Embed Size (px)
Citation preview

1
© Copyright 2008 American Academy of Professional Coders
How to DissectHow to Dissect
Operative Reports toOperative Reports to
Find Find Missing PiecesMissing Pieces

2
© Copyright 2008 American Academy of Professional Coders
DISCLAIMER
This course was current at the time it was published. This course was prepared as a tool to assist the
participant in the correct and complete coding of operative reports. Although every reasonable effort has
been made to assure the accuracy of the information within these pages, the ultimate responsibility for
the correct submission of claims and response to any remittance advice lies with the provider of services.
The American Academy of Professional Coders (AAPC) employees, agents, and staff make no
representation, warranty, or guarantee that this compilation of information is error-free and will bear no
responsibility or liability for the results or consequences of the use of this course. This guide is a general
summary that explains commonly accepted aspects of code selection, but it is not a legal document.
Specific payers, including Medicare Carriers, may use different and sometimes varied policies and
procedures. Official provisions are contained in the relevant laws, regulations, rulings and contractual
agreements of providers.
NOTICES
Current Procedural Terminology (CPT®) is copyright © 2007 American Medical Association. All Rights
Reserved. CPT® is a registered trademark of the American Medical Association (AMA).
It is recommended that the participant of this course will familiar with general surgical coding and billing
requirements such as those published by NHIC, Corp at:
http://www.medicarenhic.com/providers/pubs/surgeryguide.pdf
How to Dissect Operative Reports and Find Missing PiecesWritten by: Stephanie L. Jones CPC, CPC-E/M
Special editorial thanks for contributions made by:Melanie Witt, RN, CPC, CPC-OBGYN, MATerry A. Fletcher, CPC, CCS-P, CCS, CPC-E/M, CPC-Cardio, CMSCS, CMC
Copyright ©2008 American Academy of Professional Coders
1-800-626-2633 www.aapc.com

3
© Copyright 2008 American Academy of Professional Coders
CONTENTS
Introduction...........................................................................................................................................................4
STEP 1: COMPREHENSION
Understand the Procedure ..................................................................................................................................4
You Said “Puce” and He Said “Purplish Red”.....................................................................................................4
STEP 2: VISUALIZATION
The Highlighter.....................................................................................................................................................5
STEP 3: RESEARCH
How to Research..................................................................................................................................................7
STEP 4: CONTEMPLATION
Finding the Missing Pieces..................................................................................................................................8
Coding and Documentation.................................................................................................................................8
Modifier Review..................................................................................................................................................12
Medical Necessity ..............................................................................................................................................14
Unlisted Procedures...........................................................................................................................................15
STEP 5: COMPENSATION
Billing and Payment ...........................................................................................................................................15
Practical Operative Notes – Dissected Examples............................................................................................16
Attachment A: Major Surgery Global Calendar Reference ..............................................................................20
Attachment B: Special Supplemental Handout ..............................................................................................202
SPECIAL WORKSHOP EXCLUSIVE
RECOVERY AUDIT CONTRACTORS SPECIAL OVERVIEW REPORT.......................................................29

4
© Copyright 2008 American Academy of Professional Coders
Introduction
The coding of operative reports gives some coders, practice administrators, and physicians a big
headache. Beyond the basic principle of proper claim submission, are all billable services being captured
by the coder? Are services medically necessary and otherwise supported? Do diagnoses properly reflect
the pre and post-operative condition? Have all compliance issues been properly adhered to? Coder
productivity and the adverse impact on accounts receivable (AR) due to backlogs and inaccuracies are
real concerns for many surgical practices. They are looking to eliminate missed opportunities, rejections,
and to significantly reduce risk of errors in coding.
Coding can be subjective and based on the knowledge and judgment of each individual coder. Some
coders are immersed in a high volume of repetitive cases, making coding relatively routine and easy. New
coders and coders who experience a wide berth of cases are faced with a bigger challenge. Computer
Assisted Coding software (CACs) can help and are growing in use; most popularly in practices where
documentation is already in an electronic format and where documented medical terms are limited and
recurring such as orthopedics, gastroenterology, interventional cardiology, podiatry, and urology. CACs
“read” entire medical records and can vastly improve the productivity of a coder by suggesting codes.
These codes must be validated by coders. And, the CACs may not intuitively find what may have been
performed but was NOT documented. CACs can’t go back and “talk to” the surgeon.
How to Dissect Operative Reports to Find Missing Pieces is designed to provide a simple framework for
coders who are working with or without CACs to better ensure that all services are documented and
coded accurately. This program will review the FIVE STEPS of operative report coding and billing and
discuss methods for achieving best results.
Step 1- Comprehension
Understand the ProcedureReading the complete operative report, pathology reports, and other supporting documentation is not
enough. The coder must completely understand the content, the instruments, and all terms. For some
coders who are familiar with the surgeon and procedures repetitively done, this is an easier task. For the
rest of us who are not also practicing physicians, this requires research!
You Said “Puce” and He Said “Purplish Red”
There are several different ways to say the same things. A coder may look ad nauseam for the terms
listed by the CPT® code and never find an exact match in the operative report. That is why it is imperative

5
© Copyright 2008 American Academy of Professional Coders
to understand everything written in the report. Sometimes the use of a particular surgical supply or
instrument will help define what was done. Sometimes it just requires a thorough understanding of the
anatomy involved.
For the coder who is new to coding a procedure, one way of quickly starting the research process is by
focusing initial discovery efforts on the procedures listed in the summary. These procedures may not be
listed correctly and procedures documented within the body of the report may not be listed in the
summary at all. However, it will help a coder with a place to start to begin to “picture” what is involved in
the procedures and whether or not the body of the report accurately portrays them.
Step 2- Visualization
The Highlighter
The best coders focus primarily on the body of the operative report. The headings, summary, indications,
and findings are important but the body of the report will drive code selection because sometimes there
are differences between them. These differences hold an important key to “finding missing pieces”. For
example, a complication may be documented in the body and not mentioned elsewhere, which allows for
a different, higher or additional code or modifier.
Typically, approximately 20 percent of an operative report contains words that are less important to a
coder. Breaking the information down is a vital first step. It enables a coder to “see” what codes are
documented. If you are not working with a CAC, which may do this for you automatically, this is most
easily accomplished on paper with highlighter pens. Highlighting “key words” (some are described below)
and words that you are not familiar with will start the process of accurate and complete coding and point
the direction for any research that is necessary. When you encounter an unfamiliar medical term, or are
unsure what an instrument is or what it does, it is important to find out. Researching techniques are
discussed later in this curriculum.
Key words to highlight include (but are not limited) to the following. This will help set the stage for the
kinds of terms you are looking for. These terms may appear in any tense, and/or in a singular or plural
format:
• Locations and Anatomical Structures involved (the surgical site and components within)
• Procedure Method - examples below include but are not limited to :
Arthrodesis
Burr, Puncture
Debridement
Destruction
Dilation
Drainage

6
© Copyright 2008 American Academy of Professional Coders
Excision
Exploration
Fusion
Graft
Harvest
Implantation
Incision
Injection
Infusion
Introduction
Ligation
Paring
Plicate
Probe
Reconnection
Reconstruction
Release
Removal
Repair
Replacement
Resection
Screening
Scope /-oscopy
Snare
Shaving
Transfer
• Type - examples below include, but are not limited to :
Simple, Intermediate, Complicated ,Extensive
Radical, Complete, Partial
Conversion, Revision
Open, Closed
Note that the surgeon may define these differently than the CPT® code.
• Size/Number - examples below include but are not limited to :
Separate Incisions, Excisions
Centimeters, Small, Medium, Large
# Of Visits (i.e. Maternity Care)
• The surgical instrument/s, medical devices used

7
© Copyright 2008 American Academy of Professional Coders
Step 3-Research
How to Research
Common coding sense is a learned skill. With this skill a coder can identify coding/billing risk and help to
minimize missed reimbursement. For most of us this requires some good old-fashioned research. It is not
enough to ask a co-worker. A coder needs to know the answers to the following (and more): What is the
specialty specific terminology most frequently used by this practice? What does the procedure itself look
like? What conditions normally prompt the procedure? Are there various approaches to the procedure? Is
the procedure similar to another procedure identified by a different CPT® code?
With the highlighted operative report you have a good idea of where you need to start. Tools that can
assist a coder in the research process include:
• Published Tools:
There are many reference books available to help coders. One example is the specialty specific
Coding Companion published by Ingenix, which includes the CPT® code with its official
description, a detailed illustration, and one-page format including lay descriptions, coding tips,
terminology, cross coding, and national Medicare relative value units. The Coder’s Desk
Reference is a condensed, albeit similar, resource also published by Ingenix. Other tools many
coders can’t live without include the American Medical Association’s (AMA) CPT® Assistant
Archives 1990-2007, which is a searchable CD featuring codes that have been written about in
the CPT® Assistant, and the AMA CodeManager® that includes clinical vignettes, illustrations,
and helpful code look-ups.
Many professional associations make available valuable tools such as the American Academy of
Orthopedic Surgeons (AAOS) Complete Global Service Data for Orthopaedic Surgery, which
offers details on inclusions and exclusions for more than 1,500 musculoskeletal procedures with
clinical examples. The AAPC Web site is also valuable for research, offering a search feature.
• Internet Research:
The Internet provides a wealth of information in less time than it takes to type the word “Google”.
Although it is important to be wary of the accuracy of data from unknown sources, the Internet will
often return image results that can be helpful when visualizing a procedure. For example, when
using the search terms “anatomy of the stomach" on http://google.com, more than 30 images are
returned that detail the structures of the stomach.

