-
8/3/2019 High Velocity Missle Injury
1/6
High VelocityAn Experimental
Missi!e InjuryStudy of the Retentive Forces of Tissue
Joseph J. Amato, MD, Boston, MassachusettsLawrence J. Billy, MD,
St . Louis, MissouriNoel $. Lawson, MD, Detroit, MichiganNorman M.
Rich, MD, Washington, DC
As early as 1848 Hugiuer noted that high velocitybullets used in
the Paris street fights producedwounds of an explosive nature [I].
He theorizedthat the severity of the wound was proportional tothe
water content of the tissues. However, woundswithin similar tissues
varied from extremely minorto severe. Woodruff [2] in 1898
questioned the in-consistent character of high velocity bullets in
pro-ducing tissue destruction and first described theformation of
the temporary cavity in high velocitymissile wounds. Wilson [3] in
1921 also noted thebizarre behavior of the high velocity bullet and
theexplosive effect within certain tissues.
Cavitation is a feature of all missile wounds.This phenomenon is
the momentary lateral expan-sion of the tissue within the missile
tract caused bya deposition of kinetic energy. It is now knownthat
the severity of the wound depends not only onthe behavior of the
missile within tissues, but alsoon the histologic character of the
tissues beingstruck.
Previous observations of high velocity injurieshave been made
from war casualties and from lab-oratory studies of the composite
wound [4-61. Thedeductions made from those observations haveFrom
the Biomedical Department. Bioohvsics Laboratorv. U.S.
EdaewoodArsenal, Maryland, and ihe Departmint-of Cardiothorac/c
Surgery. NewEngland Medical Center and Tufts University School of
Medicine, Boston,Massachusetts.Reprint requests should be addressed
to Dr Amato, Department ofCardiothoracic Surgery, Tufts-New England
Medical Center, 171 HarrisonAvenue, Boston, Massachusetts
02111.Presented at the Fifty-Fourth Annual Meeting of the New
England Sur-gical Society, Portsmouth, New Hampshire. September
27-29, 1973.
been taken to be characteristic of individual organinjury, and
for the most part, the description ofthe mechanism of injury has
been correct. The ini-tial experiments conducted at Edgewood
Arsenal,using high speed photography and roentgenogra-phy, have
dealt with the study of isolated vascularinjuries [ 7-91, whereas
further experiments havebeen conducted to evaluate the pattern of
injury inisolated organs such as muscles, liver, and bone.The
purpose of this paper is to demonstrate theevents that occur within
each tissue after high ve-locity bullet wounding, and to discuss
briefly theinteraction between the disruptive forces of themissile
and the retentive forces of the tissue.
Material and Methods
Individual experiments were conducted for each ofthe tissue
studies. Although each of the preparationsused was different as
will be described, th e equipmen tand ma terials were similar.
Muscle. The hind limbs of twenty anesthetized dogswere utilized
to study the sequence of events in musclewounding. Skin flaps were
created to expose the musclemass. Injury to the femur was avoided
to prevent bonefragmentation.Lioer. The liver from freshly
slaughtered goats was re-moved and suspended by the ligaments prior
to wound-ing. Numerous attempts to study injury to the liver invivo
were performed; however, detailed docum enta tionof this met hod
was impossible. Angiogram s of th e isolat -ed livers were obtained
by injecting Hypaque@ into theappropriate blood vessels.
454 The American Journal of Surgery
-
8/3/2019 High Velocity Missle Injury
2/6
I,cing. I,uni:s were removed from ten goats and imme-diately
inflated wit.h air to return them to their normalanatomic
configuration. The pulmonary arteries wereinjected with Hypaque
just prior to wounding.
Hone. Femurs were obtained from freshly slaughteredcalves. To
create an environment that would clearlyvisualize bone destruction,
the femurs were individuallyembedded in a clear gelatin which was
allowed to solidi-fy. thereby simulating the properties of
muscle.
To insure identical wounds in the foregoing experi-ments, an
0.2.5 inch sphere weighing 16 gr was used. In-juries were inflicted
on these tissues at a striking veloci-ty of approximately 3,000
feet per second. Comparativeinjuries with lower velocities of 1,000
feet per secondwere also made. The events in the sequence of
injurywere documented by high speed motion picture photog-raphy
using a Red Lake Hycam camera at 3,750 to 4,500frames per second.
The Flexitron X-Ray System capa-ble of delivering up to 1,000 amps
at 30 kv of anode po-tential producing pulses of less than one 0.1
Fsec in du-ration was used for both roentgenographic and
angio-graphic smdies.
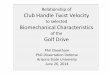
Figure 1. Roentgenogram of the temporary cavity formedin muscle
by a low velocity missile at 1.000 feet per sec-ond.
parenchyma (specific gravity 0.4 to 0.5) by show-Results ing
disruption of the blood vessels tilled wit,h Hv-paque. (Figure
8.)
