Embed Size (px)
Citation preview

Journal of the American Society of Nephrology 1703
High-Flux Dialysis Membranes Improve Lipid Profile inChronic Hemodialysis Patient&’2Peter J. Blankestijn,3 Pieter F. Vos, Ton J. Rabelink, Herman J.M. van Rijn, Hans Jansen, and
Hem A. Koomans
P.J. Blankestijn. T.J. Rabelink. HA. Koomans. Depart-ment of Nephrology, University Hospital, Utrecht, TheNetherlands
H.J.M. van Rijn, Department of Clinical Chemistry,University Hospital, Utrecht, The Netherlands
P.F. Vos. Home Dialysis Foundation, Utrecht, TheNetherlands
H. Jansen, Department of Internal Medicine Ill andBiochemistry. Erasmus University. Rotterdam , theNetherlands
(J. Am. Soc. Nephrol. 1995; 5:1703-1708)
ABSTRACTIn a controlled prospective trial, the effect of a switch
from cellulose-based, low-flux dialysis membranes topolysulphone, high-flux membranes on lipid param-
eters was evaluated. Baseline values of lipid param-eters were identical in the study group and the controlgroup in which the dialysis membrane remainedunchanged. After 6 wk, total triglyceride, very low-
density lipoprotein (VLDL) triglyceride, and VLDL cho-
lesterol decreased, respectively, 28 ± 17 (P < 0.01), 38± 17 (P < 0.01), and 24 ± 21% (P < 0.05), and theproportion of total cholesterol that was high-densitylipoprotein cholesterol increased from 15 ± 5 to 18 ±5% (P < 0.05) in the high-flux polysulphone group,whereas these variables remained unchanged in thecontrol group. Low-density lipoprotein and total cho-lesterol as well as Kt/V, protein catabolic rate, para-thyroid hormone, albumin, and body weight did not
change. No change in Iipoprotein Iipase activity wasfound. In a second study, the effects of a singlehemodialysis session with high-flux polysulphone and
low-flux, cellulose-based membranes on lipid param-
eters and lipolytic activity were compared in a cross-over fashion. Treatment with both membranes re-
suIted in a significant decrease in plasma triglyceride,VLDL triglyceride, and VLDL cholesterol. Lipoproteinlipase activity increased during hemodialysis.
1 ReceIved June 28, 1994. Accepted November 30, 1994.
2 Part of this study has been presented at the 26th Annual Meeting of the
American Society of Nephrology, November 14-17, 1993, Boston, and publishedin abstract form In JASN (1993:4:334).
3 correspondence to Dr. P.J. Blankestlin, Room F03.226. Department of Nephrol-ogy, UnIversity Hospital, P.O. Box 85500, 3508 GA Utrecht, The Netherlands.
1044.6673/0509-1 703$03.00/0Journal of the American Society of Nephrologycopy�ght C 1995 by the American Society of Nephrology
Changes in lipid parameters and lipolytic activity
were identical during the two treatments. These dataindicate a favorable change in lipid parameters afterthe switch from low-flux, cellulose-based to high-flux,
polysulphone dialysis membranes that appeared notto be caused by an enhancement of lipoproteinlipase activity. Changes are of similar magnitude as
can be obtained with dietary and pharmacologic
treatments.
Key Words: Hemodialysis, high flux, lipid abnormallties
T he typical lipid profile of patients undergoing
chronic hemodlalysis treatment demonstrates a
moderate increase in triglyceride, normal cholesterol,
decreased high-density lipoprotein (HDL) cholesterol,and increased lipoprotein (a) ( 1 ). At present, it Is not
completely clear to what extent these abnormalities
contribute to the high Incidence of cardiovascular
morbidity and mortality in these patients. However, in
the normal population, this profile is associated
with an increased risk of cardiovascular disease, and
a decrease of triglyceride levels might reduce this
risk (2).
The concentrations of lipoproteins in renal failure
patients may be increased as a consequence of in-
creased synthesis, decreased catabolism, or a combi-
nation of both processes. There is some evidence of an
increased synthesis (3). However, most studies indi-
cate that decreased breakdown predominates ( 1),
which has been ascribed, at least in part, to reduced
lipid catabolism, secondary to reduced activity of lipo-
lytic enzymes, i.e. , lipoprotein lipase (LPL) and hepatic
lipase (HL) (4). LPL Is bound to the luminal surface of
the capillary endothellal cells, where hydrolysis takes
place. It can be released Into the bloodstream by
heparin, which causes an acute decrease in triglycer-
ide (4,5). This heparin-induced lipolysis is markedly
diminished In hemodlalysis patients (4,5). Suggested
underlying mechanisms of the reduced lipolytic activ-
ity include depletion of LPL stores by repeated admin-
istration of heparin (5), the existence of LPL inhibi-
tor(s) in uremic plasma (6), and increased levels of
apolipoprotein CIII (7), whIch is an inhibitor of lipolytic
activity. Also, hyperparathyroidism might play a role,
although the exact mechanism is unclear (8). Finally,
cytokines produced during dialysis might be able to
reduce LPL activity (9). The type of dialysate buffer,
that is, acetate or bicarbonate, does not seem to
influence lipid parameters (10), whereas dialysate glu-
cose concentration up to 1 1 mmol/L does not contrib-
ute to the dyslipidemla ( 1 1). Some data suggest that
Lipid Profile During High-Flux Dialysis
1704 Volume 5 - Number 9 - 1995
switching from regular to low-molecular-weight hepa-
rin might influence dyslipidemia beneficially (12).