8
© Copyright 2008 American Academy of Professional Coders
• Local Coverage Determinations:
Medicare carriers are given the authority to establish medical policy, known as Local Coverage
Determinations (LCDs), pertinent to their areas of jurisdiction. Coders may review codes under
these to gain an insight on “reasonable and necessary” information and medical necessity
requirements. Coders can anticipate if a claim will be allowed based on the ICD-9-CM code
documented. These are usually available on your local carrier Web site.
• Ask a Surgeon:
Some practices will allow their coder an opportunity to watch an actual procedure. This can vastly
improve the coder’s skills by providing a visual understanding of what the surgeon did. For other
practices, many surgeons are happy to explain the intricacies of the procedure – especially when
prefaced with “I’d like to make sure that we eliminate missed coding opportunities. Could you
walk me through the procedure?”
Step 4-Contemplation
Finding the Missing Pieces
A “missing piece” relates to anything that puts a surgeon’s billing and/or coding in harm’s way. This
includes missing opportunities for appropriate revenue from the surgery as well as missing something that
relates to compliance of all rules and regulations related to billing and coding.
Coding and Documentation
• The Operative Report Summary versus the Body of the Report
Coding from the operative report summary alone leaves things at potential risk. The body of the
report will sometimes contain information that leads to a separately coded services, or even a
different service altogether.
• Unreported activity
If a beautician reads a file that says that the client’s hair was in a beautiful up-sweep that stayed
in place all evening---she can surmise that hair pins were probably involved. Coders need to
develop the same level of familiarity with the reports they are coding to identify when something
was probably done and not documented. Research and continued education relevant to the
procedure, related procedures, and surgical specialty are vital elements to mastering the skill of

9
© Copyright 2008 American Academy of Professional Coders
detecting probable undocumented services. When undocumented services are suspected the
coder should present the documentation to the surgeon for clarification. It may be necessary to
append the report with the missing and additional documentation. Undocumented services
without supporting documentation cannot be coded. It is important to not overlook this important
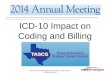
fact, especially in light of the May 2008 CERT findings that show Insufficient Documentation
errors are still a significant concern with regard to improper payments. See Figure 1.
Figure 1
Note: Derived from CMS Comprehensive Error Rate Testing (CERT) Improper Medicare Fee for
Service Payments Report - May 2008. More on this can be found on the CMS Web site at:
https://www.cms.hhs.gov/apps/er_report/index.asp.
• Radiology codes that are billable by the surgeon
Some surgical procedures require the use of imaging guidance. In turn, the surgeon may provide
both surgical services and imaging supervision and interpretation. A good clue regarding cases
where this may happen is within the notes found under the code in the professional procedure
code book such as found in the AMA CPT® 2008 Professional version. One example is found
under code 51102, which references imaging guidance supervision and interpretation codes
76942, 77002, and 77012. (Note that in the Example One: Operative Report within this
curriculum, 51102 is not provided with imaging guidance and is not coded. Codes should only be
used when actually provided and documented by the surgeon). Other common examples where
these services may occur are with biopsies, abscess drainage, gastrostomy tubes (i.e. new code

10
© Copyright 2008 American Academy of Professional Coders
49440), Saline Infused Sonohysterography Arthrography (SIS), biliary duct dilation with stent
insertion, and selective catheter placement.
• The Modifier 22
The key to the use of the modifier 22 is “services which are substantially greater than typically
required”. Since this is subjective, the operative note will need to be sent for review along with the
claim. If a note is not sent in addition to the claim, the 22 will likely be ignored by the payer. Most
helpful are descriptive statements within the operative report itself that identify the unusual
circumstances, such as increased intensity, time, technical difficulty of procedure, severity of
patient’s condition, or the physical and mental effort required by the surgeon. Most surgeries will
be coded and billed within three to five days; however, if a practice can afford to hold a claim, the
modifier 22 would appropriately report excessive follow-up visits that were required during the pre
or post operative periods that are related to the surgery. Some payers will also allow an adjusted
claim to be resubmitted. Examples of the typical appropriate use of the modifier 22 include:
Unusually lengthy procedure
Excessive blood loss for the particular procedure
Extensive well documented adhesions in abdominal surgery
Presence of excessively large surgical specimen
Trauma extensive enough to complicate the particular procedure
Other pathologies that directly interfere with the procedure but are not billed separately
• The Modifier 59
The coder must be confident when using this modifier that the service was distinct or independent
from other services performed with a surgery. Not using the modifier when it is appropriate will
result in reduced or denied payment for the service. Never use the modifier solely as a method to
get around a CCI or other payer bundling edit. Questions to help the coder clarify the correct use
of the modifier include:
Different site or organ system?
Separate incision or excision?
Separate lesion?
Separate injury?
Although seemingly black and white, even answering “yes” to the question above may not result
in proper use of the modifier according to the opinion of the payer. For example, is the knee a
single location or is it three locations; one location for each of the three separate compartments?
In which case, should a HCPCS Level II code such as G0289 be used instead of the professional

11
© Copyright 2008 American Academy of Professional Coders
procedure code with a modifier 59, or even a 51? Answers to questions like these are important
to clarify with payers.
• Use of an operating microscope
When the operating or surgical microscope is used it should be coded when the surgical codes
do not already include the operating microscope in the description of the code (i.e. code 15757).
Different payer bundling edits may include this code with other surgical codes and it may be
disallowed. When it is allowed, coding the microscope is a small difference that can add up.
Because code 69990 is an add-on code, it should not be reported with modifier 51.
• Correct number of units
Correct coding requires attention to detail. Avoid lost charges for missed units of service and do
not inflate the number of units by innocent error or otherwise. Make certain the appropriate
number is listed in the units column on the claim form.
• Appropriate Pre-op visits
CMS bundles a pre-operative visit beginning the day before the surgery into the global package.
This does not include the decision to perform the surgery, even if that happens the day before
(modifier 57). In some cases it may be necessary for the patient to see the surgeon two or three
days before the surgery. These E/M services are usually billable, even after the visit that resulted
in the decision for surgery. If a physician routinely brings a patient in two or three days before the
surgery to provide a service that is wholly related to the surgery, billing these services could be
abusive. It is necessary for the coder to pay close respect to the nature of the visit and medical
necessity of the encounter to ensure which category these services fall into. This will often require
the opinion of a practicing physician.
• Surgical Post Op Calendar Days
Because major surgeries have 90 calendar days attached to the global period, it is important to
keep a calendar that will alert the coder when a new service is now outside the global period. See
Attachment A of this curriculum for a handy date reference.
• Unrelated E/M Services
Modifier 24 reports an E/M service that is unrelated to the surgical procedure during the
postoperative (follow-up) period. The diagnosis(es) code for the unrelated E/M service should be
listed primarily to report the unrelated conditions/symptoms that required the attention of the
physician and not the ICD-9-CM-CM codes reported for the previous surgery.

12
© Copyright 2008 American Academy of Professional Coders
• Global period returns to the OR for complications or a more extensive procedure
When a patient is required to return to the OR due to complication or if a more extensive
procedure becomes necessary during the post-operative period the return trip surgeries should
be coded with one of the following modifiers:
58 Staged or related procedure in the post operative period
76 Repeat procedure by same provider
77 Repeat procedure by different provider
78 Return to the operating room for a related procedure during a postoperative period
79 Unrelated procedures by the same physician during the post-operative period
• The Best Way to Reflect the True Service
A certified coder is usually the best judge of code selection. There are times when the actual
services rendered are better described by less obvious codes. For example, an orthopedic
surgeon who provides uncomplicated closed fracture treatment without manipulation may better
represent his or her work by coding E/M services rather than coding the fracture care code at all.
Always check your payer contracts and policies when making these determinations.
In a perfect world there would be no innocent mistakes or abuses and certainly no fraud. If you are
working in the surgeon’s practice, remember there is no foul in seeking to review your documentation
concerns with the surgeon. If your research is complete, your findings may be quite valid for review and
result in keeping the surgeon out of harm’s way – whether from missed opportunity or post-payment risk.
Remember that if you are scratching you head in confusion - a payer auditor may also. For example, if
you note that 100 percent of the bladder tumors removed by your surgeon employer are documented as
“Large” it may be appropriate to point out that the proportion could be a “red flag” to payers to audit, and
to be prepared. Proactive communication with the surgeon and clarification on payer rules are part of a
coder’s “best practice”. A certified coder is a surgeon’s best tool for increased revenue under decreased
risk.
Modifier Review
Modifiers communicate that a service should be paid at a higher rate, a lower rate, or not at all. A missing
or incorrect modifier is an important “piece” because it will delay or prevent proper payment, or result in
coding abuse. For this reason the following modifiers are listed for quick review.

