based on meeting certain milestones or cost savings for case management or coordination of care.
Pay for Performance – In this revenue model, HIO-enabled pay for performance models can be deployed in two ways: (1) through feespaid by insurers on per member basis, or (2) by insurers paying financial incentives to physicians and health systems for achieving certain healthcare-related quality measures.
–A one-to-one relationship does NOT exist between the four business models and
revenue models. An HIO that adopts one business model may employ one or more
revenue models.
–Source: eHealth Initiative 2008 Survey
39
Revenue Model: Subscription FeesSubscription Fees
Description: Data providers or data users pay fees to the HIO based on subscription basis. Subscriptions can be in the form of annual membership, monthly subscription, or specific set fee for services consumed; e.g., .infrastructure management, applications –MPI/RLS. In addition, there may be fee levels or tiers based onrelative size – expenses or number of results delivered.43% of the 42 operational HIOs use subscription fees. The Vermont Health IT Fund, which supports health IT and statewide HIE activities in Vermont, is based on a subscription model. Each health insurer operating in Vermont pays a quarterly fee in one of two ways: either by paying 0.199% of all health care claims paidfor their Vermont members in the previous quarter, or a fee based on the insurer’s proportion of overall claims in the past year
Advantages:.Provides a more predictable cost for the member organization
Provides a more predictable revenue stream for the HIO
Avoids the need to track the number – potentially millions – of transactions each month for the purposes of affixing charges to each transaction
As an accounting function, subscription fees, which can also be seen as membership dues, are less taxing than transaction fees and are not as susceptible to accounting error
Example: New England Healthcare EDI Network (NEHEN)
–New England Healthcare EDI Network (NEHEN)–Established 1998
–NEHEN is a consortium of regional payers and providers who have designed and implemented a secure and innovative electronic-commerce solution for reducing administrative costs in health care.
–The mission of NEHEN is to be the premier innovator in bringing best practices with business and technical solutions to the healthcare industry for payer-provider transaction processing. NEHEN is a member-owned organization that emphasizes collaboration, a federated model, and a standards-based electronic healthcare data exchange. NEHENNet provides a single gateway into the five largest health plans’ most popular and essential electronic transactions to:
–The service is accessible through a web browser and Internet connection. This regionally-focused online service reduces administrative time and costs, increases regulatory compliance, and promotes a regional solution for many common provider transaction needs.
–New England. Number of covered lives in the coverage area: 5.0 million. Number of total patients in the coverage area: 6.0 million. Number of practicing physicians in the coverage area: over 25,000.
check patient insurance eligibility, individually or in batch
check patient eligibility with many payers simultaneously
make referral requests
check claim status
submit claim files
view electronic explanations of benefits (remittances).
40
Revenue Model: Service/Cost Sharing FeeService/Cost Sharing Fee
Description: Fees are charged or paid based on meeting certain milestones or cost savings for case management or coordination of care. Medicare Demonstrations, including the Medicare Health Support and Physician Group Practice Initiative, are two examples of payment systems whereby providers share in the generated savings. For HIO-enabled disease management programs, payers and purchasers pay HIO for delivery of disease management service on per member/per month basis.
Advantages:.None Identified
Considerations:
Sustainability models built on cost sharing mechanisms requires data to substantiate the projected cost savings. Some observers have noted that the data to demonstrate waste reduction and cost savings could take years to accumulate and analyze.
Example: Tennessee (Carespark)
–Tennessee CareSpark RHIO (CareSpark)–Established 2005
–CareSpark is a nonprofit organization with the purpose of developing and implementing a collaborative system for health improvements in a 17-county region of northeast Tennessee and southwest Virginia area with approximately 750,000 residents, 18hospitals, and 1,200 physicians. –CareSpark is developing a secure network that allows physician offices, hospitals, public health departments, pharmacies, laboratories and imaging centers to communicate electronically in order to improve patient care and safety and reduce costs. –Members of the CareSpark Clinical workgroup identified five priority health issues to be targeted through this effort: Diabetes, Hypertension and Stroke, Cardiovascular Disease, Asthma and Lung Disease, Cancer. –The Care Data Exchange will be a peer-to-peer network allowing holders of electronic medical records to retain and maintain data while a search interface handles security, record identification, and distribution.
41
Revenue Model: Pay for PerformanceService/Cost Sharing Fee
Description: Fees are charged or paid based on meeting certain milestones or cost savings for case management or coordination of care. Medicare Demonstrations, including the Medicare Health Support and Physician Group Practice Initiative, are two examples of payment systems whereby providers share in the generated savings. For HIO-enabled disease management programs, payers and purchasers pay HIO for delivery of disease management service on per member/per month basis.
Advantages:.None Identified
Considerations:
Sustainability models built on cost sharing mechanisms requires data to substantiate the projected cost savings. Some observers have noted that the data to demonstrate waste reduction and cost savings could take years to accumulate and analyze.
Example: Tennessee (Carespark)
–Tennessee CareSpark RHIO (CareSpark)–Established 2005
–CareSpark is a nonprofit organization with the purpose of developing and implementing a collaborative system for health improvements in a 17-county region of northeast Tennessee and southwest Virginia area with approximately 750,000 residents, 18hospitals, and 1,200 physicians. –CareSpark is developing a secure network that allows physician offices, hospitals, public health departments, pharmacies, laboratories and imaging centers to communicate electronically in order to improve patient care and safety and reduce costs. –Members of the CareSpark Clinical workgroup identified five priority health issues to be targeted through this effort: Diabetes, Hypertension and Stroke, Cardiovascular Disease, Asthma and Lung Disease, Cancer. –The Care Data Exchange will be a peer-to-peer network allowing holders of electronic medical records to retain and maintain data while a search interface handles security, record identification, and distribution.
42
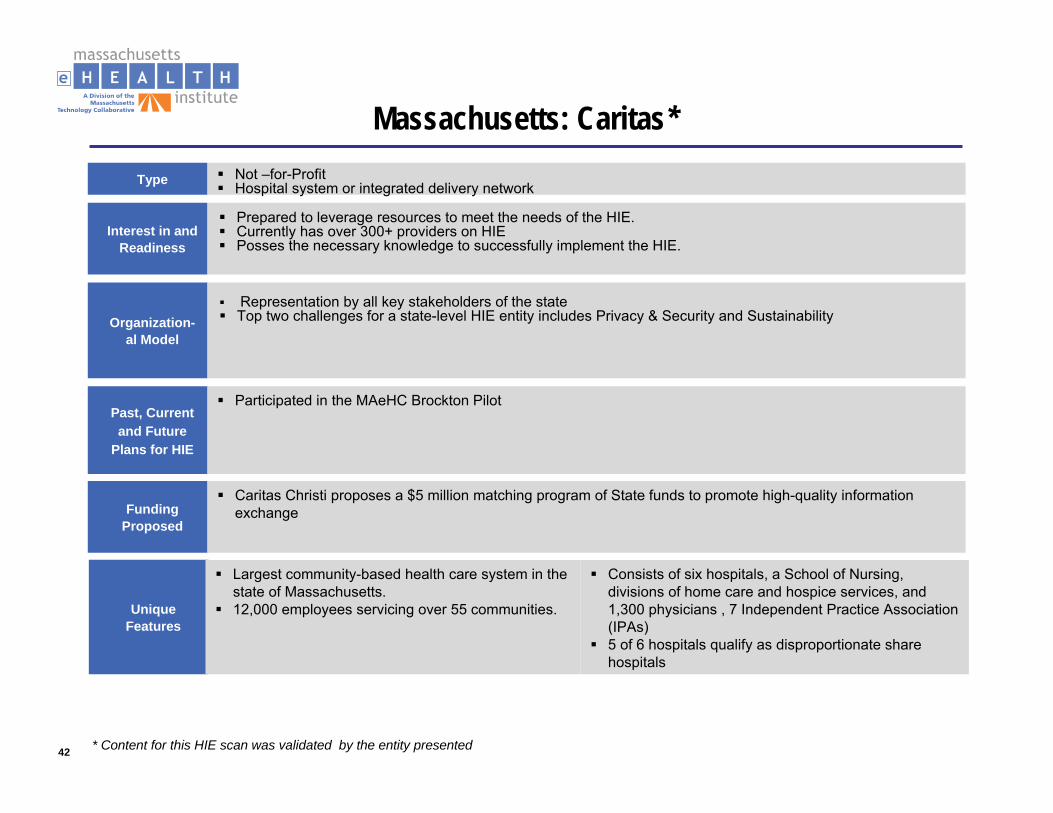
Massachusetts: Caritas*Type Not –for-Profit
Hospital system or integrated delivery network
Organization-al Model
Past, Current and Future
Plans for HIE
Participated in the MAeHC Brockton Pilot
FundingProposed
Interest in and Readiness
Unique Features
Largest community-based health care system in the state of Massachusetts.12,000 employees servicing over 55 communities.
Consists of six hospitals, a School of Nursing, divisions of home care and hospice services, and 1,300 physicians , 7 Independent Practice Association (IPAs) 5 of 6 hospitals qualify as disproportionate share hospitals
Prepared to leverage resources to meet the needs of the HIE.Currently has over 300+ providers on HIEPosses the necessary knowledge to successfully implement the HIE.
Caritas Christi proposes a $5 million matching program of State funds to promote high-quality information exchange
Representation by all key stakeholders of the stateTop two challenges for a state-level HIE entity includes Privacy & Security and Sustainability
* Content for this HIE scan was validated by the entity presented
43
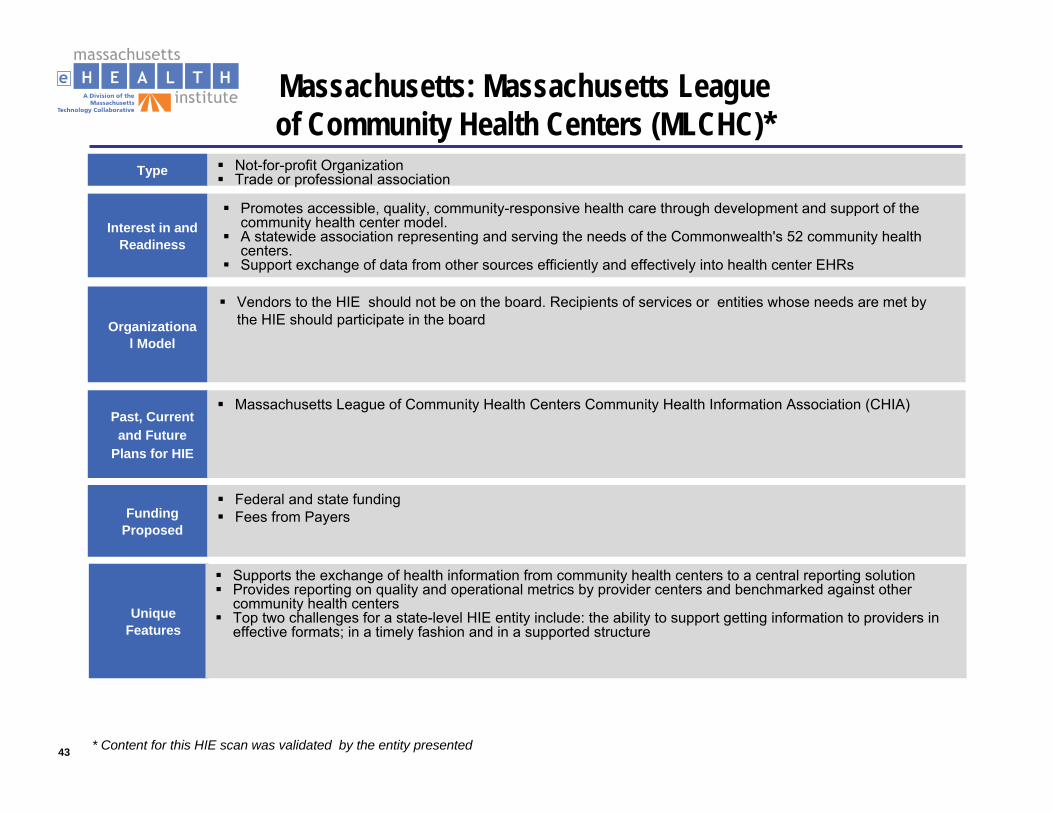
Massachusetts: Massachusetts Leagueof Community Health Centers (MLCHC)*
Type Not-for-profit OrganizationTrade or professional association
Organizational Model
Past, Current and Future
Plans for HIE
Massachusetts League of Community Health Centers Community Health Information Association (CHIA)
FundingProposed
Interest in and Readiness
Unique Features
Supports the exchange of health information from community health centers to a central reporting solutionProvides reporting on quality and operational metrics by provider centers and benchmarked against other community health centers Top two challenges for a state-level HIE entity include: the ability to support getting information to providers in effective formats; in a timely fashion and in a supported structure
Promotes accessible, quality, community-responsive health care through development and support of the community health center model.A statewide association representing and serving the needs of the Commonwealth's 52 community health centers.Support exchange of data from other sources efficiently and effectively into health center EHRs
Federal and state fundingFees from Payers
Vendors to the HIE should not be on the board. Recipients of services or entities whose needs are met by the HIE should participate in the board
* Content for this HIE scan was validated by the entity presented
44
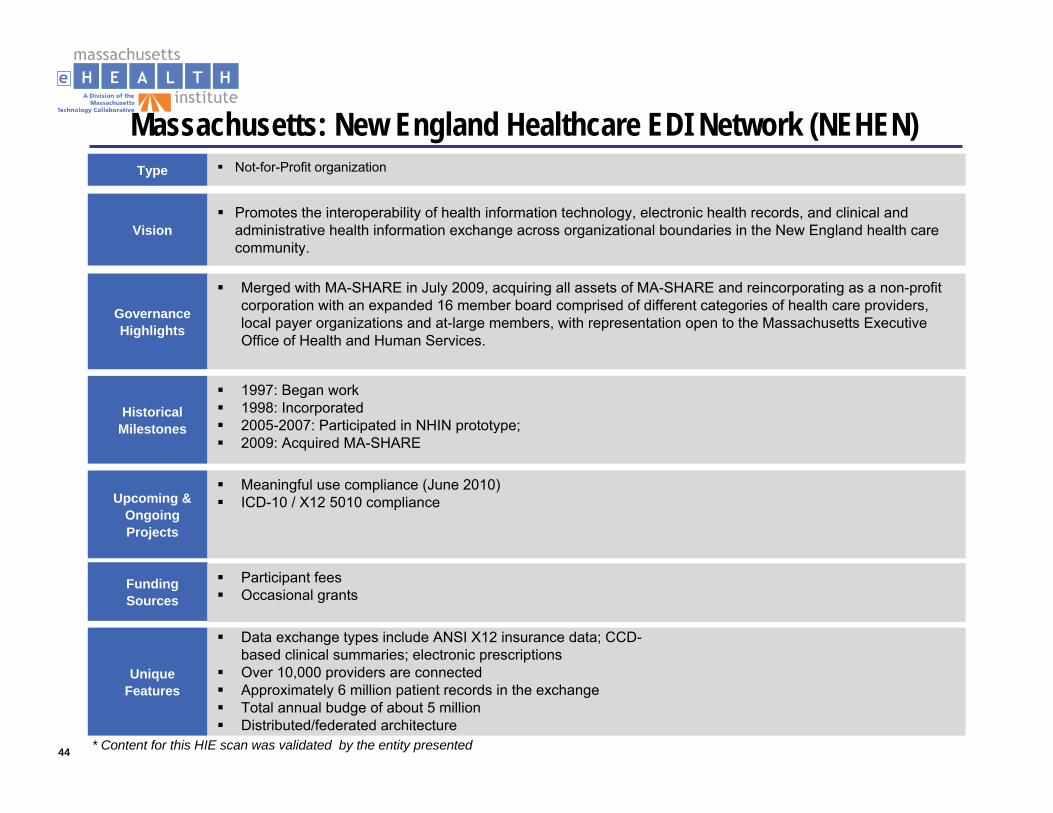
Massachusetts: New England Healthcare EDI Network (NEHEN)Type Not-for-Profit organization
Governance Highlights
Merged with MA-SHARE in July 2009, acquiring all assets of MA-SHARE and reincorporating as a non-profit corporation with an expanded 16 member board comprised of different categories of health care providers, local payer organizations and at-large members, with representation open to the Massachusetts Executive Office of Health and Human Services.