Some recent data Indicate that patients undergoing
dialysis with high-flux membranes show lower predi-
alysis triglyceride as compared with more traditional
membranes (13-15). Seres et a!. (15) found that LPL
activity after high-flux hemodialysis was higher than
after dialysis with cellulose-based membranes and
suggested that this could be the cause of the triglyc-
eride-lowering effect. However, the interpretation of
these studies ( 13-15) Is not without difficulties, be-
cause confounding factors such as dialysis character-
istics, diet, medication (especially heparin), and levels
of parathyroid hormone were changed or not men-
tioned, and blood samples were taken either in a
nonfasting or in a fasting state. Therefore, we evalu-
ated in a prospective, controlled trial whether a switch
of low-flux, cuprophane to high-flux, polysulphone
membranes has a beneficial effect on lipid parame-
ters. Dialysis characteristics, heparin dosage, medica-
tion, and diet were not changed and were evaluated. In
addition, we compared the acute effects of a single
hemodialysis treatment with either membrane on LPL
activity and lipids.
PATIENTS AND METHODS
Patients
The total population of our institution comprises approxi-mately 1 20 chronic hemodialysis patients. Of this popula-tion, we included 28 consecutive, stable, long-term (>6months on hemodialysis) patients ( 10 male), who were onlow-flux, cuprophane membranes (Asahi AM 140 and 160Nova: Asahi Medical Co, Tokyo, Japan). All were white and
gave informed consent. Patients were excluded when theywere diabetic or were on medications that raise or lowerlipids. Bicarbonate dialysate containing 1 1 mmol/L glucosewas used throughout. The diet comprised 1 .0 to 1 .2 g/kgbody wt of protein, 30 to 35% of caloric Intake as fat, and 50to 55% as carbohydrates. Primary renal diagnosis was un-known in six patients, chronic pyelonephritis with or without
urolithiasis in seven, glomerulonephritis in five, Alport’sdisease in one, polycystic kidney disease in five, glomerulo-
sclerosis in two, and hypertension in two. The median age(range) was 63 (22 to 80) yr, duration on hemodialysistreatment was 24 (6 to 1 76) months, two patients weredialyzed twice, and the remainder were dialyzed thriceweekly. Mean ± SD duration of therapy per week was 1 1 ±
1 .4 h. Total amount of heparmn administered during dialysiswas 15.247 ± 3.462 U/wk. Regular heparmn was used. The28 patients were randomly divided in two groups. Before thestart of the study, it was ascertained that the two groupswere comparable with respect to lipid parameters by com-paring the mean values of cholesterol and triglyceride mea-surements, which were done routinely every 4 months. Four-teen patients (Group A) were studied before and after switchto high-flux membranes: in the remaining 14 patients (GroupB), the dialysis membrane remained unchanged.
Protocols
The two groups were studied according to the followingprotocol. After an overnight fast, blood was collected from thearteriovenous fistula before dialysis for lipid parameters and
parathyroid hormone. Subsequently, 50 U/kg body wt ofregular heparin was injected iv in the contralateral arm. After20 mlii, blood was collected from the arteriovenous fistula ina chilled tube for LPL. In the week before the blood collection,calculated Kt/V and protein catabolic rate were recorded.Residual renal function was taken into account. From thenext dialysis session onward, the patients in Group A weredialyzed with a F6OS polysulphone, high-flux dialyzer (Fre-senlus AG, Bad Homburg, Germany). In both groups, bloodand dialysate flow, length and number of weekly sessions,and total amount of heparmn used during dialysis, as well asmedication and diet, were not changed during the studyperiod. Six weeks after the first measurements of lipid pa-rameters, blood was collected by the use of the same proto-col. Dialysis membranes were used only once. Diet adher-ence was evaluated by the use of a diet diary at baseline andafter 6 wk.
In a second study, six chronic hemodialysis patients (3
men) were randomly selected from the previous study group.In random order, 1 wk apart, they were treated with thehigh-flux, polysulphone or the low-flux, cuprophane mem-brane after an overnight fast. They were not allowed to eat ordrink during the dialysis session. Blood was sampled before,during, and at the end of the dialysis. After blood samplingfor basal values, a bolus injection of 2,500 U of heparin wasgiven at the start of dialysis. Then, a continuous infusion ofheparin was instituted: the dose was adjusted according tothe results of periodic partial thromboplastin time determi-nations but was the same during both studies. All patientswere treated three times for 3.5 h a week.
