Embed Size (px)
Citation preview

&
Organized by
The Impact of China’s Reform
HealthcareWebinar
Sponsored by
September 24, 200910 am EDT

Healthcare 101:Taking the Pulse of China’sHealthcare Reform Efforts
Ryan OngUS-China Business Council
China Business Review WebinarSeptember 24, 2009

About USCBC
• Leading organization of US companies engaged in trade & investment in China
• Founded in 1973: 35-year history• 220+ member companies• Senior-level board of directors• Offices in Washington, DC; Beijing;
Shanghai

Context: PRC HealthcareSystem Since 1979
• Deterioration of “iron rice bowl”• Result? System marked by urban/rural gaps,
high prices for consumers, and low quality:• Large number of citizens
with no health insurance• Dissatisfaction with medical
service• Chronic government
underfunding

Rounds of Healthcare Reform
• Round 1: 1992-2005• Use of market mechanisms to increase efficiency, lower cost• SARS as a turning point: by 2005, growing criticism of rising
costs, lack of coverage
• Round 2: 2006-present• Shift in direction from market to stronger government role• Formation of new Healthcare System Reform Coordinating
Group (9/2006)• Solicitation of proposals, comments from domestic,
international players

• Key documents (4/2009):• Opinions on Deepening
Healthcare Reform (State Council)
• Notice on Important Implementing Plans for Healthcare System Reform, 2009-11 (MOH)
Healthcare Reform: Framework
Source: Xinhua .

• Broadening access• Increasing insurance
coverage• Expanding health
infrastructure
• Lowering costs• Improving quality
Healthcare Reform: Goals
Source: 360.com, 9 Jun 2006 (http://embeder.360doc.com.cn/content/060906/01/7579_200181.html)

• Expand China's healthcare coverage • Improve China's national essential drug system• Build infrastructure and facilities for "grassroots
medical networks”• Promote equality in access to basic public
healthcare services• Sponsor pilot reform projects in public hospitals
“Five Pillars” ofHealthcare Reform

• Major spending package: RMB 850 billion (US $125 billion) (1/21/09)
PRC Government Spending
• Spending over next three years (2009-2011)
• Split between central (40%) and local governments (60%)
Source: Xinhua, 9 April 2009 (http://news.xinhuanet.com/politics/2009-04/09/content_11155474.htm)

Healthcare Reform: Main Players
Healthcare service delivery, public hospital reform,rural cooperatives, drug/device lists
Ministry of Health (MOH)
National Development & Reform Commission (NDRC)
Government-run healthcare insurance
Ministry of Human Resources & Social Security (MOHRSS)
Healthcare investment
Ministry of Finance (MOF)
Drug pricing, grassroots healthcare services,and personnel education
State CouncilLeading Group
For CoordinatingHealthcare Reform
Headed byVice PremierLi Keqiang

Leading Group: Other Agencies• Ministry of Education (MOE)• Ministry of Civil Affairs (MCA)• Ministry of Supervision (MOS)• State Commission Office for
Public Sector Reform• National Population & Family
Planning Commission (NPFPC)• State Council Legislative
Affairs Office (SCLAO)• State Council Development
Research Center (DRC)• China Insurance Regulatory
Commission (CIRC)
• State Food & Drug Administration (SFDA)
• State Administration of Traditional Chinese Medicine (SATCM)
• State-Owned Assets Supervision & Administration Commission (SASAC)
• All-China Federation of Trade Unions (ACFTU)
• Chinese Communist Party (CCP) Central Committee Propaganda Department

Issue #1: Essential Drugs
• State Council, MOH Implementing Opinions on Establishing the National Essential Drug System (NEDS)(8/18/09)• Timeline: 30% by end of 2009; nationwide by 2011.• Discussion of prescription/use of essential drugs• Provisions on centralized tendering/bidding, pricing and markups,
reimbursement• Also: procedures for drafting NEDL, and release of portion of
catalogue (grassroots section)

Essential Drug System:Bidding and Tendering
• Implementing Opinions on Establishing the NEDS:Requirements for provincial governments to conduct procurement for essential drugs and to draft tendering/distribution rules for other health institutions.
• MOH, SFDA, NDRC, SAIC Opinion on Continued Standardization of Centralized Procurement for Drugs by Medical Institutions (6/26/09)
• Provincial implementation plans and websites• Related: MOH Construction Guidance for Five
Grassroots Healthcare Institutions (6/26/09)

Essential Drug System:Drug Pricing
• Implementing Opinions on Establishing the NEDS:Provisions for national price-setting and provincial adjustments – based on several price factors
• NDRC pricing regulations: still awaiting plans?• Provincial plans – e.g. Guangdong pricing plans• Related: Medical Device Pricing?

Issue #2: Health Insuranceand Reimbursement
• MOHRSS Draft 2009 Workplan for Adjusting the National Reimbursement Drug List (7/31/09)• NRDL last revised in 2004• Revisions began in July; final draft by November 2009• Coordinated by leading group, with recommendations
from a 300-person expert group• CIRC opinions on private insurer participation
(6/12/09)

Issue #3: HospitalInvestment & Construction
• Framework plan: Construction of 2,000 county hospitals and 5,000 township clinics in rural areas, 2009-11.
• MOF, NDRC, MOH, MOHRSS, MCA Opinions on Improving Government Health Investment Policies (7/5/09)
• Detailed plans still coming?