Historical Milestones
1997: Began work1998: Incorporated2005-2007: Participated in NHIN prototype; 2009: Acquired MA-SHARE
FundingSources
Participant feesOccasional grants
VisionPromotes the interoperability of health information technology, electronic health records, and clinical and administrative health information exchange across organizational boundaries in the New England health care community.
Upcoming & Ongoing Projects
Meaningful use compliance (June 2010)ICD-10 / X12 5010 compliance
Unique Features
Data exchange types include ANSI X12 insurance data; CCD-based clinical summaries; electronic prescriptionsOver 10,000 providers are connectedApproximately 6 million patient records in the exchangeTotal annual budge of about 5 millionDistributed/federated architecture
* Content for this HIE scan was validated by the entity presented
45
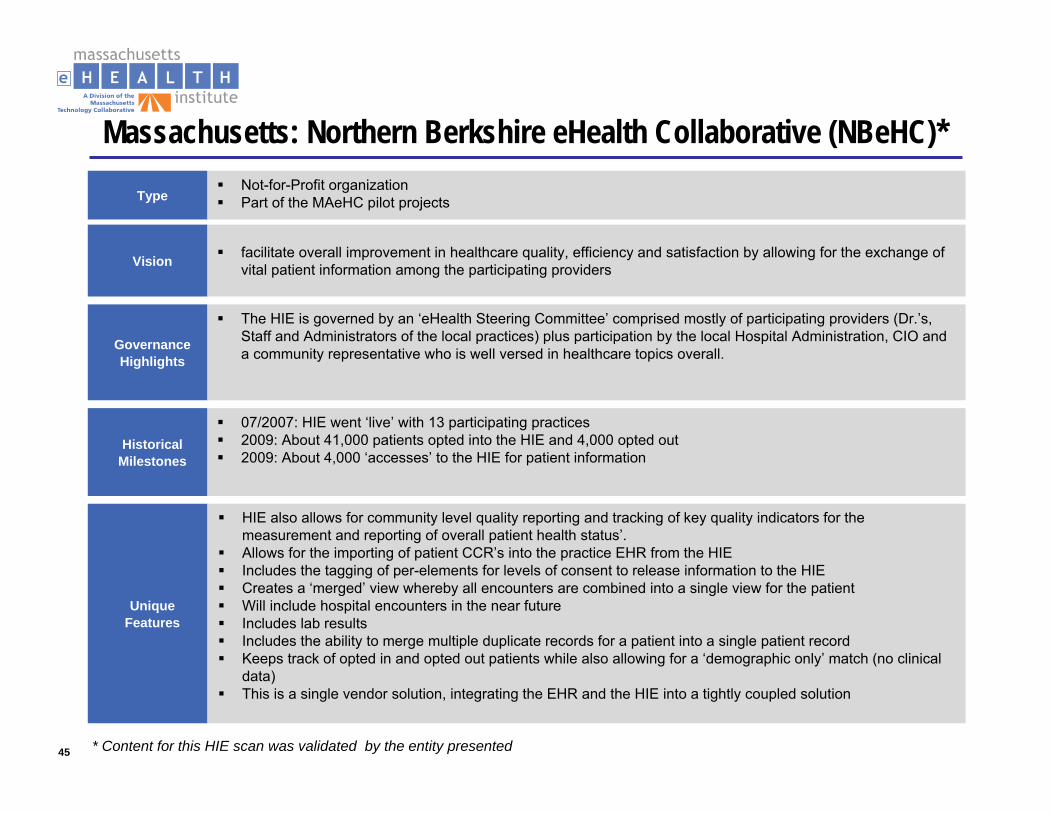
Massachusetts: Northern Berkshire eHealth Collaborative (NBeHC)*
TypeNot-for-Profit organizationPart of the MAeHC pilot projects
Governance Highlights
The HIE is governed by an ‘eHealth Steering Committee’ comprised mostly of participating providers (Dr.’s, Staff and Administrators of the local practices) plus participation by the local Hospital Administration, CIO and a community representative who is well versed in healthcare topics overall.
Historical Milestones
07/2007: HIE went ‘live’ with 13 participating practices2009: About 41,000 patients opted into the HIE and 4,000 opted out2009: About 4,000 ‘accesses’ to the HIE for patient information
Vision facilitate overall improvement in healthcare quality, efficiency and satisfaction by allowing for the exchange of vital patient information among the participating providers
Unique Features
HIE also allows for community level quality reporting and tracking of key quality indicators for the measurement and reporting of overall patient health status’.Allows for the importing of patient CCR’s into the practice EHR from the HIEIncludes the tagging of per-elements for levels of consent to release information to the HIECreates a ‘merged’ view whereby all encounters are combined into a single view for the patientWill include hospital encounters in the near futureIncludes lab resultsIncludes the ability to merge multiple duplicate records for a patient into a single patient recordKeeps track of opted in and opted out patients while also allowing for a ‘demographic only’ match (no clinical data)This is a single vendor solution, integrating the EHR and the HIE into a tightly coupled solution
* Content for this HIE scan was validated by the entity presented
46
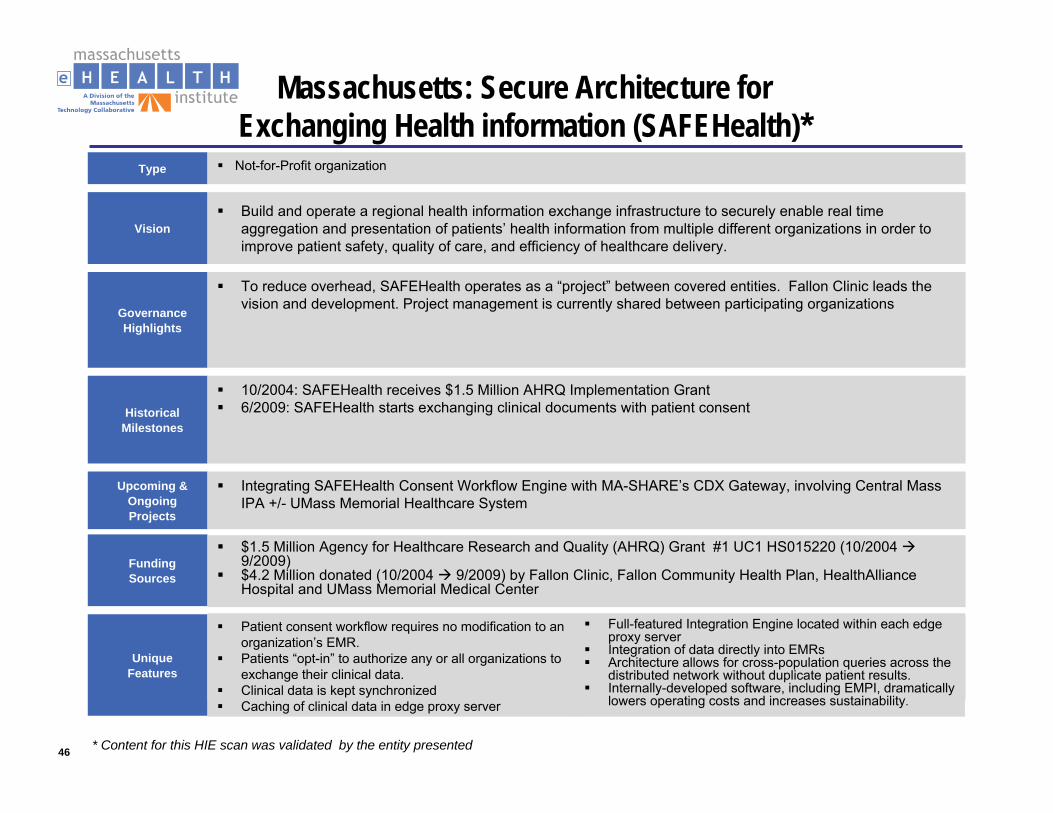
Massachusetts: Secure Architecture for Exchanging Health information (SAFEHealth)*
Type Not-for-Profit organization
Governance Highlights
To reduce overhead, SAFEHealth operates as a “project” between covered entities. Fallon Clinic leads the vision and development. Project management is currently shared between participating organizations
Historical Milestones
10/2004: SAFEHealth receives $1.5 Million AHRQ Implementation Grant6/2009: SAFEHealth starts exchanging clinical documents with patient consent
FundingSources
$1.5 Million Agency for Healthcare Research and Quality (AHRQ) Grant #1 UC1 HS015220 (10/2004 9/2009)$4.2 Million donated (10/2004 9/2009) by Fallon Clinic, Fallon Community Health Plan, HealthAlliance Hospital and UMass Memorial Medical Center
VisionBuild and operate a regional health information exchange infrastructure to securely enable real time aggregation and presentation of patients’ health information from multiple different organizations in order to improve patient safety, quality of care, and efficiency of healthcare delivery.
Upcoming & Ongoing Projects
Integrating SAFEHealth Consent Workflow Engine with MA-SHARE’s CDX Gateway, involving Central Mass IPA +/- UMass Memorial Healthcare System
Unique Features
Patient consent workflow requires no modification to an organization’s EMR. Patients “opt-in” to authorize any or all organizations to exchange their clinical data.Clinical data is kept synchronizedCaching of clinical data in edge proxy server
Full-featured Integration Engine located within each edge proxy serverIntegration of data directly into EMRsArchitecture allows for cross-population queries across the distributed network without duplicate patient results.Internally-developed software, including EMPI, dramatically lowers operating costs and increases sustainability.
* Content for this HIE scan was validated by the entity presented
47
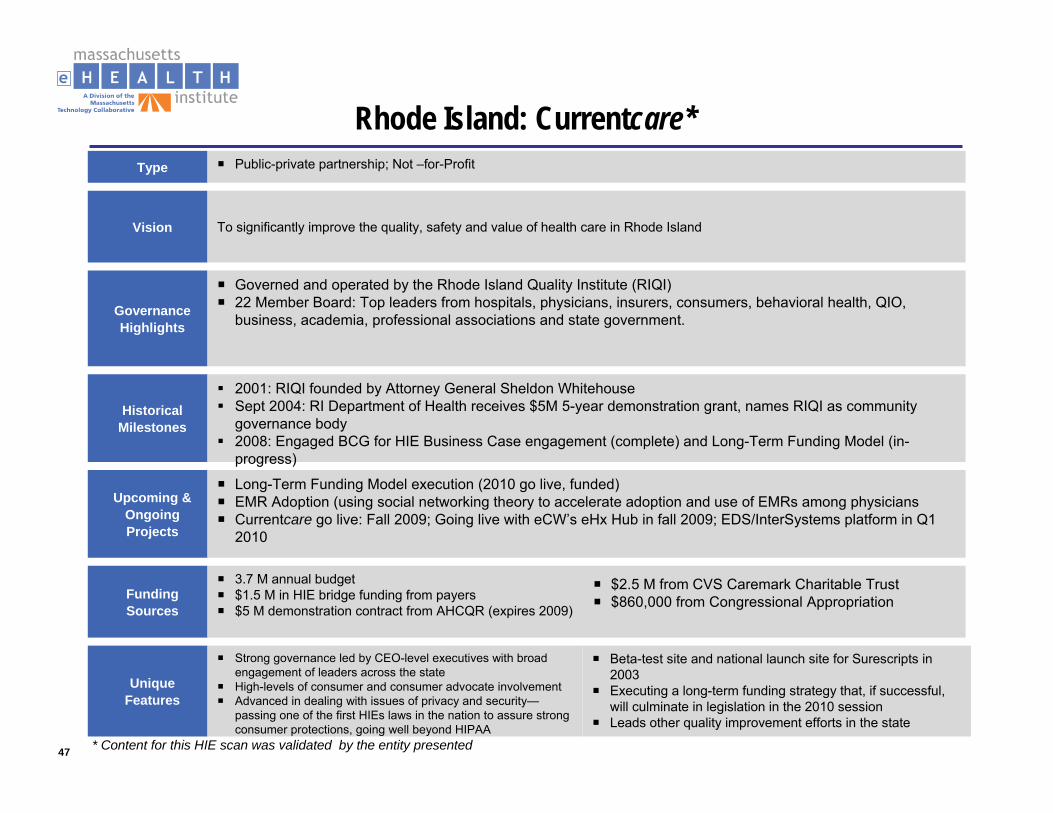
Rhode Island: Currentcare*Type Public-private partnership; Not –for-Profit
Governance Highlights
Governed and operated by the Rhode Island Quality Institute (RIQI)22 Member Board: Top leaders from hospitals, physicians, insurers, consumers, behavioral health, QIO, business, academia, professional associations and state government.
Historical Milestones
2001: RIQI founded by Attorney General Sheldon WhitehouseSept 2004: RI Department of Health receives $5M 5-year demonstration grant, names RIQI as community governance body2008: Engaged BCG for HIE Business Case engagement (complete) and Long-Term Funding Model (in-progress)June 2008: RI Health Information Exchange Act (ground-breaking privacy & security legislation)Sept 2008: patients began enrolling
FundingSources
3.7 M annual budget$1.5 M in HIE bridge funding from payers$5 M demonstration contract from AHCQR (expires 2009)
Vision To significantly improve the quality, safety and value of health care in Rhode Island
Upcoming & Ongoing Projects
Long-Term Funding Model execution (2010 go live, funded)EMR Adoption (using social networking theory to accelerate adoption and use of EMRs among physiciansCurrentcare go live: Fall 2009; Going live with eCW’s eHx Hub in fall 2009; EDS/InterSystems platform in Q1 2010
Unique Features
Strong governance led by CEO-level executives with broad engagement of leaders across the stateHigh-levels of consumer and consumer advocate involvementAdvanced in dealing with issues of privacy and security—passing one of the first HIEs laws in the nation to assure strong consumer protections, going well beyond HIPAA
Beta-test site and national launch site for Surescripts in 2003Executing a long-term funding strategy that, if successful, will culminate in legislation in the 2010 sessionLeads other quality improvement efforts in the state
$2.5 M from CVS Caremark Charitable Trust$860,000 from Congressional Appropriation
* Content for this HIE scan was validated by the entity presented

48
Michigan Health Information Network (MiHIN)*Type Public-private partnership; MI Dept of Community Health & Dept of IT
Governance Highlights
HIT Commission, appointed by Governor, serves as an advisory board to the MDHCWide group of stakeholders (13) that oversee the MiHIN’s activities and advise the MiHIN Resource Center that supports the various RHIOs within the state
Historical Milestones
April 3, 2006: MiHIN begins Conduit of Care ProjectMay 2006: HIT Commission created
Contract to participate in HISPCJune 2007: State provides funding to 7 of 9 MiHIN Regions to begin HIE planning & implementationAugust 2008: State provides funding to remaining 2 MiHIN regions to begin HIE planning
FundingSources
$10 M in state-appropriated funds (FY07-FY08)HISPC Funding
Vision The MiHIN Resource Center will foster development of health information exchanges that reduce health care costs while increasing quality and patient safety.