13
© Copyright 2008 American Academy of Professional Coders
• 22 Unusual Service: Distinctly more time consuming or difficult. Typically 20–30 percent of the
allowance.
• 24 Unrelated E/M Services by the Same Physician During the Post-operative Period.
• 25 Separately Identifiable E/M on the Same Day as a Minor Procedure.
• 50 (LT or RT) Bilateral Surgery: Typically the second side is only 0- 75 percent of the allowable
for the first side.
• 51 Multiple Procedures: Two or more separate procedures for which no single inclusive code is
available. List the procedure with the highest value first and list additional procedures in
descending value. Typically reimbursement of subsequent procedures is reduced, 50-100
percent.
• 52 Reduced Services: A (non-hospital outpatient) service partially eliminated at the physicians
election.
• 53 Discontinued Service: A (non-hospital outpatient) service that was begun yet discontinued by
the physician due to (non-elective) extenuating circumstances or threat to the patients well-being.
• 54 Surgical Care Only: Typically, reimbursement for the surgery is 70 percent.
• 55 Post-operative Care Only: Typically, reimbursement for the pre/post op care is 30 percent.
• 57 E/M Service that Results in the Initial Decision for Surgery.
• 58 Staged or Related Procedure by the Same Physician in the Post Operative Period: Planned
procedure, or procedure more extensive than the first related to the initial surgery.
• 59 Distinct Procedural Service on the Same Day: Different encounters, different sites or organ
systems, separate injury, separate incision.
• 62 Two Surgeons (Co-surgery): Two surgeons of sometimes of separate specialty are required.
This is not surgery assisting.

14
© Copyright 2008 American Academy of Professional Coders
• 63 Procedure on Infant less than 4 kg: Surgery modifier to show that work is increased due to the
weight of the infant or neonate.
• 66 Surgical Team: Several surgeons of different specialties who work together to perform highly
complex procedures.
• 76 Repeat Procedure by the Same Physician: Indicates that the service was repeated by the
same physician after the original service. This modifier avoids confusion and the assumption of
duplicate billing.
• 77 Repeat Procedure by Another Physician: This procedure indicates that another physician
repeated a procedure after the original service.
• 78 Return to the Operating Room: (Regardless of "fault") this modifier indicates a (non staged)
return to the OR for a related procedure during a post operative period.
• 79 Unrelated Procedure or Service Performed During a Post Operative Procedure.
• 80 Assistant Surgeon: This modifier indicates that an assistant surgeon’s services are applied to
the procedure code/s.
• 81 Minimum Assistant Surgeon: This is usually the assistance of a PA, LPN, or RN.
• 82 Assistant Surgeon When a Qualified Resident Is Not Available: This modifier indicates that
another physician is brought in to assist when a qualified resident is not available.
• 99 Multiple Modifiers: This modifier identifies that more than one modifier is necessary to
delineate the service and it is attached to the main procedure with all additional modifiers added
as subsequent line items.
Medical NecessityProper ICD-9-CM coding is important for establishing the medical necessity of the encounter. The official
guidelines for coding diagnoses are found at http://www.cdc.gov/nchs/data/icd9/icdguide.pdf
The treating physician determines the diagnosis. If documentation is unclear regarding the primary
diagnosis, the reason for a procedure, or secondary conditions, or if there is missing or conflicting
information, the coder must have the documentation clarified before the claim can be coded. One of the

15
© Copyright 2008 American Academy of Professional Coders
more costly mistakes made by some practices include reporting undocumented, probable or suspected
diagnoses. This can be construed as abuse, or fraud, and result in retrospective recovery of payments.
Accuracy in ICD-9-CM coding is as important as with procedural reporting.
Unlisted ProceduresGetting procedures paid that have no specific available procedure code requires reporting an unlisted
procedure and applying special attention to the claim before and after it is submitted. The best approach
for achieving payment is to work together with the payers. Your assigned commercial insurance
representatives may be helpful in starting the process. Contacting the plans’ medical director may also
have benefit. Claims for unlisted procedures are usually processed manually. Contacting the payers to
determine the appropriate unlisted codes and documentation necessary for coverage and payment of the
procedure helps facilitate the process. Provide the payer with information regarding the procedure
performed, its medical appropriateness, and the appropriate payment for it. Pre-authorization may be
needed to ensure payment. Provide payers detailed documentation of:
The nature, extent, and need for the procedure
The time, effort, and equipment necessary
Complexity of patient symptoms and relevant physical findings
Necessary follow-up care
Final diagnosis
A procedure may be so new that although it is accepted by some in the surgical community, the payer
may have insufficient information to approve the unlisted code. For example, the procedure may have no
convincing studies, or it may not be significantly accepted by one or more specialty areas that would be
expected to perform the procedure (such as with a new technique). One of the best ways a surgeon can
make his/her case is to relate the procedure to the patient’s eligible benefit structure and that the
procedure is not experimental or investigational. Making a comparative value to an existing procedure
code can also be helpful.
Step 5-Compensation
Billing and Payment
Don’t let the missing piece be your prep work and/or follow-through with proper claim payment. Ensure
that the following is always done:
• Prior authorization for the procedure is obtained
• Codes are ordered per RVU value. There are many publications to assist coders and automatic
scrubber software programs that will automatically place codes in the proper order according to
RVU. A free resource for viewing RVUs and Post Operative Global Periods can be found at:

16
© Copyright 2008 American Academy of Professional Coders
http://www.cms.hhs.gov/PhysicianFeeSched/downloads/RVU08C.jul.zip under an MS Excel file
named PPRRVU08.xls.
• Correct reimbursement per the negotiated allowable is made including:
Appropriate patient provider splits
Appropriate reimbursement of modifier that affect fees
Appropriate reimbursement for multiple procedures
Appropriate adjudication practices for bundling and coverage decisions
Practical Operative Notes – Dissected Examples
Example One: Operative Report
PREOPERATIVE DIAGNOSES: Stress urinary incontinenceand rectocele.
POSTOPERATIVE DIAGNOSES: Stress urinary incontinence, rectocele,enterocele,and postoperative urinary retention.
PROCEDURE[S]:1. Enterocele plication.2. Posterior colpoperineorrhaphy.3. Midurethral sling utilizing Advantage.4. Suprapubic catheter placement.
PROCEDURE: The patient was taken to the operating room, placed on theoperating room in dorsal supine position. The patient and the procedurewere reverified. General anesthesia was induced. She was placed in thedorsal lithotomy position, prepped and draped in the usual sterile fashion,a Foley catheter was placed. The perineal body and posterior vaginalmucosa were infiltrated with 0.5 percent Marcaine with epinephrine. Adiamond-shaped wedge of perineal skin and vaginal mucosa wasresected and the vagina was opened in the midline. An enterocele sacwas identified and entered sharply. The enterocele was plicated using 2-0 silk in a purse string fashion, 2 sutures were placed. These were tieddown; making sure no bowel was incorporated into the closure.
The levator muscles were then plicated in the midline usinginterrupted stitches of 2-0 Vicryl. Rectal exam confirmed excellentrectovaginal wall tone and no stitch injury to the rectum. Excessvaginal mucosa was trimmed and the vagina was closed with 2-0Vicryl.
(continued following page)
• The Approach isVAGINAL.
• The ENTEROCELEis repaired.
• COLPORRHAPHYis performed for therectocele.