Issue #4: Public Hospital Reform
• State Council Workplan for the Healthcare Reform in Five Key Areas in 2009 (7/12/09)• Hospital reform projects in twelve pilot cities
throughout China• Includes reforms to hospital management,
prescription and sales, medical records• Cities not yet announced

Conclusion
• Healthcare has many moving parts: Multiple agencies are involved, so the right target(s) depends on the mix of issues
• Many pieces still missing: Government agencies have not yet released key healthcare documents
• Other opportunities are under the radar: Areas like health IT, medical records, health personnel training have received less attention, but should be on companies’ watch lists
Market opportunities exist, but companies have to watch for opportunities and pitfalls

© InterChina ConsultingPUBLIC
USCBC Webinar On Healthcare
China’s Healthcare ReformAnd Its Implications For Multinational Healthcare Players
Presented to: Invited Audience
Prepared by: InterChina Consulting
Date: September 24, 2009

PUBLIC © InterChina Consulting
Framework Plan(To 2020) &
ImplementationPlan (2009-2011)
Leading GroupRepresentatives from
17 ministries and departments.
Consultative Bodies
10 organizations solicited to submit
proposals.
The PublicDraft plans posted on the Internet for public scrutiny
in October 2008.
CommercialPlayers
Chinese and multinational companies in medical devices, pharma etc.
Multinational StakeholdersProviding MNC access has been a backburner concern for Chinese policy makers
2

PUBLIC © InterChina Consulting
Emerging OpportunitiesShift in emphasis to grassroots means substantial upgrading and equipping
Beijing
ZhangzhouTownship Health Center
Located in Fujian, a relatively developed province, and serving a population of 150,000.
Shanghai
Fujian
Hong Kong
Poor and outdatedmedical equipment
Limited pharmacy collection/storage
No digitalization/information technology
3

PUBLIC © InterChina Consulting
High-End>1,000
first tier hospitals, other urban hospitals
Rest Of MarketRural healthcare network
and lower tiers of the urban network
Market PotentialOver Time
Strategic Rethink?• Stratified portfolio.• In-country manufacturing.• R&D for local market.• New distribution partners.• Re-organized sales team.• Acquisition of local players.
Status Quo:• High-end target.• High-end proposition.• Imported products.
Strategic ImplicationsTargeting rural healthcare providers would require a strategic rethink
4

PUBLIC © InterChina Consulting 5
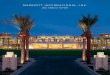
Sector By Sector: Medical DevicesNew opportunities exist in both the low-end and high-end
Pharma/ Drugs
Medical Devices
HealthcareIT
Healthcare Providers
Opportunities
• Generally good news.
• Low-End: New demand for devices generated by healthcare network build-out and upgrading.
• High-End: Public hospitals will need technologies and devices that yield higher consultation and treatment fees.
County hospitals to be
built
Township healthcenters to
be completed
‘Lead’ township healthcenters to be
renovated or expanded
Community health service stations to be built or renovated
Community healthcenters to
be built or renovated
GovernmentSubsidies
Drug Surcharges
Consultation & Treatment Fees
5%
48%
47%
Public Hospital Revenue Structure
Healthcare Network Build-Out
Low-End Opportunity
2,000
5,000
3,700
11,000
29,000
High-End Opportunity

PUBLIC © InterChina Consulting 6
Sector By Sector: PharmaceuticalsSpecific opportunities in generics and vaccines
Opportunities
• Limited new opportunities.
• Generics: High-volume demand for low-cost generics on the NEDL.
• Premium: May be an opportunity to command modest premium for quality differentiation.
Pharma/ Drugs
Medical Devices
HealthcareIT
Healthcare Providers
The National Essential Drug List
(Antibiotics Section)

PUBLIC © InterChina Consulting 7
Sector By Sector: Healthcare ITThe sophistication of the opportunities will grow over time
Opportunities
• Substantial opportunities from here on.
• Near-Term: Electronic medical records to facilitate patient data sharing.
• Mid-Term: Regional health networks.
• Long-Term: A Nationwide and unified health network.
Pilot Project: Shanghai Hospital NetworkRegional health network that facilitates exchange of imaging files and non-imaging patient data between networked parties.
Total investmentof RMB 200~300 m
in hardware, software & integration services.
Ministry Of Science and Technology
Shanghai Municipal
Government
23 HospitalsIn Shanghai
Pharma/ Drugs
Medical Devices
HealthcareIT
Healthcare Providers

PUBLIC © InterChina Consulting 8
Sector By Sector: Healthcare ProvidersBarriers remain, but could be opportunity in second & third tier urban hospitals
Opportunities
• Remains to be seen.
• Generally Vague:Diversity of ownership encouraged, but nothing said on for-profit hospitals, or barriers for foreign healthcare providers.
• Second & Third Tier Hospitals: Should the sector open, then the main opportunity could be in handling routine patient care.
• Healthcare provision remains one of the ‘restricted’ sectors in the NDRC’s ‘Catalogue For Foreign Investment’.
• Foreign ownership limited to 70%.
• Minimum investment of RMB 20 m.
• Branch organizations prohibited.
• The few foreign healthcare providers that have entered China, and have entered into joint ventures, have struggled without full control.
• Private and foreign hospitals have not been included in preferential VAT and business tax policies recently issued by the Ministry Of Finance.
Pharma/ Drugs
Medical Devices
HealthcareIT
Healthcare Providers
Barriers for MNC Healthcare Providers
1. Catalogue 2. Restrictions 3. Control 4. Tax

