Embed Size (px)
Citation preview

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Got Sepsis? Camille Hernandez ACNP/FNP
Objectives
• Explore epidemiology and pathogenesis of sepsis
• Define and discuss classifications of sepsis
• Examine latest therapies and recommendations for treatment
• Review current literature and research
Sepsis is not a Disease
Sepsis is a complex infection-induced syndrome creating a systemic inflammatory response
that potentially results in organ dysfunction, widespread inflammation, and microvascular
coagulopathies.
Sepsis Guidelines 10/7/2010
Critical Care Education Series
Germ History
• 2735 BC Chinese Emperor Sheng Nung records the use of herbal remedy for the treatment of fever
• 1546 Hieronymus Fracastorius suggests the germ theory
• 1879 Louis Pasteur identifies Streptococcus bacteria as the cause of puerperal sepsis
• 1928 Alexander Fleming recognizes that his bacterial cultures were killed by a blue mold Penicillin
Sepsis Facts
• Leading cause of morbidity and mortality for ICU admits
• Mortality rate of 29-50%, MODS mortality rate is as high as 85%
• 13th most common cause of death in the USA
• Severe sepsis causes approximately 215,000 deaths each year in the USA
• Accounts for 9.3% of all deaths in the USA
• Marked increase in the last 15 years
• Rivals myocardial infarction as modifiable cause of mortality in USA
Co$t of $epsis
• Approximately 17 Billion dollars annually • Increases associated patients hospital stay by 7.4-9.4 days • Cost of a nosocomial infection on average $13,973

Sepsis Guidelines 10/7/2010
Critical Care Education Series
American College of Chest Physicians (ACCP)/Society of Critical Care Medicine (SCCM)
* Sepsis Inflammatory Response Syndrome (SIRS) * Severe Sepsis * Septic Shock * Multiple Organ Dysfunction Syndrome (MODS)
Systemic inflammatory response syndrome (SIRS)
Manifests by 2 or more of the following conditions:
• Temperature greater than 38°C or less than 36°C
• Heart rate greater than 90 beats per minute
• Respiratory rate greater than 20 breaths per minute or PaCO2 less than 32 mm Hg
• White blood cell count greater than 12,000/mL, less than 4000/mL, or 10% immature (band) forms
Sepsis
Presence of an infectious process + SIRS, two of the following…
• Temperature greater than 38°C or less than
36°C
• Heart rate greater than 90 beats per minute
• Respiratory rate greater than 20 breaths per minute or PaCO2 less than 32 mm Hg
• White blood cell count greater than 12,000/mL, less than 4000/mL, or 10% immature (band) forms
Sepsis Guidelines 10/7/2010
Critical Care Education Series
Severe Sepsis
Sepsis and/or SIRS associated with >1 organ dysfunction,
hypo-perfusion, and hypotension that may include:
• Alteration in mental state
• Hypoxemia (PaO2 <72 mm Hg at FiO2 0.21)
• Elevated plasma lactate level
• Oliguria (output <30 mL or 0.5 mL/kg for at least 1 hr)
Septic Shock
SIRS and/or Severe Sepsis associated with organ dysfunction, hypo-perfusion and…
• Sepsis-induced hypotension
systolic blood pressure <90 mm Hg or a reduction of >40 mm Hg from baseline despite adequate fluid resuscitation
MODS
Multiple organ dysfunction syndrome (MODS):
This is the presence of (multiple >2) altered organ function in a patient who is acutely ill and in whom homeostasis cannot be maintained without intervention.

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Criteria for Acute Organ dysfunction
Cardiovascular SBP <90mmHg or MAP <65 for > 1 hour despite adequate fluid resuscitation or pressor support
Renal Urine output <0.5ml/kg for 1 hour despite adequate fluid resuscitation
Respiratory PaO2/FiO2 ratio <200
Hematologic Platelets <80,000/mm or 50% decrease in preceding 3 days
Metabolic Acidosis (unexplained)
pH <7.3 or Lactate 2.0
Pathophysiology of Sepsis
Pathogenesis of Septic Shock…
Invading Pathogen
Exo/Endotoxins induce WBC’s monocytes & macrophages (phagocytosis)
Inflammation = cytokine mediated pro-inflammatory
response
Activation of the complement cascade leads to release of inflammatory mediators proteases and oxygen free
radicals.
This leads to localized tissue damage and increased capillary permeability.
Phagocytosis
White Blood Cell engulfing yeast
Sepsis Guidelines 10/7/2010
Critical Care Education Series
Cytokines & Toll receptors
• Tumor necrosis factor (TNF) • Serum procalcitonin (PCT) • C-reactive protein (CRP) • Interleukin factors (IL-2, IL-6, IL-8, IL-10) Cytokines (tumor necrosis factor-alfa, interleukins,
interferon-y) exert multiple effects causing endothelial injury
Cell necrosis / Hypoxia / Ischemia / Acidosis Toll-like Receptors are the “alarmist” proteins
signaling immune response in your myeloid cells
Pathophysiology Sepsis
The endothelium is the thin layer of cells that line the interior surface of blood vessels, forming an interface between circulating blood in the lumen and the rest of the vessel wall. Endothelial cells line the entire circulatory system, from the heart to the smallest capillary.
The endothelium is an organ which regulates
• Blood vessel tone • Vascular permeability • Coagulation • Angiogenesis (growth of new blood vessels) • White blood cell and platelet activity • Phagocytosis (digestion) of bacteria
The endothelium produces a number of vasoactive substances like:
Nitric Oxide (potent vasodilator) Endothelin 1 (potent vasoconstrictor)