17
© Copyright 2008 American Academy of Professional Coders
A perineorrhaphy was accomplished by reapproximating the transverseperineal musculature in the midline using interrupted stitches of 2-0 Vicryl.A second layer was placed with 3-0 chromic and the skin was closed with3-0 chromic as well in a subcuticular fashion. At the end of the procedure,the vaginal had excellent length and caliber.
• PERINEORRHAPHYis performed aspart of the repair.
The retropubic space had been distended with 20 cc of 0.5 percent Marcainewith epinephrine. Two suprapubic stab incisions were made, 2 cm lateralto the midline, on each side. The vagina was opened just distal tourethral meatus. Periurethral tunnels were created on each side. Utilizinga catheter guide, the bladder was deviated to the left. On the right, the tapewas introduced alongside the urethra, guided to the endopelvic fasciaalong the posterior aspect of the pubic bone, and out through thesuprapubic stab incision. The same procedure was repeated on theopposite side with the bladder deviated in the opposite direction.Cystoscopy was carried out. The urethral meatus was noted to be slightlystenotic, and it was dilated and the, urethra was dilated. There was no injuryto the bladder and the bladder was filled to 300 cc. With suprapubic pressure,there was easy urinary leakage. A #8 Hegar dilator was placed between thesling and the urethra and the sheath was removed. With suprapubic pressure,there was still a bit of urinary leakage, and no further adjustment of the tapewas done. The vaginal aspect was irrigated. It was trimmed to the appropriatelength and the incisions closed.
• Tape Procedure –AKA: SLINGOPERATION isperformed.
• CYSTOSCOPY isperformed.
I anticipate prolonged urinary retention. The bladder was filled to 500 cc and asuprapubic catheter was placed through a separate stab incision. TheFoley catheter had been removed. The suprapubic was connected to adown drain. Sterile dressing and Neosporin was applied. A vaginal pack wasplaced. Sponge and needle count were correct x2. The patient was awakenedand transferred to the recovery room in stable and satisfactory condition.
Diagnoses: Stress urinary incontinence – 625.6Rectocele – 618.04Enterocele – 618.6Postoperative urinary retention – 788.20
Procedures: Enterocele repair – 57268 (vaginal approach)Posterior colpoperineorrhaphy (rectocele repair) – 57250Midurethral sling utilizing Advantage – 57288Cystourethroscopy - 52000Suprapubic catheter placement – 51102
• Placement of theSUPRAPUBICCATHETER
Coding Solution:
• 57288 (linked to 625.6) RVU 22.15
• 57250-22-51 (linked to 618.04 & 618.6) RVU 17.11
• 51102-51 (linked to 788.20) RVU 9.30
Coding Rationale:
The enterocele plication is bundled into the sling procedure because it is listed as a CPT® “separate
procedure” even though an enterocele repair is not bundled with a posterior repair. However, theenterocele added significantly to the time and work involved with this operation. Therefore, adding amodifier 22 to 57250 is arguably appropriate. Some payers will require a separate letter and specific

18
© Copyright 2008 American Academy of Professional Coders
statement regarding the unusual time that was required. Documentation should accompany the claim.Please note that some payers, or peers, will not agree with or accept the modifier. Also, some payers willonly allow modifier 22 to be reported with first listed procedure. The cystourethroscopy is not separatelyreportable.
Example Two: Consultation
Patient is a pleasant 27-year-old female with a family history of colon “problems”, which she states wascolon cancer. Her mother had the condition and did pass away when the patient was quiet young due to“medical problems”. She presented to Dr. Smith last week for an annual physical where she made thecomplaint of having noticed “a lot of blood” in loose stools. By written referral and Rx (filed in this chart)Dr. Smith has asked for my opinion regarding the need for a screening colonoscopy. Patient states thatthe incident of bloody stool happened one time almost three weeks ago and has not happened since. Shewas told by Dr. Smith to prep for today’s exam with expectation of possible colonoscopy. She has told methat she complied with all prep procedures and complains of feeling hungry but makes no othercomplaint. She denies having had any other symptoms such as constipation with straining. Examinationtoday shows a healthy looking young lady. Abdomen is normal and non-tender. S1, S2 normal. Lungsclear. BP 140/82. Stool occult blood positive. Despite the young age of the patient the presentingsymptoms, family history, and the positive Guaiac smear I recommend we proceed with the colonoscopy.Under separate report, including the operative report I will send report back to Dr. Smith indicatingfindings. A copy of that report will be included in this chart once it is faxed back to Dr. Smith. We willproceed with colonoscopy at this time.
Example Two: Operative Report
PREOPERATIVE DIAGNOSIS: Screening colonoscopyPOSTOPERATIVE DIAGNOSIS: Adenomatous sessile polypPROCEDURE PERFORMED: Colonoscopy and polypectomyANESTHESIA: Versed 3.0 milligrams intravenous
INDICATIONS:Family history of colon cancer, stool guaiac positive for blood.
PROCEDURE:The 27-year-old female patient is prepped and draped for the procedurein the usual fashion. Anesthesia is administered intravenously.Colonoscopy performed to the cecum; the patient did well. Thecolonoscope showed 1 centimeter sessile polyp at 20 centimeters and 1centimeter sessile polyp at 22 centimeters. These were removed withsnare cautery and recovered for biopsy. The patient had the procedureperformed under pulse oximetry, electrocardiogram monitoring, bloodpressure monitoring, 2 liters nasal oxygen.
(continued following page)
• This is not a“SCREENING.”
• The location ofthe scope:passed to theCECUM
• SNARECAUTERY wasused for BIOPSY

19
© Copyright 2008 American Academy of Professional Coders
IMPRESSION:Two 1 centimeter sessile polyps removed. Initial path report indicatesadenomatous polyps.
RECOMMENDATIONS:1. I recommend a repeat stool Guaiac in one year and a repeatcolonoscopy in three years.
Coding Solution:
• Consult 99242-25 (linked to blood in stool 578.1 and family history V16.0)
• Occult Blood Smear 82272 (linked to blood in stool 792.1 and family history V16.0)
• Colonoscopy w/ polyp by snare- 45385 (linked to benign neoplasm 211.3, & family history V16.0)
Coding Rationale:
In this case the consultation is separately reported because the GI physician’s opinion was the reason forthe visit. The GI physician subsequently decided to do the colonoscopy. In most cases, a patient is sentto the GI physician for the procedure and their opinion is not requested. When this happens there isusually no separately identifiable E/M service. Watch for cases where it is appropriate to bill for the E/M.

20
© Copyright 2008 American Academy of Professional Coders
Attachment A: Major Surgery Global Calendar Reference
DOS
>
Global DOS
>
Global DOS
>
Global DOS
>
Global DOS
>
Global
8/1/08 10/30/08 9/6/08 12/5/08 10/12/08 1/10/09 11/17/08 2/15/09 12/23/08 3/23/09
8/2/08 10/31/08 9/7/08 12/6/08 10/13/08 1/11/09 11/18/08 2/16/09 12/24/08 3/24/09
8/3/08 11/1/08 9/8/08 12/7/08 10/14/08 1/12/09 11/19/08 2/17/09 12/25/08 3/25/09
8/4/08 11/2/08 9/9/08 12/8/08 10/15/08 1/13/09 11/20/08 2/18/09 12/26/08 3/26/09
8/5/08 11/3/08 9/10/08 12/9/08 10/16/08 1/14/09 11/21/08 2/19/09 12/27/08 3/27/09
8/6/08 11/4/08 9/11/08 12/10/08 10/17/08 1/15/09 11/22/08 2/20/09 12/28/08 3/28/09
8/7/08 11/5/08 9/12/08 12/11/08 10/18/08 1/16/09 11/23/08 2/21/09 12/29/08 3/29/09
8/8/08 11/6/08 9/13/08 12/12/08 10/19/08 1/17/09 11/24/08 2/22/09 12/30/08 3/30/09
8/9/08 11/7/08 9/14/08 12/13/08 10/20/08 1/18/09 11/25/08 2/23/09 12/31/08 3/31/09
8/10/08 11/8/08 9/15/08 12/14/08 10/21/08 1/19/09 11/26/08 2/24/09 1/1/09 4/1/09
8/11/08 11/9/08 9/16/08 12/15/08 10/22/08 1/20/09 11/27/08 2/25/09 1/2/09 4/2/09
8/12/08 11/10/08 9/17/08 12/16/08 10/23/08 1/21/09 11/28/08 2/26/09 1/3/09 4/3/09
8/13/08 11/11/08 9/18/08 12/17/08 10/24/08 1/22/09 11/29/08 2/27/09 1/4/09 4/4/09
8/14/08 11/12/08 9/19/08 12/18/08 10/25/08 1/23/09 11/30/08 2/28/09 1/5/09 4/5/09
8/15/08 11/13/08 9/20/08 12/19/08 10/26/08 1/24/09 12/1/08 3/1/09 1/6/09 4/6/09
8/16/08 11/14/08 9/21/08 12/20/08 10/27/08 1/25/09 12/2/08 3/2/09 1/7/09 4/7/09
8/17/08 11/15/08 9/22/08 12/21/08 10/28/08 1/26/09 12/3/08 3/3/09 1/8/09 4/8/09
8/18/08 11/16/08 9/23/08 12/22/08 10/29/08 1/27/09 12/4/08 3/4/09 1/9/09 4/9/09
8/19/08 11/17/08 9/24/08 12/23/08 10/30/08 1/28/09 12/5/08 3/5/09 1/10/09 4/10/09
8/20/08 11/18/08 9/25/08 12/24/08 10/31/08 1/29/09 12/6/08 3/6/09 1/11/09 4/11/09
8/21/08 11/19/08 9/26/08 12/25/08 11/1/08 1/30/09 12/7/08 3/7/09 1/12/09 4/12/09
8/22/08 11/20/08 9/27/08 12/26/08 11/2/08 1/31/09 12/8/08 3/8/09 1/13/09 4/13/09
8/23/08 11/21/08 9/28/08 12/27/08 11/3/08 2/1/09 12/9/08 3/9/09 1/14/09 4/14/09
8/24/08 11/22/08 9/29/08 12/28/08 11/4/08 2/2/09 12/10/08 3/10/09 1/15/09 4/15/09
8/25/08 11/23/08 9/30/08 12/29/08 11/5/08 2/3/09 12/11/08 3/11/09 1/16/09 4/16/09
8/26/08 11/24/08 10/1/08 12/30/08 11/6/08 2/4/09 12/12/08 3/12/09 1/17/09 4/17/09
8/27/08 11/25/08 10/2/08 12/31/08 11/7/08 2/5/09 12/13/08 3/13/09 1/18/09 4/18/09
8/28/08 11/26/08 10/3/08 1/1/09 11/8/08 2/6/09 12/14/08 3/14/09 1/19/09 4/19/09
8/29/08 11/27/08 10/4/08 1/2/09 11/9/08 2/7/09 12/15/08 3/15/09 1/20/09 4/20/09
8/30/08 11/28/08 10/5/08 1/3/09 11/10/08 2/8/09 12/16/08 3/16/09 1/21/09 4/21/09
8/31/08 11/29/08 10/6/08 1/4/09 11/11/08 2/9/09 12/17/08 3/17/09 1/22/09 4/22/09
9/1/08 11/30/08 10/7/08 1/5/09 11/12/08 2/10/09 12/18/08 3/18/09 1/23/09 4/23/09
9/2/08 12/1/08 10/8/08 1/6/09 11/13/08 2/11/09 12/19/08 3/19/09 1/24/09 4/24/09
9/3/08 12/2/08 10/9/08 1/7/09 11/14/08 2/12/09 12/20/08 3/20/09 1/25/09 4/25/09
9/4/08 12/3/08 10/10/08 1/8/09 11/15/08 2/13/09 12/21/08 3/21/09 1/26/09 4/26/09
9/5/08 12/4/08 10/11/08 1/9/09 11/16/08 2/14/09 12/22/08 3/22/09 1/27/09 4/27/09