PUBLIC © InterChina Consulting
• Medtronic acquired 15% of Shandong Weigao, which holds around 40% of China’s osteoarticular market, in December 2008.
• The acquisition has been supplemented by a JV between the two companies, which will market Medtronic’s spinal products and Weigao’s orthopedic products in China.
• This year GE Healthcare entered into a minority 49/51 joint venture with Shinva Medical.
• The JV will focus on the development and manufacturing of low- and mid-range X-ray machines and auxiliary parts.
• The JV was conceived with China’s healthcare reform in mind, and participating in the strengthening of primary healthcare provision.
• Philips Healthcare acquired Shenzhen Goldway, China’s second largest patient monitoring player, in April 2008.
• The acquisition broadened Philips products and channels, giving Philips coverage of the low-, mid-and high-range monitoring segments in China.
• Smiths Medical acquired Zhejiang University Medical Instrument (ZDMI), the local leader in syringe pumps, in November 2008.
• This acquisition is intended to provide the platform (local production, product portfolio, distribution, R&D etc) for Smiths Medical to meet its 10-fold growth ambitions in China over the next 3 years.
Multinationals In ChinaA number are already moving to tap developing market segments
9

PUBLIC © InterChina Consulting
Profile: 18 year history
Ranking: Top 3 position in key segments
R&D: Relatively heavy investment
• Established: 1991.
• Headquarter: Shenzhen, Guangdong.
• Product Lines:• Patient Monitoring Devices.• Anesthesia Machines.• Diagnostic Lab Instruments.• Ultrasound Imaging Systems.
• Listing: NASDAQ (2006).• Acquisitions: Datascope (2008).
Revenues: Aggressive growth over past 5 years
1600
1200
800
400
2003 2004 2005 2006 20082007
6%
7%
8%
9%
10%
5%
# o
f R&
D S
taff
R&
D a
s %
of R
even
ue
USD million
2003 2004 2005 2006 2008*2007 2010E
85132
194294
548
836
59149
14594
100
313
235
425
412
InternationalDomestic
283
472
684 719
1036
1499
* Datascope acquisition increased international sales by USD160m10
Chinese Players: MindrayMindray is a Chinese medical device player on a stellar trajectory
Market Share of Selected Products in China in 2008
Brand PMD3-Part
Hematology Analyzer
200~400T/H Biochem Analyzer
B/W Ultrasound
Mindray 47% 39% 34% 32%
International Brands 36% 31% 53% 32%
Other Chinese Brands 17% 30% 13% 36
Source: Mindray Annual report, InterChina Analysis

PUBLIC © InterChina Consulting
Product Quality
Product Price
High
Low High
Philips, GE etc
Other Chinese suppliers
Mindray
Mindray is well positioned to benefit from China’s healthcare reforms.
11
Right ValueMindray’s positioning, with relatively strong products at affordable prices, is a value-for-money proposition.
Strong AccessMindray has an extensive sales and distribution network that provides access to the lower tier healthcare providers.
• 30 sales offices – 950 Sales & Service Personnel.
• 1,100 exclusive distributors.
Chinese Players: MindrayMindray has strong market access and provides the right value

PUBLIC © InterChina Consulting
Name (Simplified)
HQ Founding Year
Main Product Portfolio
Revenue(2008,USD m)
StockMarket Listing
Partnership With MNCs
Wangdong Beijing 1997 Imaging Equipment, MRI. 103 Shanghai No
Neusoft Medical Shenyang 1998 PMD, Ultrasound, CT,
MRI. 99 Shanghai JV with Philips
Shinva Zibo 1942 Diagnosis, Monitoring and Treatment Devices. 81 Shanghai JV with GE
Sinoways Yangzhou 1989PMD, Ultrasound, Biochemistry Analyzer. Pharma.
75(2007) No No
Goldway Shenzhen 1995 PMD. 18 No Acquired by Philips
Biolight Zhuhai 1993 Medical Electronics. ~8 No No
Landwind Guanghzou 1994Ultrasound, Radiology, Auto Chemistry Analyzer.
N.A. Singapore Acquired by Citigroup VC
Other Chinese PlayersMindray is just one of a number of emerging Chinese medical device players
Selection Of Chinese Medical Device Companies
12

PUBLIC © InterChina Consulting 13
A Shift Of Limelight.
A Shift Of Strategy?
Head to the countryside to serve the 500m peasants.
(China’s barefoot doctors, largely middle school students with basic training, in the 1960s).
“ ”
Key TakeawaysChina’s return to grassroot healthcare, multinationals expected to follow

InterChina Insight
Healthcare
What Do Changing Hospital Business Models
Mean For Foreign Healthcare Players?
By Benny Chen | March, 2008
InterChina Consulting 英特华投资咨询有限公司
Beijing
Shanghai
Shenzhen
Madrid
Milan
Washington DC
Management Consultants www.InterChinaConsulting.com
© 2007 InterChina Consulting All Rights Reserved

