Embed Size (px)
Citation preview
REVIEW
Reprint requests to: Hidetsugu Saito, MD, PhD, Inaida Research Center for Anti-aging Medicine in Hepato-Gastroenterology, School of Medicine, Keio Uni-versity, 35 Shinanomachi, Shinjuku-ku, Tokyo 160-8582, Japan, TEL: +81-3-3353-1211, FAX: +81-3-3351-8705, E-mail: [email protected]
Introduction
Hepatocellular carcinoma (HCC) is the third and fourth
leading cause of cancer-related death in Japanese men and women, respectively, and is the 5th most common cause of cancer worldwide. The incidence of HCC has
Hepatocellular Carcinoma in Keio Affiliated Hospitals – Diagnosis, Treatment, and Prognosis of this Disease –
Hidetsugu Saito,1 Tetsuya Masuda,2 Shinichiro Tada,3 Hirotoshi Ebinuma,4 Yoshiyuki Yamagishi,4 Keisuke Ojiro,4 Mika Inoue5 and Toshifumi Hibi4
161
AbstractWe have retrospectively investigated patients with hepatocellular carcinoma (HCC) (912 cas-es) treated in the Affiliated Hospitals of Keio University (the Keio Association for the Study of Liver Diseases: KASLD) and here we review the recent diagnosis and treatment of HCC. HCC is a major cause of death in Japan and a major etiology of this disease is chronic viral infection such as hepatitis C virus (HCV) and hepatitis B virus (HBV). Screening of HCC by imaging studies and measurement of serum tumor markers successfully prolonged survival of the pa-tients in Japan. The prognosis of this disease has been determined by both tumor factors and degree of liver function, and its staging is usually established with a recent system such as Ja-pan Integrated Staging Score (JIS). The 5-year survival rate of JIS stage 0, 1, 2 and 3 were 68.3%, 51.9%, 25.8% and 16.6%, respectively in our cohort. Multivariate analysis using Cox proportional hazard models showed that age (>65), HCV infection, tumor number, TB (>1.0), AFP (>20) and PIVKA-II (>40) were significant factors affecting survival among the entire patients. Major treatment strategies are hepatic resection, radio frequency ablation and trans-arterial chemo-embolization, but alternative treatments such as radiation, chemotherapy, and their combination have been used to reduce tumor sizes resulting prolongation of the survival or maintenance of patients’ quality of life, while liver transplantation has not been popular in Japan. However, the overall survival continues to decrease from year to year, and does not show a plateau phase in Kaplan-Mayer curve. These results suggest that the best way to im-prove survival can be achieved by prevention of the disease. Antiviral therapies have de-creased the incidence of HCC, indicating that treatment for chronic hepatitis is the best way to prevent HCC development at present. (Keio J Med 58 (3) : 161-175, September 2009)
Keywords: prognostic scoring system, screening, small hepatocellular carcinoma, prevention, antivi-ral therapy
1Inaida Research Center for Anti-aging Medicine in Hepato-Gastroenterology, School of Medicine, Keio University, Tokyo, Japan
2Department of Internal Medicine, Nihon Kohkan Hospital, Kanagawa, Japan3Daiwa Shouken Clinic, Tokyo, Japan
4Division of Gastroenterology and Hepatology, Department of Internal Medicine, School of Medicine, Keio University, Tokyo, Japan
5Schering-Plough Center for the Study of Chronic Liver Diseases, School of Medicine, Keio University, Tokyo, Japan
(Received for publication on January 5, 2009)(Accepted for publication on May 21, 2009)

162 Saito H, et al: HCC in Keio Affiliated Hospitals
increased in Japan in the past several decades and has re-cently increased dramatically in the United States and other Western countries, except for a small group of pa-tients whose mortality showed favorable trends.1 The in-crease is primarily related to the spread of hepatitis C vi-rus (HCV) infection, which peaked in the 1960s and 1980s in Japan and the United States, respectively. Con-siderable attention has been paid to the emerging HCC epidemic, which is often associated with hepatitis C and hepatitis B, and end-stage liver cirrhosis (LC) which oc-curs as a result of repetitive cycles of inflammation and repair and is associated with the development of HCC. End-stage liver cirrhosis and HCC can both seriously impact the quality of life of patients.
In Western countries, liver transplantation has been used successfully to treat patients with HCC;2 however, the shortage of donor livers and other technical reasons limit the option for transplantation in some patients.3,4 In Japan, liver transplantation for HCC is less common due to the shortage of cadaveric donor organs.5 Additionally, strategies to reduce tumor growth are important for pa-tients who are awaiting liver transplantation. For that purpose, ablation techniques or chemoembolization to control local tumor growth are very useful. Unlike with other cancers, the treatment indication strategy for HCC depends not only on the surgical staging of cancer growth and degree of spread but also on residual re-served liver function. These considerations determine whether treatment modalities other than surgery, such as local ablation techniques, should be employed. Thus, the treatment of HCC has progressed dramatically during the past few decades since our last review,6 and the progno-sis of HCC has improved in parallel with our understat-ing of the nature of the disease. Several review articles on HCC have been published recently7 as well as clinical guidelines for HCC from several organizations around
the world.8-11
In the present report, we summarized data of patients with HCC who had been previously admitted to the Keio University Hospital and the Keio Affiliated Hospitals, which was integrated as the Keio Association for the Study of Liver Diseases (KASLD), and review the treat-ments and prognoses of this disease.
Patients Studied
In 2007, the core members of the fourth KASLD meet-ing resolved to collect clinical data from HCC patients through the affiliated hospitals of Keio University to bet-ter understand recent trends in HCC treatment. The data were analyzed retrospectively. Survival rates were ana-lyzed using the Kaplan-Meier product limit survival method and the log-rank test was used to determine sta-tistical significance. Data from patients in different groups were compared using the Mann-Whitney U test for continuous variables. Categorical variables were ana-lyzed by x2 test or Fisher’s exact test. We used Cox pro-portional hazard models to examine the potential deter-minants of survival. The start date used for survival anal-ysis was the date of the first diagnosis. All statistical analyses were performed using the Statistical Program for Social Sciences (SPSS 13.0 for Windows; SPSS, Inc., Chicago, IL). Statistical significance was defined by a P value less than 0.05.
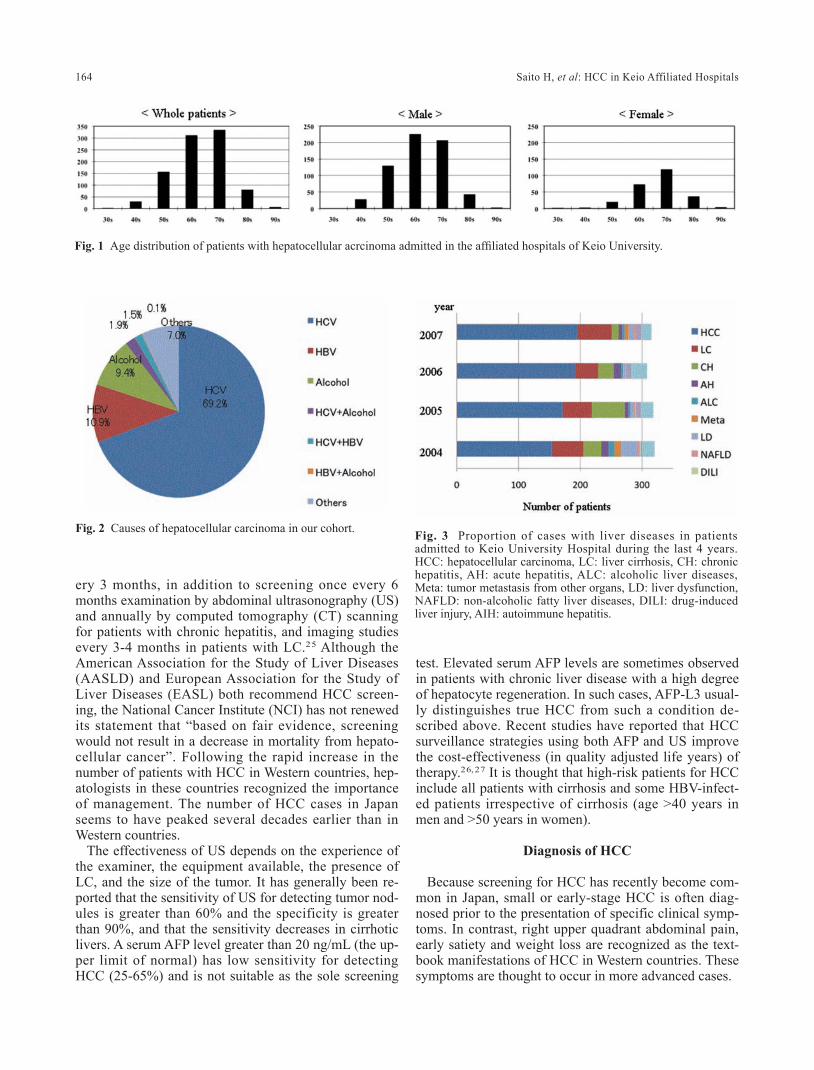
The list of the hospitals and the number of patients in-cluded are summarized in Table 1. Baseline characteris-tics of the patients are summarized in Table 2. The age distribution of patients with HCC (at the time of diagno-sis) is shown in Figure 1; a majority of the patients were elderly, probably because the main cause of HCC is HCV infection, and progression of liver fibrosis depends on age and duration of infection.12, 13 However, elderly
Institution Number of patients
Data completedKeio University HospitalSaiseikai Chuo HospitalNihon Kohkan Hospital
211244106
Subtotal 561
Data incompleteKitasato Institute HospitalSaitama Shakai Hoken HospitalKeiyu HospitalTachikawa Kyosai HospitalTokyo Dental Ichikawa HospitalEiju Sogo HospitalKawasaki City Kawasaki Hospital
161912727191412
Subtotal 351
Total 912
Table 1 Patients and hospitals enrolled in this statistics for the KASLD

Keio J Med 2009; 58 (3): 161-175 163
patients develop HCC more often than younger patients despite their lower grade of fibrosis,14 suggesting that the impact of aging is stronger for fibrosis for develop-ment of HCC. It has been said that male gender is the most significant risk factor of HCC. The peak age of fe-male patients was older than male patients and aging fac-tor may be a main causing factor in female patients.