21
© Copyright 2008 American Academy of Professional Coders
Attachment A: (continued)
DOS
>
Global DOS
>
Global DOS
>
Global DOS
>
Global DOS
>
Global
1/28/09 4/28/09 3/5/09 6/3/09 4/10/09 7/9/09 5/16/09 8/14/09 6/21/09 9/19/09
1/29/09 4/29/09 3/6/09 6/4/09 4/11/09 7/10/09 5/17/09 8/15/09 6/22/09 9/20/09
1/30/09 4/30/09 3/7/09 6/5/09 4/12/09 7/11/09 5/18/09 8/16/09 6/23/09 9/21/09
1/31/09 5/1/09 3/8/09 6/6/09 4/13/09 7/12/09 5/19/09 8/17/09 6/24/09 9/22/09
2/1/09 5/2/09 3/9/09 6/7/09 4/14/09 7/13/09 5/20/09 8/18/09 6/25/09 9/23/09
2/2/09 5/3/09 3/10/09 6/8/09 4/15/09 7/14/09 5/21/09 8/19/09 6/26/09 9/24/09
2/3/09 5/4/09 3/11/09 6/9/09 4/16/09 7/15/09 5/22/09 8/20/09 6/27/09 9/25/09
2/4/09 5/5/09 3/12/09 6/10/09 4/17/09 7/16/09 5/23/09 8/21/09 6/28/09 9/26/09
2/5/09 5/6/09 3/13/09 6/11/09 4/18/09 7/17/09 5/24/09 8/22/09 6/29/09 9/27/09
2/6/09 5/7/09 3/14/09 6/12/09 4/19/09 7/18/09 5/25/09 8/23/09 6/30/09 9/28/09
2/7/09 5/8/09 3/15/09 6/13/09 4/20/09 7/19/09 5/26/09 8/24/09 7/1/09 9/29/09
2/8/09 5/9/09 3/16/09 6/14/09 4/21/09 7/20/09 5/27/09 8/25/09 7/2/09 9/30/09
2/9/09 5/10/09 3/17/09 6/15/09 4/22/09 7/21/09 5/28/09 8/26/09 7/3/09 10/1/09
2/10/09 5/11/09 3/18/09 6/16/09 4/23/09 7/22/09 5/29/09 8/27/09 7/4/09 10/2/09
2/11/09 5/12/09 3/19/09 6/17/09 4/24/09 7/23/09 5/30/09 8/28/09 7/5/09 10/3/09
2/12/09 5/13/09 3/20/09 6/18/09 4/25/09 7/24/09 5/31/09 8/29/09 7/6/09 10/4/09
2/13/09 5/14/09 3/21/09 6/19/09 4/26/09 7/25/09 6/1/09 8/30/09 7/7/09 10/5/09
2/14/09 5/15/09 3/22/09 6/20/09 4/27/09 7/26/09 6/2/09 8/31/09 7/8/09 10/6/09
2/15/09 5/16/09 3/23/09 6/21/09 4/28/09 7/27/09 6/3/09 9/1/09 7/9/09 10/7/09
2/16/09 5/17/09 3/24/09 6/22/09 4/29/09 7/28/09 6/4/09 9/2/09 7/10/09 10/8/09
2/17/09 5/18/09 3/25/09 6/23/09 4/30/09 7/29/09 6/5/09 9/3/09 7/11/09 10/9/09
2/18/09 5/19/09 3/26/09 6/24/09 5/1/09 7/30/09 6/6/09 9/4/09 7/12/09 10/10/09
2/19/09 5/20/09 3/27/09 6/25/09 5/2/09 7/31/09 6/7/09 9/5/09 7/13/09 10/11/09
2/20/09 5/21/09 3/28/09 6/26/09 5/3/09 8/1/09 6/8/09 9/6/09 7/14/09 10/12/09
2/21/09 5/22/09 3/29/09 6/27/09 5/4/09 8/2/09 6/9/09 9/7/09 7/15/09 10/13/09
2/22/09 5/23/09 3/30/09 6/28/09 5/5/09 8/3/09 6/10/09 9/8/09 7/16/09 10/14/09
2/23/09 5/24/09 3/31/09 6/29/09 5/6/09 8/4/09 6/11/09 9/9/09 7/17/09 10/15/09
2/24/09 5/25/09 4/1/09 6/30/09 5/7/09 8/5/09 6/12/09 9/10/09 7/18/09 10/16/09
2/25/09 5/26/09 4/2/09 7/1/09 5/8/09 8/6/09 6/13/09 9/11/09 7/19/09 10/17/09
2/26/09 5/27/09 4/3/09 7/2/09 5/9/09 8/7/09 6/14/09 9/12/09 7/20/09 10/18/09
2/27/09 5/28/09 4/4/09 7/3/09 5/10/09 8/8/09 6/15/09 9/13/09 7/21/09 10/19/09
2/28/09 5/29/09 4/5/09 7/4/09 5/11/09 8/9/09 6/16/09 9/14/09 7/22/09 10/20/09
3/1/09 5/30/09 4/6/09 7/5/09 5/12/09 8/10/09 6/17/09 9/15/09 7/23/09 10/21/09
3/2/09 5/31/09 4/7/09 7/6/09 5/13/09 8/11/09 6/18/09 9/16/09 7/24/09 10/22/09
3/3/09 6/1/09 4/8/09 7/7/09 5/14/09 8/12/09 6/19/09 9/17/09 7/25/09 10/23/09
3/4/09 6/2/09 4/9/09 7/8/09 5/15/09 8/13/09 6/20/09 9/18/09 7/26/09 10/24/09

22
© Copyright 2008 American Academy of Professional Coders
Attachment B:
Special Supplemental Handout
Special Editorial Thanks for “Real” Operative Reports Provided by:Terry A. Fletcher, CPC, CCS-P, CCS, CPC-EM, CPC-Cardio, CMSCS, CMC
DISCLAIMERThis supplement was current at the time it was published. Although every reasonable effort has been made to assure the accuracyof the information within these pages, the ultimate responsibility for the correct submission of claims and response to any remittanceadvice lies with the provider of services. The American Academy of Professional Coders (AAPC) employees, agents, and staff makeno representation, warranty, or guarantee that this compilation of information is error-free and will bear no responsibility or liabilityfor the results or consequences of the use of this course. This guide is a general summary that explains commonly acceptedaspects of code selection, but it is not a legal document. Specific payers, including Medicare Carriers, may use different andsometimes varied policies and procedures. Official provisions are contained in the relevant laws, regulations, rulings andcontractual agreements of providers.
NOTICESCurrent Procedural Terminology (CPT
®) is copyright © 2007 American Medical Association. All Rights Reserved. CPT
® is a
registered trademark of the American Medical Association (AMA).
Please note that all names, dates, and other relevant PHI have been changed in order to ensure full compliance with HIPAAregulations. Any similarity to actual person/s is entirely coincidental. These supplemental handouts will be reviewed during theworkshop as time allows.

