-
tlepatitis, Colitis, and Lupus Manifestations
NIGEL GRAY, M.B.,* IAN R. MACKAY, M.D.,t LEON I. TAFT, M.B.,
B.Sc.,t SARA WEIDEN, M.Sc., Ph.D.,t and IAN J. WOOD, M.D.~
T HE ASSOCIATION of chronic ulcerative colitis with liver
disease has been the subject of frequent comment in the l i
terature over the past two decades. ~-~ It is difficult to
generalize about the nature of the association between the two
conditions, due to the variety of pathological changes described in
both organs, and the differences in diagnostic criteria employed by
various authors.
A study has been made of 8 patients suffering from both ulcera-
tive colitis and chronic active hepat i t is / The latter
corresponds to postneerotie cirrhosis as defined by Popper and
Schaffner/ Four of these had evidence of systemic lupus
erythematosus (S.L.E.) and one had mult isystem disease suggestive
of S.L.E. although the L.E. cell test was repeatedly negative. ]n
the present study, the re- lationship between these eouditions has
been examined to assess the r61e of immunological disturbances.
Cases 4 and 5 have also been reported elsewhere/' s
CASE REPORTS Case 1
Chrom;c ulcerative colitis assoc:iated with chro~dc hepalitis. A
16-year- old hairdresser presented in March, 1957, with a 21~ year
history of mild, sometimes bloodstained, d iarrhoea and anaemia.
There was no history of j~undice nor contact with v ira l
hepatitis. She had suffered a severe haematemesis 9 months
previously and had been diagnosed as having chronic hepatitis.
Invest igat ions (Table 1) indicated chronic hepat i t is ;
sigmoidoscopy showed an active ulcerative colitis of moderate
degree. Neither bar ium meal nor splenic venogram revealed
esophageal variees but the splenic venous pressure was elevated to
402 nnn. of water.
Progress: She was treated with cortisone and iron, and remained
well unt i l Aug'ust, 1957, when she had a fur ther hematemesis.
However, there
]?rom the Clinica.1 Research Unit of the Royal Melbourne
Hospital and the WaFter and Eliza: Hall Institute of Medical
Research, Melbourne, Victoria., Australia.
~Drug Houses of Australia, Fellow for 1957. IWorking with the
aid of a grant from the National Health and Medical Research
Council of Australia. We wish to thank Dr. J. Bolton and Dr. M.
Etheridge for permitting access to their
cases. Mr. R.. Inglis and Miss E. Earle assisted in the
preparation of the photographs and sections.
NEW SERIES VOL. 3, NO. 7, I?S8 481
-
Gray et al.
was an improvement in bromsulphthalein excretion, blood
sedimentation rate, and serum gamma globulin level. Cortisone was
discontinued and she remained well, apart from mild diarrhea.
Case 2 Chronic ulcerative cotitis associated with chro~ic active
hepatitis with
response to cortisone. A 51-year-old housewife had suffered from
watery diarrhea for 10 years. She presented in May, 1954, with
generalized edema and increasing ascites for 3 weeks. Recently
there had been blood and mucus in the motions. There was
hypergammaglobulinaemia and a low serum albumin ; liver biopsy
showed chronic active hepatitis and sig- moidoseopy advanced
~lcerative colitis. Numerous antibiotics were given without
improvement, t~owever, she responded dramatically to cortisone, the
diarrhea, ascites, and edema subsided, and she was restored to
health.
Case 3
Chronic hepatitis, possibly postviral, associated with fatal
chro~ic ulcerative colitis, ,without respon, se to cortisone. A
23-year-old school- teacher presented in March, 1952, following 11
months jaundice of in- sidious onset. Laparotomy in the fourth
month of her illness had re- vealed a cirrhotic liver (Fig. 1).
Subsequently the jaundice improved slightly .but had recurred one
month prior to admission. She was mildly jaundiced and there were
numerous spider nevi. The liver and spleen were palpable 2 era.
below the eostM margin. Investigations, inclnding liver biopsy,
showed chronic hepatitis of presumably viral origin.
Progress: She ~mproved and remained well until July, 1955, when
review indicated inactive chronic hepatitis. Iter bowel function
was normal at this time. In March, 1957, she had severe diarrhea
with blood and mucus. Sigmoidoscopy and barium enema revealed
pronounced ulcerative colitis. Her liver function tests were
substantially unchanged. A temporary improvement was obtained with
transfusion, cortisone, and tetracycline, ttowever, she relapsed
one month later and was readmitted with fulminating diarrhea.
