Embed Size (px)
Citation preview

American Journal of Medica l Genetics 58:3%37 (1995)
Hereditary Disorders Among Iranian Jews
Joel Zlotogora Department of Human Genetics, Hadassah University Hospital, Hebrew University Medical School, Jerusalem, Israel
Iranian Jews represent an ancient com- munity with a very high degree of inbreed- ing. Although the community remained rel- atively isolated, it had strong ties with Babylonian Jewry in Iraq. Several genetic disorders have been reported to be frequent among Iranian Jews, in particular, cortico- sterone methyloxydase deficiency type 11, polyglandular syndrome, and rimmed vac- uole myopathy. Based on the data collected in our clinic, recessive and dominant deafness also appear to be frequent. Other diseases, such as P-thalassemia, achro- matopsia, colobomatous microphthalmia, Dubin-Johnson syndrome, and congenital myasthenia gravis, were frequent in both the Iranian and Iraqi Jewish communities.
The place of origin of the families within Iran and the results of molecular studies suggest some reason(s) for the high fre- quency of these disorders among Iranian Jews. While the high frequency of some of the disorders, such as corticosterone meth- yloxydase deficiency type 11, represents a founder effect, in other diseases (such as P-thalassemia) it was secondary to heterozy- gote advantage. @ 1995 Wiley-Liss, Inc.
KEY WORDS: founder effect, Iranian Jews, inbreeding, selection
INTRODUCTION Jews have lived throughout Persia for centuries. To-
day there is still a small Jewish community in Iran, but many of the Jews have left the country, mostly for Israel. The Iranian Jewish community includes 135,000 indi- viduals and represents about 3.5% of the Jewish popu- lation in Israel [Central Bureau of Statistics, 19931. Although the Iranian Jewish community was relatively isolated, it had strong ties with Babylonian Jewry in
Received for publication August 1, 1994; revision received Feb- ruary 1, 1995.
Address reprint requests to Joel Zlotogora, M.D., Department of Human Genetics, Hadassah Hospital, P.O.B. 12000, Jerusalem 91120, Israel.
0 1995 Wiley-Liss, Inc.
Iraq. Several rare genetic diseases have been reported to be relatively frequent in both communities, while some genetic disorders were found to be frequent in only one of the communities (Table I). The Iranian Jewish com- munity is known for a very high degree of inbreeding; in a sample of 164 unrelated individuals, 24.4% were off- spring of consanguineous marriages [Cohen et al., 19811. While marriages with members of other Jewish commu- nities are becoming more frequent, it still appears that the preference is for marriage within the community and, relatively often, within the family.
Many of the disorders present in the Iranian Jewish community have only recently been delineated; this survey summarizes our experience on these disorders.
MATERIALS AND METHODS For a survey of genetic disorders among Iranian
Jews, the files of most of the individuals who had 4 grandparents of Jewish Iranian origin were collected from the Genetics Clinic of Hadassah Medical Center. This clinic is unique in Jerusalem, and therefore all the families from the region are referred to it for counseling and prenatal diagnosis. In addition, many patients are referred from throughout the country to the clinic or to specialists from the hospital, who then sometimes refer the patients to the clinic. The survey includes all the files of consultants who visited our clinic since its open- ing in 1964.
RESULTS In 342 of 11,000 successive files from the clinic (3%),
1 (96 files) or 2 individuals (246 files) had 4 Iranian Jew- ish grandparents. Premarital counseling was one of the main reasons for genetic counseling (59 files), most often since the consultants were consanguineous (41 files).