Etiology of HCC
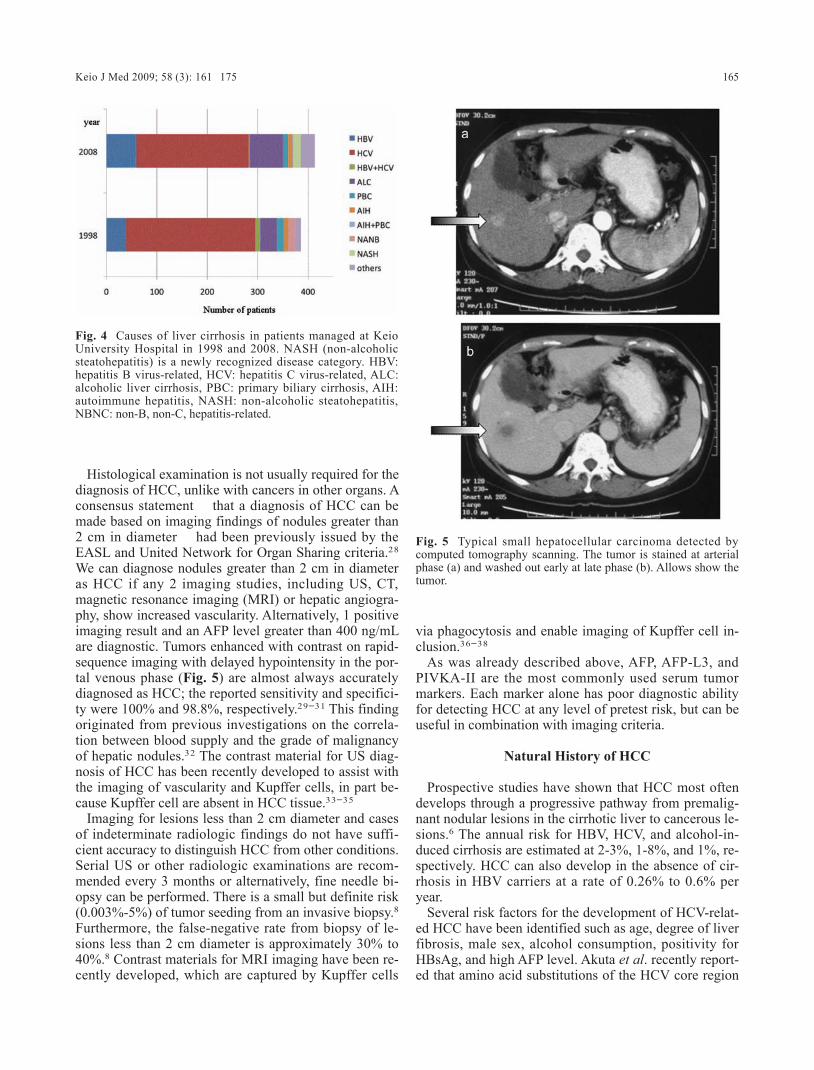
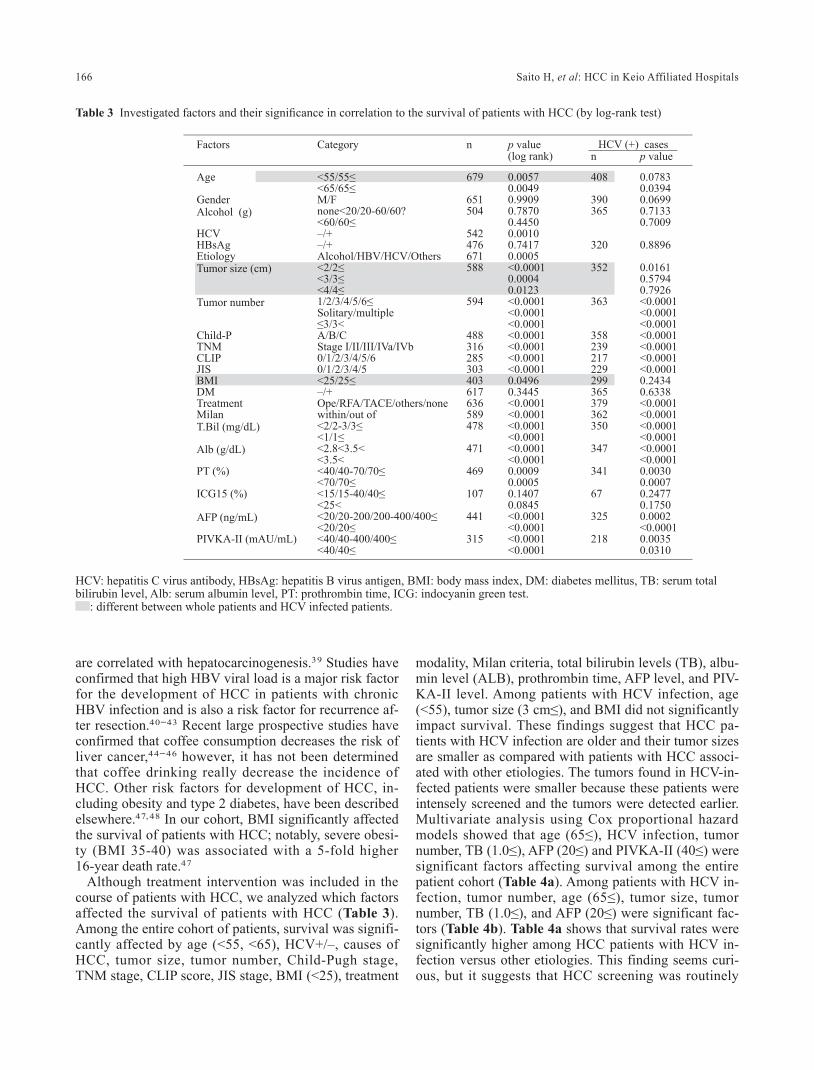
The major clinical risk factor for development of HCC is cirrhosis of the liver. The major risk factors for the de-velopment of LC are HBV- and HCV-infection and chronic heavy alcohol drinking.15 HCV has been previ-ously shown to account for the majority of cases of HCC in Japan,16 and our findings were similar; the frequency of HCV was 69% (Fig. 2). Figure 3 shows the propor-tion of cases with liver diseases due to different causes among patients admitted to Keio University Hospital during the last 4 years. It is clear that HCC was the ma-jor cause of admissions due to liver diseases. HBV was the second leading cause of HCC (seen in 10% of cases) and the infections were acquired early in life through transmission from mother to offspring in most HBV cas-es (Fig. 2). Chronic alcohol use of greater than 80 g/day for more than 10 years increased the risk of HCC 5-fold,17 and chronic alcohol use in HBV and HCV in-fection (seen in 1.78% of cases in our study) doubles the risk as compared with either infection alone. Figure 4 shows the causes of LC in patients consulting to Keio University Hospital. Chronic HCV infection was a major cause of cirrhosis; this finding is comparable to nation-
wide in Japan, but differs from the trend in Western countries, where alcoholic cirrhosis remains a major cause of LC. Insulin-resistance and the metabolic syn-drome are thought to be predisposing factors non-alco-holic steatohepatitis (NASH) and cirrhosis in 10% to 20% of cases,18 and diabetes and obesity have been shown to double the risk of HCC.19 These patients might be included in the unknown category in Figure 2. The cause of LC in 1998 did not include NASH; however, in 2008, NASH was included as one of the causes in our study (Fig. 4).
Screening of HCC
Although potentially curative treatment for early stage of HCC was achieved with a 3-year survival rate in the range of 60-80%, the rate is as low as 10% for late-stage disease worldwide. These observations strongly suggest that screening practices allowing for improved diagnosis at an early stage of this disease could have a large impact on survival. Recently, prospective cohort studies and a randomized controlled trial (RCT) suggested that HCC screening of patients with chronic liver diseases can im-prove survival rates;20-22 however, this notion remains controversial.23 Many clinicians support screening for HCC and believe that it would be unethical to perform a randomized controlled trial to demonstrate its efficacy.24
The Japan Society of Hepatology (JSH) recommends HCC screening by a tumor marker measurement (pres-ence of 2 of 3 markers: alpha-fetoprotein [AFP], lectin-bound AFP [AFP-L3] or des-γ carboxy prothrombin, also known as vitamin K antagonist-II [PIVKA-II]) ev-
Number Median Range
Age at diagnosis 912 68 30 – 96Gender M/F 631/251HCV-Ab –/+ 201/538HBsAg –/+ 570/86BMI 524 22.7 13.8 – 33.2DM –/+ 484/299Tumor size (cm) 744 2.3 0.7 – 20.0Tumor number 1/2/3/4/5/6≤ 449/123/43/18/3/111TB (mg/dL) 628 0.86 0.20 – 66.0Alb (g/dL) 620 3.8 1.9 – 8.8PT% 615 79 29 – 107ICG(15) (%) 162 22.9 2.8 – 89.2AFP (ng/mL) 576 22.0 0.5 – 874560PIVKA-II (pg/mL) 395 36 0 – 349000Child-Pugh A/B/C 422/161/57TNM I/II/III/IVa/IVb 144/117/70/24/5CLIP 0/1/2/3/4/5/6 132/112/56/20/10/9/7JIS 0/1/2/3/4/5 89/107/90/40/6/11Treatment Ope/RFA/TACE/others/none 86/134/317/189/87Milan within/out 510/227Observation period (W) 382 118.8 0.6 – 702.7
Table 2 Baseline characteristics of the patients
HCV-Ab: hepatitis C virus antibody, HBsAg: hepatitis B virus antigen, BMI: body mass index, DM: diabetes mellitus, TB: serum total bilirubin level, Alb: serum albumin level, PT: prothrombin time, ICG: indocyanin green test.
164 Saito H, et al: HCC in Keio Affiliated Hospitals
ery 3 months, in addition to screening once every 6 months examination by abdominal ultrasonography (US) and annually by computed tomography (CT) scanning for patients with chronic hepatitis, and imaging studies every 3-4 months in patients with LC.25 Although the American Association for the Study of Liver Diseases (AASLD) and European Association for the Study of Liver Diseases (EASL) both recommend HCC screen-ing, the National Cancer Institute (NCI) has not renewed its statement that “based on fair evidence, screening would not result in a decrease in mortality from hepato-cellular cancer”. Following the rapid increase in the number of patients with HCC in Western countries, hep-atologists in these countries recognized the importance of management. The number of HCC cases in Japan seems to have peaked several decades earlier than in Western countries.
The effectiveness of US depends on the experience of the examiner, the equipment available, the presence of LC, and the size of the tumor. It has generally been re-ported that the sensitivity of US for detecting tumor nod-ules is greater than 60% and the specificity is greater than 90%, and that the sensitivity decreases in cirrhotic livers. A serum AFP level greater than 20 ng/mL (the up-per limit of normal) has low sensitivity for detecting HCC (25-65%) and is not suitable as the sole screening
test. Elevated serum AFP levels are sometimes observed in patients with chronic liver disease with a high degree of hepatocyte regeneration. In such cases, AFP-L3 usual-ly distinguishes true HCC from such a condition de-scribed above. Recent studies have reported that HCC surveillance strategies using both AFP and US improve the cost-effectiveness (in quality adjusted life years) of therapy.26,27 It is thought that high-risk patients for HCC include all patients with cirrhosis and some HBV-infect-ed patients irrespective of cirrhosis (age >40 years in men and >50 years in women).
Diagnosis of HCC
Because screening for HCC has recently become com-mon in Japan, small or early-stage HCC is often diag-nosed prior to the presentation of specific clinical symp-toms. In contrast, right upper quadrant abdominal pain, early satiety and weight loss are recognized as the text-book manifestations of HCC in Western countries. These symptoms are thought to occur in more advanced cases.
Fig. 2 Causes of hepatocellular carcinoma in our cohort. Fig. 3 Proportion of cases with liver diseases in patients admitted to Keio University Hospital during the last 4 years. HCC: hepatocellular carcinoma, LC: liver cirrhosis, CH: chronic hepatitis, AH: acute hepatitis, ALC: alcoholic liver diseases, Meta: tumor metastasis from other organs, LD: liver dysfunction, NAFLD: non-alcoholic fatty liver diseases, DILI: drug-induced liver injury, AIH: autoimmune hepatitis.
