Embed Size (px)
Citation preview
f
Annals of Tropical Medicine & Parasitology, Vol. 95, No. 5, 535-538 (2001)
High prevalence of Wuchereria bancrofti infection amongMyanmar migrants in Thailand
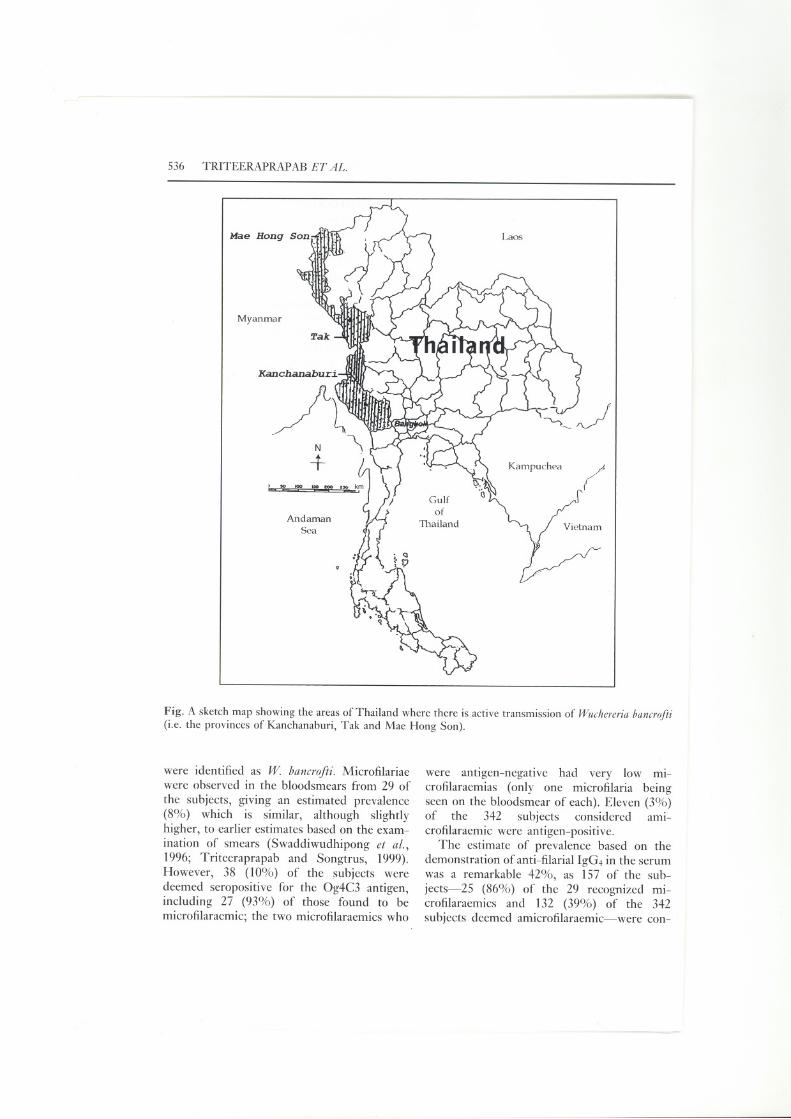
\ Wuchereria bancrofti is still a major public-health problem in the tropics and subtropics.This filarial nematode causes the vast majorityof the 100 million human cases of lymphaticfilariasis found globally (Ottesen and Ra-machandran, 1995), and about 1000 millionpeople are believed to be at risk of acquiringthe infection (WHO, 1984). In Thailand, con-trol measures have now confined the area ofactive transmission of this parasite to the threewestern provinces of Tak, Kanchanaburi, andMae Hong Son (see Fig.). The most recentestimate of the prevalence of lymphaticfilariasis in Thailand is 2.08 cases/lOO 000
(Anon., 1998). The W. bancrofti endemic toThailand is of the nocturnal subperiodic (ru-ral) strain that is transmitted mainly by theAedes niveus group of mosquitoes (Anon.,1996). Recently, however, hundreds of thou-sands of migrants from Myanmar have crossedinto Thailand to seek work, and it is estimatedthat 2%-5% of these migrants carry the noc-turnal periodic (urban) type of W. bancrofti(Anon., 1996; Swaddiwudhipong et al., 1996;Triteeraprapab and Songtrus, 1999). Since themain vector of this urban form of W. bancrofti,Culex quinquefasciatus, is prevalent in Thai-land, the migrant population from Myanmarcould form an important new reservoir ofbancroftian filariasis in Thailand. The prob-lem may be worse than currently recognizedbecause all the available estimates of theprevalence of infection in the Myanmars arebased on parasitological diagnosis using thickblood smears (Swaddiwudhipong et al., 1996;Triteeraprapab and Songtrus, 1999). The rela-tive insensitivity of this technique raises thepossibility that many migrants with low' mi-crofilaraemias are being considered unin-fected. The goal of the present study was toobtain a more accurate idea of the prevalenceof W. bancrofti infection in the Myanmar mi-grant population, by comparing estimates pro-
J
ISSN 0003-4983 (print) ISSN 1364-8594 (online)/01/050535-04Carfax Publishing