23
© Copyright 2008 American Academy of Professional Coders
Supplement # 1
Procedures Performed:
1. Left Heart Cath2. Coronary Angiography3. Aortic Arch Angiogram4. Abdominal Aortogram5. Right Femoral Angiogram
Procedure in Detail:
This is a 68 year old male. The right groin was prepped and draped in the usual sterile
fashion. Access was gained through the right femoral artery. A 6-Friench sheath was placed
in the right common femoral artery. All catheters were advanced over a guidewire and
exchanged over the long exchange wire. The left coronary was then engaged with a 6-
French JL4 left coronary catheter and multiple views were obtained. The right coronary
artery was then selectively engaged and multiple views performed. It appears to be
occluded in the ostial portion. The catheter was then replaced with a 6-french angled pigtail
catheter, which was advanced to the left ventricle and left ventriculography performed.
The catheter was then advanced to the aortic arch angiogram was done. The catheter
was placed at the level of the renal arteries in the abdominal aorta, and an abdominal
aortogram was performed. The guidewire was removed. A right femoral angiogram was
performed, and an angioseal placed **.
Procedure Codes:• 93510-26 Left heart catheterization / RVU 6.90• 93545 Inject for coronary x-rays / RVU 6.28• 93543 Injection for heart x-rays / RVU 2.92• 75650-26 Artery x-rays, head & neck / RVU 2.14• 93556-26 Imaging, cardiac cath / RVU 1.30• 93555-26 Imaging, cardiac cath / RVU 1.27• G0275 Renal angio, cardiac cath / RVU 0.39
** Note: Coding not allowed.

24
© Copyright 2008 American Academy of Professional Coders
Supplement # 2
PREOPERATIVE DIAGNOSIS: Right lower extremity claudication.
POSTOPERATIVE DIAGNOSIS: Right lower extremity claudication
NAME OF OPERATION: Right superficial femoral artery atherectomy (two levels viaantegrade approach and right lower extremity angiography.
COMPLICATION: None.
CONTRAST USED: Isovue 370,60 ml.
FLUOROSCOPY TIME: 14.7 minutes.
CLINICAL INDICATIONS: This is an 81-year-old woman with severe right lower
extremity claudication. A prior angiography demonstrated single-vessel runoff below the
knee on the right with focal disease in the right superficial femoral artery at 2 levels. She
is referred for Fox Hollow atherectomy.
PROCEDURE IN DETAIL: Informed consent was obtained. The patient was brought to
the cardiac catheterization laboratory in the fasting postoperative state. She was
prepped and draped in the usual fashion. Percutaneous entry into the right common
femoral artery was done using an antegrade approach. Three punches of the vessel
had to be done as the initial punctures did not get high enough in the common femoral
artery to allow access to the SFA, but rather we were being directed down the profunda.
Ultimately, the antegrade puncture was accomplished, and a 7-French short sheath was
inserted. Pre-procedure angiography was done to localize the disease and
measure the vessel with a catheter placed in the right superficial femoral artery.***
We then proceeded with atherectomy utilizing a Fox Hollow Atherectomy device
(two devices were used with the definitive device being 5.5 to 7-mm vessel.
Multiple plaque specimens were retrieved at both the proximal and distal SFA.
Post-procedure angiography of the right lower extremity was done and carried out to the
ankle and demonstrated single-vessel runoff, as was seen pre-procedure.
(Continued on the next page.)

25
© Copyright 2008 American Academy of Professional Coders
RIGHT LOWER EXTREMITY ANGIOGRAPHY: A right lower extremity angiography
demonstrates a patient right profunda femoris. The right common femoral artery is
patent and normal. The right superficial femoral artery is diffusely diseased, but there are
2 high-grade stenotic lesions greater than 90 plus % in the mid and distal SFA just
above the adductor canal. Mid portion of the popliteal artery has approximately 50%
stenosis, and below the knee, there is only peroneal runoff to the ankle. The anterior
tibial and posterior tibial are occluded.
IMPRESSION: Successful atherectomy using a FoxHollow device (5.5-7 with multiple
specimens retrieved. Residual stenosis is less than 10% with no evidence of dissection
and single-vessel runoff on the right is demonstrated an unchanged Postprocedure.
Procedure Codes:• 36245 Place catheter in artery / RVU 33.78• 35493-51 Atherectomy, percutaneous / RVU 12.62• 75992 Atherectomy, x-ray exam / RVU 0.00
Diagnoses Codes:• 444.22• 440.21
***Note: Coding not allowed.

26
© Copyright 2008 American Academy of Professional Coders
Supplement #3
ENDOSCOPY CENTER OPERATIVE REPORT
PREOPERATIVE DIAGNOSES:Family history of colon cancer occurring in a primary relative and a personal history ofpolyps.
POSTOPERATIVE DIAGNOSES:Family history of colon cancer occurring in a primary relative and a personal history ofpolyps with rectal polyps.
PROCEDURES:Total colonoscopy with multiple rectal polyp ablations.
PREOP FINDINGS:This 61-year-old female with a family history of colon cancer last underwent endoscopy4 years ago. Her exam today revealed small polyps in the rectum.
DETAILS OF PROCEDURE:
With the patient in the left lateral position and after sedation using 6 mg of Versed and
100 mcg of Fentanyl, the Olympus adult colonoscope was inserted and advanced to the
cecum. The ileocecal valve and appendiceal openings were normal. The scope was
withdrawn with the viewing circumferentially the cecum, right colon, hepatic flexure,
transverse colon, splenic flexure, left colon, and sigmoid. Diverticular opening noted. In
the distal rectum, small polypoid elevations were cauterized and ablated. The
scope was taken from the field and the patient taken to recovery in stable condition.
The patient will undergo follow up colonoscopy in 3 years.
Procedure Code:
• 45383
Diagnoses Code:
• 211.3

27
© Copyright 2008 American Academy of Professional Coders
Supplement # 4
ASSISTANT: None
PREOPERATIVE DIAGNOSIS: Torn medial meniscus with chondromalacia, left knee.
POSTOPERATIVE DAGNOSES:
1. Torn medial meniscus.
2. Chondromalacia, medial femoral condyle and patella, left knee.
PROCEDURES:
1. Arthroscopy.
2. Arthroscopic partial medial meniscectomy.
3. Arthroscopic chondroplasty medial femoral condyle and patellofemoral joint.
FINDING AND INDICATIONS:
This 70-year old female patient has a significant torn medial meniscus on MRI scan.
Examination under anesthesia reveals range of motion from 5 to 125. There is no
instability. Arthroscopic evaluation revealed grade 2 to 3 changes of chondromalacia
patella and femoral sulcus in the medial compartment. The articular surfaces revealed a
fairly large area of grade 3 chondromalacia with flap separation of the articular surface in
the posterior aspect. This was treated by conservative chondroplasty. There was a
significant tear of the medial meniscus, which included a radial tear of the posterior 1/3
to the peripheral margin. The anterior and posterior cruciate ligaments appeared normal.
The lateral compartment was unremarkable.
DESCRIPTION OF PRODCEDURE: The patient was given a general anesthesia and
the left lower extremity was then prepped and draped. The tourniquet was inflated.
Anteromedial and anterolateral portals were accomplished.
(Continued on the next page.)