Fig. 1 Age distribution of patients with hepatocellular acrcinoma admitted in the affiliated hospitals of Keio University.
Keio J Med 2009; 58 (3): 161-175 165
Histological examination is not usually required for the diagnosis of HCC, unlike with cancers in other organs. A consensus statement -that a diagnosis of HCC can be made based on imaging findings of nodules greater than 2 cm in diameter- had been previously issued by the EASL and United Network for Organ Sharing criteria.28 We can diagnose nodules greater than 2 cm in diameter as HCC if any 2 imaging studies, including US, CT, magnetic resonance imaging (MRI) or hepatic angiogra-phy, show increased vascularity. Alternatively, 1 positive imaging result and an AFP level greater than 400 ng/mL are diagnostic. Tumors enhanced with contrast on rapid-sequence imaging with delayed hypointensity in the por-tal venous phase (Fig. 5) are almost always accurately diagnosed as HCC; the reported sensitivity and specifici-ty were 100% and 98.8%, respectively.29-31 This finding originated from previous investigations on the correla-tion between blood supply and the grade of malignancy of hepatic nodules.32 The contrast material for US diag-nosis of HCC has been recently developed to assist with the imaging of vascularity and Kupffer cells, in part be-cause Kupffer cell are absent in HCC tissue.33-35
Imaging for lesions less than 2 cm diameter and cases of indeterminate radiologic findings do not have suffi-cient accuracy to distinguish HCC from other conditions. Serial US or other radiologic examinations are recom-mended every 3 months or alternatively, fine needle bi-opsy can be performed. There is a small but definite risk (0.003%-5%) of tumor seeding from an invasive biopsy.8 Furthermore, the false-negative rate from biopsy of le-sions less than 2 cm diameter is approximately 30% to 40%.8 Contrast materials for MRI imaging have been re-cently developed, which are captured by Kupffer cells
via phagocytosis and enable imaging of Kupffer cell in-clusion.36-38
As was already described above, AFP, AFP-L3, and PIVKA-II are the most commonly used serum tumor markers. Each marker alone has poor diagnostic ability for detecting HCC at any level of pretest risk, but can be useful in combination with imaging criteria.
Natural History of HCC
Prospective studies have shown that HCC most often develops through a progressive pathway from premalig-nant nodular lesions in the cirrhotic liver to cancerous le-sions.6 The annual risk for HBV, HCV, and alcohol-in-duced cirrhosis are estimated at 2-3%, 1-8%, and 1%, re-spectively. HCC can also develop in the absence of cir-rhosis in HBV carriers at a rate of 0.26% to 0.6% per year.
Several risk factors for the development of HCV-relat-ed HCC have been identified such as age, degree of liver fibrosis, male sex, alcohol consumption, positivity for HBsAg, and high AFP level. Akuta et al. recently report-ed that amino acid substitutions of the HCV core region
Fig. 4 Causes of liver cirrhosis in patients managed at Keio University Hospital in 1998 and 2008. NASH (non-alcoholic steatohepatitis) is a newly recognized disease category. HBV: hepatitis B virus-related, HCV: hepatitis C virus-related, ALC: alcoholic liver cirrhosis, PBC: primary biliary cirrhosis, AIH: autoimmune hepatitis, NASH: non-alcoholic steatohepatitis, NBNC: non-B, non-C, hepatitis-related.
Fig. 5 Typical small hepatocellular carcinoma detected by computed tomography scanning. The tumor is stained at arterial phase (a) and washed out early at late phase (b). Allows show the tumor.
166 Saito H, et al: HCC in Keio Affiliated Hospitals
are correlated with hepatocarcinogenesis.39 Studies have confirmed that high HBV viral load is a major risk factor for the development of HCC in patients with chronic HBV infection and is also a risk factor for recurrence af-ter resection.40-43 Recent large prospective studies have confirmed that coffee consumption decreases the risk of liver cancer,44-46 however, it has not been determined that coffee drinking really decrease the incidence of HCC. Other risk factors for development of HCC, in-cluding obesity and type 2 diabetes, have been described elsewhere.47,48 In our cohort, BMI significantly affected the survival of patients with HCC; notably, severe obesi-ty (BMI 35-40) was associated with a 5-fold higher 16-year death rate.47
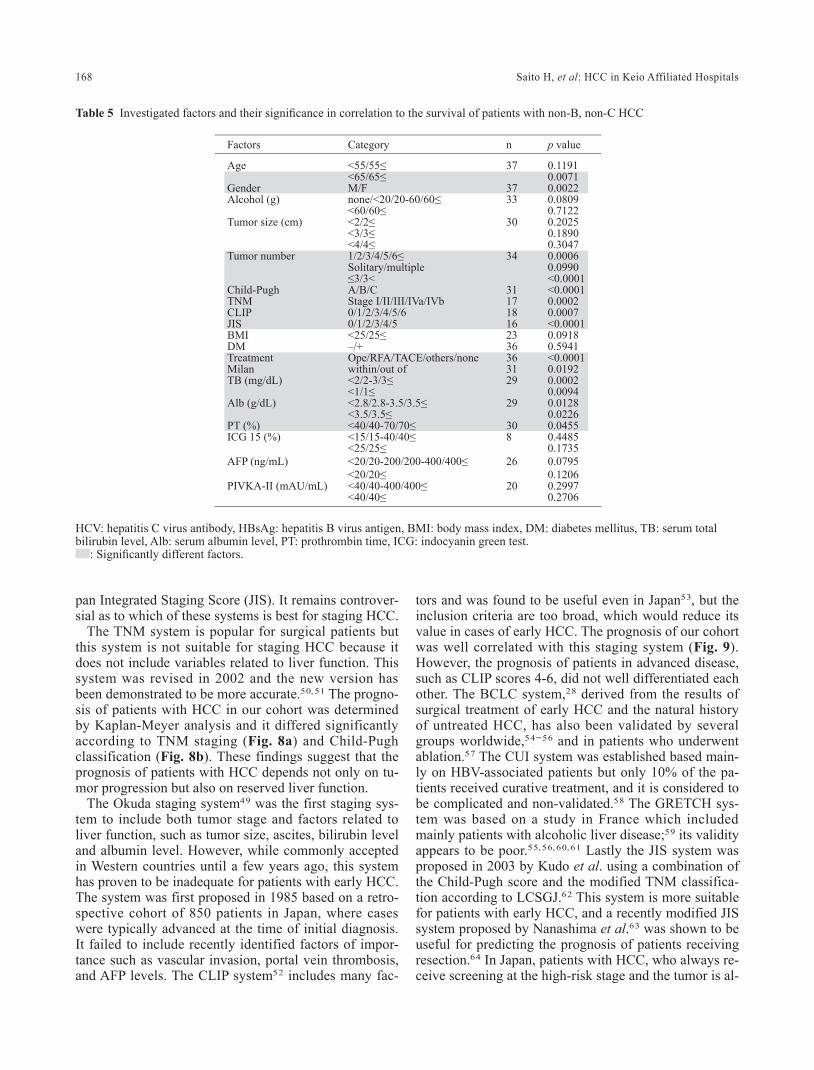
Although treatment intervention was included in the course of patients with HCC, we analyzed which factors affected the survival of patients with HCC (Table 3). Among the entire cohort of patients, survival was signifi-cantly affected by age (<55, <65), HCV+/–, causes of HCC, tumor size, tumor number, Child-Pugh stage, TNM stage, CLIP score, JIS stage, BMI (<25), treatment
modality, Milan criteria, total bilirubin levels (TB), albu-min level (ALB), prothrombin time, AFP level, and PIV-KA-II level. Among patients with HCV infection, age (<55), tumor size (3 cm≤), and BMI did not significantly impact survival. These findings suggest that HCC pa-tients with HCV infection are older and their tumor sizes are smaller as compared with patients with HCC associ-ated with other etiologies. The tumors found in HCV-in-fected patients were smaller because these patients were intensely screened and the tumors were detected earlier. Multivariate analysis using Cox proportional hazard models showed that age (65≤), HCV infection, tumor number, TB (1.0≤), AFP (20≤) and PIVKA-II (40≤) were significant factors affecting survival among the entire patient cohort (Table 4a). Among patients with HCV in-fection, tumor number, age (65≤), tumor size, tumor number, TB (1.0≤), and AFP (20≤) were significant fac-tors (Table 4b). Table 4a shows that survival rates were significantly higher among HCC patients with HCV in-fection versus other etiologies. This finding seems curi-ous, but it suggests that HCC screening was routinely
Factors Category n p value HCV (+) cases(log rank) n p value
Age <55/55≤ 679 0.0057 408 0.0783<65/65≤ 0.0049 0.0394
Gender M/F 651 0.9909 390 0.0699Alcohol (g) none<20/20-60/60? 504 0.7870 365 0.7133
<60/60≤ 0.4450 0.7009HCV –/+ 542 0.0010HBsAg –/+ 476 0.7417 320 0.8896Etiology Alcohol/HBV/HCV/Others 671 0.0005Tumor size (cm) <2/2≤ 588 <0.0001 352 0.0161
<3/3≤ 0.0004 0.5794<4/4≤ 0.0123 0.7926
Tumor number 1/2/3/4/5/6≤ 594 <0.0001 363 <0.0001Solitary/multiple <0.0001 <0.0001≤3/3< <0.0001 <0.0001
Child-P A/B/C 488 <0.0001 358 <0.0001TNM Stage I/II/III/IVa/IVb 316 <0.0001 239 <0.0001CLIP 0/1/2/3/4/5/6 285 <0.0001 217 <0.0001JIS 0/1/2/3/4/5 303 <0.0001 229 <0.0001BMI <25/25≤ 403 0.0496 299 0.2434DM –/+ 617 0.3445 365 0.6338Treatment Ope/RFA/TACE/others/none 636 <0.0001 379 <0.0001Milan within/out of 589 <0.0001 362 <0.0001T.Bil (mg/dL) <2/2-3/3≤ 478 <0.0001 350 <0.0001
<1/1≤ <0.0001 <0.0001Alb (g/dL) <2.8<3.5< 471 <0.0001 347 <0.0001
<3.5< <0.0001 <0.0001PT (%) <40/40-70/70≤ 469 0.0009 341 0.0030
<70/70≤ 0.0005 0.0007ICG15 (%) <15/15-40/40≤ 107 0.1407 67 0.2477
<25< 0.0845 0.1750AFP (ng/mL) <20/20-200/200-400/400≤ 441 <0.0001 325 0.0002
<20/20≤ <0.0001 <0.0001PIVKA-II (mAU/mL) <40/40-400/400≤ 315 <0.0001 218 0.0035
<40/40≤ <0.0001 0.0310
Table 3 Investigated factors and their significance in correlation to the survival of patients with HCC (by log-rank test)
HCV: hepatitis C virus antibody, HBsAg: hepatitis B virus antigen, BMI: body mass index, DM: diabetes mellitus, TB: serum total bilirubin level, Alb: serum albumin level, PT: prothrombin time, ICG: indocyanin green test.