duced using three methods: (1) microscopicalexamination for micro filariae (mff) in thicksmears of night-blood (blood collected be-tween 20.00 and 00.00 hours, and each smearexamined for 3-5 mins at X 100), with anymff identified to species at X 400; (2) detec-tion of the circulating parasite antigen Og4C3,using a commercial ELISA aCU TropicalBiotechnology, Townsville, Australia); and (3)ELISA-based assessment of serum levels ofspecific anti-filarial IgG4, using extracts fromadult Brugia malayi as antigen (Chanteau etal., 1991). Both of the serological assays usedare known to give more sensitive measures ofinfection than the traditional examination ofbloodsmears, although those who have beenexposed in the past but do not have currentinfection may be seropositive for anti-filarialIgG4 (Lal and Ottesen, 1988; Kwan-Lim etal., 1990; More and Copeman, 1990; Wamaeet al., 1992; Kurniawan et al., 1993; Turner etal., 1993; WHO, 1993; Lammie et al., 1994;Atmadja et al., 1995).
The subjects were 371 Myanmar migrants(aged 2-56 years) who were living in the MaeSot district of Tak province. They were se-lected at random (from the residents aged ~ 2years) during a cross-sectional survey in acommunity at Moo Nerng, in the Maekasasub-district, in January-March 1999. Thestudy was approved by the ethical committeeof the Faculty of Medicine at ChulalongkornUniversity. Verbal informed consent was ob-tained from the adult subjects and (in thepresence of two witnesses) from a parent orguardian of each of the children investigated.All the subjects who appeared to be infectedwith filarial parasites were treated with a stan-dard dose of diethylcarbamazine (DEC), asrecommended by Thailand's Filariasis Div-ISIOn.
The results of the three tests are summa-rized in the Table. All of the mff observed
@ 2001 Liverpool School of Tropical Medicine001: 1080/00034980120072248
536 TRITEERAPRAP AB ET AL.
Laos
Myanmar
N
+ Kampuchea ~(
AndamanSea
Fig. A sketch map showing the areas of Thailand where there is active transmission of Wuchereria bancrofii(i.e. the provinces of Kanchanaburi, Tak and Mae Hong Son).
were identified as W. bancrofti. Microfilariaewere observed in the blood smears from 29 of
the subjects, giving an estimated prevalence(8%) which is similar, although slightlyhigher, to earlier estimates based on the exam-ination of smears (Swaddiwudhipong et al.,1996; Triteeraprapab and Songtrus, 1999).However, 38 (10%) of the subjects weredeemed seropositive for the Og4C3 antigen,including 27 (93%) of those found to bemicrofilaraemic; the two microfilaraemics who
were antigen-negative had very low mi-crofilaraemias (only one microfilaria beingseen on the blood smear of each). Eleven (3%)of the 342 subjects considered ami-crofilaraemic were antigen-positive.