InterChina Insights
www.InterChinaConsulting.com © 2008 InterChina Consulting. All Rights Reserved
What Do Changing Hospital Business Models Mean For Foreign Healthcare Players?
March 2008
2
Having failed to make much headway during the past 20 years of reforms, the government is kicking off a campaign to improve access to affordable, quality health care. This will change the way hospitals make money, offering both opportunities and risks for foreign hospitals and healthcare investors, manufacturers and distributors of medical devices and other related groups, such as commercial insurers. “International and domestic capital will become the driving force of the next round of healthcare reform in China,” Jiang Tao, executive vice president of Hong Kong‐listed Huaxia Healthcare Holdings in Hong Kong, told a recent industry conference. With the government opening the door to both public and private investment by foreign and domestic investors, total investment per year could reach US$60 billion, Jiang said. Huaxia itself acquired a 55% interest in Chongqing Edward Hospital in May, 2007.It is in the process of acquiring a stake in Zhejiang Shuhuang Hospital, near Hangzhou, and is evaluating the possible acquisition of another 10 hospitals in China. Foreign hospitals and healthcare groups can anticipate broader opportunities among the growing populations of expatriates and affluent Chinese. Their need for better care than what has usually been available locally will boost demand for premium medical equipment, although the number of foreign‐invested hospitals will likely remain low. Demand for medium‐to‐high‐end medical devices and drugs is likely to be confined to major urban areas, underpinned by large L3 and L2 hospitals, which will generate profit from patented drugs, specialized disease treatment and value‐added services. In China’s vast rural areas, demand is driven mainly by public hospitals. There, demand and purchasing power is likely to grow most in the area of low‐end medical devices and pharmaceuticals for basic disease treatment and diagnosis, such as simple blood tests. In L1 and small community hospitals and rural health centers, the focus will be on low‐cost drugs and efficient treatment, to satisfy demand for basic medical services.
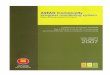
The Current Chinese Medical Care Situation China may be the world’s biggest potential healthcare market, but about half of all mainland Chinese do not go to the hospital when they get sick, according to a survey by the Ministry of Health. At the same time, systematic over‐testing, prescription of unnecessary drugs and high levels of corruption are other chronic ills requiring major reforms. The government has set a target of having 90 percent of the entire population covered by medical insurance by 2010. At present, about 54 percent of urban Chinese and 79 percent of those living in the countryside are not covered by any medical insurance. Meanwhile, basic healthcare is woefully underfunded. The Chinese government allotted only 4.8% of the country’s GDP to healthcare spending in 2006, much lower than that spent by the US, where healthcare devoured 16% percent of GDP. Beijing has cut hospital funding since the 1980s, leaving hospitals severely underfunded. Most public healthcare is by local governments, with capabilities varying largely across provinces and counties. The lack of centralized funding has shifted hospital management towards a market model. A look at the average revenue structure of Chinese public hospitals shows drug sales contributing 48% and government subsidies, 5% (this varies among different hospitals in different regions.) Some larger hospitals get significantly more subsidies from local governments, while others get none. Remaining revenues come from medical consultation and treatment fees. (See Figure 1). Government–set pricing for consultation and treatment fees are very much undervalued (‐14% margin). So hospitals are obliged to seek profits from drugs, a practice known as “Yiyao Yangyi,” or ‘feeding hospitals by drugs’. This has lead to systematic over‐testing and prescription of unnecessary expensive medicines. Strict government controls on drug prices (a maximum 15% margin for basic drugs) have prompted hospitals to raise medical services prices and broaden healthcare service dimensions. The contribution from such areas to average hospital revenues rose from 46% in 2000 to 52% in 2005.

InterChina Insights
www.InterChinaConsulting.com © 2008 InterChina Consulting. All Rights Reserved
What Do Changing Hospital Business Models Mean For Foreign Healthcare Players?
March 2008
3
China’s 9,757public hospitals are its front line for medical care. By the end of 2006, the country had only 2,000 private hospitals and 250 foreign‐invested institutions. But with average annual revenues of RMB 40 million and gross profit averaging only 4 percent, the majority of public hospitals lack resources for further development. A typical example would be a L3 hospital in Shenzhou city, Hebei province, a provincial‐level or key municipal‐level hospital with more than 500 beds. The facility has revenues of RMB 50 million, with net profit of only RMB 2.5 million. Operating on such a slim margin means the hospital cannot afford expensive medical equipment or other investments without government subsidies. Development levels vary across hospitals in different regions. Level 3 hospitals have been upgrading their equipment, while the majority of equipment used in city‐level and lower grade hospitals is vintage 1980s or earlier. This has led to residents travelling vast distances to seek medical attention in bigger facilities that are perceived to offer better care. This is true even for minor illnesses. Large hospitals are building their brand names by purchasing expensive, advanced medical equipment as a marketing tool to attract more patients. Funds are therefore often channeled to high‐profile equipment, such as CT machines, rather than to more urgently needed basic equipment that might benefit a broader range of patients. Use of increasingly sophisticated procedures such as technically advanced tests has inflated medical costs. According to a 2004 MOH survey, treatment costs rose by an average of 14% annually in 1993‐2003. The bulk of that increase was paid for by the patients themselves. In 2006, the average cost per visit for outpatients was 130 RMB, while the average cost per stay for inpatients was 4,670 RMB _ far beyond the means of most Chinese. In 2003, according to the MOH Health Yearbook, an inpatient stay cost RMB 3,910, equivalent nearly to 200% of the average income of the poorest fifth of the Chinese population. Such costs are not covered by the LIS (Labour Health Insurance Scheme), GIS (Government Health Insurance Scheme) and BMI (Basic Medical Insurance). This poses a hardship for many Chinese.
Figure 1: Average Revenue / Profit Structure of Chinese Public Hospitals and Future Direction
Source: InterChina Analysis Healthcare Reform In 2005, the Development Research Center of the State Council, the research unit of the Chinese cabinet, declared that the failure of two decades of Chinese health reforms required urgent attention. The government has clearly defined its objectives, and plans to set up four systems: the public health service system; medical services system; medical insurance system and drug supply guarantee system. The official target of ensuring medical insurance coverage for 90% of the Chinese population by 2010 is an ambitious goal. According to the National Statistics Bureau, currently only 31% of urban residents are covered by the Basic Medical Insurance (BMI), China’s main public medical insurance. Even including other types of public and commercial medical insurance, 54% of the urban population has no coverage at present. In rural areas, 79% of the population lacks any coverage. The government aims to improve access to rural medical care through co‐operative medical care systems. Rising costs, the huge population base and fast aging of the Chinese society are huge burdens. China needs to establish a very cost‐efficient healthcare infrastructure to provide disease prevention and
0
100%5%
48%
47%
12%
-14%
4%
Consultation & treatment
services
Drug
Government Subsidy
Hospital Total Revenue = 100% Hospital Profit Structure
Future Direction
• Government will increase the percentage of subsidy
• Government will break the model of ‘feeding hospitals by drugs’ and further reduce the price of basic drugs
• Increase the consultation & treatment service fee moderately to reduce loss
0
100%5%
48%
47%
12%
-14%
4%
Consultation & treatment
services
Drug
Government Subsidy
Hospital Total Revenue = 100% Hospital Profit Structure
Future Direction
• Government will increase the percentage of subsidy
• Government will break the model of ‘feeding hospitals by drugs’ and further reduce the price of basic drugs
• Increase the consultation & treatment service fee moderately to reduce loss

