-
5/22/2018 Hematopathology Lab 2
1/13
Hematopathology Lab 2
Start Slide Show
Read history , review image stacks (space bar, arrow, mouse
click)
Space bar, arrow, mouse click to reveal question
Space bar, arrow, mouse click to reveal answersAfter working
through case using PPS, open virtual slide (links in PPS
or LAB 2 Web page) and review
This PowerPoint show (PPS) uses simple
space-bar/arrow/mouse-click triggered animations to present the
case
history, targeted micrographs (from virtual slides), relevant
questions and a uniform set of "answers". Your instructor
will briefly introduce each case then ask students to work
through the questions, answers and virtual slides using the
PPS on their laptops. The micrographs are displayed adjacent to
micrographs of a "normal" or "look-alike" abnormal
smear at the same magnification. The micrographs should serve as
a guide for viewing the virtual slides. The virtual
slides for this exercise can be accessed from the links embedded
in the PPS (if you are using a workstation or laptop
on the Medical School Campus) or the LAB 2 web page. The final
exam has 10 lab questions. Five from the set ofmicrographs you
studies during week 1 (review Atlas of normal and abnormal
Hematology 2013) and five from Lab
1 and Lab 2 virtual slides (self-test tool).
http://www.med.umich.edu/digitallab/m2pathlabs/hemepath/lab2.htmlhttp://www.med.umich.edu/digitallab/m2pathlabs/hemepath/virtual.htmlhttp://www.med.umich.edu/digitallab/m2pathlabs/hemepath/virtual.htmlhttp://www.med.umich.edu/digitallab/m2pathlabs/hemepath/virtual.htmlhttp://www.med.umich.edu/digitallab/m2pathlabs/hemepath/virtual.htmlhttp://www.med.umich.edu/digitallab/m2pathlabs/hemepath/lab2.html
-
5/22/2018 Hematopathology Lab 2
2/13
Normal smears
Blood smear stack Bone marrow stack
Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide
Normal Marrow Smear (Web viewer)
http://141.214.65.171/M2%20Pathology/Hemepath/H002.svs/http://141.214.65.171/M2%20Pathology/Hemepath/H_ST.svshttp://141.214.65.171/M2%20Pathology/Hemepath/H_ST.svshttp://141.214.65.171/M2%20Pathology/Hemepath/H002.svs/
-
5/22/2018 Hematopathology Lab 2
3/13
Case #1: The patient is a 55-year-old female who presented to
her local physician with increasing
fatigue, night sweats, weight loss, and abdominal "fullness." On
physical examination, the patient
was noted to have a firm, nontender spleen, 10 cm below the left
costal margin. The liver was
slightly enlarged to 2 cm below the right costal margin. No
lymphadenopathy was identified. The
CBC showed: WBC = 105,000 cells/mm3, Hb = 10.5 gm/dl, and
platelets = 85,000/mm3.
Normal smear stack Patient stack
Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide
Case#1 (Web viewer)
http://141.214.65.171/M2%20Pathology/Hemepath/H002.svs/http://141.214.65.171/M2%20Pathology/Hemepath/smear100x03S.svshttp://141.214.65.171/M2%20Pathology/Hemepath/smear100x03S.svshttp://141.214.65.171/M2%20Pathology/Hemepath/H002.svs/
-
5/22/2018 Hematopathology Lab 2
4/13
Case #1: The patient is a 55-year-old female who presented to
her local physician with increasing
fatigue, night sweats, weight loss, and abdominal "fullness." On
physical examination, the patient
was noted to have a firm, nontender spleen, 10 cm below the left
costal margin. The liver was
slightly enlarged to 2 cm below the right costal margin. No
lymphadenopathy was identified. The
CBC showed: WBC = 105,000 cells/mm3, Hb = 10.5 gm/dl, and
platelets = 85,000/mm3.
What are the major abnormalities on the smear?
Markedly elevated WBC, much higher than sepsis case examined
previously. Neutophilia with many precursors (see virtual slide
of
bone marrow aspirate for comparison). Percentage of precursors
higher than in most reactive causes of leukocytosis. Also more
immature forms (myelocytes, prograns and a few blasts) in this
smear compared to usual "reactive left shift". Basophils easy to
spot
(usually very few in normal or reactive leukocytosis). The cells
may not be markedly abnormal appearing, just too many.