: different between whole patients and HCV infected patients.

Keio J Med 2009; 58 (3): 161-175 167
performed for the HCV-infected patients and that this screening system worked well to improve survival.
There were 56 patients with non-B, non-C (NBNC) HCC. Although number of these patients was insufficient to conclude the result, survival was significantly affected by age (65≤), gender and the disease staging (Table 5). Tumor stage seemed to be more advanced among these patients as compared with cases of HCC associated with other etiologies, presumably because they had not been previously screened for HCC. But as shown in this table, there is no significant characteristic of the patients in this category (no significant high-risk factor); therefore, screening of these patients is very difficult.
Treatment and Prognosis of HCC
In Japan, the management of HCC involves multiple disciplines, including hepatology, surgery, diagnostic and interventional radiology and pathology. Liver transplan-tation has not been frequently performed so far in Japan, and surgery and loco-regional treatment, such as abla-tion, remain the 2 major curative modalities for early-stage HCC. Before choosing a modality of treatment, tu-mor staging should be evaluated precisely. HCC staging is also important for the prognosis of HCC. Two disease processes, namely, the tumor and the underlying cirrho-sis, complicate the prognosis of HCC simultaneously, and many studies have suggested that cirrhosis rather than the size of the tumor mass is the main determinant of the prognosis. The median survival time of untreated patients with newly diagnosed HCC is weeks to months in Western countries, where screening of HCC only re-cently became popular. Survival time could be improved by screening for HCC among high-risk groups. A num-ber of factors are associated with a poor outcome: male sex, advanced age, etiologic agent, presence of more
than 1 risk factor, tumor size, tumor number, doubling time of nodules, vascular invasion, and distant metasta-sis. The complicated and heterogeneous nature of HCC has led to the development of a variety of staging sys-tems.
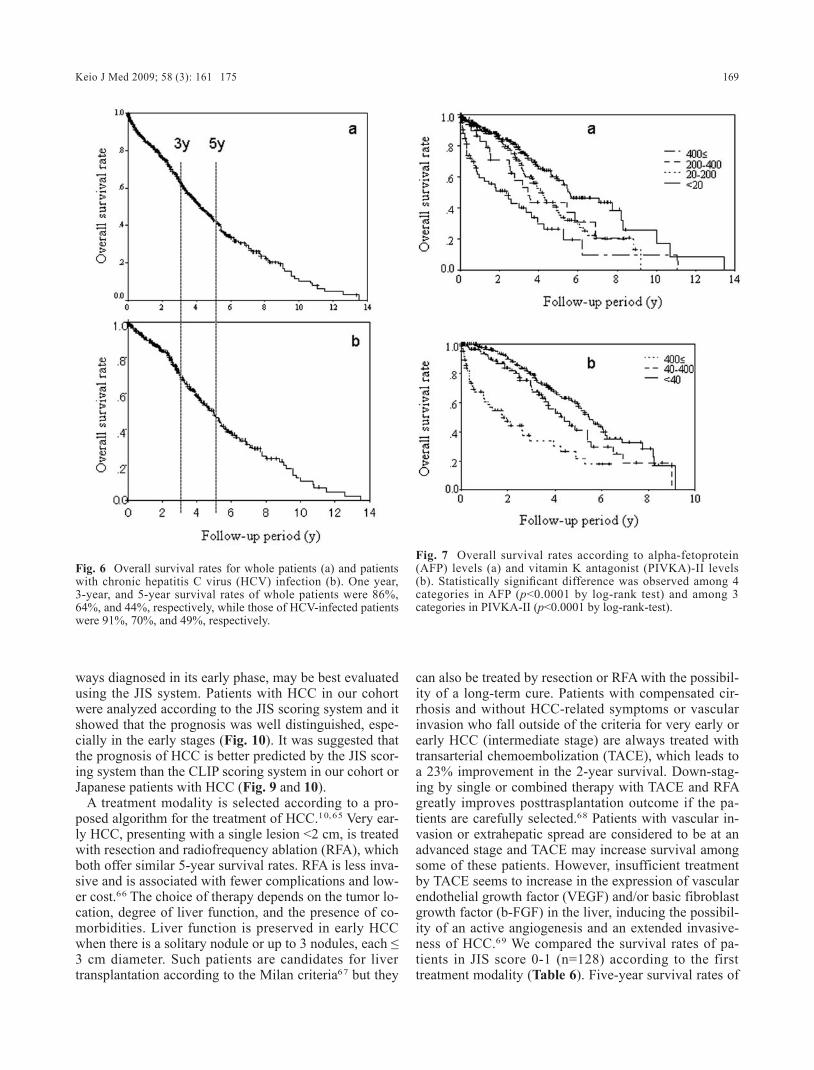
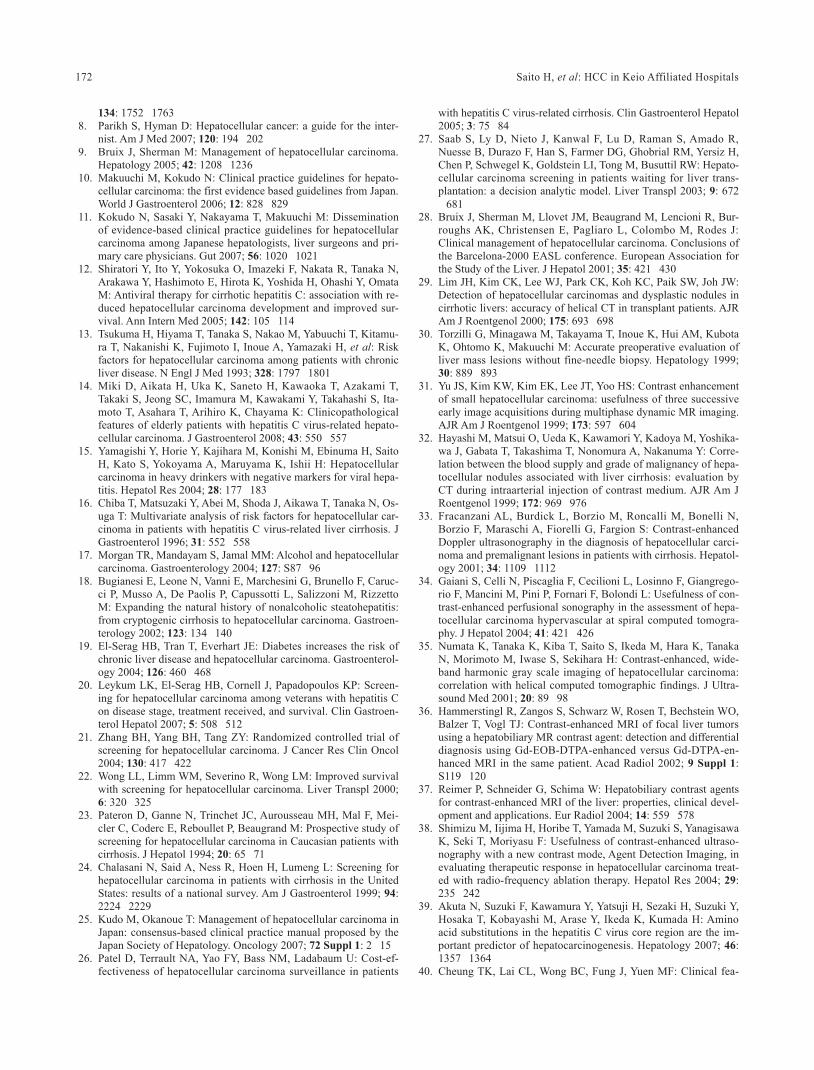
Overall survival curve in our cohort is shown in Figure 6a. One-, 3-, and 5-year survival rates were 86%, 64%, and 44%, respectively, which were higher than those obtained from the Japanese nationwide surveil-lance (year 2002-3) made by the Liver Cancer Study Group of Japan (LCSGJ) including 96,404 HCC cases. Figure 6b shows the survival curve in patients with chronic HCV infection. The survival rates at 1-, 3-, and 5-year were 91%, 70%, and 49%, respectively, which were higher than those of whole patients. This result also indicates that screening of patients with chronic liver diseases makes better outcome. The measurement of se-rum AFP and PIVKA-II levels is an easy way of screen-ing. In our case series, elevation of serum levels of AFP (>20; normal limit) (Fig. 7a) and PIVKA-II (>40; nor-mal limit) (Fig. 7b) significantly affected the survival of patients with HCC. It was suggested that AFP levels more than 400 ng/mL and/or PIVKA-II level more than 400 mAU/mL were significant bad prognostic markers. The 5-year survival rates of these patients were around 20%.
The Tumor Node Metastasis (TNM) classification, mostly used for solid tumors, has extreme limitations be-cause it does not include the severity of underlying cir-rhosis or residual liver function. Many prognostic stag-ing systems have been established; the first attempt by Professor Okuda in Japan,49 followed by systems devel-oped by Cancer of Liver Italian Program (CLIP), Barce-lona Clinic Liver Cancer (BCLC), Groupe d’Etude du Treatment du Carcinome Hepatocellulaire (GRETCH), Chinese University Prognostic System (CUPI), and Ja-
a: Whole patients
Factor hazard ratio 95% CI p value
Age 65≤ 2.703 1.668 – 4.381 <0.0001HCV + 0.505 0.305 – 0.837 0.0080Tumor number 2≤ 2.321 1.542 – 3.493 <0.0001TB (mg/dL) 1.0≤ 2.007 1.328 – 3.031 0.0009AFP (ng/mL) 20≤ 1.964 1.284 – 3.006 0.0019PIVKA-II(mAU/mL) 40≤ 1.490 0.986 – 2.252 0.0584
b: HCV infected patients
Factor hazard ratio 95% CI
Age 65≤ 2.345 1.381 – 4.070 0.0026Tumor size 2≤ 1.940 1.196 – 3.146 0.0073Tumor number 2≤ 2.546 1.579 – 4.105 0.0001TB (mg/dL) 1.0≤ 1.489 0.915 – 2.424 0.1094AFP (ng/mL) 20≤ 2.107 1.441 – 4.021 0.0008
Table 4 Significant factors affected survival of patients with HCC found by multivariate analyses
HCV: hepatitis C virus antibody, TB: serum total bilirubin level.
168 Saito H, et al: HCC in Keio Affiliated Hospitals
pan Integrated Staging Score (JIS). It remains controver-sial as to which of these systems is best for staging HCC.
The TNM system is popular for surgical patients but this system is not suitable for staging HCC because it does not include variables related to liver function. This system was revised in 2002 and the new version has been demonstrated to be more accurate.50,51 The progno-sis of patients with HCC in our cohort was determined by Kaplan-Meyer analysis and it differed significantly according to TNM staging (Fig. 8a) and Child-Pugh classification (Fig. 8b). These findings suggest that the prognosis of patients with HCC depends not only on tu-mor progression but also on reserved liver function.