Treatment with cortisone, intravenous fluids, and antibiotics did
not improve her condition and she was submitted to ileostomy and
total eolectomy. The excised colon showed gross changes of
ulcerative colitis (Fig. 2). Postoperatively size remained in
peripheral circulatory failure which did not respond to
resuscitative measures. At necropsy there was chronic hepatitis
(Fig. 3).
Case 4 Ulcerative colitis, recurrent hepatitis, arthritis and a
positive L.E.
~ell test, with response to cortisone. A 29-year-old housewife
developed
AMERICAN JOURNAL OF 482 DIGESTIVE DISEASES
-
Hepatitis, Colitis, and Lupus
Fig. 1. Case 3. A female, aged 23 years, with chronic hepatit
is, devel- oping severe ulcerative colitis 4 years later, and dying
after coleetomy. Operative l iver biopsy showing nodu lar pattern
and lymphocytic infi ltra- t ion characterist ic of ac- tive
chronic hepatit is. Haematoxyl in and Eosin. X 50. Ffg, 2. Case
3.
Colectomy specimen. There is gross ulcerat ion and
pseudopolyposis, due to severe ulcerative colitis. Fig. 3. Case 3.
Upper surface o f the l iver at postmortem. There is fine nodular i
ty and sl ight th ickening of the cap- sule due to chronic hepatit
is.
diarrhea with blood and mucus in May, 1956. Sigmoidoscopy
revealed active ulcerative colitis. The diarrhea settled after 5
months. She then developed what appeared to be viral hepatitis with
moderate jaundice. After 8 weeks rest, she enjoyed good health
until the onset of acute purulent appendicitis in February, 1957.
Two weeks after appendec- tomy, she developed a pro,gressive fever,
intermittent vomiting, edema of the ankles, aseites, mild jaundice
and then suppurative peritonitis which required drMnage. An
associated chronic hepatitis was suspected: the scrims albumin
level was 1.6 Gm. per 100 ml. and the gamma globulin was 2.7 Gin,
per 100 ml. She improved remarkably after operation but the serum
proteins remained abnormal. In August, 1957, she was clinically
well, but the gamma globulin was still elevated (3.1 Gin. per' 100
ml.) and the L.E. cell tests was positive on two occasions, She
presented in Octo- ber, 1957, with a 3-weeks history of jaundice
and migratory polyarthritis.
$The teehrAque employed for the L. E. ceil test was that
described by Magath and Winkle. 9
N EW SERI ES VOL. 3, NO, 7, I?S8 483
-
Gray et aL
She now had many spider nevi and the left wrist and some finger
joints were hot, swollen, and slightly tender. The I~.E. cell test
was again posi- tive. Biochemical tests and liver biopsy indicated
active hepatitis. Serial plasma glutamie oxalaeetic-transaminase
(P.G.O.-T.) levels remained highly elevated. Treatment with
cortisone was effective, the jaundice disappearing withill two
weeks and P.G.O.-T. levels falling from 500 units to less than 50
units within three days. 7 The arthritis rapidly im- proved and she
remained well on maintenance cortisone therapy.
Case 5
A fatal case of hepatitis and subseq.~ent ulcerative colitis,
with a posi. live L.E. cell test a~nd glomernlonep,hritis, in
April, 1953, an apparenl attack of viral hepatitis in a 20-year-old
housewife had persisted for 7 weeks. Biochemical tests and liver
biopsy were in keeping with viral hepatitis. Despite cortisone the
disease progressed. The L.E. cell test was positive in December,
1955. In May, 1956, proteinnria developed and a kidney biopsy
showed a membranous nephritis. In October, 1956, she developed
ulcerative colitis and improved with prednis01one. In Janu- ary,
1957, the diarrhea recnrred and she died one month later in hepatic
coma. At necropsy there was chronic ulcerative colitis, hepatitis,
and membranous g'lomerulonephritis.
Cas~
A p:roba~ble case of systemic lupus erythematos~s with severe
ulcerative, colitis, hepatitis, thrombocytopenic pnrpura,
~ephritis, and: a rash; partial response to cortiso~tc. In
November, 1953, a 51:year-old man bad suffered severe diarrhea for
20 months. The liver was enlarged and an erythematous rash was
present on the extremities. Sigmoidoscopy re~ vealed active
ulcerative colitis. He improved. One year later he de- veloped
diarrhea, frequent epistaxes, ulcerative stomatitis, recurrence of
the rash, and the spleen was palpable. The L.E. cell test was
positive once, and the liver biopsy showed chronic hepatitis (Fig.