What is the differential diagnosis based on the CBC and blood
smear?Chronic myeloid leukemia (CML), chronic phase, versus
leukemoid reaction (excessive reactive leukocytosis).
Would flow cytometry help with the diagnosis?
No. We know from the morphology that the proliferative process
involves relatively normal appearing granulocytes and
granulocytic
precursors. There are no antigenic findings that can separate
chronic phase CML from a reactive leukocytosis.
Would molecular or cytogenetic tests help with the
diagnosis?
Absolutely since the acquired structural genetic defect that
causes CML has been identified. The Philadelphia chromosome t(9;22)
can
be detected in the neoplastic cells using classical cytogenetics
or FISH. The translocation creates a new gene, the bcr:abl
transgene,
that can be detected using molecular (PCR) techniques.
Demonstration of either the Philadelphia chromosome or the
bcr:abl
transgene are required for diagnosis. (more questions on next
slide)
-
5/22/2018 Hematopathology Lab 2
5/13
Case #1: The patient is a 55-year-old female who presented to
her local physician with increasing
fatigue, night sweats, weight loss, and abdominal "fullness." On
physical examination, the patient
was noted to have a firm, nontender spleen, 10 cm below the left
costal margin. The liver was
slightly enlarged to 2 cm below the right costal margin. No
lymphadenopathy was identified. The
CBC showed: WBC = 105,000 cells/mm3, Hb = 10.5 gm/dl, and
platelets = 85,000/mm3.
What is the natural course of this disease? Are there changes in
the blood or bone marrow smears that one can use to monitor
progression?
The bcr:abl transgene (formed by t(9;22)) encodes a chimeric
fusion protein with a constitutively active protein
tyrosine-kinase
domain that affects many downstream signaling cascades. Clonal
expansion and immortalization of the pleuripotential
hematopoietic stem cell occurs (common to lymphoid and
non-lymphoid or myeloid lineages). In most individuals, the mutant
stem
cells continue differentiating primarily down the granulocyte
lineage. The bone marrow fills up with normal looking
granulocytic
precursors that spill out into the bloodstream and accumulate in
the spleen. Over time, additional mutations accumulate
(largelyunknown) that result in loss of differentiation, and an
increase in the percentage of minimally differentiated cells
(blasts). Ultimately,
a lymphoid or myeloid "blast crisis" is likely to occur
(conversion to acute leukemia).
The loss of maturation in the neoplastic clone results in a
gradual increase in the percentage of cells with the morphologic
features of
immature bone marrow cells called "blast forms". These cells
have a variety of microscopic appearances. It may be difficult to
tell
whether they are myeloid or lymphoid blasts based on appearance
in the microscope. Flow cytometry (detects lineage-specific
antigens on cell surface) and cytochemical stains (detects
enzymes associated with granulocytic and monocytic maturation) can
help
determine lineage.
When the percentage of blast forms in the blood or bone marrow
is > 10% but < 20% then the patient is in an "accelerated"
phase of
CML. When the percentage of blast forms in the blood or bone
marrow is 20% or greater the patient is in "blast crisis" or
blast
phase. Blast crisis or blast phase is a conversion to an acute
leukemia.
-
5/22/2018 Hematopathology Lab 2
6/13
Case #2
History #1: 58-year-old male with increasing weakness, fatigue,
malaise, and weight loss over the
previous six weeks. He sought medical attention for several
unexplained lower extremity bruises.
Petechiae and bruises noted. WBC = 155,000 cells/mm3, Hb = 9.0
gm/dl, platelets = 11,000/mm3.
History #2: Four-year-old female with a recent onset of
pharyngitis and otitis, unresponsive to
antibiotics. The patient was febrile to 101.3 degrees F with
sudden onset of fatigue, malaise, and
nondescript bone and joint pains. Physical exam revealed
conjunctival pallor and petechiae on
her lower extremities. WBC = 55,000 cells/mm3, Hb = 7.6 gm/dl,
platelets = 5,000/mm3.
History #1 stack History #2 stack
Virtual Slide History #1 (Web viewer) Virtual Slide History #2
(Web viewer)
http://141.214.65.171/M2%20Pathology/Hemepath/smear100x04S.svshttp://141.214.65.171/M2%20Pathology/Hemepath/smear100x02S.svshttp://141.214.65.171/M2%20Pathology/Hemepath/smear100x02S.svshttp://141.214.65.171/M2%20Pathology/Hemepath/smear100x04S.svs
-
5/22/2018 Hematopathology Lab 2
7/13
Case #2
History #1: 58-year-old male with increasing weakness, fatigue,
malaise, and weight loss over the
previous six weeks. He sought medical attention for several
unexplained lower extremity bruises.