The Okuda staging system49 was the first staging sys-tem to include both tumor stage and factors related to liver function, such as tumor size, ascites, bilirubin level and albumin level. However, while commonly accepted in Western countries until a few years ago, this system has proven to be inadequate for patients with early HCC. The system was first proposed in 1985 based on a retro-spective cohort of 850 patients in Japan, where cases were typically advanced at the time of initial diagnosis. It failed to include recently identified factors of impor-tance such as vascular invasion, portal vein thrombosis, and AFP levels. The CLIP system52 includes many fac-
tors and was found to be useful even in Japan53, but the inclusion criteria are too broad, which would reduce its value in cases of early HCC. The prognosis of our cohort was well correlated with this staging system (Fig. 9). However, the prognosis of patients in advanced disease, such as CLIP scores 4-6, did not well differentiated each other. The BCLC system,28 derived from the results of surgical treatment of early HCC and the natural history of untreated HCC, has also been validated by several groups worldwide,54-56 and in patients who underwent ablation.57 The CUI system was established based main-ly on HBV-associated patients but only 10% of the pa-tients received curative treatment, and it is considered to be complicated and non-validated.58 The GRETCH sys-tem was based on a study in France which included mainly patients with alcoholic liver disease;59 its validity appears to be poor.55, 56, 60, 61 Lastly the JIS system was proposed in 2003 by Kudo et al. using a combination of the Child-Pugh score and the modified TNM classifica-tion according to LCSGJ.62 This system is more suitable for patients with early HCC, and a recently modified JIS system proposed by Nanashima et al.63 was shown to be useful for predicting the prognosis of patients receiving resection.64 In Japan, patients with HCC, who always re-ceive screening at the high-risk stage and the tumor is al-
Factors Category n p value
Age <55/55≤ 37 0.1191<65/65≤ 0.0071
Gender M/F 37 0.0022Alcohol (g) none/<20/20-60/60≤ 33 0.0809
<60/60≤ 0.7122Tumor size (cm) <2/2≤ 30 0.2025
<3/3≤ 0.1890<4/4≤ 0.3047
Tumor number 1/2/3/4/5/6≤ 34 0.0006Solitary/multiple 0.0990≤3/3< <0.0001
Child-Pugh A/B/C 31 <0.0001TNM Stage I/II/III/IVa/IVb 17 0.0002CLIP 0/1/2/3/4/5/6 18 0.0007JIS 0/1/2/3/4/5 16 <0.0001BMI <25/25≤ 23 0.0918DM –/+ 36 0.5941Treatment Ope/RFA/TACE/others/none 36 <0.0001Milan within/out of 31 0.0192TB (mg/dL) <2/2-3/3≤ 29 0.0002
<1/1≤ 0.0094Alb (g/dL) <2.8/2.8-3.5/3.5≤ 29 0.0128
<3.5/3.5≤ 0.0226PT (%) <40/40-70/70≤ 30 0.0455ICG 15 (%) <15/15-40/40≤ 8 0.4485
<25/25≤ 0.1735AFP (ng/mL) <20/20-200/200-400/400≤ 26 0.0795
<20/20≤ 0.1206PIVKA-II (mAU/mL) <40/40-400/400≤ 20 0.2997
<40/40≤ 0.2706
Table 5 Investigated factors and their significance in correlation to the survival of patients with non-B, non-C HCC
HCV: hepatitis C virus antibody, HBsAg: hepatitis B virus antigen, BMI: body mass index, DM: diabetes mellitus, TB: serum total bilirubin level, Alb: serum albumin level, PT: prothrombin time, ICG: indocyanin green test.
: Significantly different factors.
Keio J Med 2009; 58 (3): 161-175 169
ways diagnosed in its early phase, may be best evaluated using the JIS system. Patients with HCC in our cohort were analyzed according to the JIS scoring system and it showed that the prognosis was well distinguished, espe-cially in the early stages (Fig. 10). It was suggested that the prognosis of HCC is better predicted by the JIS scor-ing system than the CLIP scoring system in our cohort or Japanese patients with HCC (Fig. 9 and 10).
A treatment modality is selected according to a pro-posed algorithm for the treatment of HCC.10,65 Very ear-ly HCC, presenting with a single lesion <2 cm, is treated with resection and radiofrequency ablation (RFA), which both offer similar 5-year survival rates. RFA is less inva-sive and is associated with fewer complications and low-er cost.66 The choice of therapy depends on the tumor lo-cation, degree of liver function, and the presence of co-morbidities. Liver function is preserved in early HCC when there is a solitary nodule or up to 3 nodules, each ≤3 cm diameter. Such patients are candidates for liver transplantation according to the Milan criteria67 but they
can also be treated by resection or RFA with the possibil-ity of a long-term cure. Patients with compensated cir-rhosis and without HCC-related symptoms or vascular invasion who fall outside of the criteria for very early or early HCC (intermediate stage) are always treated with transarterial chemoembolization (TACE), which leads to a 23% improvement in the 2-year survival. Down-stag-ing by single or combined therapy with TACE and RFA greatly improves posttrasplantation outcome if the pa-tients are carefully selected.68 Patients with vascular in-vasion or extrahepatic spread are considered to be at an advanced stage and TACE may increase survival among some of these patients. However, insufficient treatment by TACE seems to increase in the expression of vascular endothelial growth factor (VEGF) and/or basic fibroblast growth factor (b-FGF) in the liver, inducing the possibil-ity of an active angiogenesis and an extended invasive-ness of HCC.69 We compared the survival rates of pa-tients in JIS score 0-1 (n=128) according to the first treatment modality (Table 6). Five-year survival rates of
Fig. 6 Overall survival rates for whole patients (a) and patients with chronic hepatitis C virus (HCV) infection (b). One year, 3-year, and 5-year survival rates of whole patients were 86%, 64%, and 44%, respectively, while those of HCV-infected patients were 91%, 70%, and 49%, respectively.
Fig. 7 Overall survival rates according to alpha-fetoprotein (AFP) levels (a) and vitamin K antagonist (PIVKA)-II levels (b). Statistically significant difference was observed among 4 categories in AFP (p<0.0001 by log-rank test) and among 3 categories in PIVKA-II (p<0.0001 by log-rank-test).

170 Saito H, et al: HCC in Keio Affiliated Hospitals
patients received hepatic resection, RFA, TACE, and percutaneous ethanol injection (PEI) were 89.3%, 70.8%, 44.6%, and 43.2%, respectively.
Clinical trials for patients with advanced-stage HCC, which includes progressive liver failure, tumor growth with vascular involvement, extrahepatic spread, and physical impairment, have shown no clear benefits.70-75 A recent RCT showed that sorafenib, a multikinase in-hibitor of raf kinase, VEGF2, VEGF-receptor (R)3, and platelet-derived growth factor receptor (PDGFR)-β ki-nases, improved overall survival by about 3 months among patients at BCLC stage C as compared with pla-cebo.76 Another option may be focused radiation therapy (hypofractionated stereotactic radiotherapy), which has also been considered recently for the treatment of HCC, especially in cases with portal thrombosis or lesions just under the diaphragm.77 Carbon ion radiotherapy has been utilized in some institutions in Japan; a favorable
result was obtained but the procedure is still restricted to a small proportion of HCC.78 Interferon (IFN) is an anti-tumor drug candidate and is used as systemic treatment for HCC due to chronic HCV- or HBV-infection. Our in vitro studies demonstrated that IFN has an anti-cancer effect in addition to its viral elimination effect.79-84 Re-cent studies reported favorable clinical outcomes with IFN usage in cases of advanced-stage HCC.47,85,86 Ther-apies combining anti-cancer agents, delivered systemi-cally or transarterially, in combination with TACE or that without embolization (TAI) have been utilized in Japan under institutional ethical approval, but no clear evi-dence has been reported.
Fig. 9 Overall survival rates according to Cancer of Liver Italian Program (CLIP) scores in whole patients. Statistically significant difference was observed among 7 categories (p<0.0001 by log-rank-test).
Fig. 10 Overall survival rates according to Japan Integrated Staging (JIS) scores in whole patients. Statistically significant difference was observed among 6 categories (p<0.0001 by log-rank-test).
Fig. 8 Overall survival rates according to Child-Pugh grades (a) and TMN stages (b) in whole patients. Statistically significant difference was observed among categories in both systems (p<0.0001 by log-rank test).

Keio J Med 2009; 58 (3): 161-175 171
The Future of HCC Treatment
The mechanisms of HCC pathogenesis are gradually clarifying. Several tumor suppressors or protooncogenes are known to be mutated in HCC, including p53, Rb, and insulin-like growth factor (IGF),48, 87 and intracellular signaling pathways, such as VEGF, endothelial growth factor (EGF), and their down-stream signaling cascades, have been shown to contribute to the growth of HCC.88 Genome-wide analysis of gene transcription in the liver has recently revealed that some gene expression profiles consistently change from chronic hepatitis to HCC,89 suggesting that some key molecules to accelerate or in-hibit tumor development might be discovered in future. Imatinib, an inhibitor of several tyrosine kinases, is an-other agent that targets hepatic cancer progenitor cells.90 These new agents are very encouraging candidates for the treatment for HCC in the future. Immunologic stimu-lation may be another future therapeutic candidate for HCC.91 It has also been demonstrated that it is possible to predict HCC based on expression-profiling of forma-lin-fixed, paraffin-embedded liver tissue.92 Several pos-sible preventive agents for HCC have been identified, such as retinoids,93-95 branched-chain amino acid sup-plementation,9 6 vitamin K,9 7 and anti-viral thera-pies,98-102 and these agents may help to overcome the difficulties in treating advanced cases of HCC. A recent investigation has indicated that therapy to resolve hepatic fibrosis may also be useful for preventing the develop-ment of HCC.103 Among these various therapeutic mo-dalities, resolution of liver cirrhosis using heat shock protein 47 is the most promising in my opinion,104 be-cause this therapy may not only prevent HCC develop-ment but also improve liver function by resolution of liv-er cirrhosis.
The overall survival of patients with HCC continues to decrease from year to year, and does not show a plateau phase in Kaplan-Mayer curve, as was shown in our co-hort, which is trend that is quite different from that ob-served with other types of cancer. These results suggest that the best way to improve survival of patients with HCC through prevention of the disease. It has been con-firmed that IFN therapy for chronic HCV infection de-creases the incidence of HCC. Nucleoside or nucleotide
analogues for chronic HBV infection also decrease the incidence of HCC. This outcome has been encouraging to hepatologists and we continue to treat patients with chronic liver diseases as we have done for chronic hepa-titis C during the last few decades105-111 until HCC is fi-nally eradicated.
Acknowledgements
We thank all the members of the KASLD who offered their clinical data to establish the clinical trends of the Keio Medical Society. We especially thank Ms. Mika In-oue for her generous assistance to this work. We also thank doctors, Nobuhiro Tsukada, Norio Maeda (Saisei-kai Chuo Hospital), Yasutaka Inagaki (Nihon Kohkan Hospital), Satoshi Tsunematasu, Naoki Kumagai, Kanji Tsuchimoto (Kitasato Institute Hospital), Takeshi Yoshi-da (Saitama Shakai Hoken Hospital), Hiroshi Nagata, Shigeyuki Zeki, (Keiyu Hospital), Kazuo Kashiwazaki (Tachikawa Kyosai Hospital), Jiro Nishida (Tokyo Den-tal Collage Ichikawa Hospital), Yoshinori Horie, Masa-hiro Kikuchi (Eiju Sogo Hospital), Daisuke Ito, Hanae Takagi (Kawasaki City Kawasaki Hospital) for their spe-cial efforts.