In 127 files, a monogenic disorder was present in the propositus or hisher family. In 62 families, the disorder was one of those known to be relatively frequent among Iranian Jews: achromatopsia (6 families), anencephaly (17 families), colobomatous microphthalmia (5 fami- lies), corticosterone methyloxydase I1 deficiency (10 families), Dubin-Johnson syndrome (2 families), famil- ial hemophagocytic lymphohistiocytosis (1 family), myasthenia gravis (4 families), rimmed vacuole myopa- thy (5 families), polyglandular syndrome (10 families), and P-thalassemia (2 families). Hereditary deafness was relatively common: autosomal-recessive in 6 fami- lies, and autosomal-dominant in 6 other families. Other rare monogenic disorders were diagnosed in 38 fami-

Hereditary Disorders of Iranian Jews
TABLE I. Genetic Disorders Which Have Been Reported as Frequent Among Jewish Families Originating From Iran and/or Iraq*
Origin and number of Jewish families
33
Disorder Iran Iraq Iranian Jews only Corticosterone methyloxydase I1 deficiency Polyglandular syndrome Vacuolar myopathy
Iranian and Iraqi Jews Dubin-Johnson syndrome Achromatopsia
Congenital myasthenia gravis Microphthalmos with coloboma
Laron dwarfism FHLH Pseudocholinesterase deficiency P-thalassemia G6PD deficiency
Iraqi Jews only Thrombasthenia Behr syndrome
11 22 19 i- 3"
34 + 1" 6
9 5
5 3
Frequent Frequent Frequent
6 2
7 1
8 1
Frequent Frequent Frequent
17 25
Other origin
6 Morocco + others 7 Morocco, 2 Tunisia, 1 Lebanon
5 (Turkey,Syria, Kurdistan)
2 Yemen
Kurdistan Kurdistan Kurdistan
1 Lebanon
*The numbers are those of unrelated families reported in the literature and/or known to us with the dis- order. "Probably of Iranian origin.
lies: autosomal-recessive (27 families), autosomal- dominant (10 families), and X-linked (1 family). In 15 additional families, an undelineated autosomal- recessive disorder was present.
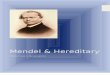
We noted the place of origin within Iran of families in which there was no monogenic disorder, since these families represent a relatively random sample of the community (Fig. 1); 18% of the families in which the place of origin was known were from the Iranian part of Kurdistan. Among the non-Kurdish Iranian Jews, 29% originated from Isfahan, 22% from Yezd, 8% from Teheran, 6% from Shiraz, and 5% from Hamadan; the others were from smaller communities.
DISCUSSION Hereditary Disorders Frequent
Among Iranian Jews In the analysis of disorders which have been reported
to be relatively frequent among Iranian Jews we dis- tinguished between two groups: those present in Iran- ian Jews only, and those present in high frequency in Iranian and Iraqi Jews (Table I).
Disorders Found in High Frequency, Apparently in Iranian Jews Only
Three diseases belong to this group and have been re- ported to be frequent only among Iranian Jews: corti- costerone methyloxydase I1 deficiency, polyglandular syndrome, and rimmed vacuole myopathy.
Corticosterone methyloxydase 11 deficiency, MIM 203040 [Cohen et al., 1977; Pascoe et al., 19921. This condition may present with a very wide range of severity. The most severely affected patients usually
present with dehydration in the first weeks of life; the clinical symptoms may resemble Addison crisis and, if untreated, the infant may die. The children with less severe disease tend to present with failure to thrive or growth retardation. Other patients may be apparently asymptomatic; however, history of postural hypoten- sion, weakness, or salt craving may be obtained. In some patients short stature is evident. The disease is characterized by an elevated ratio of 18-hydroxycorti- sonelaldosterone in the serum, and is caused by the de- ficiency of the enzyme corticosterone methyloxydase 11. The genes CYPllBl and CYPllB2 encode, respectively, P450XlB1 and P450XlB2, two cytochrome isozymes in- volved in the enzymatic function of the corticosterone methyloxydase 11.