Upcoming & Ongoing Projects
HISPC project (funded)MiHIN Project (funded)
* Content for this HIE scan was validated by the entity presented
49
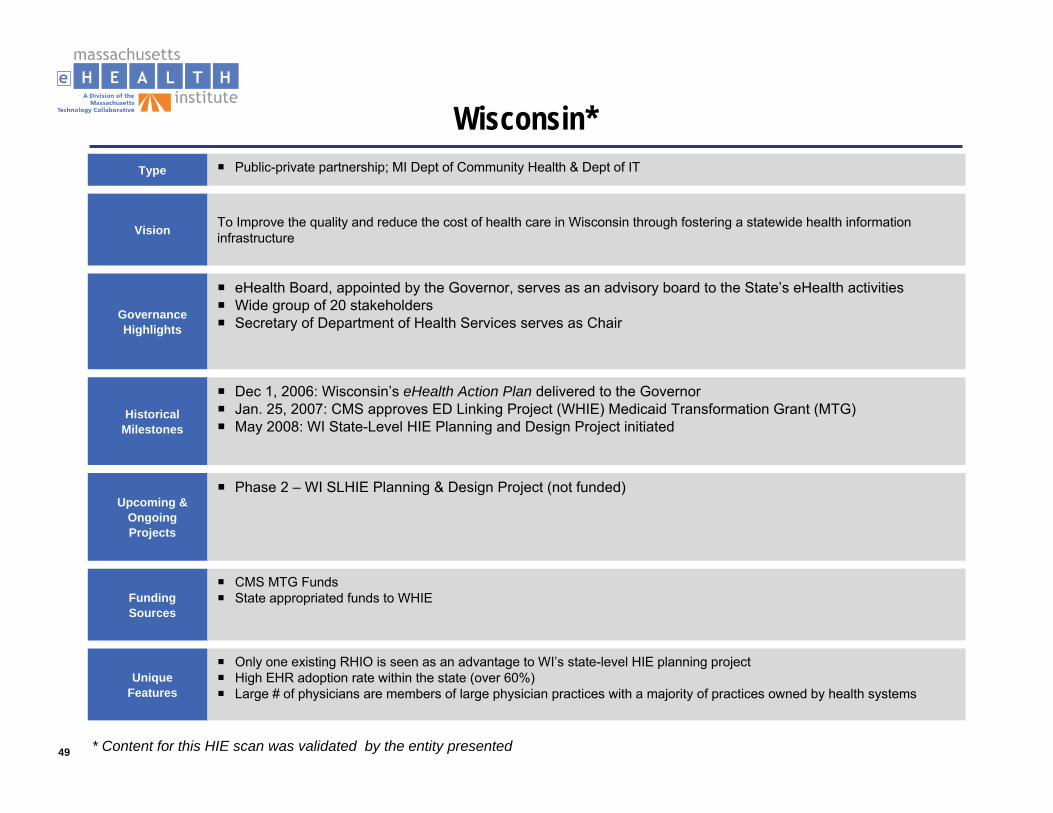
Wisconsin*Type Public-private partnership; MI Dept of Community Health & Dept of IT
Governance Highlights
eHealth Board, appointed by the Governor, serves as an advisory board to the State’s eHealth activitiesWide group of 20 stakeholdersSecretary of Department of Health Services serves as Chair
Historical Milestones
Dec 1, 2006: Wisconsin’s eHealth Action Plan delivered to the GovernorJan. 25, 2007: CMS approves ED Linking Project (WHIE) Medicaid Transformation Grant (MTG)May 2008: WI State-Level HIE Planning and Design Project initiated
FundingSources
CMS MTG FundsState appropriated funds to WHIE
Vision To Improve the quality and reduce the cost of health care in Wisconsin through fostering a statewide health information infrastructure
Upcoming & Ongoing Projects
Phase 2 – WI SLHIE Planning & Design Project (not funded)
Unique Features
Only one existing RHIO is seen as an advantage to WI’s state-level HIE planning projectHigh EHR adoption rate within the state (over 60%)Large # of physicians are members of large physician practices with a majority of practices owned by health systems
* Content for this HIE scan was validated by the entity presented
50
New York eHealth Collaborative (NYeC)
Type Public-private partnership; 501 (c)(3) Not –for-Profit
Governance Highlights
Financial sustainability committee, consumer advisory council, Policy and operations council, Education and communication committee
DOH, NYeC Board, Policy and Operations Council provide oversight and governanceNYeC Board Composition: HANYS, Medical Association, government, insurers, providers, non-profitsExecutive director and program manager
Historical Milestones
2006: HEAL NY bill passed (Healthcare Efficiency and Affordability Law for New Yorkers)Dec 2006: NYeC IncorporatedAug 2007: Designated a public-private partnership by DOHMarch 2008: NY State Department of Health awards $105 M in funding for 19 HIT projects
FundingSources
$1B budgeted over 4 years: HEAL funding capital financing - $250M for HIT initiatives– $56 M State funds for HEAL Phase 1 (2006)-26 grants– $105M State funds for 19 RHIO-level exchanges through HEAL 5 Grants (2008)– $5 M of this set aside for NYeC to manage the statewide collaboration process (Spring 2009-2011)
VisionNYeC will become a trusted, independent voice that can reflect a diverse array of interests and perspectives on key policies and standards to ensure that health IT implementation efforts are successful, and to realize the state's return on investment under HEAL-NY and other funding mechanisms. (http://www.nyehealth.org/vision)
Upcoming & Ongoing Projects
HEAL NY Project (2006), HEAL NY Phase 5 (March 2008)Developing HIT and HIE Policies and StandardsEvaluating and establishing accountability measures for NY’s Health IT StrategyConvening, educating and engaging key constituencies
51
West Virginia Health Information Network (WVHIN)
Type Public-private partnership
Governance Highlights
Healthcare associations, state CIO, payers, physicians17 members, 1 chairman (neurosurgeon)Finance committee, executive committee, physician advisory council, technical committee
FundingSources
$3.5M in start-up funding from State
VisionThe purpose of the West Virginia Health Information Network (WVHIN) is to promote the design, implementation, operation, and maintenance of a network to facilitate public and private use of health care inforamtion in the State. It is intended that the network be a public-private partnership for the benefit of all of the citizens of this State.
Upcoming & Ongoing Projects
Goal: 3-phase, 5-year roll-out of the statewide HIE; financial sustainability 3-5 years later through fee-structurePhase 1: Messaging; Phase 2: Coordinated Care; Phase 3: Quality Value
Unique Features
WVHIN is the convener and collaborator of all initiatives. They will implement by community but create a statewide network

52
Arizona Medical Information Exchange (AMIE)
Type 501 (c)(3) Not –for-Profit
Governance Highlights
AHCCCS (Arizona Health Care Cost Containment System) houses and operates the HIEGovernance Board and Board CommitteesAMIE is a government entityAMIE staffed by Project Director, Medical Director, several analysts and developers
Historical Milestones
Jan. 25,2000: AHCCCS awarded Medicaid Transformation Grant (MTG)Sept. 28, 2008: AMIE Proof of Concept is launchedDec. 29, 2008: Proof of Concept ends and evaluation of findings performed to guide next stepsFeb 1, 2009: AMIE Behavioral Health Expansion begins
FundingSources
MTG Grant through Sept. 2009Exploring other options: transaction, subscription or membership fees
Vision The Arizona Medical Information Exchange (AMIE) is a secure, web-based utility that provides health care providers instant access to your health information at the time you are receiving care.
53
Delaware Health Information Network (DHIN)
Type Public-private partnership; Quasi-public agency under direction of Delaware Health Care Commission
Governance Highlights
State government (3), Provider (1), Hospital (1), Payer (2), University of Delaware, Delaware Medical Society, DOH (1), Purchaser (1)Chair of Board appointed by Delaware Health Care Commission (DHCC)
Historical Milestones
1997: DHIN established by Delaware General AssemblyMarch 2006: RFP published for design and build of clinical information exchange (awarded to Medicity and Perot systems)June 2006: RFP for Quality Assurance Monitoring published
FundingSources
$4.7 M AHRG grant funding$2M state-appropriated funds (Bond and Capital Improvements budget)$2M community-based partner contributions (required matching funds)$700,000 Earmark through Federal budget (2004)
VisionShare real-time clinical information among all health care providers (office practices, hospitals, labs, diagnostic facilities, etc.) across the state to improve patient outcomes and patient-provider relationships, while reducing service duplication and the rate of increase in health care spending
Unique Features
Future services to include clinical messaging, clinical decision support, disease management module billing functions, claims retrieval and claims processingDelaware population < 1 M
54
Maine: HealthInfoNet Network
Type Public-private partnership; 501 (c)(3) Not-for-Profit
Governance Highlights
Consumer Advisory Committee assist in the development of electronic Personal Health Records (PHRs)Technology and Professional Practice Advisory Committee support implementing and sustaining a statewide HIE18 member Board of Directors, 1 Board Chairman
Historical Milestones
2004: Maine Health Information Network Technology created2005: HealthInfoNet established2009: HealthInfoNet Go-Live
FundingSources
Foundation, provider and government funded$8M raised so far$1.7M from State for 2010-2011
Upcoming & Ongoing Projects
Build ME statewide infrastructureExpand HealthInfoNet
55
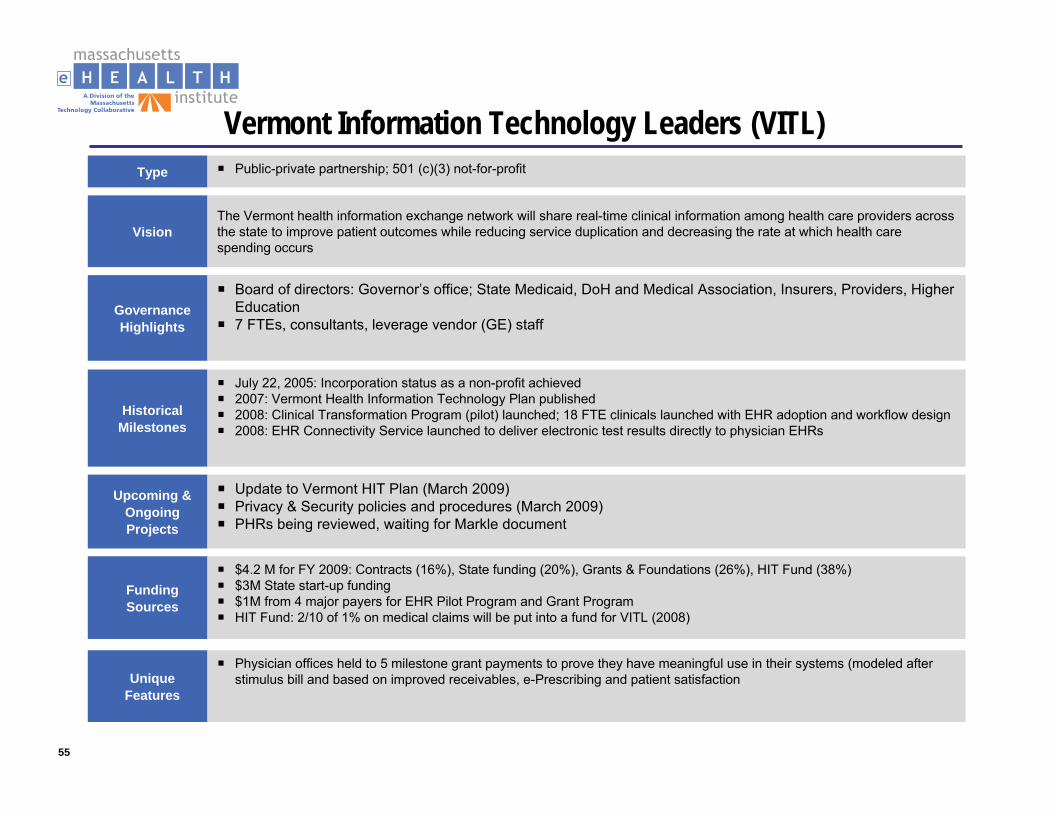
Vermont Information Technology Leaders (VITL)Type Public-private partnership; 501 (c)(3) not-for-profit
Governance Highlights