References
1. Bosetti C, Levi F, Boffetta P, Lucchini F, Negri E, La Vecchia C: Trends in mortality from hepatocellular carcinoma in Europe, 1980-2004. Hepatology 2008; 48: 137-145
2. Fisher RA, Maluf DG, Wolfe L, Williams B, Cotterell A, Stravitz RT, Heuman D, Posner M: Is hepatic transplantation justified for primary liver cancer? J Surg Oncol 2007; 95: 674-679
3. Llovet JM, Schwartz M, Mazzaferro V: Resection and liver trans-plantation for hepatocellular carcinoma. Semin Liver Dis 2005; 25: 181-200
4. Molmenti EP, Klintmalm GB: Liver transplantation in association with hepatocellular carcinoma: an update of the International Tu-mor Registry. Liver Transpl 2002; 8: 736-748
5. Sugawara Y, Makuuchi M: Advances in adult living donor liver transplantation: a review based on reports from the 10th anniver-sary of the adult-to-adult living donor liver transplantation meet-ing in Tokyo. Liver Transpl 2004; 10: 715-720
6. Saito H, Tsuchiya M: Recent advances in the study of hepatocel-lular carcinoma. Keio J Med 1992; 41: 195-204
7. El-Serag HB, Marrero JA, Rudolph L, Reddy KR: Diagnosis and treatment of hepatocellular carcinoma. Gastroenterology 2008;
Treatment n Survival rate
1-year 3-year 5-year
Hepatic resection 24 100% 95.2% 89.3%RFA 33 96.5% 70.8% 70.8%TACE 44 95.2% 79.2% 44.6%PEI 27 96.2% 88.5% 43.2%
Table 6 The survival rates of patients with HCC in the JIS score 0-1
RFA: radio frequency ablation therapy, TACE: trasarterial chemo-embolization, PEI: percutaneous ethanol injection therapy.
172 Saito H, et al: HCC in Keio Affiliated Hospitals
134: 1752-1763 8. Parikh S, Hyman D: Hepatocellular cancer: a guide for the inter-
nist. Am J Med 2007; 120: 194-202 9. Bruix J, Sherman M: Management of hepatocellular carcinoma.
Hepatology 2005; 42: 1208-1236 10. Makuuchi M, Kokudo N: Clinical practice guidelines for hepato-
cellular carcinoma: the first evidence based guidelines from Japan. World J Gastroenterol 2006; 12: 828-829
11. Kokudo N, Sasaki Y, Nakayama T, Makuuchi M: Dissemination of evidence-based clinical practice guidelines for hepatocellular carcinoma among Japanese hepatologists, liver surgeons and pri-mary care physicians. Gut 2007; 56: 1020-1021
12. Shiratori Y, Ito Y, Yokosuka O, Imazeki F, Nakata R, Tanaka N, Arakawa Y, Hashimoto E, Hirota K, Yoshida H, Ohashi Y, Omata M: Antiviral therapy for cirrhotic hepatitis C: association with re-duced hepatocellular carcinoma development and improved sur-vival. Ann Intern Med 2005; 142: 105-114
13. Tsukuma H, Hiyama T, Tanaka S, Nakao M, Yabuuchi T, Kitamu-ra T, Nakanishi K, Fujimoto I, Inoue A, Yamazaki H, et al: Risk factors for hepatocellular carcinoma among patients with chronic liver disease. N Engl J Med 1993; 328: 1797-1801
14. Miki D, Aikata H, Uka K, Saneto H, Kawaoka T, Azakami T, Takaki S, Jeong SC, Imamura M, Kawakami Y, Takahashi S, Ita-moto T, Asahara T, Arihiro K, Chayama K: Clinicopathological features of elderly patients with hepatitis C virus-related hepato-cellular carcinoma. J Gastroenterol 2008; 43: 550-557
15. Yamagishi Y, Horie Y, Kajihara M, Konishi M, Ebinuma H, Saito H, Kato S, Yokoyama A, Maruyama K, Ishii H: Hepatocellular carcinoma in heavy drinkers with negative markers for viral hepa-titis. Hepatol Res 2004; 28: 177-183
16. Chiba T, Matsuzaki Y, Abei M, Shoda J, Aikawa T, Tanaka N, Os-uga T: Multivariate analysis of risk factors for hepatocellular car-cinoma in patients with hepatitis C virus-related liver cirrhosis. J Gastroenterol 1996; 31: 552-558
17. Morgan TR, Mandayam S, Jamal MM: Alcohol and hepatocellular carcinoma. Gastroenterology 2004; 127: S87-96
18. Bugianesi E, Leone N, Vanni E, Marchesini G, Brunello F, Caruc-ci P, Musso A, De Paolis P, Capussotti L, Salizzoni M, Rizzetto M: Expanding the natural history of nonalcoholic steatohepatitis: from cryptogenic cirrhosis to hepatocellular carcinoma. Gastroen-terology 2002; 123: 134-140
19. El-Serag HB, Tran T, Everhart JE: Diabetes increases the risk of chronic liver disease and hepatocellular carcinoma. Gastroenterol-ogy 2004; 126: 460-468
20. Leykum LK, El-Serag HB, Cornell J, Papadopoulos KP: Screen-ing for hepatocellular carcinoma among veterans with hepatitis C on disease stage, treatment received, and survival. Clin Gastroen-terol Hepatol 2007; 5: 508-512
21. Zhang BH, Yang BH, Tang ZY: Randomized controlled trial of screening for hepatocellular carcinoma. J Cancer Res Clin Oncol 2004; 130: 417-422
22. Wong LL, Limm WM, Severino R, Wong LM: Improved survival with screening for hepatocellular carcinoma. Liver Transpl 2000; 6: 320-325
23. Pateron D, Ganne N, Trinchet JC, Aurousseau MH, Mal F, Mei-cler C, Coderc E, Reboullet P, Beaugrand M: Prospective study of screening for hepatocellular carcinoma in Caucasian patients with cirrhosis. J Hepatol 1994; 20: 65-71
24. Chalasani N, Said A, Ness R, Hoen H, Lumeng L: Screening for hepatocellular carcinoma in patients with cirrhosis in the United States: results of a national survey. Am J Gastroenterol 1999; 94: 2224-2229
25. Kudo M, Okanoue T: Management of hepatocellular carcinoma in Japan: consensus-based clinical practice manual proposed by the Japan Society of Hepatology. Oncology 2007; 72 Suppl 1: 2-15
26. Patel D, Terrault NA, Yao FY, Bass NM, Ladabaum U: Cost-ef-fectiveness of hepatocellular carcinoma surveillance in patients
with hepatitis C virus-related cirrhosis. Clin Gastroenterol Hepatol 2005; 3: 75-84
27. Saab S, Ly D, Nieto J, Kanwal F, Lu D, Raman S, Amado R, Nuesse B, Durazo F, Han S, Farmer DG, Ghobrial RM, Yersiz H, Chen P, Schwegel K, Goldstein LI, Tong M, Busuttil RW: Hepato-cellular carcinoma screening in patients waiting for liver trans-plantation: a decision analytic model. Liver Transpl 2003; 9: 672-681
28. Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Bur-roughs AK, Christensen E, Pagliaro L, Colombo M, Rodes J: Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol 2001; 35: 421-430
29. Lim JH, Kim CK, Lee WJ, Park CK, Koh KC, Paik SW, Joh JW: Detection of hepatocellular carcinomas and dysplastic nodules in cirrhotic livers: accuracy of helical CT in transplant patients. AJR Am J Roentgenol 2000; 175: 693-698
30. Torzilli G, Minagawa M, Takayama T, Inoue K, Hui AM, Kubota K, Ohtomo K, Makuuchi M: Accurate preoperative evaluation of liver mass lesions without fine-needle biopsy. Hepatology 1999; 30: 889-893
31. Yu JS, Kim KW, Kim EK, Lee JT, Yoo HS: Contrast enhancement of small hepatocellular carcinoma: usefulness of three successive early image acquisitions during multiphase dynamic MR imaging. AJR Am J Roentgenol 1999; 173: 597-604
32. Hayashi M, Matsui O, Ueda K, Kawamori Y, Kadoya M, Yoshika-wa J, Gabata T, Takashima T, Nonomura A, Nakanuma Y: Corre-lation between the blood supply and grade of malignancy of hepa-tocellular nodules associated with liver cirrhosis: evaluation by CT during intraarterial injection of contrast medium. AJR Am J Roentgenol 1999; 172: 969-976
33. Fracanzani AL, Burdick L, Borzio M, Roncalli M, Bonelli N, Borzio F, Maraschi A, Fiorelli G, Fargion S: Contrast-enhanced Doppler ultrasonography in the diagnosis of hepatocellular carci-noma and premalignant lesions in patients with cirrhosis. Hepatol-ogy 2001; 34: 1109-1112
34. Gaiani S, Celli N, Piscaglia F, Cecilioni L, Losinno F, Giangrego-rio F, Mancini M, Pini P, Fornari F, Bolondi L: Usefulness of con-trast-enhanced perfusional sonography in the assessment of hepa-tocellular carcinoma hypervascular at spiral computed tomogra-phy. J Hepatol 2004; 41: 421-426
35. Numata K, Tanaka K, Kiba T, Saito S, Ikeda M, Hara K, Tanaka N, Morimoto M, Iwase S, Sekihara H: Contrast-enhanced, wide-band harmonic gray scale imaging of hepatocellular carcinoma: correlation with helical computed tomographic findings. J Ultra-sound Med 2001; 20: 89-98
36. Hammerstingl R, Zangos S, Schwarz W, Rosen T, Bechstein WO, Balzer T, Vogl TJ: Contrast-enhanced MRI of focal liver tumors using a hepatobiliary MR contrast agent: detection and differential diagnosis using Gd-EOB-DTPA-enhanced versus Gd-DTPA-en-hanced MRI in the same patient. Acad Radiol 2002; 9 Suppl 1: S119-120
37. Reimer P, Schneider G, Schima W: Hepatobiliary contrast agents for contrast-enhanced MRI of the liver: properties, clinical devel-opment and applications. Eur Radiol 2004; 14: 559-578
38. Shimizu M, Iijima H, Horibe T, Yamada M, Suzuki S, Yanagisawa K, Seki T, Moriyasu F: Usefulness of contrast-enhanced ultraso-nography with a new contrast mode, Agent Detection Imaging, in evaluating therapeutic response in hepatocellular carcinoma treat-ed with radio-frequency ablation therapy. Hepatol Res 2004; 29: 235-242
39. Akuta N, Suzuki F, Kawamura Y, Yatsuji H, Sezaki H, Suzuki Y, Hosaka T, Kobayashi M, Arase Y, Ikeda K, Kumada H: Amino acid substitutions in the hepatitis C virus core region are the im-portant predictor of hepatocarcinogenesis. Hepatology 2007; 46: 1357-1364
40. Cheung TK, Lai CL, Wong BC, Fung J, Yuen MF: Clinical fea-
Keio J Med 2009; 58 (3): 161-175 173
tures, biochemical parameters, and virological profiles of patients with hepatocellular carcinoma in Hong Kong. Aliment Pharmacol Ther 2006; 24: 573-583