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Process of microcirculatory failure in shock:
Stage 1: COMPENSATION
• The pre capillary arterioles and post capillary venules vasoconstrict: this helps maintain systemic blood pressure
• increased hydrostatic pressure in the capillaries • consequently fluid is "sucked" / sequestered from the
interstitium • This is known as "trans capillary refill" • This leads to restoration of circulating volume, along
with the renin-angiotensin-aldosterone axis.
Stage 2: DECOMPENSATION
• The accumulation of hydrogen ions, lactic acid, increased PaCO2 & vasoactive substances, occurs.
• precapillary sphincters relax & post capillary venules become unresponsive and vasoconstrict
• blood "sieves" out of the capillary bed (increased capillary permeability in sepsis)
• interstitial edema / hemoconcentration / increased blood viscosity
• Intravascular dehydration results
Stage 3: MODS (curtains)
Organ dysfunction: • The brain and kidneys are normally protected
from swings in blood pressure by autoregulation
• In early sepsis - autoregulation curve shifts (due to and increase in sympathetic tone)
• In late sepsis - vasoparesis occurs then autoregulation fails
• "steal phenomena" may occur (areas of ischemia may have their blood stolen by areas with good perfusion)

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Procoagulant effects
• viscosity + decreased flow + platelet activation + clot formation in the
capillary bed = Microemboli formation • release of tissue thromboplastin + triggering of intrinsic pathway • consumption of clotting factors and
abnormal bleeding Clot Breakdown = DIC (disseminated intravascular
coagulation)
END RESULT
Leaky alveolar membranes and pulmonary alveolar
capillary damage….ARDS Systemic vasodilation and diminished myocardial
contractility…Hypotension Activates intrinsic and extrinsic pathways of the
coagulation system….DIC Vasodilatation
Delayed Capillary refill Myocardial depression Activation of clotting systems
What Sepsis looks like from the top down:
CNS • Confusion / stupor / coma secondary to: • Hypo-perfusion injury • Septic encephalopathy • Metabolic encephalopathy
Metabolic • Hyperglycemia due to sepsis &
catecholamines (both cause insulin resistance)
• Lactic acidosis • Muscular breakdown (rhabdo) • Generalized catabolic state
Sepsis Guidelines 10/7/2010
Critical Care Education Series
From the top down:
Heart • Myocardial O2 supply is dependent on diastolic
blood pressure • Circulating myocardial depressant factor
Lungs • Ventilation / perfusion mismatches • Initially due to increased dead space • Subsequently due to shunt • Acidosis - tachypnea decreased PaCO2
Kidneys • Oliguria • Kidney Injury and ultimately failure • Pre-renal failure due to intravascular dehydration,
circulating nephrotoxins, drugs.
From the top down:
Liver • ICU jaundice • Uncontrolled production of inflammatory
cytokines by the kuppfer cells (of the liver), primed by ischemia and stimulated by endotoxin (derived from the gut), leads to cholestasis and hyperbilirubinemia.
Splanchnic Circulation • GUT mucosa is usually protected from injury by
autoregulation. • Hypotension and hypovolemia leads superficial
mucosal injury • Which leads to atrophy and translocation of
bacteria into the portal circulation and stimulate liver macrophages causing cytokine release and amplification of SIRS.
Pharmacologic Therapies
• Steroid therapy • Vasopressor support • Insulin therapy • Antibiotic support • Nutrition • Recombinant human activated protein
C and Eritoran tetrasodium • Beta-adrenergic blockade