Polyglandular deficiency syndrome, MIM 263620 [Zlotogora and Shapiro, 19921. Polyglandular de- ficiency syndrome is characterized by hypoparathy- roidism, adrenal insufficiency, and chronic mucocu- taneous candidiasis, but none of the components are constant. Occasionally symptoms of other immune dis- orders are present, such as pernicious anemia, alope- cia, or gonadal failure. Most Iranian Jewish patients present with hypoparathyroidism, which may remain the only manifestation of the syndrome. The disor- der has been also reported with a very high incidence in Finland. While in Finnish patients chronic muco- cutaneous candidiasis is seen in almost every patient, it was rarely observed among the Iranian Jewish patients.
Rimmed vacuole myopathy [Argov and Yarom, 1984; Sadeh et al., 19931. Muscular weakness usu- ally appears in the third decade as gait difficulties. The

34 Zlotogora
I IRAQ c
Fig. 1. Map of Iran, showing principal towns in which Jews have been living
progression is gradual, and most patients become severely incapacitated a decade after onset. Ocular, pharyngeal, and cardiac muscles are not involved. The muscles of the shoulder girdle are severely affected in advanced cases, with relative sparing of the deltoid, biceps, and triceps. In the lower limbs, foot dorsiflexion is usually very weak at an early stage of the disease. When leg muscle weakness become widespread, the most characteristic finding becomes evident: sparing of the quadriceps. The quadriceps stay strong even in ad- vanced stages of the disorder, and this allows patients to stand and walk till late in the course of the disease. CK (creatine kinase) levels are normal or moderately elevated, and the conduction velocity is normal. In the muscle biopsy many fibers contain clefts or round vac- uoles rimmed by granular material which stain ba- sophilic on hematoxylin and eosin.
Disorders Found in High Frequency in Jews From Iran and Iraq
Some of the disorders such as thalassemia and GGPD deficiency were found to be particularly frequent in Kurdistan, which includes Jewish communities in Iran, Iraq, and Turkey. An estimated carrier frequency of P-thalassemia in Kurdish Jews is 15-20%. GGPD de- ficiency is also very frequent, with an estimated fre- quency of 1:7 males [Goodman, 19791.
Another very common disorder in Jews from Iran and Iraq is pseudocholinesterase deficiency, MIM 177400. Individuals with pseudocholinesterase deficiency are healthy, but when they are treated with the muscle relaxant succinylcholine, there is a prolonged paralysis instead of the short effects of the drug. This is due to a mutation in the enzyme butyrylcholinesterase, which usually has a spectrum broader than that of cholinesterase.
Congenital achromutopsia, MIM 21 6900 (total color blindness). Affected individuals have poor vi- sual acuity, photophobia, congenital nystagmus, and color blindness. Photophobia is striking, even in light of ordinary intensity. Vision in ordinary light is severely restricted, and relatively better in dim light. The fundus appears normal. The disorder is stationary, and very little change in clinical appearance and visual function are noted with time, except for some improvement in the nystagmus and possibly in the photophobia.
The autosomal-recessive form of the disease seems to be very rare, but it is relatively frequent among the Moroccan, Iraqi, and Iranian Jews [Zlotogora and Merin, unpublished observations].
Anencephaly, autosomal-recessive form, MIM 206500 [Zlotogora, 19951. Among families originat- ing in Iran and or IranAraq, anencephaly is the most prevalent neural tube defect. Together with high preva- lence, the distribution of different types of neural tube defects in these communities and the sex ratio of the anencephalic children suggest the existence of a major autosomal-recessive gene responsible for anencephaly in this community.
Colobomatous microphthalmia, MIM 251600 [Zlotogora et al., 19941. Colobomatous microph- thalmia has been reported as an autosomal-recessive disorder in Jews mainly from Iran and Iraq, including Kurdistan. Significant phenotypic variability exists in the severity of autosomal-recessive colobomatous microphthalmia. Some patients have a relatively mild unilateral defect, and other have a severe bilateral de- fect which may lead t o complete blindness.