28
© Copyright 2008 American Academy of Professional Coders
The knee was examined and the findings are as indicated above. Attention was directed
to the medial compartment where using the various basket forceps and _______ the
meniscal fibers were excised. Copious irrigation was performed to remove any loose
fragment. After proper balancing and trimming of the meniscus a conservative
chondroplasty of the medial femoral condyle was performed. Copious suctioning of the
joint was performed. The patellofemoral joint was then treated also with
conservative chondroplasty. The instruments were removed. The incision was closed
with a nylon suture and sterile dressing applies. The patient tolerated the procedure well
and arrived in recovery in satisfactory condition.
Procedure Codes:
• 29881-LT Knee arthroscopy/surgery / RVU 16.04• G0289-LT Arthro, loose body + chondro / RVU 2.32
Diagnoses Code:
• 717.2• 733.72• 717.7

29
© Copyright 2008 American Academy of Professional Coders
Added Value - Workshop Exclusive:
RECOVERY AUDIT CONTRACTORS
SPECIAL OVERVIEW REPORT
Prepared By: The American Academy of Professional CodersDocument Version: 072008.01.STEPHANIEJONES
Last Updated On: 7/12/2008

30
© Copyright 2008 American Academy of Professional Coders
The Recovery Audit Contractor Program
Medicare receives 9,579 claims…per minute. It is reasonable to assume that
some improper payments will happen. However, try telling that to the mass of
Americans who are uninsured and still paying taxes that foot the hefty bill for
mistakes. According to the General Accounting Office, incorrect payments by
Medicare accounted for $10.8 billion in 2007 alone. American tax payers have cried
out, “stop the waste!” and US congress listened.
In 2005 a pilot program was implemented, designed to protect the Medicare Trust
Funds. The three year project resulted in correcting $1 billion of Medicare improper
payments from 2005 through March 27, 2008. It demonstrated that it was
successful in identifying and recovering overpayments as well as affecting a
“sentinel effect” that helps prevent future errors.
How it works:
RAC auditors are paid on contingency. This is good news for Americans in that the
cost of recovery is capped at 20 cents per recovered dollar. For the contractor, this
means that if they don’t find and recover overpayments, they can’t be paid for their
work. During the pilot, the RACs were allowed to select any claim from the data they
were given for which they could request documentation and/or audit. Only claims
previously or currently under review, hospice, home health services, and E/M codes
(with regard to auditing the level of service) were excluded. A majority of the review
centered on higher paying claims that were more likely for error, which meant that
Hospitals were reviewed in greater proportions than physicians.

31
© Copyright 2008 American Academy of Professional Coders
Although proven by survey that almost 75 percent of providers felt that RAC audits
were fair and reasonable, some providers expressed concerns about the contingency
model. They feared a “witch hunt” where RACs would desperately ferret out
innocent errors or interpret guidelines to their own benefit in an attempt to ensure
covering their operating costs. To address this concern, the national RAC program
will use separate independent reviewers to sample and validate all RAC results. In
addition, RACs will be required to use medical directors to oversee the process and
Certified Professional Coders.
The Future:
The national RAC program will be fully implemented by 2010. A large amount of the
recoveries in the pilot were “black-and-white” caused by billing issues, such as
duplicate claims and wrong fee schedule amounts. Perhaps for this reason only 14
percent of the RAC audit results were appealed, of which less than 5 percent were
overturned. In the permanent national RAC program, new contractors will be initially
limited to these types of reviews and then gradually expanded to other areas such
as further coding errors and medical necessity.
RAC Pilot Project Snap Shot: Pertinent to Physicians Only:
• Number of claims reviewed: 792,387,525
• $19.9 Million collected
5 percent Duplicate Claims
54 percent Excessive/Multiple Units
41 percent Other (wrong coding, medically unnecessary, etc.)
• Average overpayment per physician claim: $150
• Average overpayment per physician per year: $800
Note: For more information http://www.cms.hhs.gov/RAC

© Copyright 2008 AAPC, written by Stephanie Jones, CPC, CPC-E/M
HOW TO DISSECT OPERATIVE REPORTS TO FIND MISSING PIECES
AAPC
Click to add presenter name
Agenda
• Presentation 9:00-10:00 am
• BREAK 10:00-10:15
• Presentation 10:15-11:30
– Added Value: Workshop Exclusive
• RAC UPDATE 11:30-Noon (Dismiss)

Introduction• Missing Pieces = Big headache
– Are all billable services being captured by the coder?– Are services necessary and otherwise supported?– Dx properly reflect the pre and post-operative condition?– Have all compliance issues been properly adhered to?
• Coder productivity and the adverse impact on AR– Backlogs– Inaccuracies
• Offices are looking to eliminate– Missed opportunities– Rejections/Denials– Reduce risk of errors in coding
Introduction (continued)• Computer Assisted Coding software (CACs)
– CACs “read” medical records and suggest codes• These codes must be validated by coders
• CACs may not intuitively find what was NOT documented
– CACs are growing in use where…• Documentation is already in an electronic format
• Documented medical terms are limited and recurring– Orthopedics
– Gastroenterology
– Interventional Cardiology
– Podiatry
– Urology
– CACs cut down coding time

Introduction (continued)• This class is designed to:
– Provide a simple framework for coders who areworking with or without CACs
• This class will discuss:– Operative report coding/billing and methods for
achieving best results
• This class will review:– Risk avoidance– Documentation– Billing and Coding
Before you can code it…
• Step 1
– Comprehension

Understand the Procedure
• Reading it is not enough!– Operative report
– Pathology report
– Other supporting documentation
• Coders must completely understand:– Content
– Instruments
– All medical terms
Being New to a Procedure
• Focus initial discovery efforts on thesummary procedures
– These procedures may not be listed correctly
– The body of the report reveals what was done
• This is just a good place to start
– What you learn will tell you If the body of thereport accurately portrays the summary

“Puce” versus “Purplish Red”
• There are several different ways to saythe same things
– The words in the CPT® code may not be anexact match in the operative report
– Surgical supplies or instruments will holdclues
• A thorough understanding of theanatomy is needed
Before you can code it…
• Step 2
–Visualization

The Highlighter• 20% of an operative report contains words
that are less important to a coder– CACs or paper with highlighter pens help break
the information down to “see” what codes aredocumented
• “Key words” (next slide)
• Unfamiliar words (that require your research)
• Key Words to highlight may appear in:– Any tense
– In a singular or plural format
Examples of Keywords
• Look for Physical Locations:
– The Anatomical Structures involved
• The surgical site
• Components within and around the site
– You will learn with time what locations arepertinent
• When new, highlight them all

Examples of Keywords (continued)• The Procedure Method points the direction to the procedure and the
code specific to the technique--Examples may include:
– Arthrodesis– Burr, Puncture– Debridement– Destruction– Dilation– Drainage– Excision– Exploration– Fusion– Graft– Harvest
Examples of Keywords (continued)– Implantation
– Incision
– Injection
– Infusion
– Introduction
– Ligation
– Paring
– Plicate
– Probe
– Reconnection
– Reconstruction
– Release

Examples of Keywords (continued)– Removal
– Repair
– Replacement
– Resection
– Screening
– Scope /-oscopy
– Snare
– Shaving
– Transfer
Examples of Keywords (continued)• Type
– Simple, Intermediate, Complicated, Extensive– Radical, Complete, Partial– Conversion, Revision– Open, Closed
• NOTE: Surgeon may use a different definition than the procedurecode allows for
• Size/Number– Separate Incisions, Excisions– Centimeters, Small, Medium, Large– Number Of Visits (i.e. Maternity Care)
• Surgical instrument/s used

Before you can code it…
• Step 3
–Research
How to Research• It is not enough to ask a co-worker
• Know valid answers to the following (and more)
– What is the Specialty specific terminology?
– What does the procedure itself look like?
– What conditions normally prompt the procedure?
– Are there various approaches to the procedure?
• Common coding sense is a learned skill
– Speed with practice

How to Research (continued)
• Examples of Published Tools:– Professional Associations
• AAOS Complete Global Service Data for Orthopedic Surgery
• AAPC Web site (member area under “search”)
– AMA• CPT® Assistant Archives CD 1990-2007
• CodeManager®
– Ingenix• The Coding Companion
• The Coder’s Desk Reference
How to Research (continued)
• Internet Research:
– http://google.com
– Medical term look up
– Anatomy
• Using the search terms “anatomy of the stomach”returns more than 30 images that detail thestructures of the stomach.

How to Research (continued)
• Local Coverage Determinations:– Gain insight on “reasonable and necessary”
information and medical necessity requirements
– Anticipate if a claim will be allowed based on theICD-9-CM codes documented
– Usually available on the local carrier website
– CMS searchable links fromhttp://www.cms.hhs.gov/DeterminationProcess/04_LCDs.asp
How to Research (continued)
• Ask a Surgeon:
– Some practices will allow their coder anopportunity to watch an actual procedure
– Many surgeons are happy to explain theintricacies of the procedure
• “I’d like to make sure that we eliminate missedcoding opportunities. Could you walk me throughthe procedure?”

Before you can code it…
• Step 4
– Contemplation
Finding the Missing Pieces
• A “missing piece” is anything that putsaccurate billing/coding in harm’s way
• This includes:– Missing opportunities for appropriate revenue
from the surgery
– Missing something that relates to compliance

Coding & Documentation (cont.)
• Unreported activity and CERT
Coding & Documentation
• Unreported activity– Develop extreme familiarity with surgeries to identify
when something was probably done… and notdocumented
• When undocumented services are suspected present thedocumentation to the surgeon
• It may be necessary to append the report with the missingand additional documentation
• Undocumented services cannot be coded.