Methods
Lipid parameters were measured as described previously(16). In brief, for the separation of lipoproteins, plasmasamples were subjected to a single ultracentrifugation stepat 4#{176}Cfor 20 h in a 50.3 Ti rotor (Beckman Instruments, PaloAlto, CA). Cholesterol and triglyceride were measured with afully automated Hitachi 7 1 7 analyzer from Boehringer
Mannheim GmbH (Mannheim, Germany) with the enzymaticapplications with reagents obtained from the same company.The phosphotungstlc acid-magnesium chloride precipitationmethod was used to measure HDL cholesterol together withthe cholesterol-cholesteroloxidase-phenol 4-aminophenazonemethod. Lipoprotein (a) was measured as described elsewhere(17).
LPL and HL were determined separately by an immuno-chemical method, essentially as described by Huttunen et a!.(18), with a gum acacia-stabilized l3Hltrioleoylglycerol emul-
sion. HL activity was determined as the salt-resistant lipasein the presence of 1 M NaC1. LPL activity was determinedafter the Inhibition of HL with a goat antibody raised againstHL purified from postheparin human plasma. Fasted ratserum was added as a source of apolipoprotein CII. A traceramount of I ‘4Cloleate was added to the substrate as aninternal standard for the extraction of l3Hjoleate liberatedfrom [3Hltrioleoylglycerol substrate. In each series of deter-minations, pooled plasmas with high and low LPL and HLwere included as a reference. The normal values of LPL are>70 U/L in men and >80 U/L in women and ofHL are >300U/L in men and >225 U/L in women.
Kt/V was calculated with the urea values determinedbefore and after hemodialysis (19). Data are presented asmean ± SD. Results of both studies were analyzed by atwo-way analysis of variance. If the variance ratio obtainedby the analysis of variance reached statistical significance,
75
50
25 Ia)C(a
.C
0a)Ca)0
a)
I-25
-50
-75
I**
LT��rr
Blankestijn et al,
Journal of the American Society of Nephrology 1705
the differences between the means of the observations were
analyzed at the 5 and 1% significance levels by the least
significance difference test.
RESULTS
The patients who were switched to the high-flux
membrane (Group A) and the control patients (GroupB) did not differ with regard to age, duration on
chronic hemodialysis therapy, frequency (in both
groups, one patient twice weekly and the remainder
thrice weekly), length of weekly sessions ( 10.0 ± 1.5
versus 10.8 ± 1 .4 h/wk), and total amount of heparin
administered during the hemodialysis session (14.835
± 2,230 versus 16.398 ± 3,900 U/week). The switch
did not cause any clinically detectable changes or side
effects, although the study was not specifically de-
signed to address this question. Lipid parameters at
baseline did not differ (Table 1 ). After 6 wk of treat-
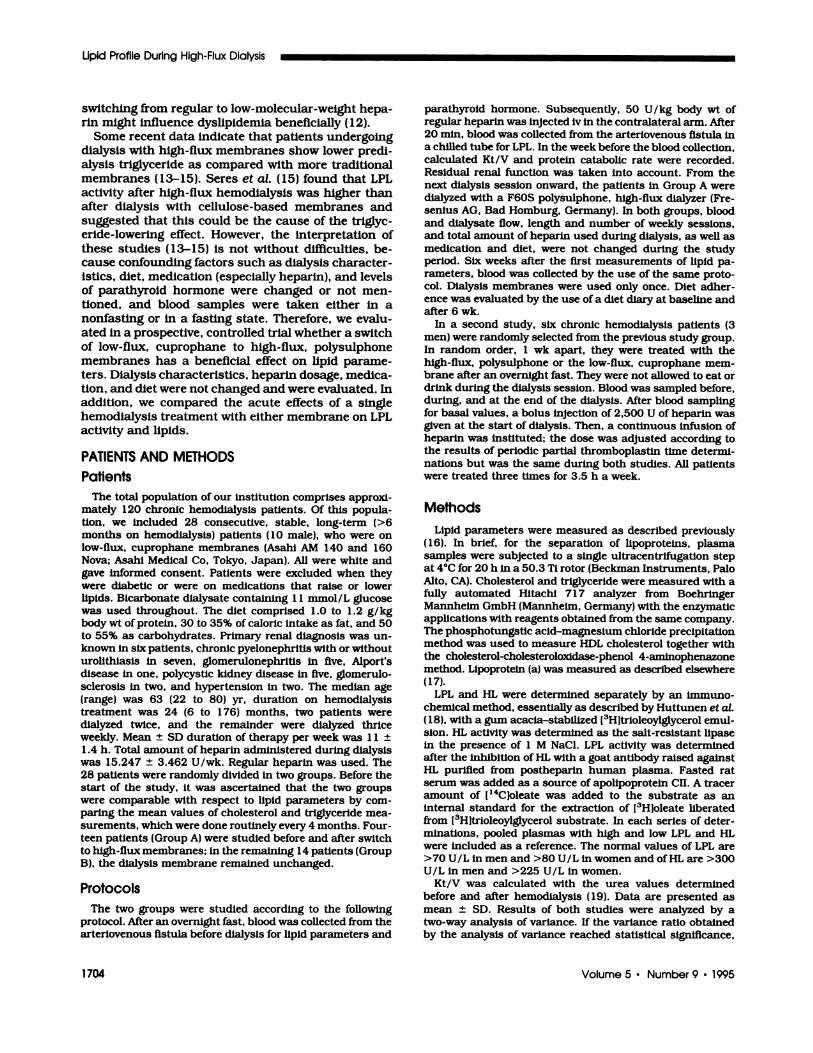
ment with a high-flux membrane, fasting total triglyc-
eride, very low-density lipoprotein (VLDL) triglyceride,
and VLDL cholesterol were significantly decreased In
Group A, respectively, by 28 ± 17 (P < 0.01), 38 ± 17
(P < 0.01), and 24 ± 21% (P < 0.05)(Table 1; Figure 1).