InterChina Insights
www.InterChinaConsulting.com © 2008 InterChina Consulting. All Rights Reserved
What Do Changing Hospital Business Models Mean For Foreign Healthcare Players?
March 2008
4
low‐cost medical services for common people. The government has to optimize resource allocation to increase overall efficiency and confine spending to reasonable levels. Achieving that aim will require adjustments in the structure of the hospital system. According to MOH statistics, about 80% of medical resources (hospital staff, beds, equipment, etc.) are concentrated in large urban hospitals. This has contributed to two chronic weaknesses in the system. The largest urban hospitals are much more crowded than smaller hospitals, with people waiting in long queues for even minor ailments. The development of many smaller hospitals that might alleviate that problem has lagged due to a lack of patients. So smaller facilities lack the financial resources to upgrade facilities and recruit good doctors. Meanwhile, chronic underfunding has left rural hospitals and clinics inadequate and outdated. To address those issues, the government plans to significantly increase funding for smaller community hospitals and implement an incentive program for patients, especially those with minor diseases, to visit smaller hospitals by providing a higher level of reimbursement for such visits. MOH data shows that central and regional governments have already invested RMB 21 billion in improving the rural healthcare system. China has set up community hospitals in 95% of its prefecture‐level cities and 86% of districts under municipalities and counties. There are now more than 3,400 community healthcare centers and nearly 12,000 community clinics. Smaller medical facilities provide basic medical care, sanitation and health prevention services to urban residents. However, the current community medical service system still falls far short of the demand generated by expanding medical insurance coverage. The next challenge will be adjusting supply and demand. To encourage patients to frequent smaller community hospitals rather than big city hospitals, the government is allowing community hospital patients to claim a higher percentage for reimbursement. In Beijing, patients going to community hospitals can get 10% higher reimbursements than those going to large hospitals. Such policies can help reallocate resources to smaller hospitals and enable them to depend less on external sources of funding for the long term. This can improve their quality of services and boost their
purchasing power for acquiring better medical equipment. Large hospitals will continue to require government subsidies as revenues fall when patients shift to community and rural health centers for treatment and diagnosis of routine ailments. At the same time, due to increasingly strict price controls for basic drugs, large hospitals will have to seek profits from patented drugs. Consultation and treatment fees will have to rise to compensate for lost revenue from drug sales. Large hospitals can create the most value‐added from specialized disease treatment and highly sophisticated surgical operations. Some large hospitals can also increase use of high value‐added services such as VIP patient rooms and one stop maternity rooms etc., targeting middle‐class and affluent patients. Large hospitals must continue to invest in advanced equipment and technology and R&D to maintain their leading position. This will allow hospitals to increase revenues from premium prices but will also boost costs and risks. From a bureaucratic perspective, to avoid excess competition between large hospitals and ensure overall efficiency, hospital management must also be reformed. In some regions like Shanghai and Wuxi, hospitals are beginning to use a group model that can help centralize drug and medical‐device purchasing power. The first wave of government spending on rural healthcare is focusing on purchasing essential medical equipment for rural hospitals. Small community hospitals and rural clinics generally have few beds and serve populations of a few thousand people or less. This business model is all about low cost, volume and efficiency. Once the government has set up the basic infrastructure, the hospitals will need to generate more revenue by treating an increasing number of patients. Most basic drugs will be sold through such facilities. With simpler diagnoses, use of low‐end medical equipment, and low‐cost treatments for routine illnesses, overall costs of public health should drop significantly. Finally, along with the above changes, China urgently needs to retrain doctors and upgrade medical teaching. The country only introduced a nationwide medical exam and licensing system in 2000. Most of China’s 1 million rural doctors, charged with caring