41. Hung IF, Poon RT, Lai CL, Fung J, Fan ST, Yuen MF: Recurrence of hepatitis B-related hepatocellular carcinoma is associated with high viral load at the time of resection. Am J Gastroenterol 2008; 103: 1663-1673
42. Ohata K, Hamasaki K, Toriyama K, Ishikawa H, Nakao K, Eguchi K: High viral load is a risk factor for hepatocellular carcinoma in patients with chronic hepatitis B virus infection. J Gastroenterol Hepatol 2004; 19: 670-675
43. Yuen MF, Tanaka Y, Shinkai N, Poon RT, But DY, Fong DY, Fung J, Wong DK, Yuen JC, Mizokami M, Lai CL: Risk for hepatocel-lular carcinoma with respect to hepatitis B virus genotypes B/C, specific mutations of enhancer II/core promoter/precore regions and HBV DNA levels. Gut 2008; 57: 98-102
44. Larsson SC, Wolk A: Coffee consumption and risk of liver cancer: a meta-analysis. Gastroenterology 2007; 132: 1740-1745
45. Inoue M, Yoshimi I, Sobue T, Tsugane S: Influence of coffee drinking on subsequent risk of hepatocellular carcinoma: a pro-spective study in Japan. J Natl Cancer Inst 2005; 97: 293-300
46. Hu G, Tuomilehto J, Pukkala E, Hakulinen T, Antikainen R, Var-tiainen E, Jousilahti P: Joint effects of coffee consumption and se-rum gamma-glutamyltransferase on the risk of liver cancer. Hepa-tology 2008; 48: 129-136
47. Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ: Over-weight, obesity, and mortality from cancer in a prospectively stud-ied cohort of U.S. adults. N Engl J Med 2003; 348: 1625-1638
48. El-Serag HB, Rudolph KL: Hepatocellular carcinoma: epidemiol-ogy and molecular carcinogenesis. Gastroenterology 2007; 132: 2557-2576
49. Okuda K, Ohtsuki T, Obata H, Tomimatsu M, Okazaki N, Hasega-wa H, Nakajima Y, Ohnishi K: Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 pa-tients. Cancer 1985; 56: 918-928
50. Ramacciato G, Mercantini P, Cautero N, Corigliano N, Di Bene-detto F, Quintini C, Ercolani G, Varotti G, Ziparo V, Pinna AD: Prognostic evaluation of the new American Joint Committee on Cancer/International Union Against Cancer staging system for he-patocellular carcinoma: analysis of 112 cirrhotic patients resected for hepatocellular carcinoma. Ann Surg Oncol 2005; 12: 289-297
51. Varotti G, Ramacciato G, Ercolani G, Grazi GL, Vetrone G, Cescon M, Del Gaudio M, Ravaioli M, Ziparo V, Lauro A, Pinna A: Comparison between the fifth and sixth editions of the AJCC/UICC TNM staging systems for hepatocellular carcinoma: multi-centric study on 393 cirrhotic resected patients. Eur J Surg Oncol 2005; 31: 760-767
52. A new prognostic system for hepatocellular carcinoma: a retro-spective study of 435 patients: the Cancer of the Liver Italian Pro-gram (CLIP) investigators. Hepatology 1998; 28: 751-755
53. Ueno S, Tanabe G, Sako K, Hiwaki T, Hokotate H, Fukukura Y, Baba Y, Imamura Y, Aikou T: Discrimination value of the new western prognostic system (CLIP score) for hepatocellular carci-noma in 662 Japanese patients. Cancer of the Liver Italian Pro-gram. Hepatology 2001; 34: 529-534
54. Grieco A, Pompili M, Caminiti G, Miele L, Covino M, Alfei B, Rapaccini GL, Gasbarrini G: Prognostic factors for survival in pa-tients with early-intermediate hepatocellular carcinoma undergo-ing non-surgical therapy: comparison of Okuda, CLIP, and BCLC staging systems in a single Italian centre. Gut 2005; 54: 411-418
55. Marrero JA, Fontana RJ, Barrat A, Askari F, Conjeevaram HS, Su GL, Lok AS: Prognosis of hepatocellular carcinoma: comparison of 7 staging systems in an American cohort. Hepatology 2005; 41: 707-716
56. Sala M, Forner A, Varela M, Bruix J: Prognostic prediction in pa-tients with hepatocellular carcinoma. Semin Liver Dis 2005; 25: 171-180
57. Guglielmi A, Ruzzenente A, Pachera S, Valdegamberi A, Sandri M, D’Onofrio M, Iacono C: Comparison of seven staging systems in cirrhotic patients with hepatocellular carcinoma in a cohort of patients who underwent radiofrequency ablation with complete response. Am J Gastroenterol 2008; 103: 597-604
58. Leung TW, Tang AM, Zee B, Lau WY, Lai PB, Leung KL, Lau JT, Yu SC, Johnson PJ: Construction of the Chinese University Prognostic Index for hepatocellular carcinoma and comparison with the TNM staging system, the Okuda staging system, and the Cancer of the Liver Italian Program staging system: a study based on 926 patients. Cancer 2002; 94: 1760-1769
59. Chevret S, Trinchet JC, Mathieu D, Rached AA, Beaugrand M, Chastang C: A new prognostic classification for predicting surviv-al in patients with hepatocellular carcinoma. Groupe d’Etude et de Traitement du Carcinome Hepatocellulaire. J Hepatol 1999; 31: 133-141
60. Giannini E, Risso D, Botta F, Romagnoli P, Malfatti F, Fumagalli A, Testa E, Podesta E, Chiarbonello B, Polegato S, Testa R: Prog-nosis of hepatocellular carcinoma in anti-HCV positive cirrhotic patients: a single-centre comparison amongst four different stag-ing systems. J Intern Med 2004; 255: 399-408
61. Kudo M, Chung H, Haji S, Osaki Y, Oka H, Seki T, Kasugai H, Sasaki Y, Matsunaga T: Validation of a new prognostic staging system for hepatocellular carcinoma: the JIS score compared with the CLIP score. Hepatology 2004; 40: 1396-1405
62. Kudo M, Chung H, Osaki Y: Prognostic staging system for hepa-tocellular carcinoma (CLIP score): its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J Gastroenterol 2003; 38: 207-215
63. Nanashima A, Sumida Y, Morino S, Yamaguchi H, Tanaka K, Shi-basaki S, Ide N, Sawai T, Yasutake T, Nakagoe T, Nagayasu T: The Japanese integrated staging score using liver damage grade for hepatocellular carcinoma in patients after hepatectomy. Eur J Surg Oncol 2004; 30: 765-770
64. Luo KZ, Itamoto T, Amano H, Oshita A, Ushitora Y, Tanimoto Y, Ohdan H, Tashiro H, Asahara T: Comparative study of the Japan Integrated Stage (JIS) and modified JIS score as a predictor of survival after hepatectomy for hepatocellular carcinoma. J Gastro-enterol 2008; 43: 369-377
65. Bruix J, Castells A, Bosch J, Feu F, Fuster J, Garcia-Pagan JC, Visa J, Bru C, Rodes J: Surgical resection of hepatocellular carci-noma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenterology 1996; 111: 1018-1022
66. Livraghi T, Meloni F, Di Stasi M, Rolle E, Solbiati L, Tinelli C, Rossi S: Sustained complete response and complications rates af-ter radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: Is resection still the treatment of choice? Hepatology 2008; 47: 82-89
67. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Boz-zetti F, Montalto F, Ammatuna M, Morabito A, Gennari L: Liver transplantation for the treatment of small hepatocellular carcino-mas in patients with cirrhosis. N Engl J Med 1996; 334: 693-699
68. Yao FY, Kerlan RK, Jr., Hirose R, Davern TJ, 3rd, Bass NM, Feng S, Peters M, Terrault N, Freise CE, Ascher NL, Roberts JP: Excel-lent outcome following down-staging of hepatocellular carcinoma prior to liver transplantation: an intention-to-treat analysis. Hepa-tology 2008; 48: 819-827
69. Sergio A, Cristofori C, Cardin R, Pivetta G, Ragazzi R, Baldan A, Girardi L, Cillo U, Burra P, Giacomin A, Farinati F: Transcatheter arterial chemoembolization (TACE) in hepatocellular carcinoma (HCC): the role of angiogenesis and invasiveness. Am J Gastroen-terol 2008; 103: 914-921
70. Tamoxifen in treatment of hepatocellular carcinoma: a randomised controlled trial. CLIP Group (Cancer of the Liver Italian Pro-gramme). Lancet 1998; 352: 17-20
71. Castells A, Bruix J, Bru C, Ayuso C, Roca M, Boix L, Vilana R, Rodes J: Treatment of hepatocellular carcinoma with tamoxifen: a

174 Saito H, et al: HCC in Keio Affiliated Hospitals
double-blind placebo-controlled trial in 120 patients. Gastroenter-ology 1995; 109: 917-922
72. Farinati F: Tamoxifen treatment in hepatocellular carcinoma. Gas-troenterology 1996; 111: 272-274
73. Grimaldi C, Bleiberg H, Gay F, Messner M, Rougier P, Kok TC, Cirera L, Cervantes A, De Greve J, Paillot B, Buset M, Nitti D, Sahmoud T, Duez N, Wils J: Evaluation of antiandrogen therapy in unresectable hepatocellular carcinoma: results of a European Organization for Research and Treatment of Cancer multicentric double-blind trial. J Clin Oncol 1998; 16: 411-417
74. Llovet JM, Sala M, Castells L, Suarez Y, Vilana R, Bianchi L, Ay-uso C, Vargas V, Rodes J, Bruix J: Randomized controlled trial of interferon treatment for advanced hepatocellular carcinoma. Hep-atology 2000; 31: 54-58
75. Yuen MF, Poon RT, Lai CL, Fan ST, Lo CM, Wong KW, Wong WM, Wong BC: A randomized placebo-controlled study of long-acting octreotide for the treatment of advanced hepatocellular car-cinoma. Hepatology 2002; 36: 687-691
76. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, Schwartz M, Porta C, Zeuzem S, Bolondi L, Greten TF, Galle PR, Seitz JF, Borbath I, Haussinger D, Giannaris T, Shan M, Moscovici M, Voliotis D, Bruix J: Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008; 359: 378-390
77. Takeda A, Takahashi M, Kunieda E, Takeda T, Sanuki N, Koike Y, Atsukawa K, Ohashi T, Saito H, Shigematsu N, Kubo A: Hypo-fractionated stereotactic radiotherapy with and without transarteri-al chemoembolization for small hepatocellular carcinoma not eli-gible for other ablation therapies: Preliminary results for efficacy and toxicity. Hepatol Res 2008; 38: 60-69