Other lipid parameters did not change; however, the
contribution of HDL cholesterol to total cholesterol
increased from 15 ± 5 to 18 ± 5% (P < 0.05) in the
high-flux group. LPL and HL were low and showed no
change in Group A and were therefore not measured
in Group B (Table 1 ). Baseline Kt/V, protein catabolic
rate, parathyroid hormone, and body weight, as well
as albumin, were not significantly different and re-
maimed unchanged in both groups (Table 2). Residual
renal function did not change.
In the second study, we found that, during dialysis
sessions with the high-flux, polysulphone membrane
and with the low-flux, cuprophane membrane, there
was a clear effect on lipid parameters. Baseline values
were identical (Table 3). In all six patients, triglyceride
decreased within 1 h ofhemodialysis from 2.27 ± 0.47
TG VLDL-TG VLDL-chol
Figure 1 . Percent change in lipids. Open bars, high-fluxpolysulphone; hatched bars, low-flux, cellulose based. TG,triglyceride; chol, cholesterol. Comparison with value atweek 0: � = P < 0.05, ** = � < oo��
to 1 .33 ± 0.36 during high-flux polysulphone and
from 2.38 ± 0.88 to 1 .6 1 ± 0.7 1 mmol/L during
low-flux cellulose based (both P < 0.05) and remained
low during the remainder of the dialysis session (Table
3). VLDL triglyceride and VLDL cholesterol decreased
significantly during both treatments (Table 3). There
were no differences in the degrees of decrease in lipids
between the two membranes. Lipolytic activity was
undetectable before the start of hemodialysis, in-
creased within 1 h, and decreased toward the end
(Figure 2). Values at 1 , 2, and 3.5 h of hemodialysis
were, respectively, during high-flux polysulphone 30
± 10, 13 ± 6, and 9 ± 8 U/L and during low-flux
cuprophane 29 ± 12, 7 ± 2, and 6 ± 3 U/L. There was
no difference between the two study groups.
DISCUSSION
This is the first prospective, controlled trial examin-
ing the effect on lipid profile of a switch from low-flux,
TABLE 1 . Lipid profile before and after switch to dialysis with high-flux polysulphone membranea
ParameterHigh Flux Control
WeekO Week#{243} WeekO Week 6
Total TG (mmol/L) 2.58 ± 1.17 1.82 ± 0.59c 2.43 ± 0.96 2.48 ± 0.80VLDL TG (mmol/L) 1.88 ± 1.30 1.08 ± 0.44c 1.71 ± 0.96 1.71 ± 0.85HDL + LDL TG (mmol/L) 0.78 ± 0.22 0.74 ± 0.19 0.72 ± 0.22 0.77 ± 0.18Total chol (mmol/L) 5.18 ± 1 .1 1 4.71 ± 0.95 5.07 ± 0.89 5.20 ± 0.57VLDL chol (mmol/L) 1.45 ± 0.61 1 .04 ± 037b 39 ± 0.76 1.33 ± 0.53LDL chol (mmol/L) 2.98 ± 0.72 2.87 ± 0.73 2.84 ± 0.82 2.99 ± 0.59HDL chol (mmol/L) 0.75 ± 0.16 0.81 ± 0.16 0.85 ± 0.20 0.88 ± 0.19HDL/total chol (%) 15.3 ± 4.5 18.0 ± 50b 16.8 ± 3.7 16.8 ± 4.1Lp(a) (mgIL) 350 ± 243 340 ± 130 328 ± 242 412 ± 178
LPL (U/L) 83 ± 35 89 ± 25HL (U/L) 243 ± 66 250 ± 58
a Data are means ± SD. In the control group. the dialysis membrane remained unchanged. 1G. triglyceride; chol, cholesterol; Lp(a), lipoprotein A;
LDL, low-density lipoprotein.b p < 0.01 , comparison with value at Week 0.C p < 0.05, comparison with value at Week 0.