Board of directors: Governor’s office; State Medicaid, DoH and Medical Association, Insurers, Providers, Higher Education7 FTEs, consultants, leverage vendor (GE) staff
Historical Milestones
July 22, 2005: Incorporation status as a non-profit achieved2007: Vermont Health Information Technology Plan published2008: Clinical Transformation Program (pilot) launched; 18 FTE clinicals launched with EHR adoption and workflow design2008: EHR Connectivity Service launched to deliver electronic test results directly to physician EHRs
FundingSources
$4.2 M for FY 2009: Contracts (16%), State funding (20%), Grants & Foundations (26%), HIT Fund (38%)$3M State start-up funding$1M from 4 major payers for EHR Pilot Program and Grant ProgramHIT Fund: 2/10 of 1% on medical claims will be put into a fund for VITL (2008)
VisionThe Vermont health information exchange network will share real-time clinical information among health care providers across the state to improve patient outcomes while reducing service duplication and decreasing the rate at which health care spending occurs
Upcoming & Ongoing Projects
Update to Vermont HIT Plan (March 2009)Privacy & Security policies and procedures (March 2009)PHRs being reviewed, waiting for Markle document
Unique Features
Physician offices held to 5 milestone grant payments to prove they have meaningful use in their systems (modeled after stimulus bill and based on improved receivables, e-Prescribing and patient satisfaction
56
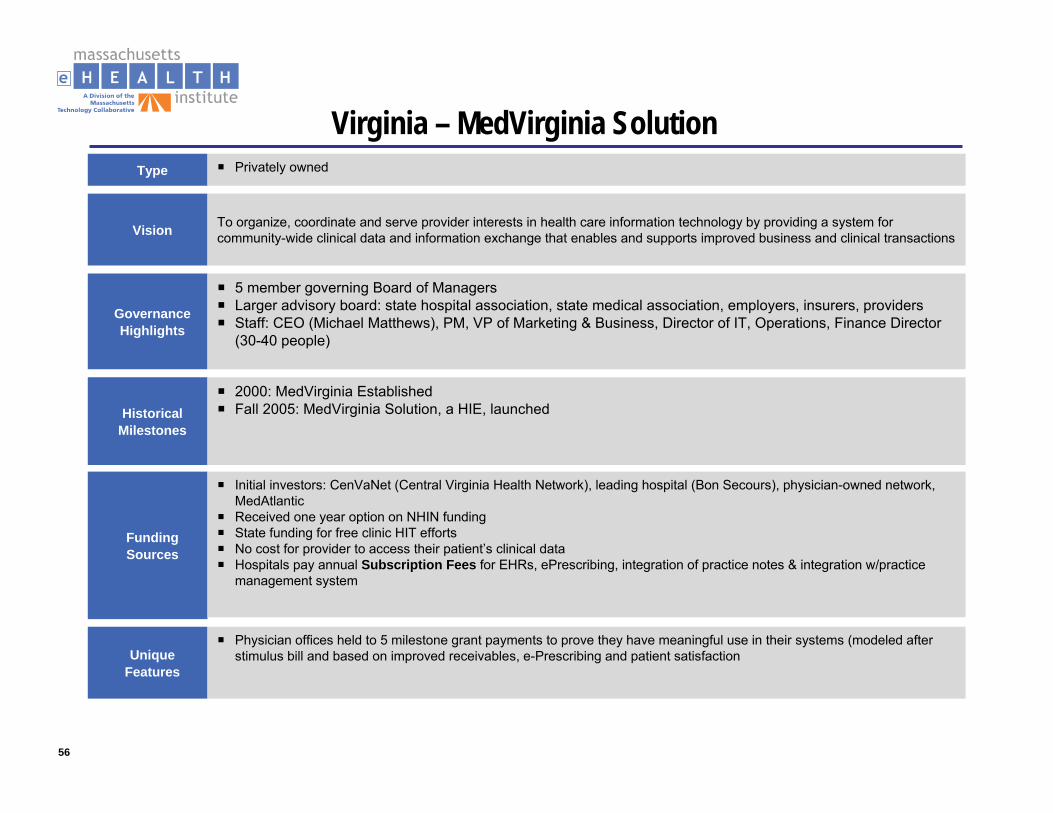
Virginia – MedVirginia SolutionType Privately owned
Governance Highlights
5 member governing Board of ManagersLarger advisory board: state hospital association, state medical association, employers, insurers, providersStaff: CEO (Michael Matthews), PM, VP of Marketing & Business, Director of IT, Operations, Finance Director (30-40 people)
Historical Milestones
2000: MedVirginia EstablishedFall 2005: MedVirginia Solution, a HIE, launched
FundingSources
Initial investors: CenVaNet (Central Virginia Health Network), leading hospital (Bon Secours), physician-owned network, MedAtlanticReceived one year option on NHIN fundingState funding for free clinic HIT effortsNo cost for provider to access their patient’s clinical dataHospitals pay annual Subscription Fees for EHRs, ePrescribing, integration of practice notes & integration w/practice management system
Vision To organize, coordinate and serve provider interests in health care information technology by providing a system for community-wide clinical data and information exchange that enables and supports improved business and clinical transactions
Unique Features
Physician offices held to 5 milestone grant payments to prove they have meaningful use in their systems (modeled after stimulus bill and based on improved receivables, e-Prescribing and patient satisfaction
57
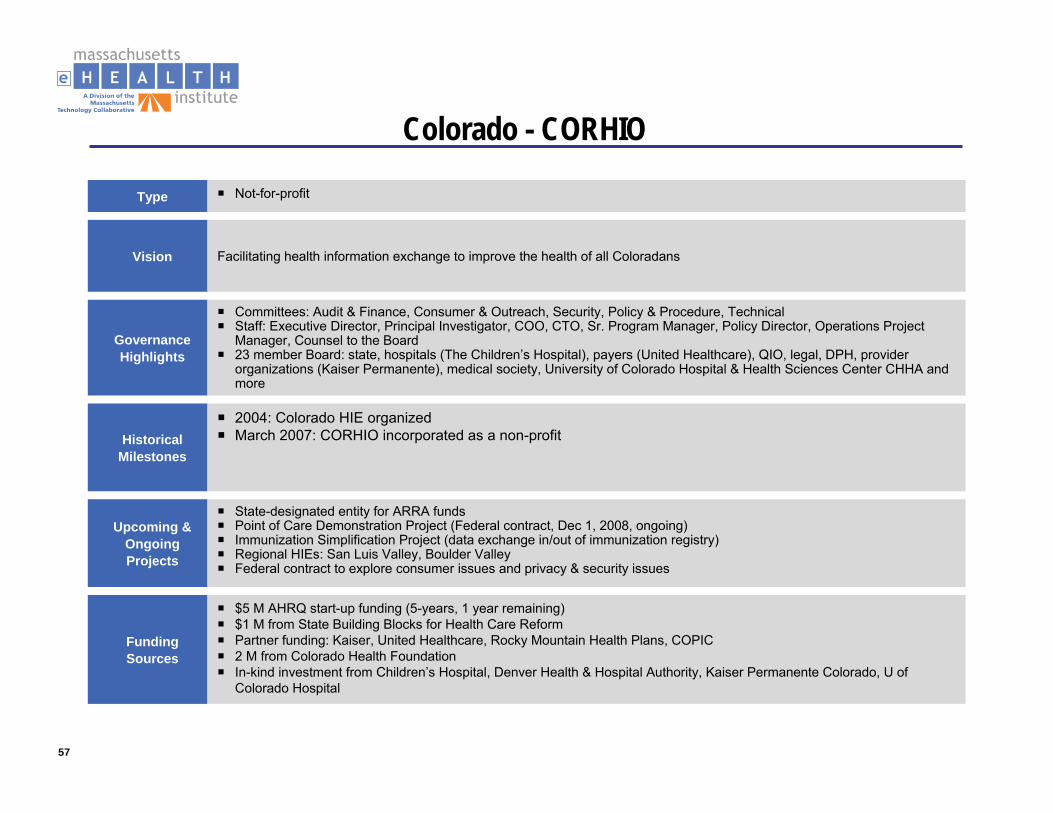
Colorado - CORHIO
Type Not-for-profit
Governance Highlights
Committees: Audit & Finance, Consumer & Outreach, Security, Policy & Procedure, TechnicalStaff: Executive Director, Principal Investigator, COO, CTO, Sr. Program Manager, Policy Director, Operations Project Manager, Counsel to the Board23 member Board: state, hospitals (The Children’s Hospital), payers (United Healthcare), QIO, legal, DPH, provider organizations (Kaiser Permanente), medical society, University of Colorado Hospital & Health Sciences Center CHHA and more
Historical Milestones
2004: Colorado HIE organizedMarch 2007: CORHIO incorporated as a non-profit
FundingSources
$5 M AHRQ start-up funding (5-years, 1 year remaining)$1 M from State Building Blocks for Health Care ReformPartner funding: Kaiser, United Healthcare, Rocky Mountain Health Plans, COPIC2 M from Colorado Health FoundationIn-kind investment from Children’s Hospital, Denver Health & Hospital Authority, Kaiser Permanente Colorado, U of Colorado Hospital
Vision Facilitating health information exchange to improve the health of all Coloradans
Upcoming & Ongoing Projects
State-designated entity for ARRA fundsPoint of Care Demonstration Project (Federal contract, Dec 1, 2008, ongoing)Immunization Simplification Project (data exchange in/out of immunization registry)Regional HIEs: San Luis Valley, Boulder ValleyFederal contract to explore consumer issues and privacy & security issues
58
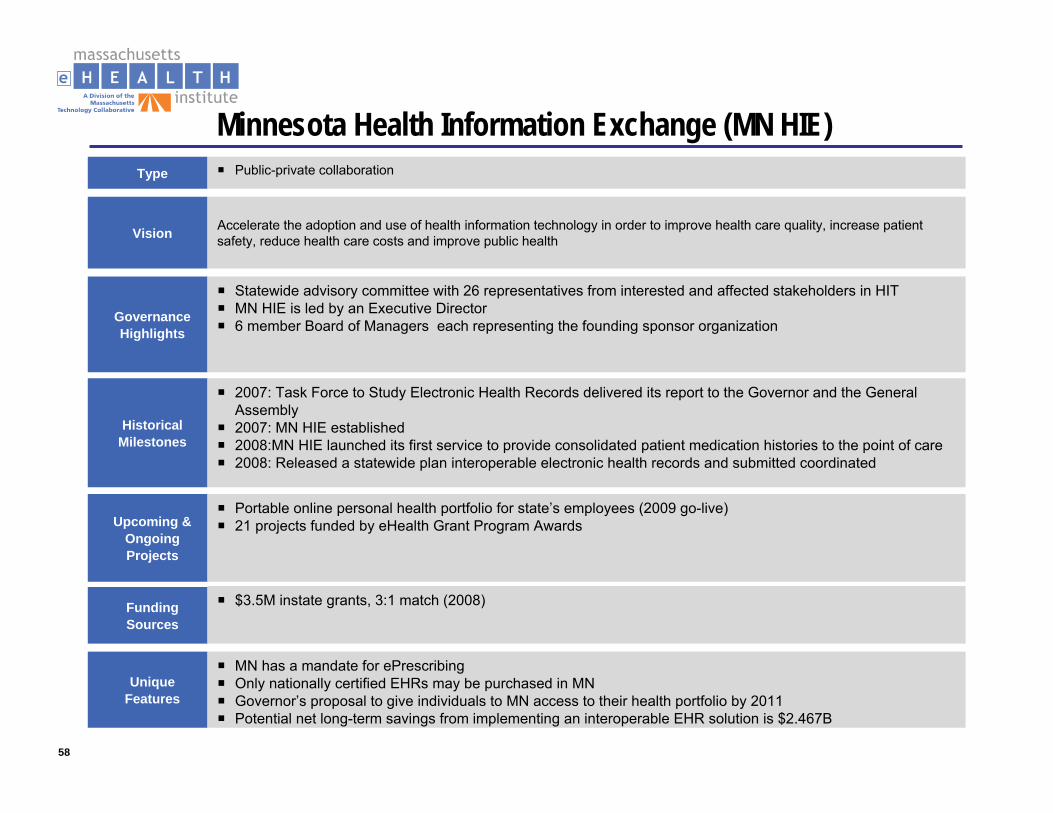
Minnesota Health Information Exchange (MN HIE)Type Public-private collaboration
Governance Highlights
Statewide advisory committee with 26 representatives from interested and affected stakeholders in HITMN HIE is led by an Executive Director 6 member Board of Managers each representing the founding sponsor organization
Historical Milestones
2007: Task Force to Study Electronic Health Records delivered its report to the Governor and the General Assembly2007: MN HIE established2008:MN HIE launched its first service to provide consolidated patient medication histories to the point of care2008: Released a statewide plan interoperable electronic health records and submitted coordinated
FundingSources
$3.5M instate grants, 3:1 match (2008)
Vision Accelerate the adoption and use of health information technology in order to improve health care quality, increase patient safety, reduce health care costs and improve public health
Upcoming & Ongoing Projects
Portable online personal health portfolio for state’s employees (2009 go-live)21 projects funded by eHealth Grant Program Awards
Unique Features
MN has a mandate for ePrescribingOnly nationally certified EHRs may be purchased in MNGovernor’s proposal to give individuals to MN access to their health portfolio by 2011Potential net long-term savings from implementing an interoperable EHR solution is $2.467B
59
Maryland - Chesapeake RegionalInformation System for our Patients (CRISP)
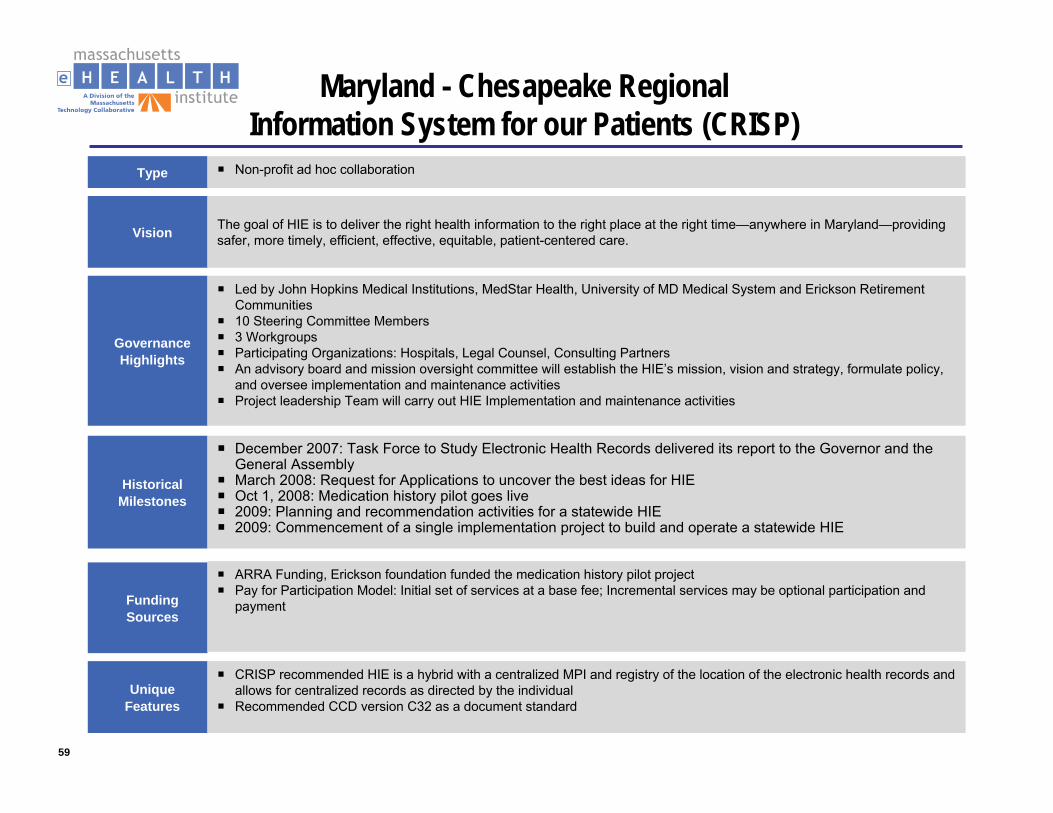
Type Non-profit ad hoc collaboration
Governance Highlights
Led by John Hopkins Medical Institutions, MedStar Health, University of MD Medical System and Erickson Retirement Communities 10 Steering Committee Members3 WorkgroupsParticipating Organizations: Hospitals, Legal Counsel, Consulting PartnersAn advisory board and mission oversight committee will establish the HIE’s mission, vision and strategy, formulate policy, and oversee implementation and maintenance activitiesProject leadership Team will carry out HIE Implementation and maintenance activities
Historical Milestones
December 2007: Task Force to Study Electronic Health Records delivered its report to the Governor and the General AssemblyMarch 2008: Request for Applications to uncover the best ideas for HIEOct 1, 2008: Medication history pilot goes live2009: Planning and recommendation activities for a statewide HIE2009: Commencement of a single implementation project to build and operate a statewide HIE
FundingSources
ARRA Funding, Erickson foundation funded the medication history pilot projectPay for Participation Model: Initial set of services at a base fee; Incremental services may be optional participation and payment
Vision The goal of HIE is to deliver the right health information to the right place at the right time—anywhere in Maryland—providing safer, more timely, efficient, effective, equitable, patient-centered care.