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Low Dose Steroid Therapy
Glucocorticoids have been demonstrated to have significant side effects in disease
states like sepsis:
• Improved metabolic, endocrine, phagocytic, and hemodynamic function
• Inhibition of inflammatory responses of the endothelial cell activation and damage
Randomized controlled trials
• The first study of 24 patients examined the effect of low dose steroid on the circulating cytokines, this study showed a reduction in the circulating blood levels of IL-6 and IL-8 in patients with hyper-dynamic septic shock, but not the IL-10 which is the anti-inflammatory cytokine. Limitations of this study were the small sample size and the death of almost 1/3 of the patients.
• The second RTC assessed prognostic importance of basal cortisol concentrations and response to cortisol to determine the effects of low dose steroids. This study had 40 patients and showed a 28 day mortality of 29% in the steroid group and 78% in the standard therapy (not statistically significant.)
• In the absence of shock, low dose steroids are not recommended.
Randomized controlled trials
• European large multicenter trial (CORTICUS) failed to show a mortality benefit but did show faster resolution of septic shock in patients that received steroids.
• Crit Care Med 2008 Vol. 36, no.1
Sepsis Guidelines 10/7/2010
Critical Care Education Series
Hydrocortisone Pearls
• Physiologic (low) doses 200-300mg daily in divided (TID/QID) doses is the current recommendation.
• Solu-Cortef 100mg IV TID or 50mg IV QID
• Indicated for treatment of septic shock in patients that require vasopressor support
Vasopressor support in sepsis
Current agents are:
• Norepinephrine (Levophed)
• Dopamine
• Phenylephrine (NeoSynephrine)
• Dobutamine
• Vasopressin (Not really a pressor)
Current research in pressor support
Norepinephrine vs. Dopamine • Dopamine at 10ug/kg/min was successful
in 31% of patients, survival rate of 17%
• Norepinephrine at 0.5-20ug/min had a 93% success rate, survival rate of 59%
10 of the 11 patients not responsive to Dopamine initially responded with the
addition of Norepinephrine