2
time (h)
Lipid Profile During High-Flux Dialysis
1706 Volume 5 ‘ Number 9 ‘ 1995
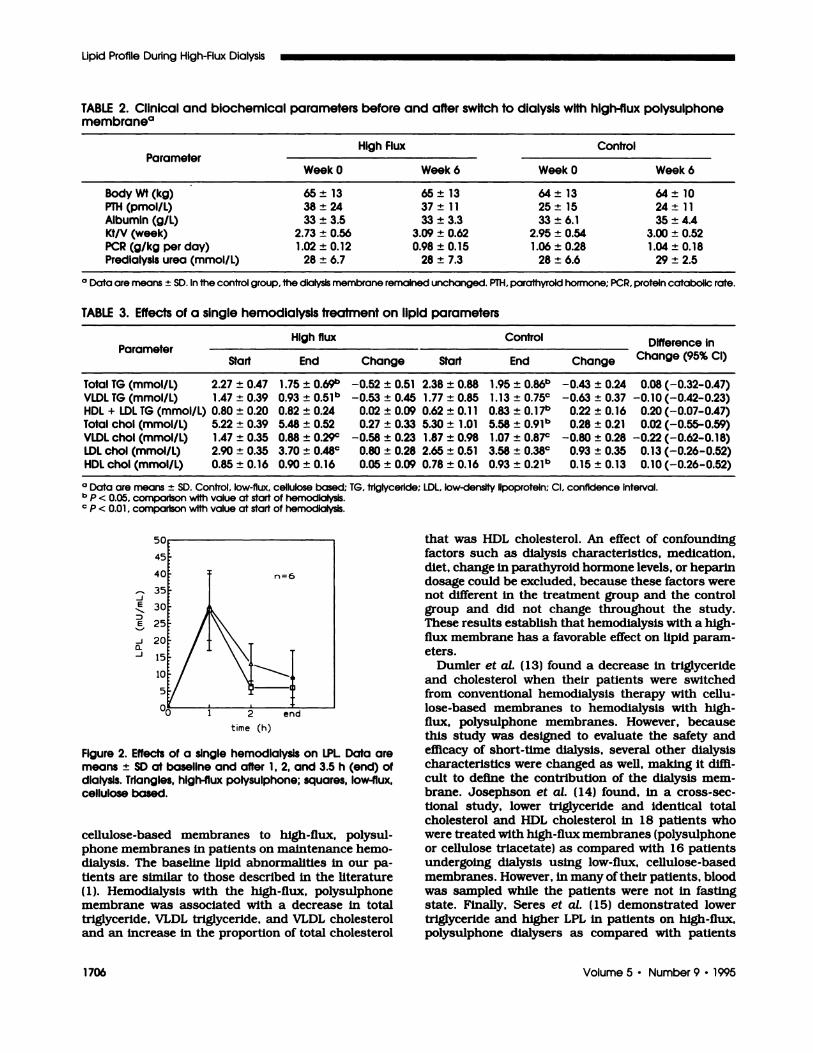
TABLE 2. Clinical and biochemical parameters before and after switch to dialysis with high-flux polysulphonemembranea
ParameterHigh Flux Control
Week 0 Week 6 Week 0 Week 6
BodyWt(kg) 65±13 65±13 64±13 64±10
PTH (pmol/L) 38 ± 24 37 ± 11 25 ± 15 24 ± 11
Albumin (gil) 33 ± 3.5 33 ± 3.3 33 ± 6.1 35 ± 4.4Kt/V (week) 2.73 ± 0.56 3.09 ± 0.62 2.95 ± 0.54 3.00 ± 0.52PCR (g/kg per day) 1.02 ± 0.12 0.98 ± 0.15 1.06 ± 0.28 1.04 ± 0.18Predlalysis urea (mmol/L) 28 ± 6.7 28 ± 7.3 28 ± 6.6 29 ± 2.5
0 Data are means ± SD. In the control group, the dialysis membrane remained unchanged. PTH, parathyroid hormone; P�R. protein catabolic rate.
TABLE 3. Effects of a single hemodialysis treatment on lipid parameters
ParameterHigh flux Control Difference in
Ch 95% CIange ( )Start End Change Start End Change
Total TG (mmol/L) 2.27 ± 0.47 1.75 ± 069b -0.52 ± 0.51 2.38 ± 0.88 1.95 ± 086b -0.43 ± 0.24 0.08 (-0.32-0.47)VLDL TG (mmol/L) 1.47 ± 0.39 0.93 ± 051b -0.53 ± 0.45 1.77 ± 0.85 1.13 ± 0.75C -0.63 ± 0.37 -0.10 (-0.42-0.23)HDL + LDL TG (mmol/L) 0.80 ± 0.20 0.82 ± 0.24 0.02 ± 0.09 0.62 ± 0.1 1 0.83 ± 017b 0.22 ± 0.16 0.20 (-0.07-0.47)Total chol (mmol/L) 5.22 ± 0.39 5.48 ± 0.52 0.27 ± 0.33 5.30 ± 1.01 5.58 ± 091b 0.28 ± 0.21 0.02 (-0.55-0.59)VLDL chol (mmol/L) 1.47 ± 0.35 0.88 ± 0.29’� -0.58 ± 0.23 1.87 ± 0.98 1.07 ± 0.87c -0.80 ± 0.28 -0.22 (-0.62-0.18)LDI chol (mmol/L) 2.90 ± 0.35 3.70 ± 0.48c 0.80 ± 0.28 2.65 ± 0.51 3.58 ± 0.38C 0.93 ± 0.35 0.13 (-0.26-0.52)HDL chol (mmol/L) 0.85 ± 0.16 0.90 ± 0.16 0.05 ± 0.09 0.78 ± 0.16 0.93 ± 021b o�5 � 0.13 0.10 (-0.26-0.52)
a Data are means ± SD. control, low-flux, cellulose based; 1G. triglycerIde; LDL. low-density lipoprotein; cI. confidence Interval.
b p < 0.05, comparison with value at start of hemodialysis.C p < 0.01 . comparison with value at start of hemodialysis.