Dubin-Johnson syndrome, MIM 237500 (hyper- bilirubinemia II) [Shani et al., 29701. Chronic or intermittent jaundice is the most common finding in pa- tients with Dubin-Johnson syndrome. Onset has been

Hereditary Disorders of Iranian Jews 35
Some of the classical recessive diseases are rare among Iranian Jews. For instance, cystic fibrosis has been diagnosed in Israel only in 1 Iranian Jewish pa- tient, and its incidence in this community was calcu- lated to be 1:39,000 [Kalman, 19941. Only one lyso- soma1 storage disease (Pompe disease) was diagnosed in 1 family of Iranian Jews. Since the Department of Human Genetics is the referral center for lysosomal storage diseases in Israel, we presume that they seldom occur among Iranian Jews.
Molecular Analysis of Diseases Known to be Frequent Among Iranian Jews
pthalassemia. Five mutations were found among the Iranian Kurdish Jewish P-thalassemia patients, 4 of which have been characterized. One mutation, “nonsense 39,” which is relatively frequent in Iranian Kurdish Jews (7112 alleles examined), was found in only 1 of 59 mutant alleles from Iraqi Kurdish Jews. The 4 other mutations are rare: “frameshift 36137” was found in 2 alleles, and each of the other mutations was found in only 1 allele. None of these 4 mutations were found in other Kurdish Jews [Rund et al., 19911.
In a relatively small sample of GGPD-deficient Jewish individuals from Kurdistan, the G6PD Mediterranean mutation was prevalent. It was found in 87% of the males examined (718 males), and in a t least 79% of the females carriers (13 females carriers or homozygotes) [Oppenheim et al., 19931.
Pseudocholinesterase deficiency. This disorder is caused by a mutation in the butyrylcholinesterase gene. The mutation D70G is present, with a very high frequency in Jews from Iran (7%) and Iraq (5%) [Neville et al., 19901.
Corticosterone methyloxydase II deficiency. In Iranian Jews this disease is due to a mutation in the gene CYP11B2. All the Iranian Jewish patients exam- ined were homozygous for two different mutations, R181W, which reduces the 18 hydroxylase activity but leaves the llp-hydroxylase intact, and V386A, which causes a small reduction in the production of 18-hydro- corticosterone [Pascoe et al., 19921. Some healthy indi- viduals from patients’ families were found to be ho- mozygous for one or the other mutation. Therefore, each mutation is insufficient to produce a disease state. Both mutations seem to be frequent among the Iranian Jews, but have not been the subject of systematic screening.
Laron dwarfism. Molecular analysis was per- formed in only 2 of the Iraqi Jewish patients. Both were homozygous for a deletion of a large portion of the extracellular hormone-binding domain of the human growth hormone receptor [Godowski et al., 19891. To our knowledge there are no data on patients of Jewish Iranian origin.
Origin of Families of Patients With Disorders Found in High Frequency in Iranian Jews
Jews have been living in Persia for centuries; the first concrete figures appeared in the 12th century, when some 30,000 Jews lived in Hamadan, 15,000 in Isfahan, and 10,000 in Shiraz, while other Jews lived in many smaller communities [Roth, 19721. Later, during the
G6PD deficiency.
observed in infancy or late adulthood, but generally oc- curs between ages 15-35 years. Some of the patients have bleeding symptoms which may be attributed to a deficiency or decreased levels of factor VII, as found in higher frequency among patients with Dubin-Johnson syndrome than in the general population.
The disease has been reported to be relatively fre- quent in Jews from Iran, Iraq, and Morocco, while it is rare in other Jewish communities.
Congenital familial myasthenia gravis, MIM 254210 [Goldhammer et al., 19901. The most com- mon manifestations are ptosis, and limited facial ex- pression with a myopathic appearance, together with mandibular prognathism, malocclusion, and open bite. Facial muscular weakness is always present with bilat- eral ptosis, but without ophthalmoplegia. Many pa- tients have weak masticatory muscles and are easily fatigued after prolonged speech. Limb involvement is mild, and there is almost no progression with the years. All patients reported have a positive Tensilon test and show some improvement with pyridostigmine.