InterChina Insights
www.InterChinaConsulting.com © 2008 InterChina Consulting. All Rights Reserved
What Do Changing Hospital Business Models Mean For Foreign Healthcare Players?
March 2008
5
for the country's rural majority, have no formal medical education and little knowledge of Western medicines. Improving medical training is another potentially fertile area for improvement. Conclusions China will benefit from forming joint ventures with foreign hospital operators and foreign healthcare management companies to improve hospital profitability. Beijing encourages foreign investors to run hospitals, although it limits the foreign share in any such joint venture to 70% and bans WFOES. Foreign medical device and pharmaceutical companies will see greater opportunities for sales of low‐end products to rural areas, although competition is bound to be stiff. Meanwhile, demand for advanced medical equipment and technologies will also rise as the bigger urban hospitals revamp their operations. Foreign players will face serious risks if they continue to focus mainly on struggling private hospitals. Most of such facilities, 80% of which are concentrated in wealthy regions of northern, eastern and southern China, remain loss‐making despite preferential policies such as a three‐year tax holiday. The private medical sector also faces growing competition from public hospitals.
Notes: 1. Level 1 hospitals: Generally township hospitals with
<100 beds, providing medical and healthcare services to a community with population below 100,000
2. Level 3 hospitals: Provincial‐level or key municipal‐level hospitals with >500 beds, providing high‐level specialized medical and healthcare services to multiple regions
3. Level 2 hospitals: District‐level hospitals with between 100 and 500 beds, providing comprehensive medical and healthcare services to several communities.
4. LIS: A compulsory insurance. It covers employees working for state‐owned or state‐run enterprise and collective‐owned enterprise above county level.
5. GIS: It covers civil servants and other government workers
6. BMI: It is an insurance scheme established in 1998. It builds a medical insurance fund by constantly (mainly every month) and compulsorily charging premium from employees and employers. As the name suggests, it covers basic and common diseases.
Contributed by Mr. Benny Chen, Consultant, InterChina Consulting Shanghai Office
[email protected] Benny Chen, a Chinese national, is a Consultant in InterChina's Shanghai Office. InterChina regularly advises and supports clients regarding healthcare projects in China. Edited by Kazuhiko Shimizu, Shanghai‐based writer and editor.

InterChina Insights
www.InterChinaConsulting.com © 2008 InterChina Consulting. All Rights Reserved
What Do Changing Hospital Business Models Mean For Foreign Healthcare Players?
March 2008
6
InterChina Consulting Leading Consultancy: InterChina is a boutique management consultancy specialized in strategy, corporate and human resources services for companies doing business in China. Since being founded in 1994, InterChina has emerged as one of the leading consultancies in China, and half our project volume is accounted for by clients choosing to return to InterChina when new consultancy needs arise. Comprehensive Services: InterChina supports clients along the sequence of challenges faced when entering or expanding in China, and our 3 specialized consulting practices combine to provide a suite of comprehensive and complementary services:
• InterChina’s Strategy Practice assists our clients better understand and penetrate their markets in China.
• InterChina’s Corporate Practice
supports our clients establish and expand corporate structures in China.
• And InterChina’s Human
Resources Practice helps our clients recruit executives and other key positions in China.
Differentiated Approach: We deploy consulting methodologies developed in China for China. Our strategy solutions are practical, since we often support clients implement the strategies we recommend, and our corporate solutions are always oriented towards strategic objectives. We involve our clients in the consulting process, transferring understanding and receiving feedback, enabling our clients to better adapt to the Chinese environment and ensuring continuity following the project. Strong Sector Expertise: As our clients are international companies with demanding consultancy needs, InterChina has developed expertise in select sectors to further our delivery of pioneering and practical solutions. These sectors include (but are not limited to): Automotive &
Components, Machinery & Components, Food & Beverage, Chemicals, Energy & Power, Trade, Distribution & Retail, and Financial Services. Stable Consulting Team: InterChina’s Board of Partners is both Western and Chinese, and our Partners provide stability through their commitment to the company. In fact, InterChina enjoys one of the highest employee retention rates in China, and as stability is fundamental for Consulting Teams to be successful, our clients benefit directly as a result. Moreover, all our 50 plus consultants are committed and capable professionals, with a balance of experience and skills that allow InterChina to customize Project Teams to meet the needs of individual clients. Local Presence: InterChina has three operations offices in China, located in Beijing, Shanghai and Shenzhen, supported by liaison offices in Europe, located in Madrid and Milan, and North America, located in Washington D.C. For further information, please feel free to contact us at: [email protected]

InterChina Insight
Barring The Pharmacy Doors China’s Three Regulatory Barriers For Foreign Pharmaceutical Players
By Franc Kaiser | April 2009
InterChina Consulting 英特华投资咨询有限公司
Beijing
Shanghai
Shenzhen
Madrid
Milan
Washington DC
Management Consultants www.InterChinaConsulting.com
© 2009 InterChina Consulting All Rights Reserved

InterChina Insights
www.InterChinaConsulting.com © 2009 InterChina Consulting. All Rights Reserved
Barring the Pharmacy Doors China’s Three Regulatory Barriers for Foreign
Pharmaceutical Players April 2009
2
With the Chinese pharmaceutical market growing 15 percent a year as China expands its healthcare system for its 1.3 billion people (by 2020, all Chinese should be covered by a basic medical insurance), it would appear to offer abundant potential for foreign players. In the past 20 years, top American, European and Japanese drug makers have spent billions trying to crack the market. But the reality is that apart from a few big‐name multinationals, most players have made only modest advances in this market. Foreign manufacturers account for only 10% to 20% of the market, depending on the type of medicine. Even the largest
players, such as Roche of Switzerland and Bayer of Germany, earn only a small fraction of their global turnover in China. A remarkable number of foreign‐invested drug makers are active here, but most are just sourcing inexpensive raw materials (API, or Active
Pharmaceutical Ingredients) from Chinese suppliers for finishing preparations in their own plants elsewhere in the world. Given China’s huge market potential, what’s going wrong here? Why are foreign pharmaceutical makers, especially generic drug producers, not more active in China?
There are several ways to answer this question, but the main barrier to expansion by multinationals is found in China’s regulations and policies, which prevent foreign companies from applying proven business models used in Europe and the USA. After expending much effort to overcome those regulatory hurdles over the past 20 years, some multinationals have gained a foothold. But many small and medium foreign pharmaceutical companies face confusion, uncertainty and a high degree of risk in China. Basically, there are three main regulatory barriers: 1. Drug registration. 2. Prices. 3. No separation of production and marketing
licenses.
“Even the largest players earn only a small fraction of their global turnover in China.”