78. Mayahara H, Oda Y, Kawaguchi A, Kagawa K, Murakami M, Hi-shikawa Y, Igaki H, Tokuuye K, Abe M: A case of hepatocellular carcinoma initially treated by carbon ions, followed by protons for marginal recurrence with portal thrombus. Radiat Med 2005; 23: 513-519
79. Ebinuma H, Saito H, Kosuga M, Wakabayashi K, Saito Y, Takagi T, Nakamoto N, Okuyama T, Ishii H: Reduction of c-myc expres-sion by an antisense approach under Cre/loxP switching induces apoptosis in human liver cancer cells. J Cell Physiol 2001; 188: 56-66
80. Kaneko F, Saito H, Saito Y, Wakabayashi K, Nakamoto N, Tada S, Suzuki H, Tsunematsu S, Kumagai N, Ishii H: Down-regulation of matrix-invasive potential of human liver cancer cells by type I in-terferon and a histone deacetylase inhibitor sodium butyrate. Int J Oncol 2004; 24: 837-845
81. Masuda T, Saito H, Kaneko F, Atsukawa K, Morita M, Inagaki H, Kumagai N, Tsuchimoto K, Ishii AH: Up-regulation of E-cadherin and I-catenin in human hepatocellular carcinoma cell lines by so-dium butyrate and interferon-alpha. In vitro Cell Dev Biol Anim 2000; 36: 387-394
82. Nakamura M, Saito H, Ebinuma H, Wakabayashi K, Saito Y, Tak-agi T, Nakamoto N, Ishii H: Reduction of telomerase activity in human liver cancer cells by a histone deacetylase inhibitor. J Cell Physiol 2001; 187: 392-401
83. Tada S, Saito H, Tsunematsu S, Ebinuma H, Wakabayashi K, Ma-suda T, Ishii H: Interferon regulatory factor-1 gene abnormality and loss of growth inhibitory effect of interferon-alpha in human hepatoma cell lines. Int J Oncol 1998; 13: 1207-1216
84. Wakabayashi K, Saito H, Kaneko F, Nakamoto N, Tada S, Hibi T: Gene expression associated with the decrease in malignant pheno-type of human liver cancer cells following stimulation with a his-tone deacetylase inhibitor. Int J Oncol 2005; 26: 233-239
85. Feun LG, O’Brien C, Molina E, Rodriguez M, Jeffers L, Schiff ER, Marini A, Savaraj N, Ardalan B: Recombinant leukocyte in-terferon, doxorubicin, and 5FUDR in patients with hepatocellular carcinoma-A phase II trial. J Cancer Res Clin Oncol 2003; 129: 17-20
86. Shiratori Y, Shiina S, Teratani T, Imamura M, Obi S, Sato S, Koike Y, Yoshida H, Omata M: Interferon therapy after tumor ab-lation improves prognosis in patients with hepatocellular carcino-ma associated with hepatitis C virus. Ann Intern Med 2003; 138: 299-306
87. Nussbaum T, Samarin J, Ehemann V, Bissinger M, Ryschich E, Khamidjanov A, Yu X, Gretz N, Schirmacher P, Breuhahn K: Au-tocrine insulin-like growth factor-II stimulation of tumor cell mi-gration is a progression step in human hepatocarcinogenesis. Hep-atology 2008; 48: 146-156
88. Thomas MB, Abbruzzese JL: Opportunities for targeted therapies in hepatocellular carcinoma. J Clin Oncol 2005; 23: 8093-8108
89. Furuta K, Sato S, Yamauchi T, Kakumu S: Changes in intrahepatic gene expression profiles from chronic hepatitis to hepatocellular carcinoma in patients with hepatitis C virus infection. Hepatol Res 2008; 38: 673-682
90. Knight B, Tirnitz-Parker JE, Olynyk JK: C-kit inhibition by ima-tinib mesylate attenuates progenitor cell expansion and inhibits liver tumor formation in mice. Gastroenterology 2008; 135: 969-979, 979 e1
91. Gonzalez-Carmona MA, Lukacs-Kornek V, Timmerman A, Sha-bani S, Kornek M, Vogt A, Yildiz Y, Sievers E, Schmidt-Wolf IG, Caselmann WH, Sauerbruch T, Schmitz V: CD40ligand-express-ing dendritic cells induce regression of hepatocellular carcinoma by activating innate and acquired immunity in vivo. Hepatology 2008; 48: 157-168
92. Hoshida Y, Villanueva A, Kobayashi M, Peix J, Chiang DY, Ca-margo A, Gupta S, Moore J, Wrobel MJ, Lerner J, Reich M, Chan JA, Glickman JN, Ikeda K, Hashimoto M, Watanabe G, Daidone MG, Roayaie S, Schwartz M, Thung S, Salvesen HB, Gabriel S, Mazzaferro V, Bruix J, Friedman SL, Kumada H, Llovet JM, Gol-ub TR: Gene expression in fixed tissues and outcome in hepato-cellular carcinoma. N Engl J Med 2008; 359: 1995-2004
93. Muto Y, Moriwaki H, Ninomiya M, Adachi S, Saito A, Takasaki KT, Tanaka T, Tsurumi K, Okuno M, Tomita E, Nakamura T, Ko-jima T: Prevention of second primary tumors by an acyclic reti-noid, polyprenoic acid, in patients with hepatocellular carcinoma. Hepatoma Prevention Study Group. N Engl J Med 1996; 334: 1561-1567
94. Muto Y, Moriwaki H, Saito A: Prevention of second primary tu-mors by an acyclic retinoid in patients with hepatocellular carci-noma. N Engl J Med 1999; 340: 1046-1047
95. Takai K, Okuno M, Yasuda I, Matsushima-Nishiwaki R, Uematsu T, Tsurumi H, Shiratori Y, Muto Y, Moriwaki H: Prevention of second primary tumors by an acyclic retinoid in patients with he-patocellular carcinoma. Updated analysis of the long-term follow-up data. Intervirology 2005; 48: 39-45
96. Muto Y, Sato S, Watanabe A, Moriwaki H, Suzuki K, Kato A, Kato M, Nakamura T, Higuchi K, Nishiguchi S, Kumada H, Ohashi Y: Overweight and obesity increase the risk for liver can-cer in patients with liver cirrhosis and long-term oral supplemen-tation with branched-chain amino acid granules inhibits liver car-cinogenesis in heavier patients with liver cirrhosis. Hepatol Res 2006; 35: 204-214
97. Mizuta T, Ozaki I, Eguchi Y, Yasutake T, Kawazoe S, Fujimoto K, Yamamoto K: The effect of menatetrenone, a vitamin K2 analog, on disease recurrence and survival in patients with hepatocellular carcinoma after curative treatment: a pilot study. Cancer 2006; 106: 867-872
98. Ikeda K, Arase Y, Saitoh S, Kobayashi M, Suzuki Y, Suzuki F, Tsubota A, Chayama K, Murashima N, Kumada H: Interferon beta prevents recurrence of hepatocellular carcinoma after complete resection or ablation of the primary tumor-A prospective random-ized study of hepatitis C virus-related liver cancer. Hepatology 2000; 32: 228-232
99. Liaw YF, Sung JJ, Chow WC, Farrell G, Lee CZ, Yuen H, Tan-wandee T, Tao QM, Shue K, Keene ON, Dixon JS, Gray DF, Sabbat

Keio J Med 2009; 58 (3): 161-175 175
J: Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med 2004; 351: 1521-1531
100. Matsumoto A, Tanaka E, Rokuhara A, Kiyosawa K, Kumada H, Omata M, Okita K, Hayashi N, Okanoue T, Iino S, Tanikawa K: Efficacy of lamivudine for preventing hepatocellular carcinoma in chronic hepatitis B: A multicenter retrospective study of 2795 pa-tients. Hepatol Res 2005; 32: 173-184
101. Mazzaferro V, Romito R, Schiavo M, Mariani L, Camerini T, Bhoori S, Capussotti L, Calise F, Pellicci R, Belli G, Tagger A, Colombo M, Bonino F, Majno P, Llovet JM: Prevention of hepa-tocellular carcinoma recurrence with alpha-interferon after liver resection in HCV cirrhosis. Hepatology 2006; 44: 1543-1554
102. Nishiguchi S, Kuroki T, Nakatani S, Morimoto H, Takeda T, Nak-ajima S, Shiomi S, Seki S, Kobayashi K, Otani S: Randomised tri-al of effects of interferon-alpha on incidence of hepatocellular carcinoma in chronic active hepatitis C with cirrhosis. Lancet 1995; 346: 1051-1055
103. Sato Y, Murase K, Kato J, Kobune M, Sato T, Kawano Y, Takimo-to R, Takada K, Miyanishi K, Matsunaga T, Takayama T, Niitsu Y: Resolution of liver cirrhosis using vitamin A-coupled liposomes to deliver siRNA against a collagen-specific chaperone. Nat Bio-technol 2008; 26: 431-442
104. Friedman SL: Targeting siRNA to arrest fibrosis. Nat Biotechnol 2008; 26: 399-400
105. Kagawa T, Morizane T, Saito H, Miyaguchi S, Tsunematsu S, Tada S, Guevara FM, Kumagai N, Tsuchimoto K, Watanabe T, et al: A randomized, controlled trial of weekly administration of lymphoblastoid interferon in patients with chronic hepatitis C. J Hepatol 1993; 17: 91-96
106. Saito H, Ebinuma H, Atsukawa K, Takahashi M, Masuda T, Ohi-shi T, Nojiri O, Mizuoka K, Ishii H: Disappearance of serum hep-atitis C virus RNA within two days after one dose interferon ad-ministration is predictive for response to high-dose interferon-al-pha 2b treatment for chronic hepatitis C. Keio Interferon-alpha 2b Study Group. Keio J Med 1997; 46: 74-80
107. Saito H, Ebinuma H, Nagata H, Inagaki Y, Saito Y, Wakabayashi K, Takagi T, Nakamura M, Katsura H, Oguchi Y, Ishii H: Interfer-on-associated retinopathy in a uniform regimen of natural interfer-on-alpha therapy for chronic hepatitis C. Liver 2001; 21: 192-197
108. Saito H, Ebinuma H, Satoh I, Miyaguchi S, Tada S, Iwabuchi N, Kumagai N, Tsuchimoto K, Morizane T, Ishii H: Immunological and virological predictors of outcome during interferon-alpha therapy of chronic hepatitis C. J Viral Hepat 2000; 7: 64-74
109. Saito H, Ishii H: Recent understanding of immunological aspects in alcoholic hepatitis. Hepatol Res 2004; 30: 193-198
110. Saito H, Tada S, Ebinuma H, Ishii H, Kashiwazaki K, Nishida J, Yoshida T, Zeki S, Yoshida H, Yoshioka M, Inagaki Y, Kumagai N, Hibi T: Induction therapy with twice-daily interferon-beta does not improve the therapeutic efficacy of consensus interferon monotherapy for chronic hepatitis C. Keio J Med 2006; 55: 111-117
111. Saito H, Tada S, Ebinuma H, Ishii H, Kashiwazaki K, Takahashi M, Tsukada N, Nishida J, Tanaka S, Shiozaki H, Hibi T: Role of erythrocytes as a reservoir for ribavirin and relationship with ad-verse reactions in the early phase of interferon combination thera-py for chronic hepatitis C virus infections. J Clin Microbiol 2006; 44: 3562-3568




















![EBCR Hepato Hery [Batas1]](https://img.pdfslide.net/doc/110x75/55cf9d32550346d033ac9f67/ebcr-hepato-hery-batas1.jpg)