The estimate of prevalence based on thedemonstration of anti-filarial IgG4 in the serumwas a remarkable 42%, as 157 of the sub-jects-25 (86%) of the 29 recognized mi-crofilaraemics and 132 (39%) of the 342subjects deemed amicrofilaraemic-were con-
---
BANCROFTIAN FILARIASIS IN MY ANMAR MIGRANTS 537
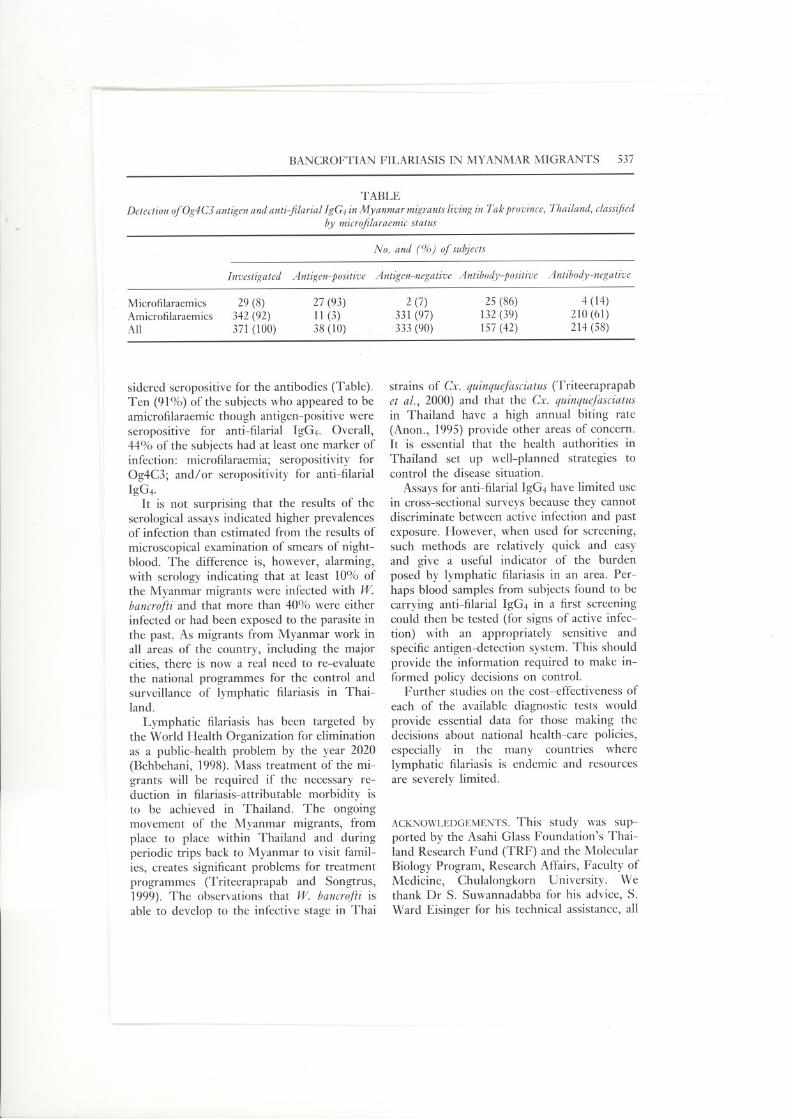
TABLE
Detection ofOg4C3 antigen and anti-filarial IgG4 in Myanmar migrants living in Tak province, Thailand, classifiedby microfilaraemic status
sidered seropositive for the antibodies (Table).Ten (91%) of the subjects who appeared to beamicrofilaraemic though antigen-positive wereseropositive for anti-filarial IgG4. Overall,44% of the subjects had at least one marker ofinfection: microfilaraemia; seropositivity forOg4C3; and/or seropositivity for anti-filarialIgG4.
It is not surprising that the results of theserological assays indicated higher prevalencesof infection than estimated from the results ofmicroscopical examination of smears of night-blood. The difference is, however, alarming,with serology indicating that at least 10% ofthe Myanmar migrants were infected with Wbancrofti and that more than 40% were eitherinfected or had been exposed to the parasite inthe past. As migrants from Myanmar work inall areas of the country, including the majorcities, there is now a real need to re-evaluatethe national programmes for the control andsurveillance of lymphatic filariasis in Thai-land.
Lymphatic filariasis has been targeted bythe World Health Organization for eliminationas a public-health problem by the year 2020(Behbehani, 1998). Mass treatment of the mi-grants will be required if the necessary re-duction in filariasis-attributable morbidity isto be achieved in Thailand. The ongoingmovement of the Myanmar migrants, fromplace to place within Thailand and duringperiodic trips back to Myanmar to visit famil-ies, creates significant problems for treatmentprogrammes (Triteeraprapab and Songtrus,1999). The observations that W bancrofti isable to develop to the infective stage in Thai
strains of Cx. quinquefasciatus (Triteeraprapabet al., 2000) and that the Cx. quinquefasciatusin Thailand have a high annual biting rate(Anon., 1995) provide other areas of concern.It is essential that the health authorities in
Thailand set up well-planned strategies tocontrol the disease situation.
Assays for anti-filarial IgG4 have limited usein cross-sectional surveys because they cannotdiscriminate between active infection and pastexposure. However, when used for screening,such methods are relatively quick and easyand give a useful indicator of the burdenposed by lymphatic filariasis in an area. Per-haps blood samples from subjects found to becarrying anti-filarial IgG4 in a first screeningcould then be tested (for signs of active infec-tion) with an appropriately sensitive andspecific antigen-detection system. This shouldprovide the information required to make in-formed policy decisions on control.
Further studies on the cost-effectiveness ofeach of the available diagnostic tests wouldprovide essential data for those making thedecisions about national health-care policies,especially in the many countries wherelymphatic filariasis is endemic and resourcesare severely limited.