Unique Features
CRISP recommended HIE is a hybrid with a centralized MPI and registry of the location of the electronic health records and allows for centralized records as directed by the individual Recommended CCD version C32 as a document standard
60
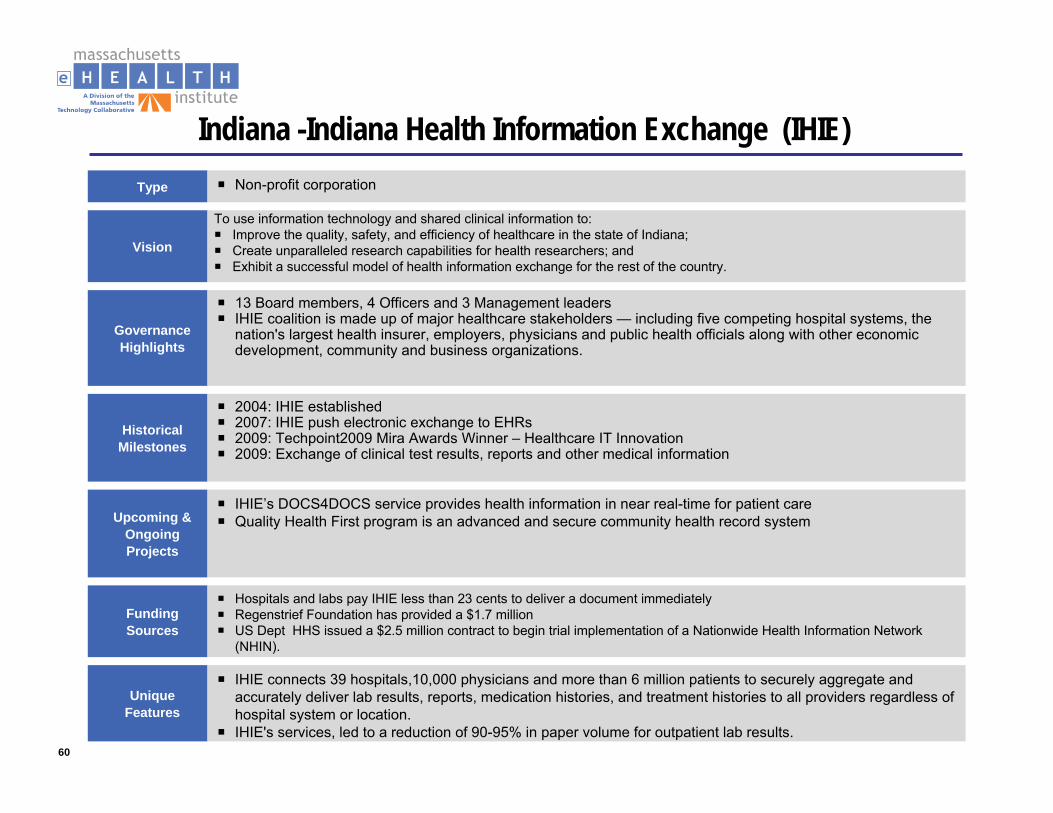
Indiana -Indiana Health Information Exchange (IHIE)Type Non-profit corporation
Governance Highlights
13 Board members, 4 Officers and 3 Management leadersIHIE coalition is made up of major healthcare stakeholders — including five competing hospital systems, the nation's largest health insurer, employers, physicians and public health officials along with other economic development, community and business organizations.
Historical Milestones
2004: IHIE established2007: IHIE push electronic exchange to EHRs2009: Techpoint2009 Mira Awards Winner – Healthcare IT Innovation2009: Exchange of clinical test results, reports and other medical information
FundingSources
Hospitals and labs pay IHIE less than 23 cents to deliver a document immediately Regenstrief Foundation has provided a $1.7 millionUS Dept HHS issued a $2.5 million contract to begin trial implementation of a Nationwide Health Information Network (NHIN).
Vision
Upcoming & Ongoing Projects
IHIE’s DOCS4DOCS service provides health information in near real-time for patient careQuality Health First program is an advanced and secure community health record system
Unique Features
IHIE connects 39 hospitals,10,000 physicians and more than 6 million patients to securely aggregate and accurately deliver lab results, reports, medication histories, and treatment histories to all providers regardless of hospital system or location.IHIE's services, led to a reduction of 90-95% in paper volume for outpatient lab results.
To use information technology and shared clinical information to:Improve the quality, safety, and efficiency of healthcare in the state of Indiana; Create unparalleled research capabilities for health researchers; and Exhibit a successful model of health information exchange for the rest of the country.
61
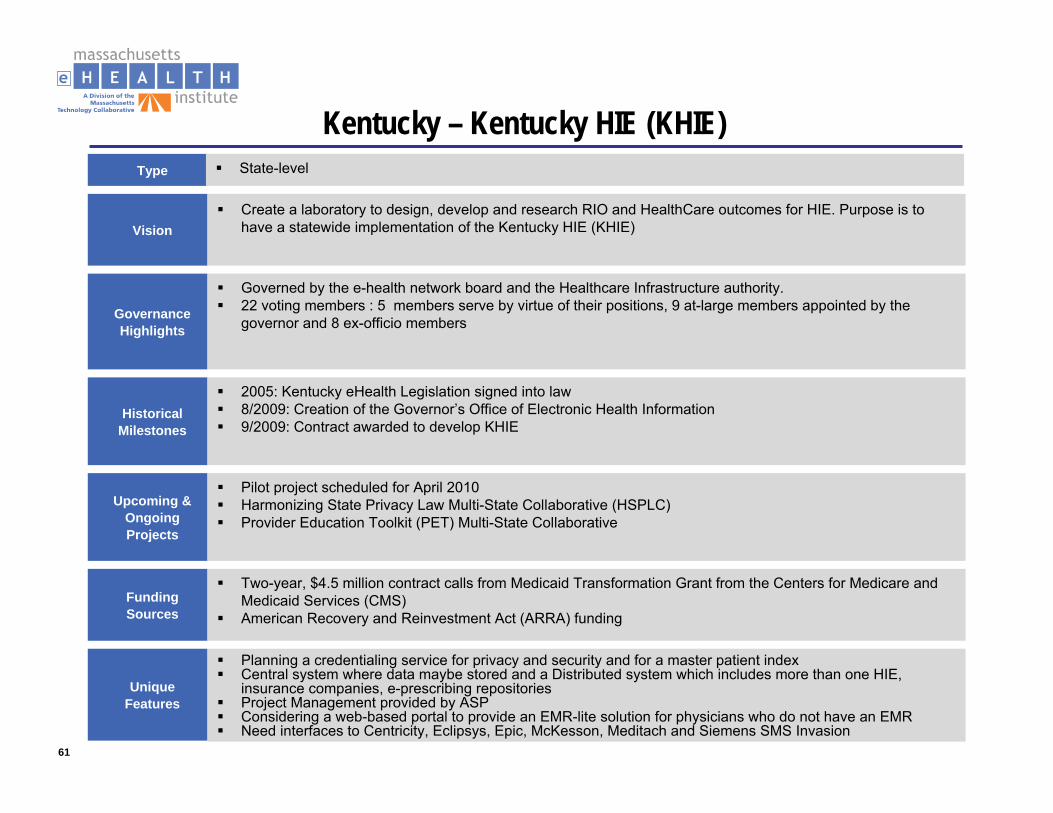
Kentucky – Kentucky HIE (KHIE)Type State-level
Governance Highlights
Governed by the e-health network board and the Healthcare Infrastructure authority.22 voting members : 5 members serve by virtue of their positions, 9 at-large members appointed by the governor and 8 ex-officio members
Historical Milestones
2005: Kentucky eHealth Legislation signed into law 8/2009: Creation of the Governor’s Office of Electronic Health Information 9/2009: Contract awarded to develop KHIE
FundingSources
Two-year, $4.5 million contract calls from Medicaid Transformation Grant from the Centers for Medicare and Medicaid Services (CMS)American Recovery and Reinvestment Act (ARRA) funding
Vision
Upcoming & Ongoing Projects
Pilot project scheduled for April 2010Harmonizing State Privacy Law Multi-State Collaborative (HSPLC)Provider Education Toolkit (PET) Multi-State Collaborative
Unique Features
Planning a credentialing service for privacy and security and for a master patient indexCentral system where data maybe stored and a Distributed system which includes more than one HIE, insurance companies, e-prescribing repositoriesProject Management provided by ASPConsidering a web-based portal to provide an EMR-lite solution for physicians who do not have an EMRNeed interfaces to Centricity, Eclipsys, Epic, McKesson, Meditach and Siemens SMS Invasion
Create a laboratory to design, develop and research RIO and HealthCare outcomes for HIE. Purpose is to have a statewide implementation of the Kentucky HIE (KHIE)
62
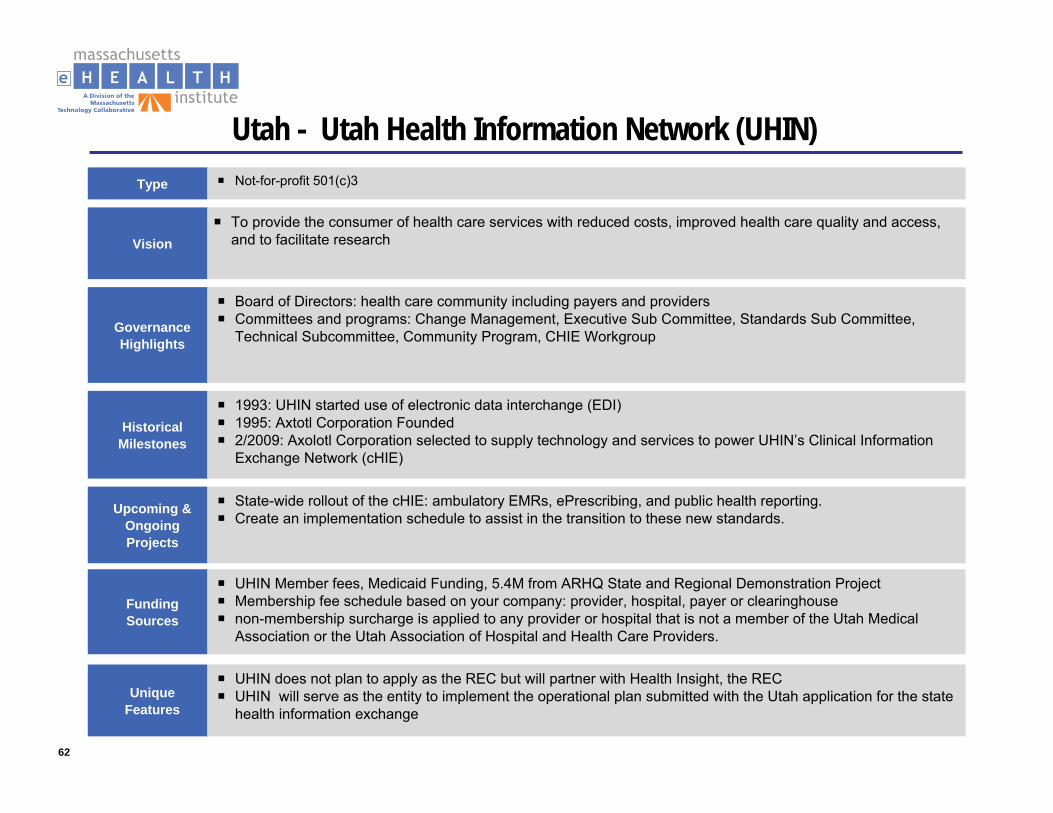
Utah - Utah Health Information Network (UHIN)Type Not-for-profit 501(c)3
Governance Highlights
Board of Directors: health care community including payers and providersCommittees and programs: Change Management, Executive Sub Committee, Standards Sub Committee, Technical Subcommittee, Community Program, CHIE Workgroup
Historical Milestones
1993: UHIN started use of electronic data interchange (EDI)1995: Axtotl Corporation Founded2/2009: Axolotl Corporation selected to supply technology and services to power UHIN’s Clinical Information Exchange Network (cHIE)
FundingSources
UHIN Member fees, Medicaid Funding, 5.4M from ARHQ State and Regional Demonstration ProjectMembership fee schedule based on your company: provider, hospital, payer or clearinghousenon-membership surcharge is applied to any provider or hospital that is not a member of the Utah Medical Association or the Utah Association of Hospital and Health Care Providers.
Vision
Upcoming & Ongoing Projects
State-wide rollout of the cHIE: ambulatory EMRs, ePrescribing, and public health reporting.Create an implementation schedule to assist in the transition to these new standards.
Unique Features
UHIN does not plan to apply as the REC but will partner with Health Insight, the RECUHIN will serve as the entity to implement the operational plan submitted with the Utah application for the state health information exchange
To provide the consumer of health care services with reduced costs, improved health care quality and access, and to facilitate research
63
Nebraska – Nebraska Health Information Initiative (NeHII)Type Approved Articles of Incorporation and Bylaws - NeHII, Inc, Application for 501(c)(3) status,
Governance Highlights
22 Board of Directors: 4 Officers - President, Vice President, Secretary and Treasurer, 11 Elected Directors, 4 Appointed Directors, 1 Legal Counsel and 2 Project Advisors
Historical Milestones
2005: NHII Initiative began2005-2008: Strategic planning, Issued RFI and RFP, Axolotl, Inc selected as the HIE partner7/2009: Successful completion of NeHII Pilot project8/2009: Statewide HIE rollout
FundingSources
USDA Distance Learning and Telemedicine (DLT) grant , AHRQ HIT grants, FCC funding for rural health networks, NLM Knowledge Management and Applied Information Grants, federal Health Resources and Services Administration grant ($1.6 Million), HRSA telehealth/telemedicine projects ,$ 200,000 to $500,000 from the Robert Wood Johnson Foundation Local Funding Partnerships (LFP)
Vision
Upcoming & Ongoing Projects
Include interfacing with Medicaid's information systems, personal health and chronic disease platformsAdded applications to provide the necessary clinical analytics and decision support tools to enhance quality, patient safety, as well as "meaningful use"
Unique Features
Patients can opt out of the initiative but cannot exclude exchange of certain records or prevent access by specific providers or insurersNeHII, IncState Designated Entity (SED) for Health Information Exchange
To be a leader in the secure exchange of health information enabling a healthier Nebraska.The mission of the NeHII Collaborative is to provide Nebraska a system for the secure exchange and use of health information.
64
North Carolina - North Carolina Healthcare Information & Communications Alliance, Inc. (NCHICA)
Type Non-profit 501(c) 3 organization
Governance Highlights
32 Board of Directors8 Board Officers
Historical Milestones
4/1994: NCHICA Chartered as a non-profit6/1999: NCHICA HIPAA Implementation Planning Task Force established 10/2002: NCHICA receives WEDI SNIP Regional Achievement Award 09/2007 -2009: Awarded NHIN Trial Implementation contract
FundingSources
Health & Wellness Trust FundFederal ($1.5 million)Membership fees and in-kind supportPrivate Sector—Industry/Large employers
Vision
Upcoming & Ongoing Projects
NC CACHI grassroots initiative to explore ideas and issues surrounding health information, such as privacy and electronic health records.Planning, establishing standards and advocating for the creation of health information exchange for North Carolina that connects with the Nationwide Health Information Network (NHIN)
Unique Features
Long-standing relationship and credibility among health care stakeholders across the StateSignificant involvement of large employersONC contract awardee for NHIN PrototypeEstablishment of Consumer Council
Dedicated to improving health and care in North Carolina by accelerating the adoption of information technology and enabling policies
65
Ohio – HealthBridgeType Not-for-profit organization
Governance Highlights
12 member board representing employers, health plans, hospitals, physicians and other community members
Historical Milestones
1997: HealthBridge Formed2003: Awarded the National Health Information Network to securely exchange data including summary patient records for providers and patients4/2008: Health Information Exchange between Healthbridge and CCHIE2009: Exchange of clinical test results, reports and other medical information
FundingSources
Self-sustaining, cash positive business model that does not rely on grant funding for ongoing costs.HHS funds to help create the standards and agreements necessary for secure electronic communication of health information between selected communities and states.