InterChina Insights
www.InterChinaConsulting.com © 2009 InterChina Consulting. All Rights Reserved
Barring the Pharmacy Doors China’s Three Regulatory Barriers for Foreign
Pharmaceutical Players April 2009
3
Barrier 1: Drug Registration Given the increasing demand inside China for improved, modern medicines, foreign companies that once only considered China for sourcing raw materials should take a fresh look now at whether their finished preparations will sell. For many companies, the analysis starts with a look at the regulatory environment, and unfortunately often ends there. Although regulations and policies on pharmaceutical production and imports into China are publicly available, in almost all cases they require additional interpretation to understand what they mean for a particular company. The overall authority is the SFDA (since August 2008, reporting directly to the Ministry of Health), which oversees drug registrations and clinical trial approvals. However, the SFDA provides only relatively theoretical guidelines. In reality, drug approvals and registration times are on a “case by case” basis. This leaves foreign market entrants with a great deal of uncertainty, since they often cannot predict how long it will actually take to obtain an approval, or even if a drug will be approved at all.
A foreign drug producer wanting to import finished preparations produced in other countries should plan at least 1.5 ‐ 2 years ahead to go through the application process, do bioequivalency tests, and receive approval by the SFDA. If clinical trials must be conducted in China, at least 1 additional year should be allocated for that process. China’s requirements for documentation and other‐market test results are rather ambiguous, and leave ample space for interpretation of whether additional time‐ and cost‐intensive clinical trials will be necessary again in China. The regulations also lack a concise definition of “new” drugs and “generic” drugs. However, especially for non‐innovative drug makers, it is crucial to know what the local SFDA views as “generic” and what it does not. A preliminary discussion with SFDA representatives can be a sobering experience that yields no satisfying answers. There is no choice but to embark on the byzantine registration process to find out whether or not the drug will be approved.

InterChina Insights
www.InterChinaConsulting.com © 2009 InterChina Consulting. All Rights Reserved
Barring the Pharmacy Doors China’s Three Regulatory Barriers for Foreign
Pharmaceutical Players April 2009
4
Barrier 2: Government‐Set Prices Apart from the licensing issue, pharmaceutical
makers have to contend with government price controls that can shrink their margins. The key to prescription drug pricing in China is government reimbursement lists which specify which drugs are covered by insurance. Those on the lists are the drugs that become blockbusters. Getting onto those lists is crucial for success.
The SFDA (State Food and Drug Administration), issues a State Basic Drug List, which lists all drugs related to clinical use (around 2,000 drugs). The generic formula of the drugs must be included in this list. Apart from that, the Ministry of Labor and Social Security has a State BMI (Basic Medical Insurance) and Labor Injury Insurance Drug List, which is the actual list specifying which drugs are eligible for reimbursement. The reimbursement list includes both Western‐style and TCM (Traditional Chinese Medicines) drugs, but not over‐the‐counter drugs. This is the “golden list” as most drugs (at least in value) in China are prescription drugs sold to hospitals. If a foreign drug maker sells a product whose formula is included in the list, it may gain access to a large market. The downside: The (hospital) prices are capped by the government. Drug makers need to be mindful of two basic price ceilings: First, the NDRC (National Development and Reform Commission) price ceiling, which sets retail
prices (both for hospitals and pharmacy retail chain outlet sales). Normally one finds two different prices per formula, a higher price for an innovator brand, and a lower price for a generic version. Second, the drug maker needs to get to know the provincial price adjustments for specific formulae. The bad news is that the NDRC normally calculates those price ceilings by surveying local drug manufacturers on their average production costs and margin calculations. The Chinese government is seeking to reduce prices for commonly and widely used drugs to make them more affordable for the average consumer and to discourage corruption at the hospital level. The authorities are seeking to bring prices down still further by requiring hospitals to conduct annual local or provincial‐level tenders, and provincial Ministry of Health professional committees are setting additional price limitation targets. Since last year, hospitals are only allowed to purchase two brands of any one formula, which restricts the number of suppliers. Furthermore, two to three bidding rounds naturally reduce prices as drug makers are fighting for their contracts, mostly purely based on price alone. Foreign drug makers sometimes still enjoy a bit of extra goodwill: In 2006, foreign drug makers suffered an average of only 5% price reductions, whilst domestic brands faced reductions of 20%–30%. Once a drug maker understands the prevailing retail price ceilings, it will need to calculate his own landing price (i.e. CIF if imported), working backward from the given governmental price ceiling. The lion’s share of mark‐ups for innovative drugs is normally assumed by the hospital (around 35% and more). For generics, the lion’s share of mark‐ups is taken by distributors, over 50% of the price. Generics generally travel through several tiers of distributors before reaching hospitals.
“Key to prescription drug pricing is government reimbursement lists which specify which drugs are covered by insurance.”