The sequence of injury to the isolated organswas demonstrated in
each of the experiments. Themuscle (specific gravity 1.02 to 1.04)
preparationsbest demonstrate each of the phases of low andhigh
velocity injury. The low velocity woundcreates a-direct pathway of
destruction with verylittle motion within the surrounding tissues.
(Fig-ure 1.) A small temporary cavity can be seen whenthe missile
strikes muscle tissue at 1,000 feet persecond. However, when muscle
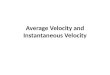
is struck at 3,000feet per second, the initial movement of
impactdemonstrates the phenomenon of tail splash,which is the
backward hurling of destroyed tissue.(Figure 2.) Within
microseconds, a large space isformed within the wound tract; this
is referred toas the temporary cavity. The maximal diameter ofthe
temporary cavity is approximately thirty timesthe size of the
original missile. (Figures 3 and 4.)The tissue undulates for 5 to
10 msec and comes torest as the permanent tract.
Liver (specific gravity 1.01 to 1.02) is similar tothe density
of muscle. However, both the tempo-rary cavity formed by a high
velocity missile strik-ing at 3,000 feet per second (Figures 5 and
6) andthe resulting permanent tract (Figure 7) are largerthan those
of muscle.
Although previously never visualized andthought possibly to be
nonexistent [IO], a tempo-rary cavity is formed within the lung
tissue by a
Both high speed photography and roentgenogra-phy demonstrated
large temporary cavities in thefemurs that had been injured by the
high velocitysphere. Bone has a high density with a specificgravity
of 1.11 or greater depending on the degreeof ossification within
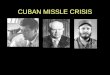
the bone. As the missile pen-etrates the bone, fragmentation occurs
(Figure 9)with the fragment.s going toward the edges ~)f helarge
cavity. As undulation occurs, these fragmentsreturn to the center
of the cavity and the majorityremain there. After a lag phase, a
number of thesebone spicules are seen to move forward in the
di-rection of the missile.
missile striking at 3,000 feet per second. Angio- Figure 2. The
phenomenon of tail splashing is demon-grams demonstrate a small
cavity within the lung strated in tissue a few milliseconds after
impact.
Volume 127, Apri l 1974 45 5
-
8/3/2019 High Velocity Missle Injury
3/6
Amato et al
Figure 3. Roentgenogram demonstrating the maximalsize of the
temporary cavity in muscle tissue caused bya high velocity
missile.Comments
Ballistics, the study of the motion of a projec-tile, is divided
into three phases: interior, exterior,and terminal. Interior
ballistics deals with the mo-tion of the bullet within the gun
barrel. Exteriorballistics, the second phase, studies the flight
ofthe bullet to the target. The final phase, terminalballistics, is
the study of the bullet within the tar-get. The study of the motion
of a bullet within thetissues is termed wound ballistics. As
tissues arestruck by a missile, multiple disruptive forcescombine
to produce tissue destruction. The majorforces consist of the
velocity, the mass, and thechange in shape or presented area of the
bulletwhen it reaches the tissue. The most importantforce is the
velocity of the missile within thetissues. The initial velocity on
impact is called
Figure 4. High speed photograph of the temporary cavitywithin
muscle tissue caused by a high velocity bullet.
striking velocity. If the bullet leaves the tissue, theremaining
velocity is called the residual velocity.The effective velocity of
the injury is the differ-ence between the two velocities (VI - V,).
The ki-netic energy (KE) imparted to the tissues ex-pressed in foot
pounds can be written:
KE = M(V12 - V22)/2 gwhere M equals mass and g equals gravity.
If smallamounts of energy are released within the tissue,as in the
low velocity wound, destruction will beconfined to the pathway of
the bullet. The energyreleased by high velocity missiles forms
initialshock waves with pressure of up to 100 to 200 at-mospheres,
imparting momentum to the tissuesboth forward and laterally. These
tissues acceler-ate in an outward direction creating a large
spaceknown as the temporary cavity, its duration beingonly 10 to 30
msec. The tissues undulate and un-dergo stretching and compression.
Because of theheterogeneity and varied density of the tissues,there
is added mechanical damage due to theshearing effect between these
tissues.