Petechiae and bruises noted. WBC = 155,000 cells/mm3, Hb = 9.0
gm/dl, platelets = 11,000/mm3.
History #2: Four-year-old female with a recent onset of
pharyngitis and otitis, unresponsive to
antibiotics. The patient was febrile to 101.3 degrees F with
sudden onset of fatigue, malaise, and
nondescript bone and joint pains. Physical exam revealed
conjunctival pallor and petechiae on
her lower extremities. WBC = 55,000 cells/mm3, Hb = 7.6 gm/dl,
platelets = 5,000/mm3.
What are the major abnormalities on the smear?
Many (>20%) of the WBC are mononuclear cells that differ from
both normal monocytes and activated lymphocytes . Most havenuclei
with lighter staining, finely divided, less clumped chromatin and
occasional nucleoli (some multiple). These fit the generalcategory
of "blast" forms. Blast is an imprecise term that refers to cells
with nuclear characteristics shared by early stages
ofdifferentiation in the bone marrow.
Blasts have an "active" appearing nucleus (finely dispersed
chromatin, nucleoli). There may be evidence of
cytoplasmicdifferentiation that can help identify lineage (e.g.
granules). Normal bone marrows have 1-2% blasts that include the
earliest stagesof myeloid (non-lymphoid/non-erythroid) and lymphoid
(pro-, pre-B and pro-, pre-T) differentiation. Any blasts in a
blood smear isabnormal and, if unexplained, may require a bone
marrow aspiration/biopsy to evaluate for a possible stem cell
neoplasm.
The disorders in this case illustrate two types of stem cell
neoplasms. All stem cell neoplasms arise from stem and/or early
progenitorcells in the bone marrow (What are the major groups? How
do they differ from one another? See schematic of hematopoiesis in
Atlasor Dr. Stoolmanslecture). The neoplastic stem cells in these
cases both self renew and give off progeny that differentiate to a
limiteddegree. In acute leukemias, maturation of the neoplastic
cells arrests at a relatively early stage of lymphoid or
non-lymphoiddifferentiation. The abnormal cells accumulate in the
bone marrow, suppress normal hematopoiesis (what does this cause?)
and mayspill out into the bloodstream (few or many).
Are these histories and smears from patients with acute
leukemias, viral infections or sepsis ?
Both are acute leukemias. It can be difficult for the novice to
distinguish a reactive lymphocytosis (e.g. florid mononucleosis)
fromleukemia based on the appearance of the atypical cells in the
smear alone. The history, CBC and clinical findings are crucial
pieces ofinformation. Patients with acute leukemia generally have
the signs, symptoms and laboratory findings indicating bone
marrowinsufficiency or failure in addition to the presence of blast
forms. Patients with reactive lymphocytosis should not have such
findings.
Once you have determined that there are a large percentage
(>20%) blasts in blood or bone marrow, know how
additionalimmunologic studies (flow cytometry primarily),
cytochemical stains, cytogenetics and molecular studies are used to
establish aprecise classification in acute leukemias (see questions
below). You should be able to identify Auer rods and know the
clinical
significance of the finding.
-
5/22/2018 Hematopathology Lab 2
8/13
Case #2
History #1: 58-year-old male with increasing weakness, fatigue,
malaise, and weight loss over the
previous six weeks. He sought medical attention for several
unexplained lower extremity bruises.
Petechiae and bruises noted. WBC = 155,000 cells/mm3, Hb = 9.0
gm/dl, platelets = 11,000/mm3.
History #2: Four-year-old female with a recent onset of
pharyngitis and otitis, unresponsive to
antibiotics. The patient was febrile to 101.3 degrees F with
sudden onset of fatigue, malaise, and
nondescript bone and joint pains. Physical exam revealed
conjunctival pallor and petechiae on
her lower extremities. WBC = 55,000 cells/mm3, Hb = 7.6 gm/dl,
platelets = 5,000/mm3.
Look carefully at multiple abnormal cells. Does their appearance
provide any clues to that help refine the diagnosis?