4). He deteri- orated, and was found to have persistent
thrombocytopenia which did not respond to ACTH therapy. He improved
satisfactorily after splenec- tomy and, apart from occasional
diarrhea, remained moderately well on cortisone for 2 years. In
April, 1957, he had a prolonged exacerbation of the colitis. The
liver was enlarged and biopsy again showed chronic hepatitis.
Colectomy was considered but he responded to increased cortisone
dosage, itowever he relapsed again in July, 1957, and total
colectomy (Fig. 5), ileoreetal anastomosis and defunctioning
ileostomy produced considerable improvement. Operative renal biopsy
revealed an unusual nephritis with pronounced interstitial
lymphocyte infiltration (Fig. 6). When last seen, six months later,
he was moderately well.
AMERICAN JOURNAL OF: 484 DIGESTIVE DISEASES
-
Hepatitis, Colitis, and Lupus
Fig. 4. Case 6. A male, aged 51 years, with severe ulcerative
colitis. chronic hepatit is, thromhocytopenic purpura, nephrit is,
skin rash, and a positive L.E. cell tes t . The l iver biopsy shows
distent ion of structure with lymphocytic inf i l trat ion, fibro-
sis, bi le duct prol i ferat ion, and ir- regular ity of the
polygonal cells. Haematoxyl in and Eosin. X 200. Fig. 5. Case 6.
Microphotograph of mucosa of colectomy specimen show- ing gross in
f lammatory inf i l trat ion. some ulceration, and exudat ion due
to ulcerative colitis. Haematoxy l in and Eosin. X 150. Fig. 6.
Case 6. Opera- tive renal b iopsy . .Fue l of glomerulosclerosis
and per igtomerular lymphocytic inf i l trat ion. Haematoxyl ln and
Eosin. X 150.
Case 7 Chronic ulcerative cotitis, hepatitis, asthma, and
nephritis. L.E. cd~
test negative. Fair response to ~ortisonc. A 50-year-old woman
was seen in December, 1954, suffering from ulcerative colitis with
anemia for 10 years. She improved with transfusion. Three months
later she relapsed with persistent diarrhea, malaise, anorexia,
upper abdominal pain, and jatmdiee. The liver was enlarged and
biochemical tests were in accord- ance with viral hepatitis,
possibly homologous serum jaundice. She ira- proved with supportive
treatment, but in June, 1956, she had jaundice for one week, severe
asthma and simlsitis. I Ier bowel function was normal at this time.
The liver was still enlarged. Biochemical tests and liver biopsy
indicated chronic hepatitis. She improved rapidly and remained well
unti l February, 1957. She was then investigated because of pro-
teinuria.. At renal biopsy (Fig. 7), medulla only was obtained and
this showed considerable interstitial fibrosis. In November, 1957,
she had (~iarrhea, sinusitis, impetigo, and anemia. TI~e Coombs
test was positive
NEW SERIES VOL. 3, NO. 7, 1958 485
-
Gray et al.
7 8
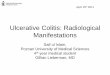
Fig. 7. Case 7. A female, aged 50 years, with chronic ulcerative
colitis, hepatitis, asthma, and nephritis. The L.E. cell test was
negative. Percutaneous renal biopsy showing interstitial fibrosis,
tubular atrophy and hyaline casts in the medulla. Haematoxylin and
Eosin. X I50. Fig. 8. Case 7. Rectal biopsy. There is inflammatory
infiltration of the lamina propria by lymphocytes, plasma cells~
and some polymorphs. Haematoxylin and Eosin. )< 250.
but the L.E. cell test was repeatedly negative. Signmidoseopy
showed recurrence of the ulcerative colitis (Fig. 8). She improved
slowly with medical treatment including cortisone, and at discharge
was well, apart from mild diarrhea.
Case 8 Hepatitis, ulcerative ~olitis, polyarthritis, pleurisy,
pericarditis, and a
positive L.E. cell test. Fair response to cortisone. In July,
1952, a 30- year-old man complained of intermittent diarrhea for 2
years, poly- arthritis for two months, and hemoptysis. He was
slightly jaundiced and both liver and spleen were enlarged.
Sigmoidoscopy showed ulcera- tive colitis; biochemical tests and
liver biopsy revealed active hepatitis. He was treated with
cortisone and the jaundice decreased over the next 12 months.