VisionOur mission is to improve the quality and efficiency of healthcare in our community. To do this we serve as a trusted third party working with all participating healthcare stakeholders to facilitate creation of an integrated and interoperable community healthcare system.
Upcoming & Ongoing Projects
ePrescribing initiatives Indiana Health Information Exchange sending information to HealthLINC and HealthBridge providersFull interconnectivity of clinical information flowing in both directions across all participating HIEs
Unique Features
Ambulatory order entry allows hospitals to receive lab orders from physician officesCCD records planned for in future along with community wide CDR, advanced administrative functions andadvanced pop health and research capabilitiesPlanned PHR integration
66
Tennessee – Midsouth eHealth Alliance (MSeHA)Type Not-for-profit 501(c) 3
Governance Highlights
Four board members – providers, mayor, governor, public health. Open seat for managed care organization and a seat for QIO and head of business coalitione-Health Council which provides oversight and equal representation for all HIO's in the state Operations committee in place to manage participation Nine Technical Advisors
Historical Milestones
2004: MSeHA established5/2006: Emergency Department data exchange7/2008: Rollout to 15 Emergency Department and 25 other facilities
FundingSources
Grants from ARQH ($5.1M over 5 years) State funding ($7.2M over 5 years)Evaluating a per person served model Analyzing the state health plans
Vision
Upcoming & Ongoing Projects
Unique Features
Behavioral health, substance abuse is not in the system. HIV is not considered sensitiveASP model for operational processes
Established to demonstrate: data sharing, interoperability, lessons learned and evaluation
Migration to a standalone commercial version of the softwareDevelopment of a strategy for sustaining the AllianceAnalysis of key benefits and impact of data exchange in ED and ambulatory settings Analysis of how information exchange is improving community healthcare delivery.
67
Appendix B: HIE Interoperability HIE Section of Review of Health IT
Plan Deloitte November 2009 (cont’d)
68
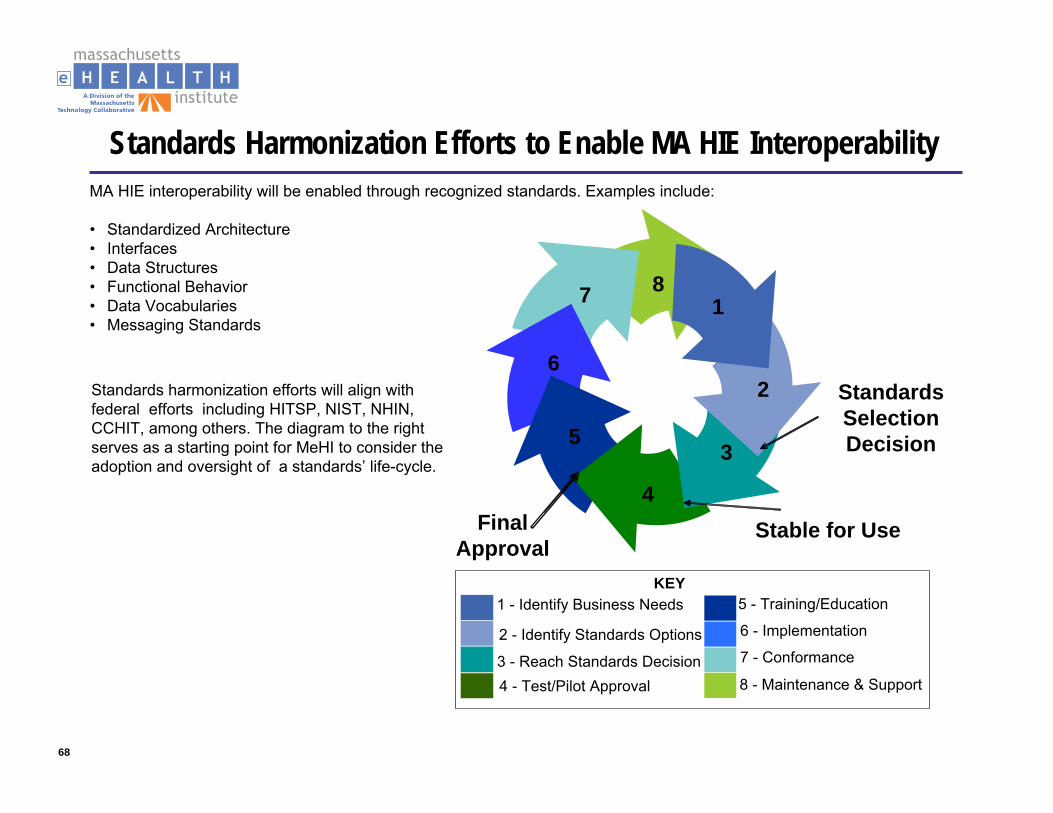
Standards Harmonization Efforts to Enable MA HIE InteroperabilityMA HIE interoperability will be enabled through recognized standards. Examples include:
• Standardized Architecture• Interfaces• Data Structures• Functional Behavior• Data Vocabularies• Messaging Standards
Standards harmonization efforts will align with federal efforts including HITSP, NIST, NHIN, CCHIT, among others. The diagram to the right serves as a starting point for MeHI to consider the adoption and oversight of a standards’ life-cycle.
Standards Selection Decision
Stable for Use
1
2
3
4
5
6
7 8
Final Approval
1 - Identify Business Needs
2 - Identify Standards Options
3 - Reach Standards Decision4 - Test/Pilot Approval
5 - Training/Education
6 - Implementation
7 - Conformance
8 - Maintenance & Support
KEY
69
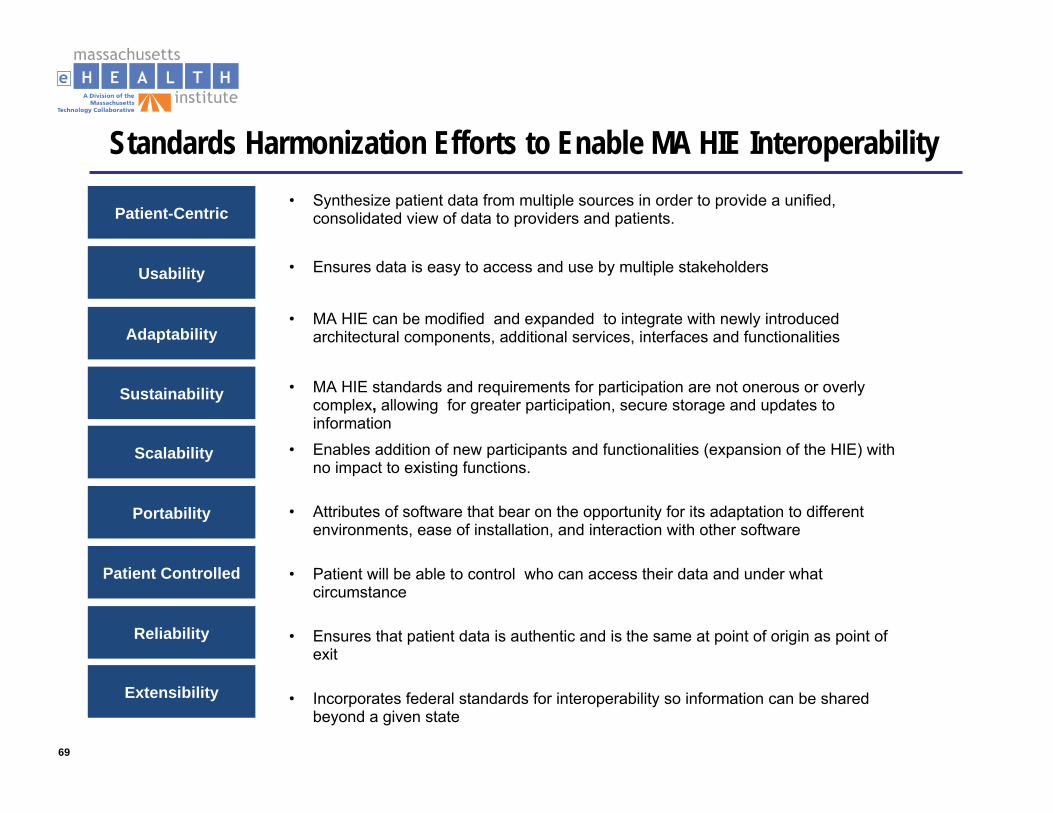
Standards Harmonization Efforts to Enable MA HIE Interoperability
Adaptability
Sustainability
Scalability
Patient-Centric
Usability
Portability
Patient Controlled
Reliability
Extensibility
• MA HIE can be modified and expanded to integrate with newly introduced architectural components, additional services, interfaces and functionalities
• MA HIE standards and requirements for participation are not onerous or overly complex, allowing for greater participation, secure storage and updates to information
• Enables addition of new participants and functionalities (expansion of the HIE) with no impact to existing functions.
• Synthesize patient data from multiple sources in order to provide a unified, consolidated view of data to providers and patients.
• Ensures data is easy to access and use by multiple stakeholders
• Attributes of software that bear on the opportunity for its adaptation to different environments, ease of installation, and interaction with other software
• Patient will be able to control who can access their data and under what circumstance
• Ensures that patient data is authentic and is the same at point of origin as point of exit
• Incorporates federal standards for interoperability so information can be shared beyond a given state
70
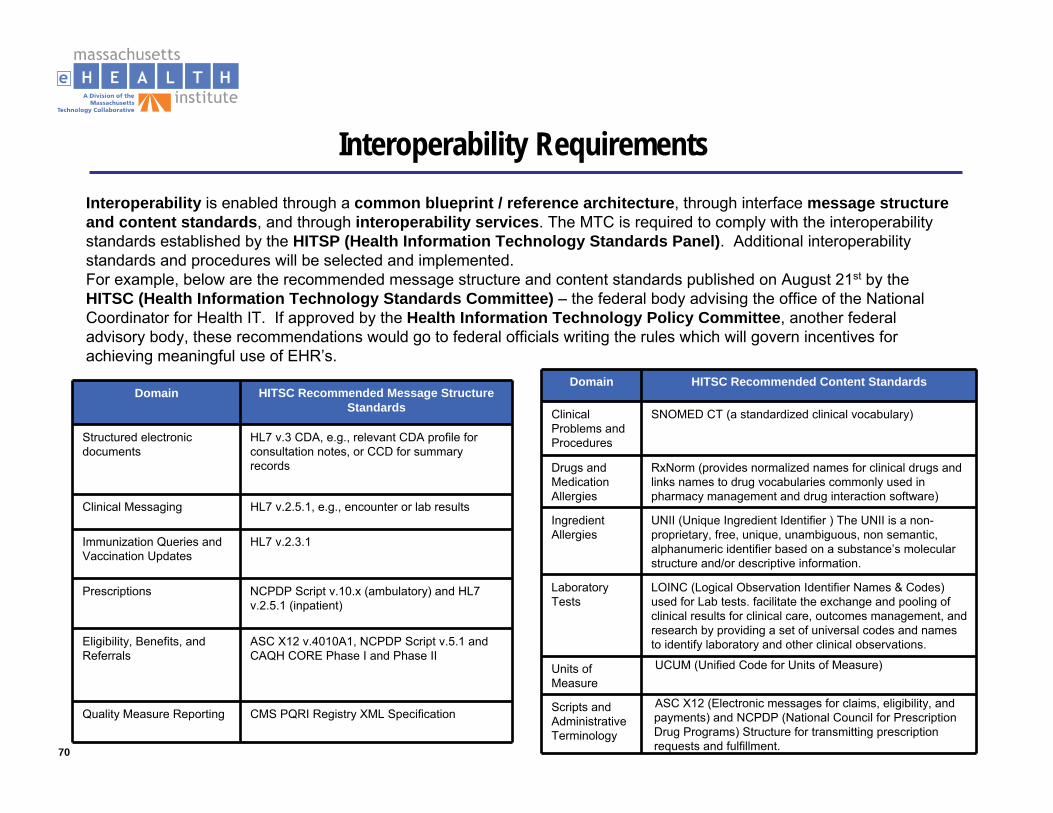
Interoperability RequirementsInteroperability is enabled through a common blueprint / reference architecture, through interface message structure and content standards, and through interoperability services. The MTC is required to comply with the interoperability standards established by the HITSP (Health Information Technology Standards Panel). Additional interoperability standards and procedures will be selected and implemented. For example, below are the recommended message structure and content standards published on August 21st by the HITSC (Health Information Technology Standards Committee) – the federal body advising the office of the National Coordinator for Health IT. If approved by the Health Information Technology Policy Committee, another federal advisory body, these recommendations would go to federal officials writing the rules which will govern incentives for achieving meaningful use of EHR’s.
Domain HITSC Recommended Content Standards
Clinical Problems and Procedures
SNOMED CT (a standardized clinical vocabulary)
Drugs and Medication Allergies
RxNorm (provides normalized names for clinical drugs and links names to drug vocabularies commonly used in pharmacy management and drug interaction software)
Ingredient Allergies
UNII (Unique Ingredient Identifier ) The UNII is a non-proprietary, free, unique, unambiguous, non semantic, alphanumeric identifier based on a substance’s molecular structure and/or descriptive information.
Laboratory Tests
LOINC (Logical Observation Identifier Names & Codes) used for Lab tests. facilitate the exchange and pooling of clinical results for clinical care, outcomes management, and research by providing a set of universal codes and names to identify laboratory and other clinical observations.
Units of Measure
UCUM (Unified Code for Units of Measure)
Scripts and Administrative Terminology
ASC X12 (Electronic messages for claims, eligibility, and payments) and NCPDP (National Council for Prescription Drug Programs) Structure for transmitting prescription requests and fulfillment.