Laron dwarfism, MIM 262500 (pituitary dwarf- ism II) [Adam et al., 19811. While birth weight is usually normal in patients, length at birth is short. From early infancy the children grow slowly. Onset of dentition is late and defective; the teeth are often dis- colored. The genitalia are small, but the patients reach sexual maturity and are able to reproduce. Almost all patients demonstrate some degree of mental retarda- tion. This form of the syndrome is associated with defective growth hormone receptors.
Familial hemophagocytic lymphohistiocytosis (FHLH) [Stark et al., 19841. FHLH, which occurs in infants and young children, is characterized by a fatal, deteriorating course marked by fever, hepato- splenomegaly, frequent nervous system involvement, and sometimes lymphadenopathy or skin rash. FHLH, which is a very rare disorder, has been reported in 3 Iranian Jewish families, and in 1 from Iraq.
Other Inherited Disorders Among Jews From Iran
Hereditary deafness was relatively frequent among Iranian Jewish families attending our clinic. Autoso- mal-recessive deafness was present in 6 families, and it may have been the cause in many of the isolated cases. These families originated from various places in Iran.
In 6 other families, deafness was dominant; otoscle- rosis was diagnosed in 2 of these. In the other 4 fami- lies, deafness was sensorineural and relatively mild with late onset. This represents a particularly high in- cidence of a disorder considered to be very rare. It may be that the disease is due to a common founder, even though these large families were unrelated and origi- nated from different parts of Iran.
In addition, 27 different, rare autosomal-recessive diseases have been diagnosed among the Iranian Jews in our clinic, and 15 other disorders still remain unde- lineated. Most of these recessive disorders were present in families in which the parents were consanguineous (28142 families).

36 Zlotogora
Safawid dynasty, Isfahan became the capital of the Per- sian empire, and it included the leading Jewish commu- nity. In addition, many Jews remained dispersed in var- ious communities in Iran. In the 1930’s, many Jews immigrated to larger towns such as Teheran (which became the capital of modern Iran), Yezd, and Isfahan. Since there are no written personal family records, most of the Jewish families living nowadays do not know their ancient origin. As for the families attending our clinic, most originated from Isfahan; other common places of origin were Yezd, Teheran, Shiraz, and Hamadan, or from the Kurdish part of Iran (Fig. 1).
In cases of corticosterone methyloxydase I1 deficiency and rimmed vacuole myopathy, almost all the families originated from Isfahan. In some of the families both diseases were transmitted from an affected parent to some of the children. These observations are probably the consequence of the high frequency of the disorders in the Isfahan community, which was relatively iso- lated, and in which the degree of consanguinity was very high. It is probable that the mutation(s) which causes corticosterone methyloxydase I1 deficiency and rimmed vacuole myopathy has not yet spread to the whole Iranian Jewish community.
Congenital myasthenia gravis is another disease in which all affected Iranian Jewish families known to us originated from Isfahan; however, other cases origi- nated from Iraq. Therefore, the founder may have been from Isfahan, and later, a carrier of the mutation may have migrated to Iraq. Another possibility is that the mutation first occurred in Iraq, and later a carrier founded a family in Isfahan.
In the autosomal-recessive form of microphthalmos with coloboma, 3 of the 5 Iranian Jewish families orig- inated from Yezd, a relatively small Jewish community, thus suggesting this town as the origin of the founder in Iran.
As for polyglandular deficiency syndrome, achro- matopsia, and Dubin-Johnson syndrome, the families originated from various parts of Iran. These observa- tions suggest that the mutations occurred a long time ago and spread within and outside the community.
Why Are Many Hereditary Disorders Frequent Among Iranian Jews?