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Current research in pressor support
Epinephrine vs. Phenylephrine • Both effectively increased MAP
• Epinephrine increased gastric mucosal PCO2 production, decreased pH, altered oxygen supply in the splanchnic circulation, and was associated with tachyarrythmias, and increased regional lactate concentration.
• Phenylephrine reduced cardiac output, lowered heart rate, and reduced oxygen delivery
Pressor Pearls
• Norepinephrine and/or Dopamine are first line agents.
• Epinephrine, phenylephrine, vasopressin are not recommended first line agents but can be considered in refractory shock or to augment first-line agents.
• Second choice of inotropic support in the presence of documented poor cardiac output (low Ejection fraction) is Dobutamine
Vasopressin
Vasopressin is a peptide hormone that controls the reabsorption of molecules in the tubules of the kidneys by affecting the tissue's permeability. It also increases peripheral vascular resistance, which in turn increases arterial blood pressure. It plays a key role in homeostasis, by the regulation of water, glucose, and salts in the blood. 0.01-0.04 units/min IV gtt NO TITRATION REQUIRED!
Sepsis Guidelines 10/7/2010
Critical Care Education Series
Insulin Coverage
There is insufficient information from randomized controlled trials to
determine the optimal target range of blood glucose in the severely septic patient.
The NICE-SUGAR trial is the largest most
compelling study to date on glucose control in ICU patients given its inclusion of multiple ICUs and hospitals, and a more general patient population.
Surviving Sepsis Campaign Statement on Glucose Control in Severe Sepsis (June 2009)
Based on the results of this trial, we recommend against intravenous insulin therapy titrated to keep blood glucose in the normal range (80-110 mg/dl) in patients with severe sepsis.
It is clear that attempts to normalize blood glucose with IV insulin during critical illness results in higher rates of hypoglycemia.
Until additional information is available, teams seeking to implement glucose control should consider initiating insulin therapy when blood glucose levels exceed 180 mg/dL with a goal blood glucose approximating 150 mg/dl as was observed in the beneficial arm of the NICE-SUGAR trial.
Antibiotic Coverage
• The major sources of infection in severe sepsis or shock are pneumonia and intra-abdominal infections and other sources generally account for < 5 percent of cases.
• The prevalence of pneumonia as a cause of sepsis lends support to the case for treating severe sepsis with early antibiotic administration.
• In a recent study of ventilator-acquired pneumonia, patients with significant organ dysfunction (required criteria for severe sepsis) who received antibiotics later had far greater ICU mortality: 37 percent vs. 7 percent, P=0.006; hospital mortality: 44 percent vs. 15 percent, P=0.01.
Sepsis Guidelines 10/7/2010
Critical Care Education Series
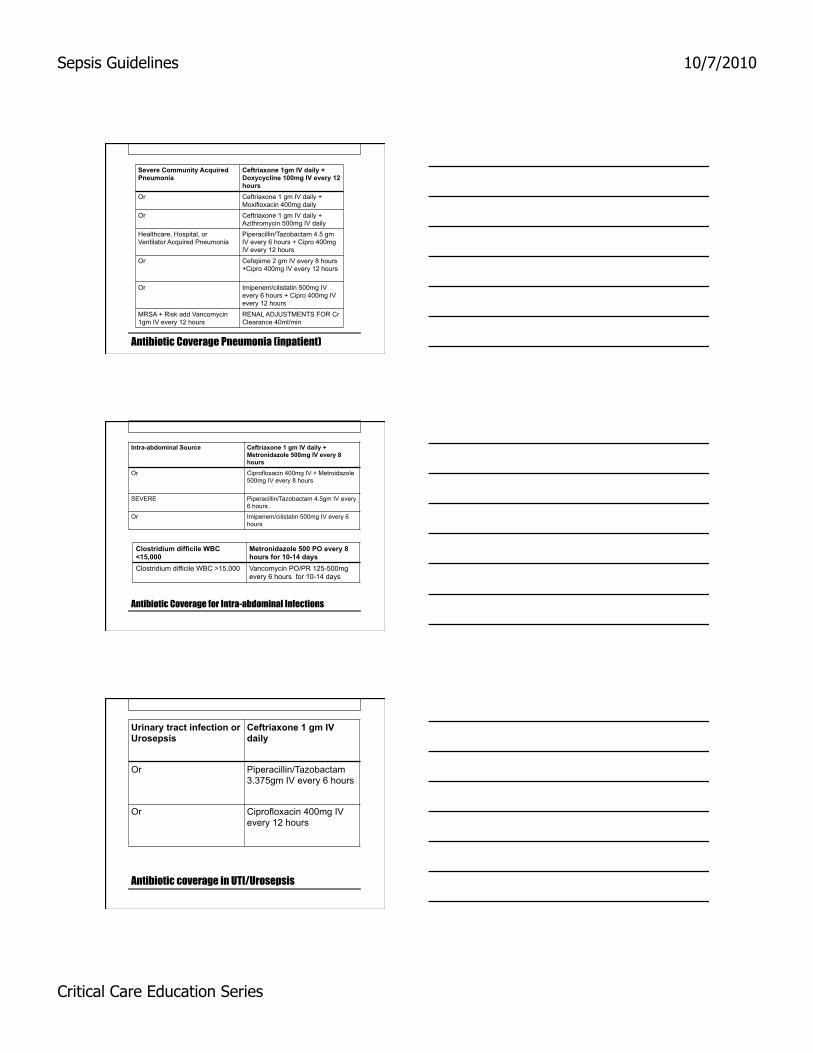
Antibiotic Coverage Pneumonia (inpatient)
Severe Community Acquired Pneumonia
Ceftriaxone 1gm IV daily + Doxycycline 100mg IV every 12 hours
Or Ceftriaxone 1 gm IV daily + Moxifloxacin 400mg daily
Or Ceftriaxone 1 gm IV daily + Azithromycin 500mg IV daily
Healthcare, Hospital, or Ventilator Acquired Pneumonia
Piperacillin/Tazobactam 4.5 gm IV every 6 hours + Cipro 400mg IV every 12 hours
Or Cefepime 2 gm IV every 8 hours +Cipro 400mg IV every 12 hours
Or Imipenem/cilistatin 500mg IV every 6 hours + Cipro 400mg IV every 12 hours
MRSA + Risk add Vancomycin 1gm IV every 12 hours
RENAL ADJUSTMENTS FOR Cr Clearance 40ml/min
Antibiotic Coverage for Intra-abdominal Infections
Intra-abdominal Source Ceftriaxone 1 gm IV daily + Metronidazole 500mg IV every 8 hours
Or Ciprofloxacin 400mg IV + Metroidazole 500mg IV every 8 hours
SEVERE Piperacillin/Tazobactam 4.5gm IV every 6 hours
Or Imipenem/cilistatin 500mg IV every 6 hours
Clostridium difficile WBC <15,000
Metronidazole 500 PO every 8 hours for 10-14 days
Clostridium difficile WBC >15,000 Vancomycin PO/PR 125-500mg every 6 hours for 10-14 days
Antibiotic coverage in UTI/Urosepsis
Urinary tract infection or Urosepsis
Ceftriaxone 1 gm IV daily
Or Piperacillin/Tazobactam 3.375gm IV every 6 hours
Or Ciprofloxacin 400mg IV every 12 hours