However he continued to have intermittent diarrhea and
polyarthritis. In May, 1954, Raynaud's phenomenon and changes in
the skin of his fingers suggestive of scleroderma were observed. In
July, 1954, he developed pleurisy, periearditis, congestive cardiac
failure, and the L.E. cell test and Coombs test were positive. In
November, 1956, his symptoms became more pronounced., he had
pleural effusions and ascites, and there was biochemical evidence
of impaired renal function. Necropsy showed cirrhosis and chronic
ulcerative colitis.
DISCUSSION
Fat ty inf i l trat ion of the liver is the commonest
pathological change found in pat ients with chronic ulcerative
colitis. Est imates of its occurrence vary ; Kimmelst ie l et al. 1
reported 15 per cent of
AMERICAN JOURNAL OF 486 DIGESTIVE DISEASES
-
Hepatitis, Colitis, and Lupus
93 cases, and Jones et a l /52 per cent of 91 cases. The
incidence of cirrhosis in association with ulcerative colitis was
shown to be 4 per cent of 284 cases by Hoffbauer et al2 and 19 per
cent of 32 cases by Kleclmer et al. 4 In each of the above series
histological con- firmation of the liver lesion was obtained.
The outstanding problem is the mechanism whereby the liver
disease and colitis occur together. It is uncertain whether one of
these conditions is primary, or whether there is a common etiologi-
cal factor. It is frequently suggested that ulcerative colitis is
the initial lesion/ and that the hepatitis is due either to a
conditioned nutritional deficiency or to portal toxemia. However in
two of our cases (Cases 3 and 5) the hepatitis preceded the colitis
and in cer- tain others (Cases 1, 2, 4, 6, and 8) it may well have
been latent. Moreover in three of our cases (Cases 1, 4, and 5) the
colitis was not severe and a nutritional deficiency was not
apparent. In view of these facts we wish to present an alternative
concept whereby an immunological disturbance may be responsible for
both lesions.
We are influenced in this regard by our previous experience with
chronic hepatitis unassociated with ulcerative colitis. Persistence
of viral activity had been postulated as a cause of nonnutritional
chronic active hepatitis, but such a process finds no parallel
among other viral diseases. An alternative hypothesis was provided
by Joske and Kin. g n and l~Iackay et al. ~2 who found a positive
L.E. cell test in a group of cases of chronic hepatitis. The
process was termed hpoid hepatitis and it was suggested that
continuing activi- ty of the disease was due to an immunological
reaction. Further evidence relevant to this concept was obtained by
study of the auto- immune complement fixation (A.I.C.F.) reaction
developed by Gajdusek ~ at this Institute. This reaction was
frequently positive in classical S.L.E. and lupoid hepatitis.
~3
If it is accepted that immunological mechanisms are concerned in
the pathogenesis of S.L.E. and in the continuance of active hepa-
titis in certain cases, then a similar immunological process may be
involved in the etiology of the ulcerative colitis in our cases.
With this thought in mind it is of interest to summarize some of
the relevant features of the eight cases in this study (see Table
2). A raised serum gamma globulin level was found in all cases, the
L.E. cell test was positive in four cases, the A.I.C.F. reaction
was posi- rive in six cases and a significant clinical response to
cortisone was observed in five cases. In addition other phenomena
thought to
NEW SERIES VOL. 3, NO. 7, 1958 487
-
-;~
T
AB
LE
1
. C
lin
ica
l a
nd
La
bo
rato
ry F
ind
ing
s in
Ca
ses
of
Ch
ron
ic H
ep
ati
tis
an
d Ulc
era
tiv
e C
oli
tis
OO
oo
Ca
se#
/ se
x/a
ge
D
ate
Se
rum
~
ert
tln
S
eru
m glo
b.
Hg
b
bil
iru
bin
alb
. (G
in./
10
0 mI.)
Se
rum
E
SP
~
(Gin
./
(ra
g,/
(G
in./
a
lk. p
ho
s, (ra
m./
B
SP
re
- Sig
moid
ose
opy
10
0m
l.)
10
0m
l.) 1
00
ml.
) T
ota
l G
am
ma (K
-Au
.)
hr.
a)
ten
tio
n
fin
din
gs
Ba
riu
m e
ne
ma
1/F
/16
3
/57
8
/57
2/F
/51
5
/54
3/F
/23
4
/52
7
/55
3
/57
4/F
/29
3
/57
5
/57
s/
57
1
0/5
7
5/F
/20
4
/53
1
2/5
5
10
/56
6/M
/51
1
2/5
4
~
4/57
~
"We
st e
rgre
n.