A high frequency of hereditary diseases has been re- ported in many isolated communities, such as among the Hutterites, Amish people, Finns, French Canadi- ans, and Ashkenazi Jews. In many cases, genealogical studies demonstrated a common origin for the carriers, and a founder effect together with genetic drift was proposed to explain the high frequency of the disorders [Diamond and Rotter, 19871. Molecular studies have demonstrated that a common mutation is often respon- sible for the high frequency of a disorder within the population. In corticosterone methyloxydase I1 defi- ciency among the Iranian Jews, all the affected pa- tients were homozygous for two mutations in the gene CYPllB, an observation which is in accordance with the existence of a common founder for all the patients.
Another possible explanation for the high frequency of hereditary disorders may be a selection in favor of
the carriers. This was proven for sickle cell anemia in Africa, and is the probable explanation for the high fre- quency of thalassemia in various parts of the world. In the Mediterranean countries where p-thalassemia is frequent, more than one frequent mutation was found to be present in the population. Among Jews from Iran- ian Kurdistan, 5 different mutations explain the high frequency of the disease, a finding which is in accor- dance with a selective advantage for carriers of the dis- ease, The observation that the mutations are different from those found in other Kurdish Jewish communities confirms the relative isolation of the Iranian Kurds [Rund et al., 19911. Similarly, the high frequency of GGPD deficiency among Jews in Kurdistan is thought to be due to a selective advantage against malaria. However, the preliminary molecular studies in this population demonstrated that only one major muta- tion, GGPD Mediterranean, is frequent, and therefore it was suggested that a founder effect may have played a significant role [Oppenheim et al., 19931.
A selective advantage has been also proposed to ex- plain the very high incidence of pseudocholinesterase deficiency in Jews from Iran and Iraq. It may be that this advantage is related to the high contents of sola- nine-derived glycoalkaloids in various products such as eggplant, which were a major part of the diet of Jews from the area. These glycoalkaloids are potent in- hibitors of the common, but not of the G70G, butyryl- cholinesterase allele, which is frequent among Iranian and Iraqi Jews. Therefore, carriers of the mutation un- der such a diet have an advantage since they still have a functional cholinesterase [Neville et al., 19921.
The Iranian and Iraqi Jewish communities are closely related, historically and geographically. The Iraqi Jewish community is nowadays twice the size of the Iranian community. There is a similar high consan- guinity rate in the two communities, and rare autoso- mal-recessive disorders have also been found in Iraqi Jews, with an increased frequency for disorders such as Behr syndrome with 3-methylglutaconic aciduria [Elpeleg et al., 19941 and thrombasthenia [Seligsohn and Rososhansky, 19841 (Table I). The finding of disor- ders common to both communities is probably due to different reasons. One is a common selective advantage in disorders such as P-thalassemia, GGPD deficiency, and most probably pseudocholinesterase deficiency. Another may be a common founder in diseases such as Dubin-Johnson syndrome or Laron dwarfism.
Further studies of inherited disorders in the Iranian Jewish community will be important, and in particular for mapping the genes involved. Molecular studies will allow a determination of the carrier frequency of these disorders, and perhaps a better understanding of the reasons for their high frequency.
REFERENCES Adam A, Josefsberg Z, Pertzelan A, Zadik Z, Chemke JM, Laron Z
(1981): Occurrence of four types of growth hormone related dwarfism in Israeli communities. Eur J Pediatr 137:35-39.
Argov Z, Yarom R (1984): “Rimmed vacuole myopathy” sparing the quadriceps. A unique disorder in Iranian Jews. J Neurol Sci 64:3344.
Central Bureau of Statistics (1993): Statistical Abstracts of Israel. Jerusalem.

Hereditary Disorders of Iranian Jews 37
Oppenheim A, Jury CL, Rund D, Vulliamiamy TJ, Luzzatto L (1993): G6PD Mediterranean accounts for the high prevalence of G6PD deficiency in Kurdish Jews. Hum Genet 91:293-294.
Pascoe L, Curnow KM, Slutsker L, Rosler A, White PC (1992): Muta- tions in the human CYF’11B2 (aldosterone synthetase) gene caus- ing corticosterone methyloxydase I1 deficiency. Proc Natl Acad Sci USA 89:4996-5000.