Patient with history #1 has one of several types of Acute
Myeloid Leukemia (AML). Suspect the diagnosis when blasts have
cytoplasmic granularity. Finding a few blasts with Auer rods
confirms the diagnosis but occurs in small percentage of cases.
Additional studies (see questions below) needed to confirm and
further sub classify these neoplasms.
Patient with history #2 most likely has one of two types of
Acute Lymphoblastic Leukemia (ALL): Acute B-lymphoblastic leukemia
or
Acute T-lymphoblastic leukemia (synonymous with acute precursor
B- and precursor T- lymphoblastic leukemias, respectively).Suspect
the diagnosis when blasts have a high nuclear/cytoplasmic ratio and
agranular cytoplasm. Cannot determine whether B- or
T-blasts without additional studies. Some poorly differentiated
AMLs have similar blasts.
Lymphoblastic neoplasms may present as leukemias, bone marrow
and blood involvement primarily, or lymphomas, thymic, nodal
or extra-nodal infiltrates primarily (can you explain this
behavior ?). You may see them referred to as B-lymphoblastic or
T-
lymphoblastic leukemia/lymphoma as a result.
The relative frequencies of different types vary in children and
adults (e.g. ALL > AML in children, AML > ALL in adults). The
clinical
presentations and the approach to diagnosis are similar,
regardless of age.
Would flow cytometry help with the diagnosis?Absolutely. One can
usually determine the lineage of an acute leukemia using a panel of
antibodies that react with stem cell,
granulocytic, monocytic, T and B cell antigens. Currently part
of the initial diagnostic work-up for all suspected acute
leukemias.
Cytochemical stains for enzymes associated with granulocytic
(myeloperoxidase, MPO) and monocytic (non-specific esterase,
NSE)
differentiation is helpful in diagnosing AML. No cytochemical
stains help with ALL.
Would molecular or cytogenetic tests help with the
diagnosis?
Absolutely. Necessary for confirmation of acute promyelocytic
leukemia (t15;17; APL), identification of de novo acute
leukemias
associated with Ph1 translocation and detection of the recurrent
genetic abnormalities used by the WHO system to classify acute
leukemias. Likely that impact of cytogenetic, FISH and molecular
genetic studies will grow as we learn more about the genetic
basisof these cancers.
-
5/22/2018 Hematopathology Lab 2
9/13
Case #2
History #1: 58-year-old male with increasing weakness, fatigue,
malaise, and weight loss over the
previous six weeks. He sought medical attention for several
unexplained lower extremity bruises.
Petechiae and bruises noted. WBC = 155,000 cells/mm3, Hb = 9.0
gm/dl, platelets = 11,000/mm3.
History #2: Four-year-old female with a recent onset of
pharyngitis and otitis, unresponsive to
antibiotics. The patient was febrile to 101.3 degrees F with
sudden onset of fatigue, malaise, and
nondescript bone and joint pains. Physical exam revealed
conjunctival pallor and petechiae on
her lower extremities. WBC = 55,000 cells/mm3, Hb = 7.6 gm/dl,
platelets = 5,000/mm3.
Is a bone marrow aspirate and biopsy necessary to establish the
diagnosis?
If the differential count shows a blast percentage that equals
or exceeds 20% on the peripheral blood smear then the diagnosis
of
acute leukemia is made. However, bone marrow aspiration and
biopsy may be needed to collect enough material for additional
diagnostic studies. If a patient has 20% blast forms in the
blood or bone marrow smear is sufficient for a diagnosis of acute
leukemia. However, more
information required for treatment decisions and precise
classification. Treatments for acute myeloid leukemias and
acute
lymphoblastic leukemias (B and T cell types) are different. Also
there are treatments targeted at some of the recurrent genetic
abnormalities that contribute to leukemogenesis. One example is
ATRA-containing regimens for acute promyelocytic leukemias
(diagnosed by the presence of the t(15;17) translocation) but
others are under development.
The current classification of acute leukemias was developed by
an International panel under the auspices of the World Health
Organization and published in 2008. It replaced the
French-American-British [FAB] classification system. The WHO
guidelinesemphasize cytogenetic (large structural chromosomal
abnormalities, e.g. translocations) and molecular features (small
mutations,
e.g. FLT3, NPM1 and CEBPA) then supplement with morphologic,
immunologic and clinical characteristics where needed.