InterChina Insights
www.InterChinaConsulting.com © 2009 InterChina Consulting. All Rights Reserved
Barring the Pharmacy Doors China’s Three Regulatory Barriers for Foreign
Pharmaceutical Players April 2009
5

InterChina Insights
www.InterChinaConsulting.com © 2009 InterChina Consulting. All Rights Reserved
Barring the Pharmacy Doors China’s Three Regulatory Barriers for Foreign
Pharmaceutical Players April 2009
6

InterChina Insights
www.InterChinaConsulting.com © 2009 InterChina Consulting. All Rights Reserved
Barring the Pharmacy Doors China’s Three Regulatory Barriers for Foreign
Pharmaceutical Players April 2009
7
Barrier 3: Marketing Licenses Don’t Exist In China Given that the vast majority of drug sales in China are generic, it seems strange that generic giants have failed to make inroads in China. Big generic
manufacturers like Israel’s Teva, and Ranbaxy and Dr. Reddy of India often make less than 1% of their global turnover in China. The main reason for this is a regulation stipulating that companies selling locally‐made finished preparations also have to manufacture them in China. Hence, a company
needs to own a production license (which is normally granted only after the required production equipment is bought and in place) to market a drug in China. Chinese producers are allowed to make APIs for foreign brands, but not to produce finished preparations sold in China. The authorities do not distinguish between production licenses, sales licenses, marketing authorization licenses and so forth. “In‐licensing” or “contract manufacturing” for generic finished preparations is an alien concept for Chinese regulators. They tend to view making pharmaceuticals as similar to steel or car production and cannot distinguish between marketing and production. Moreover, recent quality control scandals such as the allergic reactions to heparin made from API produced in China have left Beijing nervous about separating the responsibility of drug sellers from that of the manufacturers. Foreign generic players are thus unable to source finished preparations from Chinese manufacturers and sell them under their own brand (and within their own drug portfolio) in China. So large, generic players such as Iceland’s Actavis and Ranbaxy have been more or less forced to establish their own production sites in China at considerable expense, and even after 5 years in production, have not recouped their investments. This regulatory regime means that drug makers end up creating excess production capacity to ensure
they can market a particular drug. Foreign pharmaceutical makers have begun modest efforts to lobby for change, with the European Chamber of Commerce in China putting forward a recommendation in its 2004 white paper to allow marketing licenses. But so far there has been no reaction. We see little chance that marketing licenses will be introduced in the coming three years or so, as there are no discussions within SFDA or NDRC on this topic. Instead, it is more likely that China will get stricter regarding contract manufacturing to avoid more trouble over quality issues. Given the skewed playing field that foreign drug makers face, those hoping to expand sales in China need good advisors who know the local pharmaceuticals market and can suggest the best strategy for success.
“Companies selling locally‐made finished preparations also have to manufacture them in China.”

InterChina Insights
www.InterChinaConsulting.com © 2009 InterChina Consulting. All Rights Reserved
Barring the Pharmacy Doors China’s Three Regulatory Barriers for Foreign
Pharmaceutical Players April 2009
8
Contributed by Mr. Franc Kaiser, Senior Consultant, InterChina Consulting
[email protected] Franc Kaiser, a Swiss national, is a Senior Consultant at InterChina’s Shanghai Office. He is regularly advising InterChina’s international clients regarding sales and business development in China’s health care industry. Edited by Kazuhiko Shimizu, Shanghai‐based writer and editor.

InterChina Insights
www.InterChinaConsulting.com © 2009 InterChina Consulting. All Rights Reserved
Barring the Pharmacy Doors China’s Three Regulatory Barriers for Foreign
Pharmaceutical Players April 2009
9
InterChina Consulting Leading Consultancy: InterChina is a boutique management consultancy specialized in strategy, corporate and human resources services for companies doing business in China. Since being founded in 1994, InterChina has emerged as one of the leading consultancies in China, and half our project volume is accounted for by clients choosing to return to InterChina when new consultancy needs arise. Comprehensive Services: InterChina supports clients along the sequence of challenges faced when entering or expanding in China, and our 3 specialized consulting practices combine to provide a suite of comprehensive and complementary services: • InterChina’s Strategy Practice assists our clients
better understand and penetrate their markets in China.
• InterChina’s Corporate Practice supports our
clients establish and expand corporate structures in China.
• And InterChina’s Human Resources Practice
helps our clients recruit executives and other key positions in China.
Differentiated Approach: We deploy consulting methodologies developed in China for China. Our strategy solutions are practical, since we often support clients implement the strategies we recommend, and our corporate solutions are always oriented towards strategic objectives. We involve our clients in the consulting process, transferring understanding and receiving feedback, enabling our clients to better adapt to the Chinese environment and ensuring continuity following the project. Strong Sector Expertise: As our clients are international companies with demanding consultancy needs, InterChina has developed expertise in select sectors to further our delivery of pioneering and practical solutions. These sectors include (but are not limited to): Automotive, Energy
& Power, Machinery, Chemicals, Healthcare, Food & Beverage, and Distribution & Retail. Stable Consulting Team: InterChina’s Board of Partners is both Western and Chinese, and our Partners provide stability through their commitment to the company. In fact, InterChina enjoys one of the highest employee retention rates in China, and as stability is fundamental for Consulting Teams to be successful, our clients benefit directly as a result. Moreover, all our 50 plus consultants are committed and capable professionals, with a balance of experience and skills that allow InterChina to customize Project Teams to meet the needs of individual clients. Local Presence: InterChina has three operations offices in China, located in Beijing, Shanghai and Shenzhen, supported by liaison offices in Europe, located in Madrid and Milan, and North America, located in Washington D.C. For further information, please visit our website at www.InterChinaConsulting.com

PUBLIC © InterChina Consulting