The second disruptive force is the mass of thebullet. Increase
in mass will cause proportional in-crease in tissue destruction. A
third disruptiveforce is the shape of the bullet or the change
inpresented area on striking the tissues. The bulletmay present
itself in a direct nose-on position onstriking with a large amount
of yaw, or tumbling.If the degree of yaw is minimal at impact, the
bul-let will travel quickly through the tissue and exitwith a
greater residual velocity. If there is a largeangle of yaw, or if
the bullet tumbles, the area ofthe bullet presenting to the tissues
is larger andthe pathway of the bullet is longer and wider,causing
marked retardation of the bullet withinthe tissues. Deformation of
the bullet or fragmen-tation will likewise increase the presented
area andcause tumbling within the tissues. Consequently,more energy
is deposited, creating greater damagePI.The retentive forces that
combat the disruptiveforces vary with the individual tissues. The
char-acteristic pattern of injury is determined by thedensity of
tissues combined with the degree ofelasticity and cohesion within
these tissues. Mus-cle and liver are tissues with similar
densities.Muscle tissue is composed of cells with a contrac-tile
force embedded within a structured connectivetissue framework, that
is, endomysium, perimys-ium, and epimysium. The liver is surrounded
by afibroelastic membrane. The existing connectivetissue is limited
to the arteries, veins, lymphatics,
456 The American Journal of Surgery
-
8/3/2019 High Velocity Missle Injury
4/6
Figure 6. The maximal temporary cavity within liver tis-sue
caused by a high velocity bullet (high speed motionpicture
photography).
Figure 5. Venogram of the liver showing the maximal for-mation
of the temporary cavity in high velocity missile in-jury.
Figure 7. Permanent missile tract within liver tissuecaused by a
missile fired at 3,000 feet per second.
Figure 8. Pulmonary angiogram demonstrating the tem-porary
cavity formed in lung parench,yma by a high ve-locity bullet.
and bile ducts. The further supporting structures nal position.
Krauss [9] in 1957 has shown thatof the reticuloendothelial system
are composed of there is only a small area of actual cellular
destruc-fine reticular fibers that add little supporting tion
surrounding the temporary cavity immediate-strength to the liver.
It was found that the energy ly after injury. Although the muscle
tissue hasabsorbed per centimeter of both liver and muscle been
displaced approximately 3 cm radially, only atissue t,raversed is
essentially identical [9]. How- 5 mm rim of destroyed tissue is
seen. Although aever, the formation of the temporary cavity within
zone of extravasation and capillary disruption ap-the liver and the
resultant permanent tract are pears, it is difficult to determine
whether most ofboth larger. Both muscle and liver, when first the
suhsequent changes might, not be caused bystruck by a high velocity
missile, exhibit a phe- impaired blood supply [9]. It is apparent
that. thenomenon called tail splashing. This phenomenon cohesive
structure of the liver is less than that ofis similar to a body of
water being struck with a muscle. Consequently, when struck with a
high ve-rock. On injury, the firmly harnessed cellular com- locity
missile, the entire pathway of the temporaryponents of muscle
expand laterally forming a large cavity loosens cells from their
cellular supportingtemporary cavity, and except for the central
por- structures during undulation of the cavity. Thetion of the
wound tract, they return to their origi- permanent missile tract
approximates the tempo-
Volume 127, Apri l 1974 45 7
-
8/3/2019 High Velocity Missle Injury
5/6
Amato et al
Figure 9. The high velocity bullet fragments the bonewithin the
temporary cavity.rary cavity in size because of the volume of
tissuelost during injury.
As discussed and demonstrated in detail in aseparate report
[IO], the passage of a high velocitymissile through lung does
create a temporary cavi-ty that is smaller and less impressive than
that ofmuscle or liver tissue. The elastic fibers within
thespongework of lung parenchyma absorb the energyand recoil so
that the missile tract is hardly per-ceptible.
Although the question has been raised as towhether bone, because
of its brittle character,reacts to these injuries by producing a
true tempo-rary cavity, the cavitys formation was clearly visi-ble.
Bone is dense tissue composed of calcium saltsembedded within an
organic intercellular sub-stance of collagen. The critical velocity
for fractur-
Figure 10. The exit wound formed by a high velocity mis-sile
that has struck bone. Fragments of bone are seenexiting the wound
as secondary missiles.
ing bone is approximately 200 feet per second. Thefemurs struck
with high velocity missiles demon-strate a severe amount of
destruction but are heldwithin the surrounding framework of
periosteumand muscle connective tissue. Most interesting isthe
phenomenon of bone fragments visualizedmoving forward in the
direction of the bullet.These bone spicules act as secondary
missiles,creating further destruction within the tissues.With the
deformation or fragmentation of missileor bone, the skin at the
exit site becomes shatteredand torn by these multiple fragments.
(Figure 10.)Summary
Wound ballistics is defined as the study of themotion of
missiles within the tissues. To under-stand tissue destruction we
must realize that theseverity of injury depends on an intricate
balanceof the action of the missile and the reaction of thetissues.