In some cases, the older FAB classification is still used. This
system separates leukemias into acute myeloid (AML) and acute
lymphoblastic (ALL) types based on immunologic, cytologic
(appearance in microscope) and cytochemical features (e.g.
detection of
lineage-specific enzymes myeloperoxidase [granulocytic] or
non-specific esterase [monocytic]). AMLs are subdivided based on
degree
and lineage(s) of differentiation (M0-M7, details not important)
and the ALLs are subdivided into precursor-B and precursor-T
types
based largely on antigenic profiles defined by flow
cytometry.
-
5/22/2018 Hematopathology Lab 2
10/13
Case #3: The patient is a healthy 65-year-old male who was noted
to have slightly enlarged
axillary and cervical lymph nodes on an annual physical
examination. The patient offered no
complaints and was given a "clean bill of health" one year
previously. No organomegaly was
noted. The CBC showed: WBC = 45,000 cells/mm3, Hb = 13.5 gm/d.,
platelets = 185,000/mm3.
Compare the blood smear in this patient to the normal and
abnormal smears from other cases.
Normal smear stack Patient stack
Virtual Slide Normal Blood Smear (Web viewer) Virtual Slide
Case#3 (Web viewer)
http://141.214.65.171/M2%20Pathology/Hemepath/H002.svs/http://141.214.65.171/M2%20Pathology/Hemepath/BS0023b_100X.svshttp://141.214.65.171/M2%20Pathology/Hemepath/BS0023b_100X.svshttp://141.214.65.171/M2%20Pathology/Hemepath/H002.svs/
-
5/22/2018 Hematopathology Lab 2
11/13
Case #3: The patient is a healthy 65-year-old male who was noted
to have slightly enlarged
axillary and cervical lymph nodes on an annual physical
examination. The patient offered no
complaints and was given a "clean bill of health" one year
previously. No organomegaly was
noted. The CBC showed: WBC = 45,000 cells/mm3, Hb = 13.5 gm/d.,
platelets = 185,000/mm3.
Compare the blood smear in this patient to the normal and
abnormal smears from other cases.
What are the major abnormalities on the smear?
Too many small lymphocytes with
soccer-ball/cracked-mud/ginger-snap nuclear chromatin (absolute
lymphocytosis). Otherwise
unremarkable.
What is the differential diagnosis based on the CBC and blood
smear?
Reactive lymphocytosis versus chronic lymphocytic leukemia or
peripheralized lymphoma (lymphoid neoplasms that arise in any
lymphoid organ may involve the peripheral blood). Need test that
can help determine whether lymphoid cells are primarily
monoclonal B-cells, aberrant T-cells or a mixture of polyclonal
T and B cells without any abnormalities.
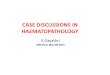
How does the flow cytometry study help with the diagnosis?
(click to see histograms)
-
5/22/2018 Hematopathology Lab 2
12/13
Flow cytometry results
-
5/22/2018 Hematopathology Lab 2
13/13
Case #3: The patient is a healthy 65-year-old male who was noted
to have slightly enlarged
axillary and cervical lymph nodes on an annual physical
examination. The patient offered no
complaints and was given a "clean bill of health" one year
previously. No organomegaly was
noted. The CBC showed: WBC = 45,000 cells/mm3, Hb = 13.5 gm/d.,
platelets = 185,000/mm3.
Compare the blood smear in this patient to the normal and
abnormal smears from other cases.
How does the flow cytometry study help with the diagnosis?
Can identify a monoclonal B-cell population (generally, but not
always, means neoplasm) and identify antigens that are specific
for
some specific types of lymphoid leukemias and lymphomas (e.g.
low level CD20, low-level monoclonal surface Ig, CD5 and CD23
in
classic CLL/SLL).
The flow data in this case demonstrate that most of the
lymphocytes express a single light chain type on their surfaces
(i.e. kappa
or lambda); therefore, they are monoclonal. Normally there are
many more T-cells than B-cells in the blood and the B-cells are
a
mixture of cells expressing kappa and lambda light chains (K:L
ratio = 0.5-2, may be slightly higher or lower in reactive
conditions
but rarely less than 0.1 or greater than 10).
The large number of monoclonal cells in this case confirms that
this is a B-cell neoplasm but there are many different types. In
this
case, the cells express several antigens that nail the
diagnosis: when low-levels of CD20, CD5 and CD23 are co-expressed
on small,
monoclonal B-cells then the diagnosis is chronic lymphocytic
leukemia/small lymphocytic lymphoma in >95% of cases.