Sepsis Guidelines 10/7/2010
Critical Care Education Series
IMPROVE TIME TO BROAD-SPECTRUM ANTIBIOTICS
• From the time of presentation, broad-spectrum antibiotics administered within 3 hours for ED admissions
• 1 hour for non-ED ICU admissions.
• Narrowing the spectrum and reducing the duration will reduce the likelihood of super infection, however the desire to minimize complications should not take precedence over the need for an adequate course.
Nutrition in Sepsis
Several studies support the early initiation of nutritional support in the ICU.
• A randomized multicenter trial of 499 critically ill patients found that early initiation of nutritional support reduced the overall duration of hospitalization by 10 days (25 versus 35 days; p=.003)
• In addition, patients in the intervention group showed a trend toward reduced mortality, compared to those in the control group (27 versus 37 percent, respectively; p=.058).
• It is important to note that this study has not been replicated, and that other studies have failed to demonstrate this effect.
Out with the old and out with the new too.

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Current Sepsis Research
• TLR 4 Ligands
• Agents targeting lipopolysacharides , or increasing bactericidal permeability
• Agents targeting TLR signalsome
• ERITORAN
• POLYMYXIN B
• TAK-242
Recombinant Human Activated Protein C
Drotrecogin alfa, DrotAA, (Xigris)
• Antithrombotic
• Profibrinolytic
• Anti-inflammatory properties
Approved by FDA in November 2001 for the treatment of severe sepsis in adults with a high risk of death.
Xigris was administered at a dose of 24mcg/kg/hr for 96 hours at a cost of approximately $7,000 (US).
Xigris removed from the market October 2011
• Bleeding was the most serious side effect • Not recommended for pediatrics • Not recommended with a baseline platelet count
of less than 30,000/mm3 • Not recommended for patients at high risk for
surgery • Not recommended for patients at a low risk for
death or single organ failure APACHE II <25 • Some question as to usefulness in <50 yr olds
although this is not listed in most literature • Not recommended in patients with on-going
Heparin therapy (reduces the efficacy of Xigris)

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Investigational drug Eritoran
Eritoran’s mechanism of action differentiates it from others
Instead of using antibodies to target cytokine network activity, particularly endotoxin, Eritoran competes!
Eritoran is an analog of lipid A, which competes with endotoxin for binding sites, thereby blocking activation of toll-like receptor 4 (TLR-4).
TLR-4 has been linked to the innate immune system and is thought to play an important role in the course of severe sepsis.
Phase III Study for Eritoran Does Not Meet Primary Endpoint
• Phase III Clinical Trial ACCESS (A Controlled Comparison of Eritoran and Placebo in Patients with Severe Sepsis) trial.
• The purpose of the study was to evaluate the 28 day all-cause mortality risk of eritoran versus placebo.
• The Phase III trial enrolled severe sepsis 1500 patients at 251 locations with a moderate-to-high risk of mortality as determined by baseline APACHE II (Acute Physiology and Chronic Health Evaluation II) scores from 21 to 37. Unfortunately the drug was pulled off the market by Eisai in January 2011 failing to meet primary endpoint.
Beta-blockade in sepsis
• New Recent data suggest that beta-blocker effects on metabolism, glucose homeostasis, cytokine expression, and myocardial function may be beneficial in the setting of sepsis. Shock , 2009 Feb;31(2):113-9
• Cardio-protective effects • Improved oxygen utilization Beta-blockers might be useful in sepsis, especially if
you are a rat.

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Early Goal Directed Therapy
Surviving Sepsis Campaign
11 International professional societies and multiple specialties came together with the clear objective of:
• Early identification
• Early treatment in stopping the sepsis cascade
EARLY GOAL DIRECTED THERAPY was developed.
Early Goal Directed Therapy
• EGDT involves a more definitive resuscitation approach that begins on presentation to the emergency department or in the first 6 hours of sepsis induced hypo-perfusion.
• EGDT may be perceived as a radical approach to some.
• EGDT involves hemodynamic optimization.
EGDT blueprint
• Early recognition and diagnosis of sepsis • Central venous catheter placement capable of monitoring central
venous oxygen saturation (SVO2). • 500ml bolus of crystalloid every 30 minutes to achieve a CVP of
-12mmHg • Vasopressor support to achieve a MAP of >65mmHg • Vasodilator administration to maintain a MAP of <90mmHg • Transfusion of red blood cells to maintain a hematocrit of at least
30% • SVO2 of >70%, if below the addition of Dobutamine, and
mechanical ventilation with sedation to decrease oxygen consumption in a patient that could not achieve hemo-dynamic optimization.
• Urine output maintained at >0.5ml/kg/hr and early (within 1 hour) antibiotic administration.