.J
E.�,-
E
-J
0.-J
Figure 2. Effects of a single hemodialysis on LPL Data aremeans ± SD at baseline and after 1, 2, and 3.5 h (end) ofdialysis. Triangles, high-flux polysulphone; squares, low-flux,cellulose based.
cellulose-based membranes to high-flux, polysul-
phone membranes in patients on maintenance hemo-
dialysis. The baseline lipid abnormalities in our pa-
tients are similar to those described in the literature
( 1). Hemodialysis with the high-flux, polysulphone
membrane was associated with a decrease in total
triglyceride, VLDL triglyceride, and VLDL cholesterol
and an Increase In the proportion of total cholesterol
that was HDL cholesterol. An effect of confounding
factors such as dialysis characteristics, medication,
diet, change in parathyroid hormone levels, or heparin
dosage could be excluded, because these factors werenot different in the treatment group and the control
group and did not change throughout the study.
These results establish that hemodialysis with a high-
flux membrane has a favorable effect on lipid param-
eters.
Dumler et a!. ( 13) found a decrease in triglyceride
and cholesterol when their patients were switched
from conventional hemodialysis therapy with cellu-
lose-based membranes to hemodialysis with high-
flux, polysulphone membranes. However, because
this study was designed to evaluate the safety and
efficacy of short-time dialysis, several other dialysis
characteristics were changed as well, making it diffi-
cult to define the contribution of the dialysis mem-
brane. Josephson et a!. ( 14) found, in a cross-sec-
tional study, lower triglyceride and identical total
cholesterol and HDL cholesterol in 18 patients who
were treated with high-flux membranes (polysulphone
or cellulose triacetate) as compared with 1 6 patients
undergoing dialysis using low-flux, cellulose-based
membranes. However, in many oftheir patients, blood
was sampled while the patients were not in fasting
state. Finally, Seres et a!. ( 15) demonstrated lower
triglyceride and higher LPL in patients on high-flux,
polysulphone dialysers as compared with patients

Blankestijn et al,
Journal of the American Society of Nephrology 1707
dialyzed with cellulose-based membranes. However,
their study was mainly cross-sectional. Moreover, be-
cause blood samples were obtained immediately after
dialysis, the steady-state effects on lipids and LPL
were not evaluated in that study.
The change in lipid variables In this study could very
well fit with an enhancement of lipolytic activity (5).
However, we found that the decrease in predialysis
triglyceride did not coincide with an increase in pre-
dialysis lipolytic activity. Therefore, we studied in a
subset of patients the effects of a single dialysis on
lipid parameters and lipolytic activity. Both dialysis
treatments caused similar decrements in triglyceride,
VLDL triglyceride, and VLDL cholesterol and an incre-
ment in low-density lipoprotein, presumably the re-
sult of the increased VLDL catabolism during dialysis.
This triglyceride-lowering effect of hemodialysis was
also found by others (20,2 1) and is probably caused by
the increase in plasma LPL activity. LPL is bound to
the endothelium and released by heparin (5). Teraoka
et a!. (20) found that lipolytic activity increased and
triglyceride levels decreased during hemodialysis with
heparmn, but not when heparin was omitted. We also
found a transient increase in LPL during hemodialy-
sis, but importantly, this effect was similar with the
two membrane types. Therefore, our data make It
unlikely that the long-term triglyceride-lowering effect
of high-flux membranes Is due to LPL stimulation. A
possible explanation is offered in a recent report by
Otsubo et a!. (22). They showed that treatment with
high-flux cellulose triacetate membranes decreased
triglyceride and increased HDL cholesterol and that
these changes were associated with a favorable
change in the apolipoprotein CII/CIII ratio. In that
study, apolipoprotein CII remained unchanged,
whereas apolipoprotein CIII decreased during treat-
ment with the high-flux membrane. This change
might be of significance. LPL requires interaction with
apolipoprotein CII to be active (5). Indeed, patients
with an apolipoprotein CII deficiency have a critically
impaired LPL-mediated lipolysis, although their pos-
theparin LPL activity is normal when measured in vitro
in the presence of exogenous activators (23). Apoli-
poprotein CIII is a competitive Inhibitor of apolipopro-
tein CII (5) and Is increased In uremic patients (7).
Therefore, a decrease in the apolipoprotein Cli/Cill
ratio renders a decrease in the susceptibility of the
substrate lipoprotein to LPL action, without affecting
in vitro LPL measurements.
The two types of membranes used In this study,
namely, low-flux, cellulose-based and high-flux, poly-
sulphone, differ from each other at least in two as-
pects, that is, in biocompatibility and in permeability.