Domain HITSC Recommended Message Structure Standards
Structured electronic documents
HL7 v.3 CDA, e.g., relevant CDA profile for consultation notes, or CCD for summary records
Clinical Messaging HL7 v.2.5.1, e.g., encounter or lab results
Immunization Queries and Vaccination Updates
HL7 v.2.3.1
Prescriptions NCPDP Script v.10.x (ambulatory) and HL7 v.2.5.1 (inpatient)
Eligibility, Benefits, and Referrals
ASC X12 v.4010A1, NCPDP Script v.5.1 andCAQH CORE Phase I and Phase II
Quality Measure Reporting CMS PQRI Registry XML Specification
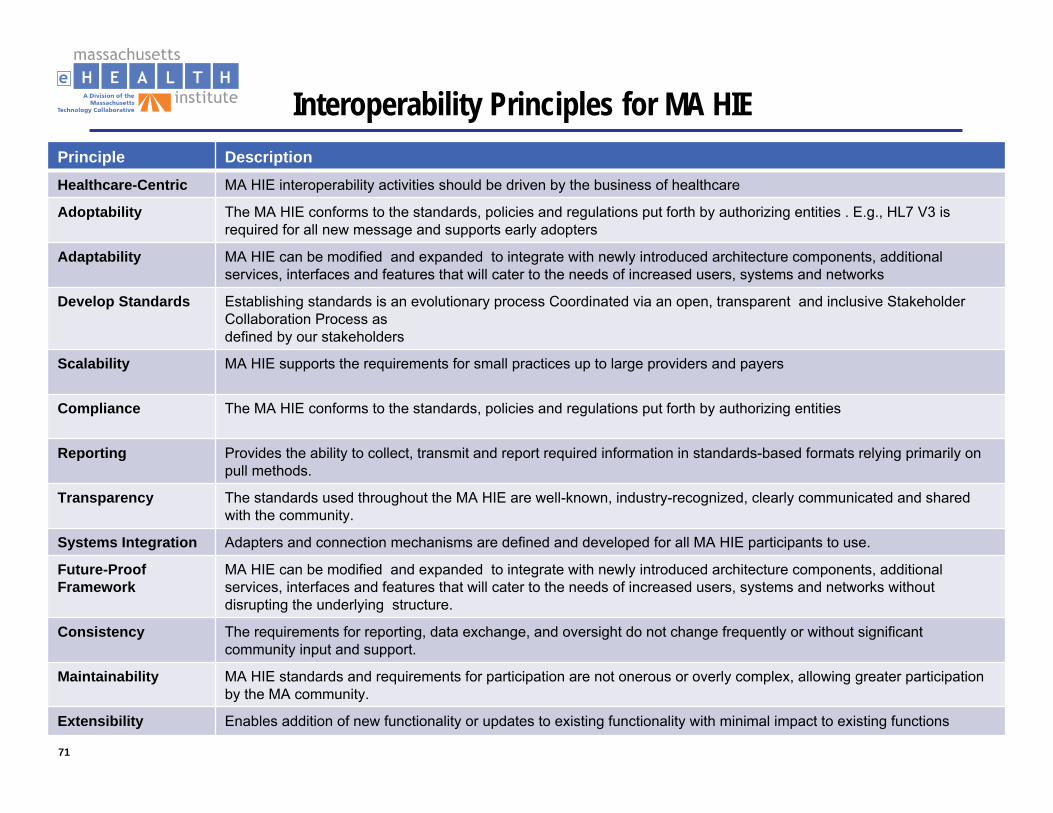
71
Interoperability Principles for MA HIEPrinciple DescriptionHealthcare-Centric MA HIE interoperability activities should be driven by the business of healthcare
Adoptability The MA HIE conforms to the standards, policies and regulations put forth by authorizing entities . E.g., HL7 V3 is required for all new message and supports early adopters
Adaptability MA HIE can be modified and expanded to integrate with newly introduced architecture components, additional services, interfaces and features that will cater to the needs of increased users, systems and networks
Develop Standards Establishing standards is an evolutionary process Coordinated via an open, transparent and inclusive Stakeholder Collaboration Process asdefined by our stakeholders
Scalability MA HIE supports the requirements for small practices up to large providers and payers
Compliance The MA HIE conforms to the standards, policies and regulations put forth by authorizing entities
Reporting Provides the ability to collect, transmit and report required information in standards-based formats relying primarily on pull methods.
Transparency The standards used throughout the MA HIE are well-known, industry-recognized, clearly communicated and shared with the community.
Systems Integration Adapters and connection mechanisms are defined and developed for all MA HIE participants to use.
Future-Proof Framework
MA HIE can be modified and expanded to integrate with newly introduced architecture components, additional services, interfaces and features that will cater to the needs of increased users, systems and networks without disrupting the underlying structure.
Consistency The requirements for reporting, data exchange, and oversight do not change frequently or without significant community input and support.
Maintainability MA HIE standards and requirements for participation are not onerous or overly complex, allowing greater participation by the MA community.
Extensibility Enables addition of new functionality or updates to existing functionality with minimal impact to existing functions
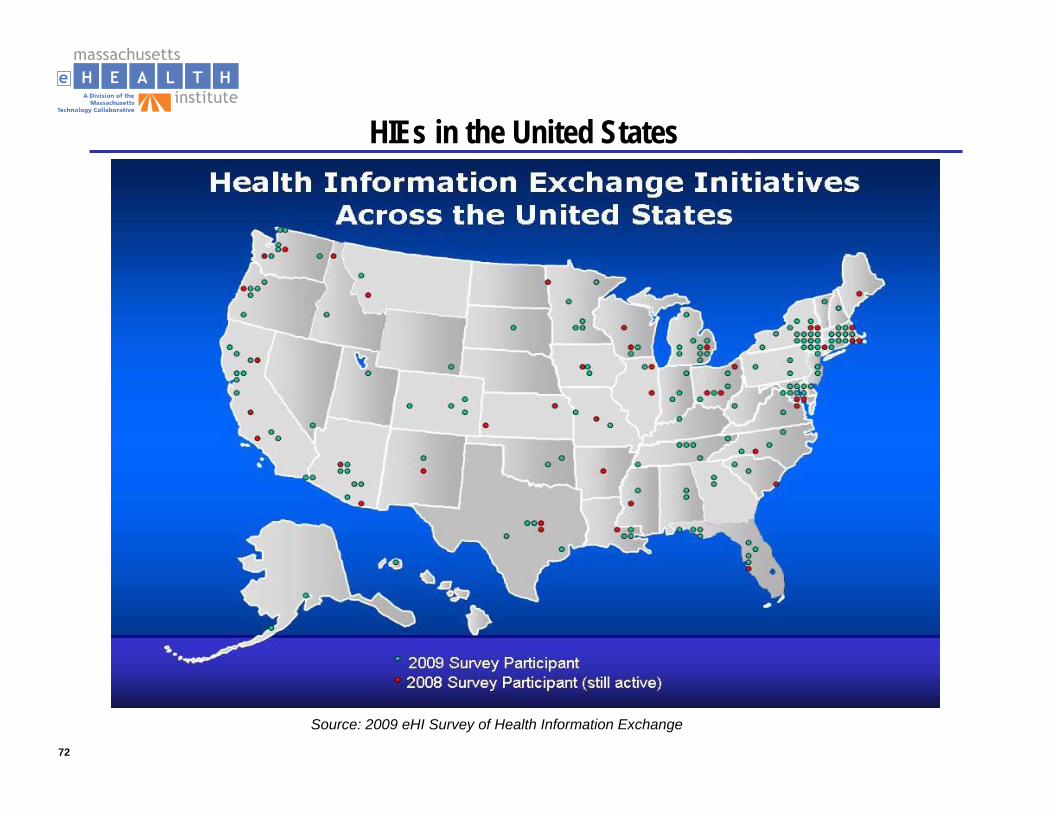
72
HIEs in the United States
Source: 2009 eHI Survey of Health Information Exchange
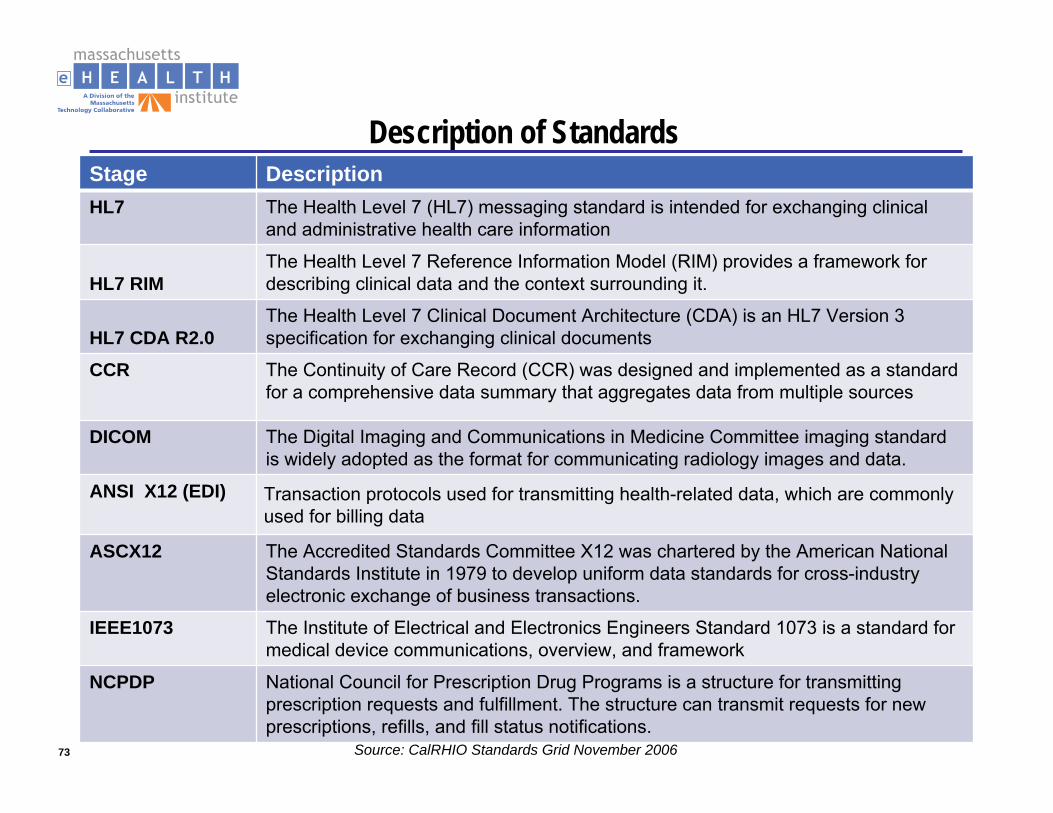
73
Description of StandardsStage DescriptionHL7 The Health Level 7 (HL7) messaging standard is intended for exchanging clinical
and administrative health care information
HL7 RIM The Health Level 7 Reference Information Model (RIM) provides a framework for describing clinical data and the context surrounding it.
HL7 CDA R2.0The Health Level 7 Clinical Document Architecture (CDA) is an HL7 Version 3 specification for exchanging clinical documents
CCR The Continuity of Care Record (CCR) was designed and implemented as a standard for a comprehensive data summary that aggregates data from multiple sources
DICOM The Digital Imaging and Communications in Medicine Committee imaging standard is widely adopted as the format for communicating radiology images and data.
ANSI X12 (EDI) Transaction protocols used for transmitting health-related data, which are commonly used for billing data
ASCX12 The Accredited Standards Committee X12 was chartered by the American National Standards Institute in 1979 to develop uniform data standards for cross-industry electronic exchange of business transactions.
IEEE1073 The Institute of Electrical and Electronics Engineers Standard 1073 is a standard for medical device communications, overview, and framework
NCPDP National Council for Prescription Drug Programs is a structure for transmitting prescription requests and fulfillment. The structure can transmit requests for new prescriptions, refills, and fill status notifications.
Source: CalRHIO Standards Grid November 2006
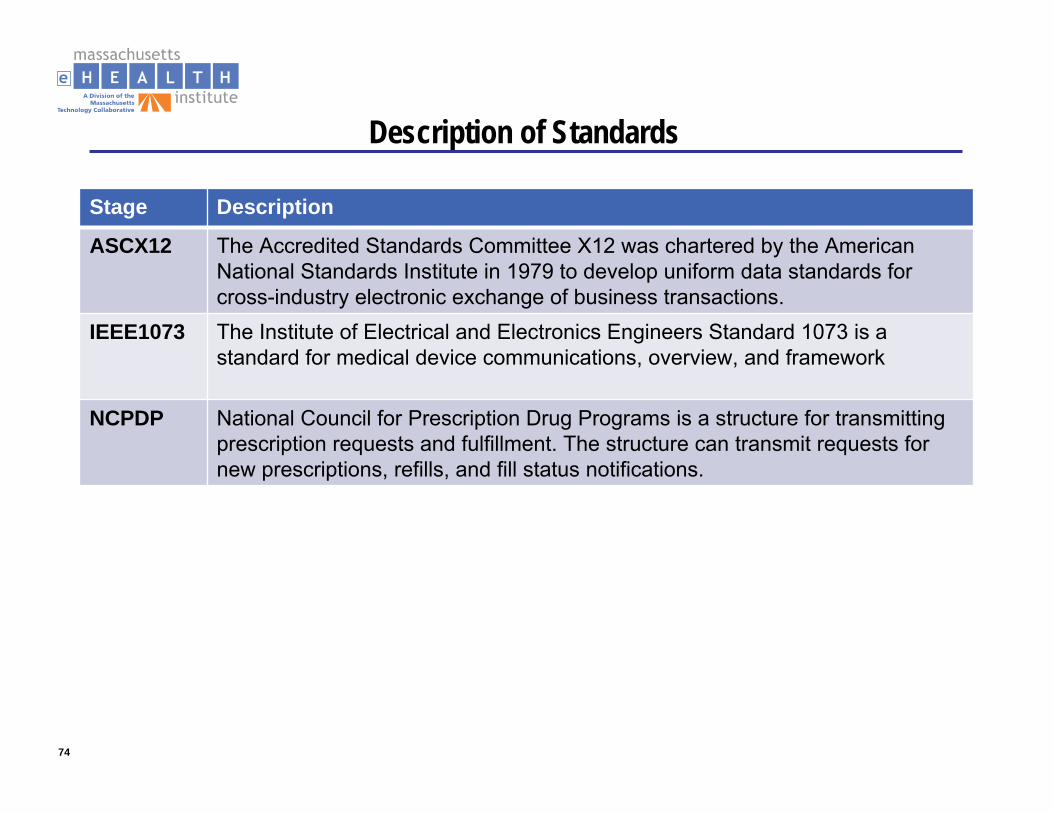
74
Description of Standards
Stage Description
ASCX12 The Accredited Standards Committee X12 was chartered by the American National Standards Institute in 1979 to develop uniform data standards for cross-industry electronic exchange of business transactions.
IEEE1073 The Institute of Electrical and Electronics Engineers Standard 1073 is a standard for medical device communications, overview, and framework
NCPDP National Council for Prescription Drug Programs is a structure for transmitting prescription requests and fulfillment. The structure can transmit requests for new prescriptions, refills, and fill status notifications.
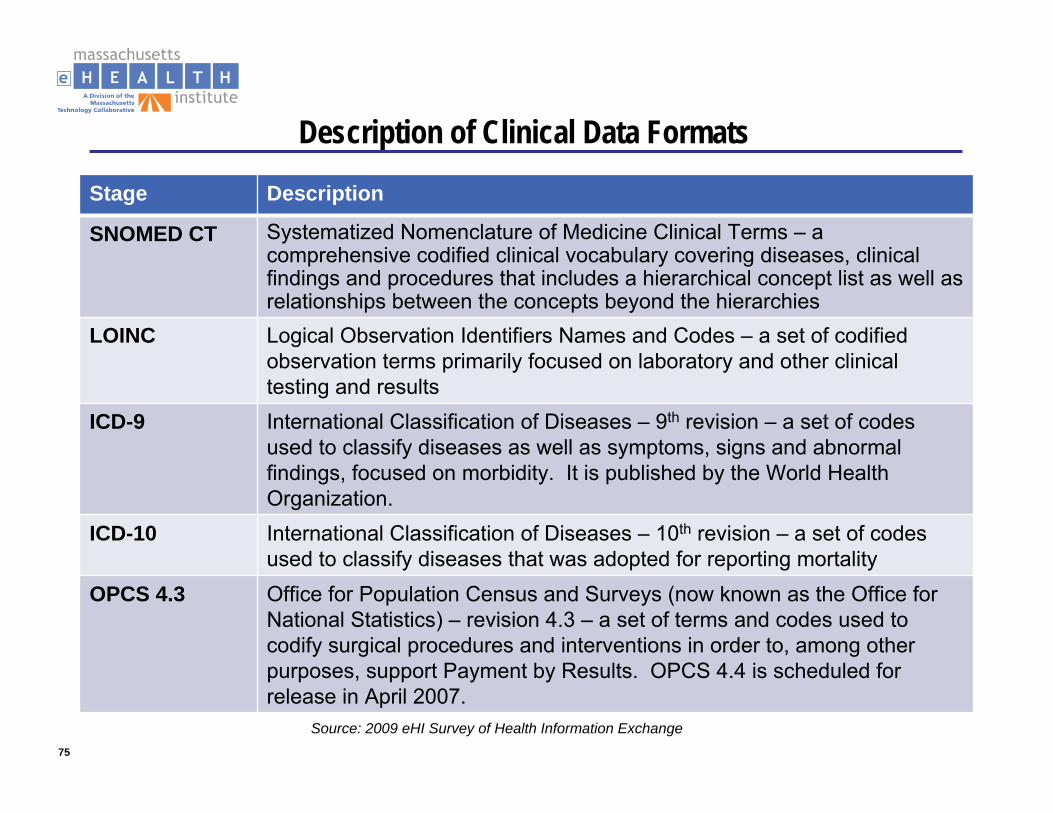
75
Description of Clinical Data Formats
Stage Description
SNOMED CT Systematized Nomenclature of Medicine Clinical Terms – a comprehensive codified clinical vocabulary covering diseases, clinical findings and procedures that includes a hierarchical concept list as well as relationships between the concepts beyond the hierarchies
LOINC Logical Observation Identifiers Names and Codes – a set of codified observation terms primarily focused on laboratory and other clinical testing and results
ICD-9 International Classification of Diseases – 9th revision – a set of codes used to classify diseases as well as symptoms, signs and abnormal findings, focused on morbidity. It is published by the World Health Organization.