8.7
0
.6
4.1
3
.5
2.3
2
3
50
1
8.4
%
lTlc
era
tiv
e co
liti
s
4.5
0
.6
3.3
2
.5
1.5
1
6
15
1
1
%
8.8
1.O
2
.9
4.1
3
.2
40
4
4
Ad
va
nc
ed
ulc
era
- ti
ve
co
liti
s
13
.1
4.0
3
.7
3.4
1
.5
57
5
4
12
.5
2.0
2
.9
3.2
1
.2
79
8
9
7.0
1
.2
2.7
3
.9
1.8
4
7
60
11
.1
2.3
1
.6
4.5
2
.7
37
9
0
12
.8
1.6
2
.7
5.2
2
.7
3
24
%
1
4.3
0
.6
4.3
5
.2
3.1
4
6
60
3
2 %
1
2.5
6
.0
2.1
6
.0
4.3
1
7
70
12
.5
10
.0
3.7
5
.3
3.9
2
1
90
..
10
.9
3.2
2
.5
3.9
1
.3
77
6
3
38
%
7
.9
0.6
2
.6
3.5
2
.7
54
..
10
.9
2.0
3
.8
5.4
3
6
65
11
.1
3.4
2
.9
4.7
7
1
95
(Co~
thl~
led)
Ad
va
nc
ed
ulc
era
- ti
ve
co
liti
s
~T
oY
llq
al
llq
ll~
OS
~
Ad
van
ced
M
cera
- tir
e c
oli
tis
Ad
van
ced
ul
cera
- tiv
e co
litis
Ad
van
ced
ul
cera
- tiv
e co
litis
~ Pii
)este
lll ~ ~ C
OlO
ll
Muc
osal
ul
cera
tion
Loss
of
hau
stra
tion
Mu
co
sa
l ulc
era
tio
n
Lo
ss o
f h
au
str
at.
ion
No
rma
l
Lo
ss o
f h
au
str
ati
on
-
Hepatitis, Colitis, and Lupus
N~ m
,o ~ g :
NEW SERIES VOL. 3, NO. 7, 19S8
c~
o
) ,.=
have an immunological basis such as thrombocytopenia,
arthralgia, asthma, a positive Coombs test, and visceral le- sions
characterized by lymphocyte ac- tivity were seen in some cases.
It is interesting to speculate o~ the na- ture of the factors
initiating the multi- system disease exemplified by the pres- ent
group of eases. It has been suggested that the pr imary disturbance
in such dis- eases is in the mesenchymal antibody producing system,
a* Alternatively, it is possible that induced autoantigenicity of
some body component is responsible. If this is so, pr imary damage
to the liver may be the initiating mechanism.
"Other ease studies favouring an im- munological factor in
chronic ulcerative colitis were reported by Kirsner and Palmer 1"~
who described the occurrence of colitis in a patient who developed
arthritis, possible scleroderma, pneu- monitis, and febrile
episodes suggestive of S.L.E., and also in a patient with rheumatic
fever, pneumonitis, hepatitis, hyperglobulinemia, and hemolytic
ane- mia. These patients, particularly the second, would fall into
the clinical pat- tern of S.L.E. although results of the L.E. cell
test were not recorded. Kirsner and Palmer 1~ suggested bowel
hypersen- sitivity to an initial bacterial invasion as a possible
causative factor in ulcerative colitis, but this does not
necessarily ac- count for the other lesions.
No attempt has been made here to as- certain how often chronic
hepatitis and ulcerative colitis are associated, nor is it
suggested that the association of the two conditions necessarily
depends on ira-
489
-
Gray et al.
TABLE 2. Clinical and Laboratory Data Relevant to the
Immunologica l Basis of Hepatit is Associated with Colitis
Serum gamma g lobul in l~esponse
Case g . /100 ml. L .E . cell A . I .C .F / Coombs to no. (max
imum level) test t i te r test Ar thr i t i s cort isone
1 3.5 - - - - - - :No Poor 2 3.2 .. 4 - - No Exce l lent 3 1.8 -
- 4 - - :No Poor 4 3.1 -I- 4 - - Yes Exce l lent 5 3.9 -~- 8 - - No
Poor 6 2.1 + 64 - - No ]Y[oderate 7 ].8 - - - - + Yes 1Y[oderate 8
2.8 + .. + Yes ~oderate
aExpressed as rec iproca l of max imum pos i t ive serum t i ter
.
munological mechanisms. Itowever, the occurrence in eight pa-
tients of hepatitis and colitis, with other probable auto-immune
dis- orders in some of them, appears to be more than fortuitous. It
may even be that cases such as these are, in fact, variants of true
systemic lupus erythematosus.