Roth HH Jr (ed) (1972): “Encyclopedia Judaica” (Jerusalem: Keteri,
Rund D, Cohen T, Filon D, Dowling CE, Warren TC, Barak I, Rachmilewitz E, Kazazian HH, Oppenheim A (1991): Evolution of a genetic disease in an ethnic isolate: P-thalassemia in the Jews of Kurdistan. Proc Natl Acad Sci USA 88:310-314.
Sadeh M, Gadoth N, Hadar H, Ben-David E (1993): Vacuolar myopa- thy sparing the quadriceps. Brain 116:217-232.
Seligsohn U, Rososhansky S (1984): A Glanzmann’s thrombasthenia cluster among Iraqi Jews in Israel. Thromb Haemostas 52:230-231.
Shani M, Seligsohn U, Gilon E, Sheba C , Adams A (1970): Dubin- Johnson syndrome in Israel. I. Clinical laboratory and genetics as- pects. Q J Med 39:349-358.
Stark B, Hershko H, Rosen N, Cividalli G, Karshai H, Soffer D (1984): Familial hemophagocytic lymphohistiocytosis (FHLH) in Israel. 1. Description of 11 patients of Iranian-Iraqi origin and review of the literature. Cancer 54:2109-2121.
Zlotogora J (1995): A major gene is responsible for anencephaly among Iranian Jews. Am J Med Genet 5687-89.
Zlotogora J, Shapiro MS (1992): Polyglandular autoimmune syndrome type I among Iranian Jews. J Med Genet 29:834-836.
Zlotogora J, Legum C, Raz J, Merin S, BenEzra D (1994): Autosomal recessive microphthalmos with colobomatous malformations. Am J Med Genet 49:261-262.
Vol. 13. pp 302-320.
Cohen T, Theodor R, Rosler A (1977): Selective hypoaldosteronism in Iranian Jews: a n autosomal recessive trait. Clin Genet 11:25-30.
Cohen T, Simhai B, Steinberg AG, Levene C (1981): Genetic polymor- phisms among Iranian Jews in Israel. Am J Med Genet 8:180-191.
Diamond JM, Rotter J I (1987): Observing the founder effect in human evolution. Nature 329:105-106.
Elpeleg ON, Costeff H, Joseph A, Shental Y, Weitz R, Gibson KM (1994): 3-methylglutaconic aciduria in the Iraqi-Jewish optic atro- phy plus (Costeffl syndrome. Dev Med Child Neurol36:167-172.
Godowski PJ, Leung DW, Meacham LR, Galgani JP , Hellmiss R, Keret R, Rotwein PS, Parks JS, Laron Z, Wood WI (1989): Charac- terization of the human growth hormone receptor gene and demon- stration of a partial gene deletion in two patients with Laron- dwarfism. Proc Natl Acad Sci USA 86:8083-8087.
Goldhammer Y, Blatt I, Sadeh M, Goodman RM (1990): Congenital myasthenia associated with facial malformations in Iraqi and Iranian Jews. A new genetic syndrome. Brain 113:1291-1306.
Goodman RM (1979): “Genetic Disorders Among the Jewish People.” Baltimore and London: The Johns Hopkins University Press, pp 163-170.
Kalman YM (1994): Genetic heterogeneity in diseases: the long QT syndrome and cystic fibrosis. M.S. thesis, Hebrew University, Jerusalem.
Neville LF, Gnatt A, Padan R, Seidman S, Soreq H (1990): Anionic site interactions in human butyrylcholinesterase disrupted by two adjacent single point mutations. J Biol Chem 26520735-20738.
Neville LF, Gnatt A, Loewenstein Y, Seidman S, Ehrlich G, Soreq H (1992): Intramolecular relationships in cholinesterases revealed by oocyte expression of site-directed and natural variants of human BCHE. EMBO J 11:1641-1649.