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Results
263 enrolled patients • 130 were randomly assigned to
EGDT & 133 to standard therapy • In-hospital mortality : • EGDT = 30.5 percent • Standard care = 46.5 percent
(P=0.009 • Resuscitation parameters • EGDT had a higher central venous
oxygen saturation (70.4±10.7 % • vs. Standard 65.3±11.4 %)
• EGDT had lower lactate concentration (3.0±4.4 vs. 3.9±4.4 mmol/L),
• a lower base deficit (2.0±6.6 vs. 5.1±6.7 mmol/L)
• higher pH (7.40±0.12 vs. 7.36±0.12) than the patients assigned to standard therapy (P 0.02 for all comparisons)
• During the same period, mean APACHE II scores were significantly lower, indicating less severe organ dysfunction, in the patients assigned to early goal-directed therapy than in those assigned to standard therapy (13.0±6.3 vs. 15.9±6.4, P<0.001).
EGDT Research
• Mortality lowered by 16% • Shorter length of hospital stay • Control group (standard therapy) had a higher in-
hospital death due to sudden cardiovascular collapse
Conclusions Early goal-directed therapy provides significant
benefits with respect to outcome in patients with severe sepsis and septic shock.
Radical idea = Rejection
• EGDT did change the way we look at early aggressive treatment.
Surviving Sepsis Campaign is continuing to develop strategies for continuing Sepsis Education

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Sepsis Resuscitation Bundle
• The Sepsis Resuscitation and Management Bundles were derived from the 2008 Surviving Sepsis Campaign Guidelines which incorporated the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) system approach to evaluating the literature.
• A "bundle" is a group of therapies for a given disease that, when implemented together, may result in better outcomes than if implemented individually.
25 percent reduction in mortality due to severe sepsis or septic shock
• The science supporting the individual treatment strategies in a bundle is sufficiently mature such that implementation should be considered either best practice or a reasonable and generally accepted practice.
Sepsis Resuscitation Bundle
Hospitals should use the bundles to create customized protocols and pathways that will function well within their institutions.
There are two Severe Sepsis Bundles
Sepsis Resuscitation and Sepsis Management
The bundles have been developed based upon the 2008 Surviving Sepsis Campaign Guidelines for the Management of Severe Sepsis and Septic
Shock.
The Guidelines incorporated an evidence-based review of the literature and ranked the strength of each recommendation.
Each bundle has objectives to be accomplished within specific timeframes. The Guidelines incorporated an evidence-based review of the literature and
ranked the strength of each recommendation
Sepsis Resuscitation (6 hours) 1. Check Serum lactate. 2. Obtain Blood, Urine, Sputum, Wound cultures prior to antibiotic administration. 3. Broad-spectrum antibiotics
administered within 3 hours for ED admissions and 1 hour for non-ED ICU admissions from the time of presentation.
4. In the event of hypotension and/or lactate > 4 mmol/L (36 mg/dl): a) Deliver minimum of 20 ml/kg of crystalloid/ colloid fluid b) Give Vasopressors for hypotension not responding to initial fluid resuscitation to maintain mean arterial pressure (MAP) > 65 mm Hg.
5. In the event of Persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/L (36 mg/dl): a) Achieve central venous pressure (CVP) of > 8 mm Hg, (>12 for vent patients) b) Achieve central venous oxygen saturation (ScvO2) of > 70%.* (or mixed venous O2 sat of 65%)