One could Imagine that both differences might be of
importance is establishing the change In lipid proffie.
Cuprophane instead of synthetic membranes induce
cytokine release, which can cause a reduction in LPL
activity (9). This study could not confirm different
effects on LPL activity. Alternatively, high-flux mem-
branes might be able to remove more effectively lipase-
inhibiting factors (22). This possibility is supported by
the observation that high-flux membranes cause a
decrease in apolipoprotein CIII (22). It seems most
likely that the increased permeability of the present
high-flux membranes and not the fact that they weremade of polysulphone determines the lipid-lowering
effect, because Otsubo et a!. (22) reported similar
lipid-lowering results using another type of high-flux
membrane.
The exact contribution of lipid abnormalities in
determining cardiovascular morbidity and mortality
in end-stage renal failure patients is unknown at
present. Both hypertriglyceridemia and low HDL cho-
lesterol are recognized as risk factors for coronary
heart disease (24,25) and lowering low-density 11-
poprotein cholesterol together with lowering triglycer-
ide and Increasing HDL cholesterol reduces the coro-
nary risk in the nonuremic population (26). No such
data exist for end-stage renal failure patients, and It
remains to be established whether it is beneficial to
control the uremic lipid abnormalities, by whatever
means. Recently, It has been advocated that hyper-
triglyceridemia (triglyceride >2.26 mmol/L [200 mgI
dLfl, when in the presence ofcoexisting coronary heart
disease, diabetes mellitus, chronic renal failure, or
low levels of HDL cholesterol, should be treated (2).
One or more of these conditions usually exist in
hemodialysis patients. Studies in uremic patients
have documented the efficacy of dietary modulations
(27-29) or drugs such as clofibrate, gemfibrozil, and
bezafibrate (30-32). Of note, the presenily described
switch in dialysis membrane is equally effective as
dietary modifications (27-29) and almost as effective
as fibrates (30-32). The latter, however, can have
serious side effects in renal failure patients (33,34),
which limits their clinical use. This study indicates
that the choice of dialysis membrane offers an oppor-
tunity to reduce the dyslipidemla without adverse
effects and without problems with the compliance of
the patients.
ACKNOWLEDGMENTST.J. Rabelink is sponsored by a fellowship of the Royal Dutch Acad-
emy of Sciences (KNAW).
REFERENCES
1 . Attman P0, Samuelsson 0, Alaupovic P: Lipoproteinmetabolism in renal failure. Am J Kidney Dis 1993:21:573-592.
2. International Committee for the Evaluation of Hyper-triglyceridemia as a Vascular Risk Factor: The hyper-triglyceridemias: risk and management. Am J Cardiol199 1 :68LSuppl 3]: 1A-42A.
3. Chan MK, Varghese Z, Persaud JW, Baillod RA, Moor-head JF: Hyperlipidemia in patients on maintenancehemo- and peritoneal dialysis: the relative pathogeneticroles of triglyceride production and triglyceride removal.Clin Nephrol 1982:17:183-190.
4. Chan MK, Persaud J, Varghese Z, Moorhead J: Patho-genetic roles of post-heparmn lipases in lipid abnormall-ties in hemodialysis. Kidney mt 1984:25:812-818.
5. Flier JS, Underhifi LH: Lipoprotein lipase. A multifunc-tional enzyme relevant to common metabolic diseases. NEngl J Med 1989:320:1060-1068.
Lipid Profile During High-Flux Dialysis
1708 Volume 5 ‘ Number 9 ‘ 1995
6. Murase T, Cattran DC, Rubenstein B, Steiner G: Inhibi-tion of lipoprotein lipase by uremic plasma, a possiblecause of hypertriglyceridemia. Metabolism 1975:24:1279-1286.
7. Statrans I, Felts JM, Zacherle B: Apoprotein compositionof plasma lipoproteins in uremic patients in hemodialy-sis. Clin Chim Acta 1979:93:135-43.
8. Akmal M, Kasim SE, Soliman AR, Massry SG: Excessparathyroid hormone adversely affects lipid metabolismin chronic renal failure. Kidney Int 1990:37:854-858.
9. Dinarello CA: Cytokines: Agents provocateurs in hemo-dialysis. Kidney mt 1992:41:683-694.
10. Diamond SM, Henrich WL: Acetate dialysate versusbicarbonate dialysate: A continuing controversy. Am JKidney Dis 1987:9:3-11.
1 1 . Rosborough DC, Van Stone JC: Dialysate glucose. Se-mm Dial 1993:6:260-263.
12. Deuber HJ, Schulz W: Reduced lipid concentrationsduring four years of dialysis with low molecular weightheparin. Kidney Int 1991:40:496-500.
13. Dumler F, Stalla K, Mohini R, Zasuwa G, Levin NW:Clinical experience with short time hemodialysis. Am JKidney Dis 1992:19:49-56.
14. Josephson MA, Fellner 5K, Dasgupta A: Improved lipidprofiles in patients undergoing high-flux hemodialysis.Am J Kidney Dis 1992:20:361-366.