The mass, shape, and velocity of the bulletand the change in
presented area are the majorfactors that render destruction to the
tissues. l
Our studies of the mechanism of injury to vari-ous tissues such
as the muscle, liver, lungs, andbone have demonstrated graphically
the formationof a temporary cavity within these tissues and
thesequence of events that occur within these isolatedtissues. The
size of the temporary cavity is propor-tionate to the specific
gravity of the tissues and tothe severity of the injury. However,
the elasticityand cohesiveness of the tissue counteract the
ex-pansion of the wound tract and absorb the deposi-tion of kinetic
energy by the missile. The tissueswith a more cohesive structure
and with largeamounts of elastic tissue consequently demon-strate a
greater resistance to injury.References1.2.3.4.5.6.
7.
8.9.
10.
Horsely V: The destructive effects of small projectile.
Nature50: 106, 1894.Woodruff CE: The causes of the explosive effect
of modernsmall caliber bullets. NY MedJ67: 593, 1898.Wilson LB:
Dispersion of bullet energy in relation to wound
effects. Milit Surg 159: 249, 1921.Harvey EN, Butler EC,
McMillen JH: Mechanism of wounding.War Med8: 102, 1945.Rich NM:
Vietnam missile wounds evaluated in 750 patients.Milt Med 133: 9,
1968.DeMuth WE: Bullet velocity and design as determinants
ofwounding capacity: an experimental study. J Trauma 6:222,
1966.Amato JJ, Billy LJ, Gruber RP, Lawson NS, Rich NM: Vascu-lar
injuries: an experimental study of high and low velocitymissile
wounds. Arch Surg 101: 167, 1970.Herget CH: Wound ballistics.
Surgery of Trauma (BowersWB, ed). Philadelphia, Lippincott,
1956.Krauss M: Studies in wound ballistics: temporary cavity
ef-fects in soft tissues. Milit Med 121: 221, 1957.Amato JJ:
Temporary cavitation in high velocity pulmonarymissile injury. In
manuscript.
458 The Amerlcan Journalof Surgery
-
8/3/2019 High Velocity Missle Injury
6/6
High Velocity Missile Injury
Discussion
Thomas Perry, dr (Providence. RI): Could you relateto us rhe
approximate velocity of the various gun mis-siles that we
ordinarily see in practice?
F. A. Simeone (Providence, RI): I want to congratu-late l)r
Amato on his excellent presentation of an impor-tant subject in a
field that we do not like to talk aboutbut that will be with us for
some time to come.
Doctor Amato has illustrated the dramatic changesthat a missile
produces in matter as it expends its kinet-ic energy. A very
important practical question is raisedby the demonstration, namely,
how much viable tissuehas been rendered nonviable by the missile?
For exam-ple, the advantage of delayed primary closure of a
con-tused wound is based on the fact that at the time of clo-sure,
some five days after wounding, nonviable tissuehas declared itself
and is easily distinguished from livingtissue. This distinction is
difficult to make with certain-ty at the time of injury.
I want to ask Dr Amato if he has made observationsthat would
indicat.e the extensiveness of the necrosis oftissues surrounding
the temporary cavitation. In otherwords, is there a relation
between the severity of the vio-lence and the depth at which living
tissue has beenkilled by the formation of the temporary cavities?
Thiskind of information would be of obvious practical
im-portance.
J. Amato (closing): Thank you Dr Perry. To answerDr Simeone,
yes, there is a relation between the severityof the violence and
the depth at which the cells within
the tissues have actually heen killed by the formation otthe
temporary cavity. Although I cannot recall all of thedata at this
time, our laboratory investigators as well asother investigators
had shown that in muscle tissue, forexample, the actual area of
destruction of cells aroundthe temporary cavity measured
approximately 5 mm indepth at the time of injury. The remaining
destructionwhich became demarcated within hours and days is
ac-tually, I believe, a result of loss of vascularity t.o
thetissues that had been stretched within the temporarycavity.
In answer to Dr Perrys question, in the science of bal-listics
there are several measurements of velocity.Muzzle velocity is the
velocity at which the bullet leavesthe gun. Striking velocity is
that velocity at which thebullet strikes the target, and residual
velocity is that ve-locity at which the bullet leaves the target.
The most im-portant measurement is the effective velocity which
isthe striking velocity minus the residual velocity. In
mostinstances, when speaking of the velocity, one is referringto
the muzzle velocity. The ordinary .22 short has a ve-locity of 900
feet per second. The .25 caliber travels at,800 feet per second.
The .38 caliber has a velocity of ap-proximately 925 feet per
second, whereas the .45 caliberhas a velocity of 850 feet per
second. As these missilestravel though air, both gravity and air
drag slow them toa lower striking velocity. It is also interesting
to knowthat it takes a velocity of approximately 175 feet persecond
to penetrate the skin. When you consider thatthe velocity of an
M-16 is 3,259 feet per second, the dif-ference in tissue
destruction caused by these missiles iseasily understood.
Volume 127, Apri l 1974 459