Sepsis Guidelines 10/7/2010
Critical Care Education Series
Sepsis Management (24 hours)
1. Low‐dose steroids administered for septic shock in accordance with a standardized ICU policy.
2. Glucose control maintained > lower limit of normal,
but < 150 mg/dl (8.3 mmol/L). 3. Tidal volumes 4-6 ml/kg or Inspiratory plateau
pressures maintained < 30 cm H2O for mechanically ventilated patients.
Sepsis Management (24 hours)
Other recommendations include: • GI prophylaxis for all critically ill patients (No PPI in
patients with C. difficile) • Chemical or Mechanical prophylaxis VTE • No correction of INR with fresh frozen plasma in the
absence of planned procedures • Correction of thrombocytopenia when counts are
<5,000/mm and consider for < 30,000/mm • Permissive hypercapnia (modest) to improve tidal
volumes and improve plateau pressures
Take home for providers
• Have a low threshold for suspecting sepsis
• Early intervention saves lives and organs!
Sepsis Guidelines 10/7/2010
Critical Care Education Series
Questions???
References • Albanese, J., Leone, M., Dalmas, A., & Martin, C. (2005). Terlipressin or norepinephrine in hyperdynamic septic shock: a prospective, randomized
study. Critical Care Medicine. 33, 9. • Albuszies, G., Radermacher, P., Vogt, J., Wachter, U., Weber, S., & Schoaff, M. (2005). Effect of increased cardiac output on hepatic and intestinal
microcirculatory blood flow, oxygenation, and metabolism in hyperdynamic murine septic shock. Critical Care Medicine. 33, 10. • Andreoli, T. E., Carpenter, C. C., Griggs, R. C., & Loscalzo, J. (2004). Cecil essentials of medicine. (6th ed.). Philadelphia: Saunders. • Angus, D., Linde-Zwirble, W., Lidicker, J., Clermont, G., Carcillo, J., & Pinsky M. (2001). Epidemiology of severe sepsis in the United States: Analysis
of incidence, outcome, and associated costs of care. Critical Care Medicine, 29, 1303-1310. • Annane, D., Sebille, V., Charpentier, C., Bollaert P., Francois, B., Korach, J., & Capellier, G. (2002). Effect of treatment with low doses of
hydrocortisone and fludrocortisone on mortality in patients with septic shock. Journal of the American Medical Association, 288, 7, 862-871. • Arts, D.G., de Keizer, N.F., Vroom, M.B., & de Jonge, E. (2005). Reliability and accuracy of sequential organ failure assessment (SOFA) scoring.
Critical Care Medicine. 33, 9. • Balk, R. (2004). Optimum treatment of severe sepsis and septic shock: evidence in support of the recommendations. Disease-a-month, 50, 4, 1-33. • Beale, R.J., Hollenberg, S.M., Vincent, J.L., & Parrillo, J.E. (2004). Vasopressor and inotropic support in septic shock: an evidence based review.
Critical Care Medicine. 32, 11. • Bochud, P., Bonten, M., Marchetti, O., & Calandra, T. (2004). Antimicrobial therapy for patients with severe sepsis and septic shock: an evidence-based
review. Critical Care Medicine. 32, 11. • Briegel, J., Jochum, M., Gippner-Steppert, C., & Thiel, M. (2001). Immunomodulation in septic shock: Hydrocortisone differentially regulates cytokine
responses. Journal of the American Society of Nephrology, 12, 17. • Cariou, A., Vinsonneau, C., & Dhalnaut, J.F. (2004). Adjunctive therapies in sepsis: an evidence based review. Critical Care Medicine. 32, 11. • Chien, J.Y., Jerng, J.S., Yu, C.J., & Yang, P.C. (2005). Low serum level of high-density lipoprotein cholesterol is a poor prognostic factor for severe
sepsis. Critical Care Medicine. 33, 8. • Cohen, J., Brun-Buisson, C., Torres, A., & Jorgensen, J. (2004). Diagnosis of infection in sepsis: an evidence-based review. Critical Care Medicine. 33,
10. • Confalonieri, M., Urbino, R., Potena, A., Piatella, M., Pagiri, P., & Puccio, G. (2005). Hydrocortisone infusion for severe community-acquired
pneumonia. Critical Care
References
• Medicine, 171, 242-24. • FDA briefing document: anti-infective advisory committee drotrecogen alfa (activated) [recomibinant human activated protein C (rhAPC)]
(2001). Indianapolis, IN: Eli Lilly and Company. • Fourrier, F. (2004). Recombinant human activated protein C in the treatment of severe sepsis: an evidence-based review. Critical Care
Medicine. 32, 11. • Gibot, S., Cravoisy, A., Kolopp-Sarda, M.N., Bene, M.C., Faure, G., & Bollaert, P.E. (2005). Time course of strem-1, procalcitonin, and C-
reactive protein plasma concentrations during sepsis. Critical Care Medicine. 33, 4. • Keh, D., & Sprung, C. (2004). Use of corticosteroid therapy in patients with sepsis and septic shock: an evidence based review. Critical
Care Medicine. 33, 10. • Laterre, P.F., Levy, H., Clermont, G., Ball, D.E., Garg, R., & Nelson, D.R. (2004). Hospital mortality and resource use in subgroups of the
recombinant human activated protein c worldwide evaluation in severe sepsis (PROWESS) trial. (2004). Critical Care Medicine. 32, 11. • Levy, M.M., Macias, W.L., Vincent, J.L., Russell, J.A., Silva, E., & Trzaskoma, B. (2005). Early changes in organ function predict eventual
survival in severe sepsis. Critical Care Medicine. 33, 10. • Marshall, J.C., Maier, R., Jimenez, M., & Dellinger, P. (2004). Source control in the management of severe sepsis and septic shock: an
evidence-based review. Critical Care Medicine. 32, 11. • Marshall, J.C., Vincent, J.L., Guyatt, G., Angus, D., Abraham, E., & Bernard, G. (2005). Outcome measures for clinical research in sepsis:
a report of the 2nd Cambridge colloquium of the international sepsis forum. Critical Care Medicine, 33, 8, 1708-1716. • Micek, S., Shah, R., & Marin, K. (2003). Management of severe sepsis: Integration of multiple pharmacologic interventions.
Pharmacotherapy, 23, 11, 1486-1496. • Pizarro, C.F., Troster, E.J., Damiani, D., & Carcillo, J.A. (2005). Absolute and relative adrenal insufficiency in children with septic shock.
Critical Care Medicine. 33, 4. • Revelly, J.P., Tappy, L., Martinez, A., Bollmann, M., Cayeux, M.C., & Berger, M.M. (2005). Lactate and glucose metabolism in severe and
cardiogenic shock. Critical Care Medicine. 33, 10. • Rhodes, A., & Bennett, D. (2004). Early goal-directed therapy: an evidence-based review. Critical Care Medicine. 32, 11.