ICD-10 International Classification of Diseases – 10th revision – a set of codes used to classify diseases that was adopted for reporting mortality
OPCS 4.3 Office for Population Census and Surveys (now known as the Office for National Statistics) – revision 4.3 – a set of terms and codes used to codify surgical procedures and interventions in order to, among other purposes, support Payment by Results. OPCS 4.4 is scheduled forrelease in April 2007.
Source: 2009 eHI Survey of Health Information Exchange
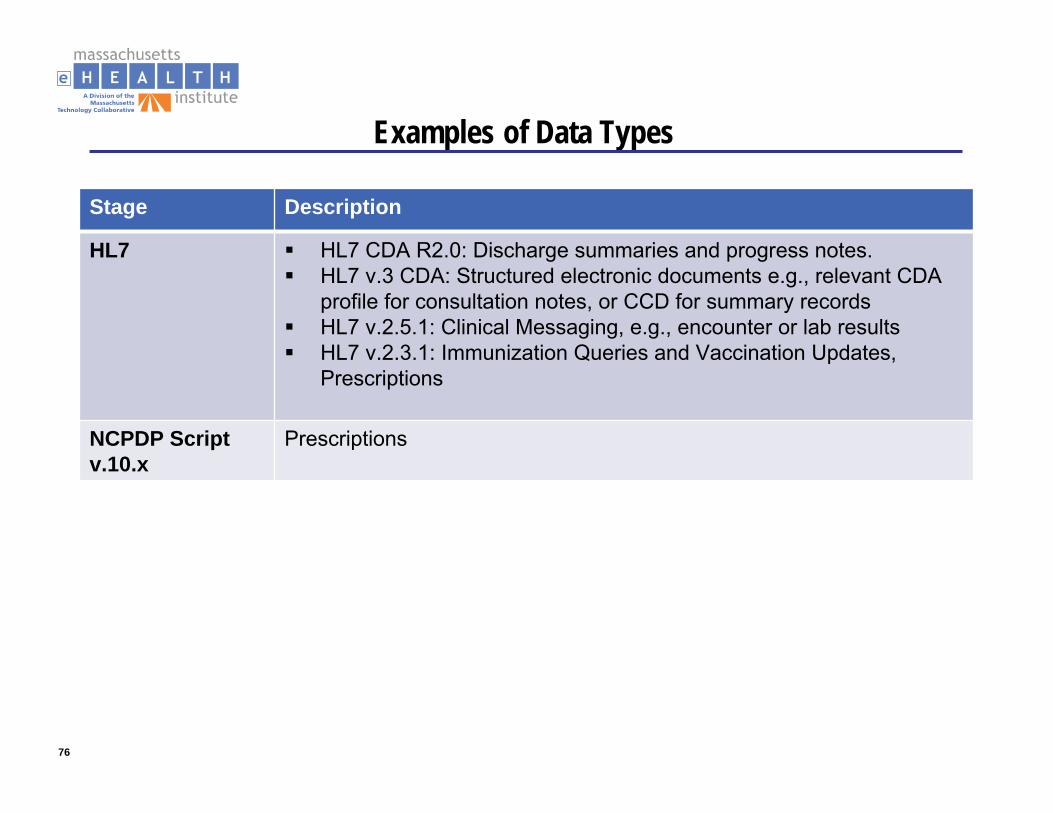
76
Examples of Data Types
Stage Description
HL7 HL7 CDA R2.0: Discharge summaries and progress notes.HL7 v.3 CDA: Structured electronic documents e.g., relevant CDA profile for consultation notes, or CCD for summary recordsHL7 v.2.5.1: Clinical Messaging, e.g., encounter or lab resultsHL7 v.2.3.1: Immunization Queries and Vaccination Updates, Prescriptions
NCPDP Script v.10.x
Prescriptions
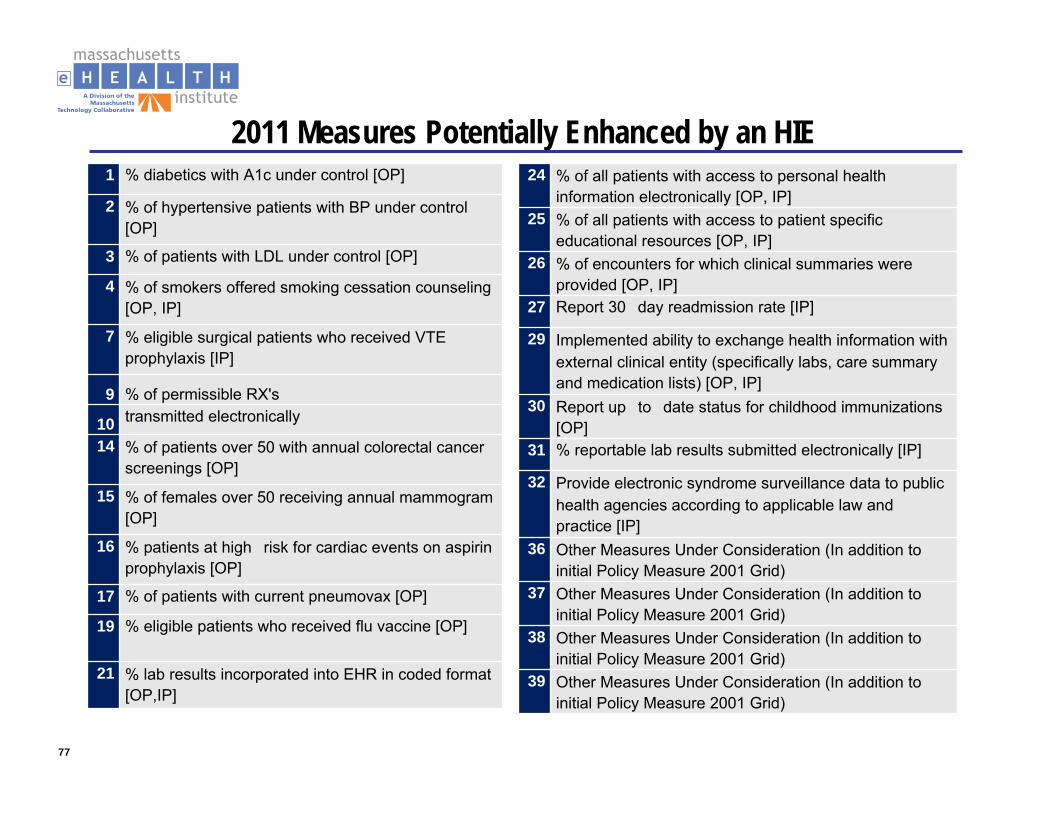
77
2011 Measures Potentially Enhanced by an HIE1 % diabetics with A1c under control [OP]
2 % of hypertensive patients with BP under control [OP]
3 % of patients with LDL under control [OP]
4 % of smokers offered smoking cessation counseling [OP, IP]
7 % eligible surgical patients who received VTE prophylaxis [IP]
9 % of permissible RX's
10 transmitted electronically
14 % of patients over 50 with annual colorectal cancer screenings [OP]
15 % of females over 50 receiving annual mammogram [OP]
16 % patients at high�risk for cardiac events on aspirin prophylaxis [OP]
17 % of patients with current pneumovax [OP]
19 % eligible patients who received flu vaccine [OP]
21 % lab results incorporated into EHR in coded format [OP,IP]
24 % of all patients with access to personal health information electronically [OP, IP]
25 % of all patients with access to patient specific educational resources [OP, IP]
26 % of encounters for which clinical summaries were provided [OP, IP]
27 Report 30�day readmission rate [IP]
29 Implemented ability to exchange health information with external clinical entity (specifically labs, care summary and medication lists) [OP, IP]
30 Report up�to�date status for childhood immunizations [OP]
31 % reportable lab results submitted electronically [IP]
32 Provide electronic syndrome surveillance data to public health agencies according to applicable law and practice [IP]
36 Other Measures Under Consideration (In addition to initial Policy Measure 2001 Grid)
37 Other Measures Under Consideration (In addition to initial Policy Measure 2001 Grid)
38 Other Measures Under Consideration (In addition to initial Policy Measure 2001 Grid)
39 Other Measures Under Consideration (In addition to initial Policy Measure 2001 Grid)
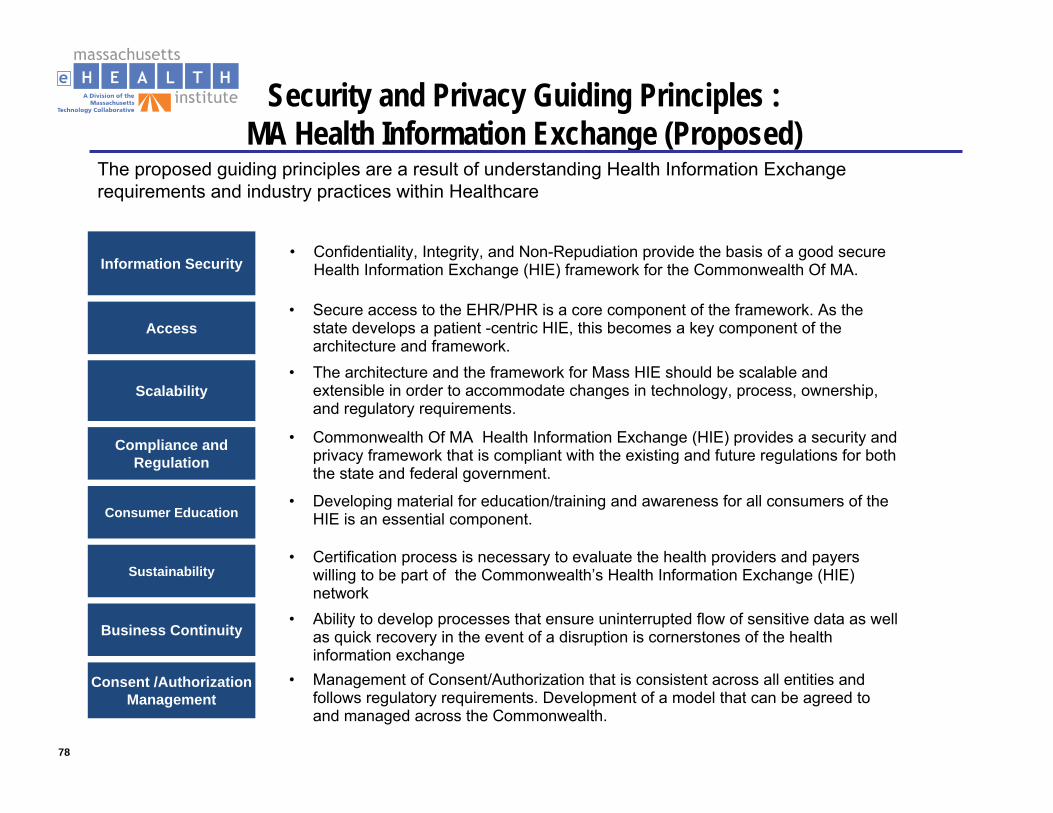
78
Security and Privacy Guiding Principles : MA Health Information Exchange (Proposed)
The proposed guiding principles are a result of understanding Health Information Exchange requirements and industry practices within Healthcare
Scalability• The architecture and the framework for Mass HIE should be scalable and
extensible in order to accommodate changes in technology, process, ownership, and regulatory requirements.
Compliance and Regulation
• Commonwealth Of MA Health Information Exchange (HIE) provides a security and privacy framework that is compliant with the existing and future regulations for both the state and federal government.
• Developing material for education/training and awareness for all consumers of the HIE is an essential component. Consumer Education
• Certification process is necessary to evaluate the health providers and payers willing to be part of the Commonwealth’s Health Information Exchange (HIE) network
Sustainability
Business Continuity• Ability to develop processes that ensure uninterrupted flow of sensitive data as well
as quick recovery in the event of a disruption is cornerstones of the health information exchange
• Confidentiality, Integrity, and Non-Repudiation provide the basis of a good secure Health Information Exchange (HIE) framework for the Commonwealth Of MA.Information Security
Access• Secure access to the EHR/PHR is a core component of the framework. As the
state develops a patient -centric HIE, this becomes a key component of the architecture and framework.
Consent /Authorization Management
• Management of Consent/Authorization that is consistent across all entities and follows regulatory requirements. Development of a model that can be agreed to and managed across the Commonwealth.
79
Nationwide Privacy & Security Framework for Electronic Exchange of Individually Identifiable Health Information - Principles
MeHI will leverage the existing Nationwide Privacy & Security Framework, including the following principles:
INDIVIDUAL ACCESSIndividuals should be provided with a simple and timely means to access and obtain their individually identifiable health information in a readable form and format
CORRECTION Individuals should be provided with a timely means to dispute the accuracy or integrity of their individually identifiable health information, and to have erroneous information corrected or to have a dispute documented if their requests are denied
OPENNESS AND TRANSPARENCY There should be openness and transparency about policies, procedures, and technologies that directly affect individuals and/or their individually identifiable health information
INDIVIDUAL CHOICE Individuals should be provided a reasonable opportunity and capability to make informed decisions about the collection, use, anddisclosure of their individually identifiable health information
COLLECTION, USE, AND DISCLOSURE LIMITATION Individually identifiable health information should be collected, used, and/or disclosed only to the extent necessary to accomplish a specified purpose(s) and never to discriminate inappropriately
DATA QUALITY AND INTEGRITYPersons and entities should take reasonable steps to ensure that individually identifiable health information is complete, accurate, and up-to-date to the extent necessary for the person’s or entity’s intended purposes and has not been altered or destroyed in an unauthorized manner.
ACCOUNTABILITY These principles should be implemented, and adherence assured, through appropriate monitoring and other means and methods should be in place to report and mitigate non-adherence and breaches
Source: Nationwide Privacy and Security Framework For Electronic Exchange of Individually Identifiable Health Information, December 15, 2008, Office of the National Coordinator for Health Information Technology





