SUMMARY
1. An analysis has been made of eight cases in which hepatitis
and ulcerative colitis occurred together. Current explanations of
this association, including conditioned nutrit ional deficiency and
portal toxemia causing liver damage, failed to account for all the
features of our particular cases.
2. Of the eight patients, three had chronic hepatitis of
uncertain pathogenesis and concurrent ulcerative colitis of varying
severity and five others had, in addition, systemic lesions
including nephri- tis, pleurisy, pericarditis, polyarthritis, and
thromboeytopenic purpura. 3. Evidence for an auto-immune
pathogenesis in these cases in- eluded elevated serum gamma
globulin levels, positive L.E. cell tests in four cases, and
positive "auto- immune complement fixa- t ion" reactions in six
cases. Five patients responded well to corti- sone. The dense
lymphocytic aggregates seen in histological sec- tions of affected
tissues were also thought to be of significance.
4. This immunological disturbance may depend upon induced
auto-antigenicity of some body component as a result of initial
AMERICAN JOURNAL OF 490 DIGESTIVE DISEASES
-
Hepatitis, Colitis, and Lupus
tissue damage--alternatively there may be a fundamental anomaly
of antibody producing tissues.
REFERENCES
1. IfIMlkIELSTIEL, P., LARGE, It. L., and ERNER, H. D. Liver
damage in ulcerative eo]itis. A~. J. Path. 28/259, 1952.
2. JONES, G. W., BAGeENSTOSS, A. H., and I~_~RGEN, J. A.
iEIepatie lesions and dysfunc- tion associated with chronic
ulcerative colitis. Am. J. Med. Sci. 221:279, 1951.
3. t{OFFBAUEa, F. W., McCa~TNEX', J. S., DENNIS, C., and
K.SRLSON, If. The relation- ship of chronic ulcerative colitis and
cirrhosis. Ann. Int. Med. 39:267, 1953.
4. I~LECKNEI% ~. S., STAUFFER, iVl. H., ]~ARGEN, J. A., and
DOCKEI~Ty, l~. B. Hepatic lesions in the living patient with
chronic ulcerative colitis as demonstrated by needle biopsy.
Gaztroenterology 22:13, 1952.
5. SAINT, E. G,, IfING, W. E., JOSKE, R. A., and F INCKH, E. S.
The course of infectious hepatitis with special reference to
prognosis and the chronic stage. Aust. Ann. Med. 2:113, 1953.
6. PoP~'E]~, H., and SCHAF~NEI%, F. Liver: Struetu~'e and
Function. New York, Mc- Graw-ttill, 1957.
7. O'BIglEN, E. N., GOBLE, A. J., and 5~ACKAY, IaN R. Plasma
transaminase activity as an index of effectiveness of cortisone in
chronic hepatitis. Lancet (in press), 1958.
8. TAFT, L. I., MACKAY, LxN R., and L~,kI~KIN, LOIS. Hepatitis
complicated by mani- festatious of lupus erythematosus. J. Path.
Bact. 75:399, 1958.
9. IV[AGATH, T. B., and WINKLE, V. Technic for demonstrating 'L
.E. ' (Lupus Erythe- matosus) cells in blood. A~n. J. Clin. Path.
22:586, 1952.
10. SHEI~LOCK, S. Diseases of the Liver and Biliary System.
Oxford, Blaekwell Scientific Publications, 1955.
11. JOSKE, R. A., and I~ING, W. E. The 'L.E. cell' phenomenon in
active chronic viral hepatitis. Lancet 2:477, 1955.
12. MACKAY, I.aN 1~., TAFT, L. I., and C0WLINO, D. C. Lupoid
hepatitis. Lancet 2:1323, 1956.
13. GAJDUSEK, D. C. An 'auto-immune' reaction against human
tissue a~tigens in cer- tain chronic diseases. Natwrc 179:666,
1957.
14. MACKAY, IAN 1~., and LAaKISr, LOIS. The significance of the
presence in human serum of complement fixil~g antibodies to human
tissue antigens. Submitted for publication, 1958.
15. KmsNEa, J. B., and PALMEI% W. L. Ulcerative colitis.
Considerations of its aetiol- ogy and treatment. J .A.M.A. 155:341,
1954:.
NEW SERIES VOL. 3, NO. 7, 1958 4.91