Sepsis Guidelines 10/7/2010
Critical Care Education Series
And more….
• Salgado, C.D., O’Grady, N., & Farr, B.M. (2005). Prevention and control of antimicrobial-resistant infections in intensive care patients. Critical Care Medicine. 33, 10.
• Schmidt, H., Muller-Werdan, U., Hoffmann, T., Francis, D.P., Peipoli, M.F., & Rauchhaus, M. (2005). Autonomic dysfunction predicts mortality in patients with multiple organ dysfunction syndrome of different age groups. Critical Care Medicine. 33, 9.
• Sessler, C., Perry, J., & Varney, K. (2004). Management of severe sepsis and septic shock. Current Opinion in Critical Care, 10, 354-363. • Shapiro, N., Howell, M., & Talmor, D. (2004). A blueprint for a sepsis protocol. Academy of Emergency Medicine, 12, 4, 352-359. • Su, F., Nguyen, N., Wang, Z., Cal, Y., Rogiers, P., & Vincent, J. (2005). Fever control in septic shock: beneficial or harmful? Shock, 23, 6,
516-520. • Suzuki, T., Morisaki, H., Serita, R., Yamamoto, M., Kotake, Y., & Ishizaka, A. (2005). Infusion of the B-adrenergic blocker esmolol
attenuates myocardial dysfunction in septic rats. Critical Care Medicine. 33, 10. • Treciak, S., & Dellinger, P. (2004). Other supportive therapies in sepsis: an evidence-based review. Critical Care Medicine. 32, 11. • Vender, J.S., Szokol, J.W., Murphy, G.S., & Nitsun, M. (2004). Sedation, analgesia, and neuromuscular blockade in sepsis: an evidence-
based review. Critical Care Medicine. 33, 10. • Vincent, J., Abraham, E., Annane, D., Bernard, G., Rivera, E., & Van den Berghe, G. (2002). Reducing mortality in sepsis: New directions.
Critical Care, 6(3), S1-18. • Vincent, J.L., & Gerlach, H. (2004). Fluid resuscitation in severe sepsis and septic shock: an evidence-based review. Critical Care
Medicine. 32, 11. • Vincent, J.L., Bernard, G.R., Beale, R., Doig, C., Putensen, C., & Dhainaut, J.F. (2005). Drotrecogin alfa treatment in severe sepsis from
the global open-label trial ENHANCE: further evidence for survival and safety and implications for early treatment. Critical Care Medicine. 33, 10.
• Waxman, A., Ward, N., Thompson, T., Lilly, C., Lisbon, A., & Hill, N. (2005). Roundtable debate: Controversies in the management of the septic patient – desperately seeking consensus. Critical Care, 9, E1-10.
• Yildiz, O., Doganay, M., Aygen, B., Guven, M., Kelestimur, F., & Tutus, A. (2002). Physiological-dose steroid therapy in sepsis. Critical Care, 6, 251-258.
• Zimmerman, J.L. (2004). Use of blood products in sepsis: an evidence-based review. Critical Care Medicine. 33, 10.