15. Seres DS, Strain GW, Hashim SA, Goldberg Li, LevinNW: Improvement of plasma lipoprotein profiles duringhigh-flux dialysis. J Am Soc Nephrol 1993:3:1409-1415.
16. Gimpel JA, Van Rijn HJM, Kortlandt W: Lipoproteins,lipids and apolipoproteins as risk factors for angio-graphically assessed coronary artery disease. Clin ChemEnzym Comms 1992:5:63-68.
17. Leerink CB, Gimpel JA, Kortlandt W, Bouma BN, vanRijn HJM: Kinetic analysis oflipoprotein (a) inhibition ofplasminogen activation by tissue plasminogen activatorin vitro. Fibrinolysis 1991:5:233-238.
18. Huttunen JK, Ehnholm C, Kekki M, Nikkila EA: Post-heparmn plasma lipoprotein lipase and hepatic lipase innormal subjects and in patients with hypertriglyceridae-mia: Correlations to sex, age and various parameters oftriglyceride metabolism. Clin Sci Mol Med 1976:50:249-260.
19. Dauglrdas JT: Chronic hemodialysis prescription: Aurea kinetic approach. In: Daugirdas JT, Ing TS, Eds.Handbook ofDialysis. 2nd Ed. Boston: Little, Brown andCompany. 1994:92-120.
20. Teraoka J, Matsui N, Nakagawa 5, Takeuchi Y: The roleofheparmn in the changes oflipid patterns during a singledialysis. Clin Nephrol 1982:17:96-99.
2 1 . Wessel-Aas T, Christophersen B: Systemic heparmniza-tion of uremic patients and its effects on blood lipids and
in vivo toxicity ofthe plasma. Clin Nephrol 1982; 18:135-140.
22. Otsubo Y, Uchida Y, Yasumoto Y, Yamashita W, ArimaT: Apo CIII is a potent factor on lipid abnormalities inhemodialysis patients [Abstract]. J Arm Soc Nephrol1993:4:375.
23. Breckenbridge WC, Little JA, Steiner G, Chow A,Poapst M: Hypertriglyceridemia associated with defi-ciency of apolipoprotein CII. N Engl J Med 1978:298:1265-1273.
24. Fontbonne A, Echwege E, Cambien F, et at.: Hypertrig-lyceridemia as a risk factor for coronary heart diseasemortality in subjects with impaired glucose tolerance ordiabetes. Results from the 1 1 -year follow-up of the ParisProspective Study. Diabetologia 1989:32:300-304.
25. Gordon T, Castelli WP, Hjortland MC, Kannel WB, Daw-ber TR: High density lipoprotein as a protective factoragainst coronary heart disease: The Framingham Study.Am J Med 1977:62:707-714.
26. Flick MH, Elo 0, Haapa K, et at.: Helsinki Heart Study.Primary prevention trial with gemfibrozil in middle-agedmen with dyslipidemia. N Engl J Med 1987:317:1237-1245.
27. Sanfelippo ML, Swenson RS, Reaven GM: Response ofplasma triglycerides to dietary change in patients onhemodialysis. Kidney Int 1978:14:180-186.
28. Gokal R, Mann JI, Ledingham DM: Dietary treatment ofhyperlipidemia in chronic hemodialysis patients. Am JClin Nutr 1978:31:1915-1918.
29. Cattran DC, Steiner G, Fenton SSA, Ampil M: Dialysishyperlipidemia: response to dietary manipulations. ClinNephrol 1980:13:177-182.
30. Goldberg AP, Applebaum-Bowden DM, Bierman EL, etat.: Increase in lipoprotein lipase during clofibrate treat-ment of hypertriglyceridemla in patients on hemodialy-sis. N Engl J Med 1979:301:1073-1076.
3 1 . Pasternack A, Vfinttinen T, Solakivi T, Kuusi T, Korte T:Normalisation oflipoprotein lipase and hepatic lipase bygemfibrozil results in correction of lipoprotein abnormal-ities in chronic renal failure. Chin Nephrol 1987:27:163-168.
32. Grutzmacher P, Scheuermann EH, Siede W, et at.: Lipidlowering treatment with bezafibrate in patients onchronic haemodialysis: pharmacokinetics and effects.Klin Wochenschr 1986:64:910-916.
33. Pierides AM, Alvarez-Ude F, Kerr DNS: Clofibrate-induced muscle damage in patients with chronic renalfailure. Lancet 1975:2:1279-1272.
34. Kijima Y, Sasaoka T, Kanayama M, Kubota 5: Untowardeffects of clofibrate in hemodialyzed patients. N Engl JMed 1977:296:515.
















![Chronic Kidney Disease and Coronary Artery Disease · and chronic kidney disease (CKD) (including end-stage kidney disease [ESKD] and trans-plant recipients) and seeks to improve](https://img.pdfslide.net/doc/110x75/5e7685650f2d2c31c072d6ef/chronic-kidney-disease-and-coronary-artery-and-chronic-kidney-disease-ckd-including.jpg)