Coding & Documentation (cont.)• Radiology codes that are billable by the surgeon
– Some surgical procedures require the use of imagingguidance and the surgeon provides supervision andinterpretation.
– A good clue: notes in the professional procedure codebook such as found in the AMA CPT 2008 Professionalversion (i.e. 36005)
– Examples include:• Biopsies and Abscess Drainage• Gastrostomy Tubes (i.e. new code 49440)• Saline Infused Sonohysterography• Arthrography• Biliary Duct Dilation & Stent Insertion• Selective Catheter Placement
Coding & Documentation (cont.)
• The Modifier 22– Extensive well-documented adhesions
– Presence of excessively large surgical specimen
– Trauma extensive enough to complicate the procedure
– Other pathologies that directly interfere with theprocedure but are not billed separately
– Excessive blood loss for the particular procedure
– Unusually lengthy procedure

Coding & Documentation (cont.)• The Modifier 59
– Never use the modifier solely as a method to getaround a CCI or other payer bundling edit
• Different site or organ system?
• Separate incision or excision?
• Separate lesion?
• Separate injury?
• Not “Black and White”– For example, is the knee a single location or is it 3?
• Should a HCPCS Level II code, such as G0289 be used?
• Or modifier 59
• Or 51?
Coding & Documentation (cont.)
• Use of an operating microscope– When the operating or surgical microscope is used it
should be coded when the surgical codes do notalready include the operating microscope in thedescription of the code (i.e. code 15757).
– Different payer bundling edits may include this codewith other surgical codes and it may be disallowed.
– 69990 should not be reported with modifier 51.

Coding & Documentation (cont.)
• Correct number of units
– Avoid lost charges for missed units of serviceand do not inflate the number of units byinnocent error or otherwise.
– Make certain the appropriate number is listedin the units column on the claim form.
Coding & Documentation (cont.)
• Appropriate Pre-op visits
– It may be necessary for the patient to see thesurgeon 2-3 days before surgery
• If a physician routinely provides a service that iswholly related to the surgery-- billing theseservices could be abusive
– Watch for nature of the visit & necessity
» Often require the opinion of a physician

Coding & Documentation (cont.)
• Surgical Post Op Calendar Days
– Because major surgeries have 90 calendardays attached to the global period, it isimportant to keep a calendar that will alert thecoder when a new service is now outside theglobal period
– See Attachment A of this curriculum for ahandy date reference
Coding & Documentation (cont.)• Key Modifiers
– Unrelated E/M Services• 24 E/M service that is unrelated to the surgical
procedure during the postoperative (follow-up) period
– Global period returns to the OR for complicationsor a more extensive procedure
• 76 Repeat procedure by same provider
• 78 Return to the operating room for a related procedureduring a postoperative period
• 79 Unrelated procedures by the same physicianduring the post-operative period
• 58 Staged or related procedure

Modifier Review• 25 Separately Identifiable E/M on the Same Day as a Minor
Procedure
• 50 (LT or RT) Bilateral Surgery: Typically the second side is only0- 75% of the allowable for the first side.
• 51 Multiple Procedures: List the procedure with the highest valuefirst and list additional procedures in descending value. Typicallyreimbursement of subsequent procedures is reduced, 0-50%.
• 52 Reduced Services: A (non-hospital OP)service partially eliminated by election.
Modifier Review (continued)• 53 Discontinued Service: a (non hospital outpatient) service that
was discontinued by the physician due to (non elective)
• 54 Surgical Care Only: Typically, reimbursement for the surgery is70%
• 55 Post-operative Care Only: Typically, reimbursement for thepre/post op care is 30%
• 57 E/M Service that Results in the Initial Decision for Surgery.
• 62 Two Surgeons: This is not surgery assisting.

Modifier Review (continued)• 63 Procedure on Infant less than 4 kg: Work is increased due to the
weight of the infant or neonate.
• 66 Surgical Team: Several surgeons of different specialties
• 77 Repeat Procedure by Another Physician: Another physicianrepeated a procedure after the original service
• 80 Assistant Surgeon
• 81 Minimum Assistant Surgeon
Coding & Documentation (cont.)
• The Best Way to Reflect the TrueService
– There are times when the actual servicesrendered are better described by less obviouscodes
• For example, an orthopedic surgeon who provides closedfracture treatment without manipulation may better representhis or her work by coding E/M services rather than coding theFx care (check payer contracts and policies)

Discuss Concerns
• Remember that if you are scratchingyour head in confusion - a payerauditor may also
– For example, if you note that 100% of thebladder tumors removed by your surgeonemployer are documented as “Large” it maybe appropriate to point out that the proportioncould be a “red flag” to payers to audit
Medical Necessity
• Proper ICD-9-CM coding is important forestablishing the medical necessity of theencounter
• One of the more costly mistakes made bysome practices include:
– Reporting undocumented, probable orsuspected diagnoses:
• Can be construed as abuse/or fraud, andresult in recovery of payments.

Unlisted Procedures• Call your insurance rep
• Contact the Medical Director
• Provide payers detaileddocumentation of:– The nature, extent, and need for the procedure
– The time, effort, and equipment necessary
– Complexity of patient symptoms and relevantphysical findings
– Necessary follow-up care
– Final diagnosis
Unlisted Procedure (continued)• Claims for unlisted procedures are usually
processed manually
• Pre-authorization may be needed to ensurepayment
• Relate how the procedure fits:
– The patient’s eligible benefit structure
– That the procedure is not experimental or investigational.
• Making a comparative value to an existingprocedure code can also be helpful.

Now you can code it…and
• Step 5
– Compensation
Billing and Payment• Prior authorization for the procedure is
obtained
• Codes are ordered per RVU value.
• Correct reimbursement per the negotiatedallowable is made including:– Appropriate patient provider splits
– Appropriate reimbursement of modifier that affect fees
– Appropriate reimbursement for multiple procedures
– Appropriate adjudication practices for bundling &coverage decisions

Practical Examples
• Please turn to page 16 in yourworkbook
Practical ExamplesPlease turn to pages 16-17 in your workbook
Coding Solution:
– 57288 (linked to 625.6)
– 57250-22-51 (linked to 618.04 & 618.6)
– 51102-51 (linked to 788.20)
Coding Rationale:
• The enterocele plication is bundled into the sling procedurebecause it is listed as a CPT “separate procedure”
• Adding a modifier 22 to 57250 is arguably appropriate
• The cystourethroscopy is not reportable

Discussion• What were the missing pieces found with this report
example?
• What would the coder need to be aware of to followfor proper payment?
• What would be examples of what to avoid with thisnote to ensure compliance?
Practical Examples (continued)• Please turn to pages 18-19 in your workbook
Coding Solution:– Consult 99242-25 (linked 578.1 and V16.0)
– Occult Blood Smear 82272 (linked to 792.1 and V16.0)
– Colonoscopy w/ polyp by snare- 45385 (linked to 211.3 & V16.0)
– Colonoscopy w/ polyp by snare- 45385-51 (linked to 211.3 & V16.0)
Coding Rationale:
• In this case the consultation is separately reported because theGI physician’s opinion was the reason for the visit.

Discussion• What were the missing pieces found with this report
example?
• What would the coder need to be aware of to followfor proper payment?
• What would be examples of what to avoid with thisnote to ensure compliance?
- Question & Answer -

Workshop Exclusive
RACs:SPECIAL AAPC REPORT
Workshop Exclusive
• According to the General Accounting Office, Medicare beneficiariesaccounted for $10.8 billion in improper payments during 2007 alone.
• The three year RAC pilot project resulted in correcting$1 billion of Medicare improper payments from 2005 through March27, 2008.
• It demonstrated that it is successful in identifying and recoveringoverpayments as well as affecting a “sentinel effect” that helpsprevent future errors.
• RAC auditors are paid on contingency

Workshop Exclusive
• Only claims previously or currently under review, hospice,home health services, and E/M codes (with regard toauditing the level of service) were excluded.
• A majority of the review therefore centered on higherpaying claims that were more likely for error, which meantthat Hospitals were reviewed in greater proportions thanphysicians.
• Almost 75% of providers felt that RAC audits were fair andreasonable
Workshop Exclusive
• The national RAC program will be fully implemented by 2010.
• The national RAC program will use separate independentreviewers to sample and validate all RAC results.
• In addition, RACs will be required to use medical directors tooversee the process and Certified Professional Coders.
• A large amount of the recoveries were from duplicate claims andwrong fee schedule amounts.
• Only 14% of the RAC audit results were appealed, of which lessthan 5 percent were overturned.

Workshop Exclusive
RAC Snap Shot: Pertinent to Physicians Only
• Number of claims reviewed: 792,387,525
• $19.9 Million collected
• 5% Duplicate Claims
• 54% Excessive/Multiple Units
• 41% Other (wrong coding, medically unnecessary,etc.)
• Average overpayment per physician claim: $150
• Average overpayment per physician per year: $800