ACKNOWLEDGEMENTS.This study was sup-ported by the Asahi Glass Foundation's Thai-land Research Fund (TRF) and the MolecularBiology Program, Research Affairs, Faculty ofMedicine, Chulalongkorn University. Wethank Or S. Suwannadabba for his advice, S.Ward Eisinger for his technical assistance, all
No. and (%) of subjects
Investigated Antigen-positive Antigen-negative Antibody-positive Antibody-negative
Microfilaraemics 29 (8) 27 (93) 2 (7) 25 (86) 4 (14)Amicrofilaraemics 342 (92) 11 (3) 331 (97) 132 (39) 210 (61)All 371 (100) 38 (10) 333 (90) 157 (42) 214 (58)

538 TRITEERAPRAPAB ET AL.
the staff of the Departmept of Parasitology atChulalongkorn University, and the health per-sonnel from the Filariasis Division, Com-municable Disease Control Department,Ministry of Public Health, for their skilledassistance in the laboratory and the field.
S. TRITEERAPRAPAB*
I. NuCHPRAYOON
C. PORKSAKORN
Y. POOVORAWAN
A. L. SCOTT
Department of MolecularMicrobiology and Immunology,
The Johns Hopkins UniversitySchool of Public Health,
Baltimore, MD 21205, USA
Received 22 February 2001,Revised and accepted 29 May 2001
Department of Parasitology,Faculty of Medicine,Chulalongkorn University,Bangkok 10330, Thailand
.. E-mail: [email protected]; fax: + 6622524963.
REFERENCES
ANON. (1995). Filariasis Division Annual Report. Bangkok: Communicable Disease Control Department,Ministry of Public Health (in Thai).
ANON. (1996). Filariasis Division Annual Report. Bangkok: Communicable Disease Control Department,Ministry of Public Health (in Thai). .
ANON. (1998). Filariasis Division Annual Report. Bangkok: Communicable Disease Control Department,Ministry of Public Health (in Thai).
ATMAD]A,A. K., ATKINSON,R., SARTONO,E., PARTONO,F., ¥ AZDANBAKHSH,M. & MAIZELS,R. M. (1995).Journal of Infectious Diseases, 172, 1567-1572.
BEHBEHANI,K. (1998). Bulletin of the World Health Organization, 76 (Suppl.), 64--67.CHANTEAU,S., PUCHART,R., SPIEGEL,A., MARTIN,P. M. V. & CARTEL,J.-L. (1991). Tropical Medicine and
Parasitology, 42, 339-342.KURNIAWAN,A., ¥AZDANBAKHSH,M., VANREE, R., MLBERSE, R., SELKIRK,M. E., PARTONO,F. &
MAIZELS,R. M. (1993). Journal of Immunology, 150, 3941-3950.KWAN-LIM, G. E., FORSYTH,K. P. & MAIZELS,R. M. (1990). Journal of Immunology, 145, 4298--4305.LAL, R. B. & OTTESEN,E. A. (1988). Journal of Infectious Diseases, 158, 1034-1037.LAMMIE,P.]., HIGHTOWER,A. W. & EBERHARD,M. L. (1994). American Journal of Tropical Medicine and
Hygiene, 51, 348-355.MORE, S. J. & COPEMAN,D. B. (1990). Tropical Medicine and Parasitology, 41, 403--406.OTTESEN,E. A. & RAMACHANDRAN,C. P. (1995). Parasitology Today, 11, 129-131.SWADDIWUDHIPONG,W., TATIP, Y., MEETHONG,M., PREECHA,P. & KOBASA,T. (1996). Southeast Asian'
Journal of TropicalMedicineand PublicHealth, 27, 847-849.TRiTEERAPRAPAB, S. & SONGTRUS, J. (1999). Journal of the Medical Association of Thailand, 82, 735-739.TRITEERAPRAPAB, S., KAN]ANOPAS, K., SUWANNADABBA.S., SANGPRAKARN, S., POOVORAWAN, ¥. & SCOTT,
A. L. (2000). Epidemiology and Infection, 125, 207-212.TURNER, P., COPEMAN, B., GERISI, D. & SPEARE, R. (1993). Tropical Medicine and Parasitology, 44, 45--48.
W AMAE, C. N., ROBERTS, J. M., EBERHARD, M. L. & W AMAE, C. N., ROBERTS, J. M., EBERHARD, M. L. &
LAMMIE, P. J. (1992). Journal of Infectious Diseases, 165, 1158-1160.
WORLD HEALTH ORGANIZATION (1984). Lymphatic Filariasis. Fourth Report of the WHO Expert Committee
on Filariasis. Technical Report Series No. 702. Geneva: WHO.WORLD HEALTH ORGANIZATION (1993). Bulletin of the World Health Organization, 71,135-141.
..
,J
,J





























