Embed Size (px)
Citation preview

Histiocytic SyndromesHistiocytic Syndromes
• Dendritic cell-related disordersDendritic cell-related disorders– Langerhans cells histiocytosisLangerhans cells histiocytosis
– juvenile xanthogranulomajuvenile xanthogranuloma
• Macrophage-related disordersMacrophage-related disorders– primary hemophagocytic syndromes (familial, sporadic)primary hemophagocytic syndromes (familial, sporadic)
– secondary hemophagocytic syndromes (viral, other)secondary hemophagocytic syndromes (viral, other)
• Malignant disordersMalignant disorders– monocytic leukemiasmonocytic leukemias
– malignant histiocytosismalignant histiocytosis

Langerhans Cell Histiocytosis Langerhans Cell Histiocytosis EpidemiologyEpidemiology
• Incidence:Incidence:– 5 cases/million population/yr (childhood LCH)5 cases/million population/yr (childhood LCH)– incidence of adult LCH is unknownincidence of adult LCH is unknown
• more common in males than females (1.3 : 1)more common in males than females (1.3 : 1)
• average age at onset: 1.8 yearsaverage age at onset: 1.8 years

Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Historical SyndromesHistorical Syndromes
• eosinophilic granulomaeosinophilic granuloma: isolated lytic : isolated lytic lesion of bone or soft tissue masslesion of bone or soft tissue mass
• Hand-Schuller-Christian diseaseHand-Schuller-Christian disease: skull : skull lesions, exophthalmos, and DI (1893)lesions, exophthalmos, and DI (1893)
• Letterer-Siwe diseaseLetterer-Siwe disease: seborrheic rash, : seborrheic rash, hepatosplenomegaly, lung involvement in hepatosplenomegaly, lung involvement in infants (1924)infants (1924)
• the spectrum of “Histiocytosis X” (1953)the spectrum of “Histiocytosis X” (1953)

Langerhans cellsLangerhans cells• described by Paul Langerhans (medical student) in described by Paul Langerhans (medical student) in
18681868• Langerhans cells (LC) reside in the epidermis (1-2% Langerhans cells (LC) reside in the epidermis (1-2%
epidermal cells) & lungepidermal cells) & lung• LCs process antigens for presentation to T cells after LCs process antigens for presentation to T cells after
migrating to lymph nodesmigrating to lymph nodes• LCs contain Birbeck granules, and express CD1a and LCs contain Birbeck granules, and express CD1a and
S-100S-100• LCs associated with “Histiocytosis X” in 1973 LCs associated with “Histiocytosis X” in 1973
(Nezelof et al)(Nezelof et al)



Generation of Generation of Langerhans cellsLangerhans cells
• LCs can be generated from stem cells:LCs can be generated from stem cells:
• obtain CD34+ stem cellsobtain CD34+ stem cells
• incubate w/ GM-CSF and TNF-alpha for incubate w/ GM-CSF and TNF-alpha for 3 weeks3 weeks
• resulting cells have Birbeck granules and resulting cells have Birbeck granules and express CD1aexpress CD1a
• have functional characteristics of LC’shave functional characteristics of LC’s


Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: PathologyPathology
• a clonal proliferation of Langerhans cellsa clonal proliferation of Langerhans cells
• LCs do not show dysplasia or atypia LCs do not show dysplasia or atypia (features of malignant cells)(features of malignant cells)
• LCH lesions contain LCs, macrophages, LCH lesions contain LCs, macrophages, T cells, eosinophils, and granulocytesT cells, eosinophils, and granulocytes
• LCs associated with “Histiocytosis X” in LCs associated with “Histiocytosis X” in 1973 (Nezelof et al)1973 (Nezelof et al)
Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Clinical manifestations IClinical manifestations I
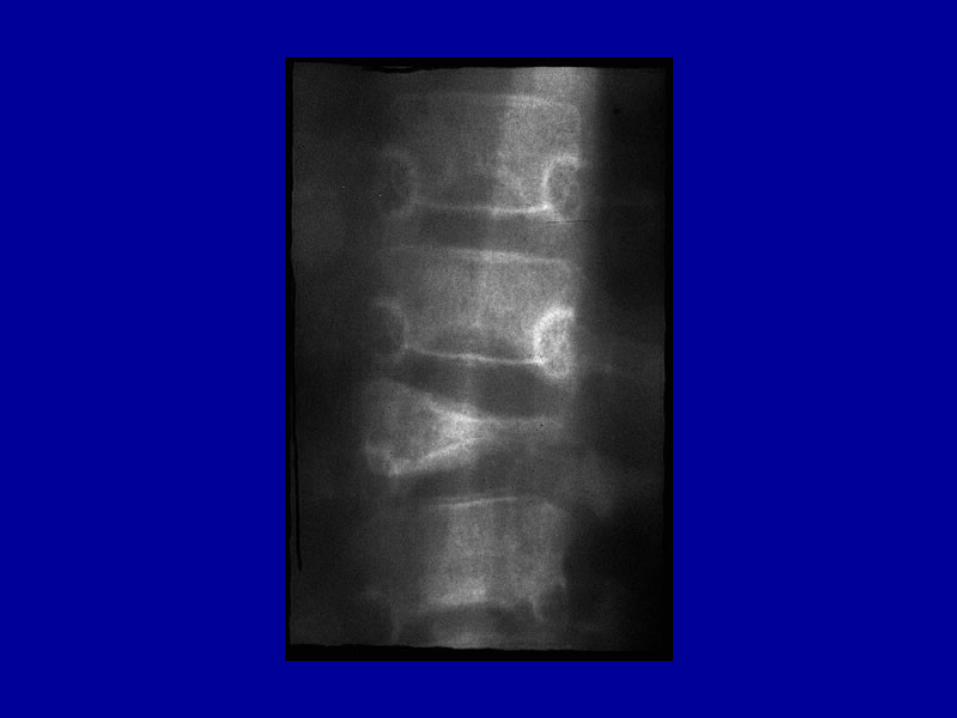
• painful swelling of bonespainful swelling of bones– unifocal bony lesion (31% at presentation)unifocal bony lesion (31% at presentation)– isolated multifocal bone involvement (19%)isolated multifocal bone involvement (19%)
• persistent otitis / mastoiditispersistent otitis / mastoiditis
• mandible involvement (“floating teeth”) mandible involvement (“floating teeth”)
• papular rash (37% at presentation)papular rash (37% at presentation)
• hepatosplenomegaly hepatosplenomegaly
• lymphadenopathylymphadenopathy





Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Clinical manifestations IIClinical manifestations II
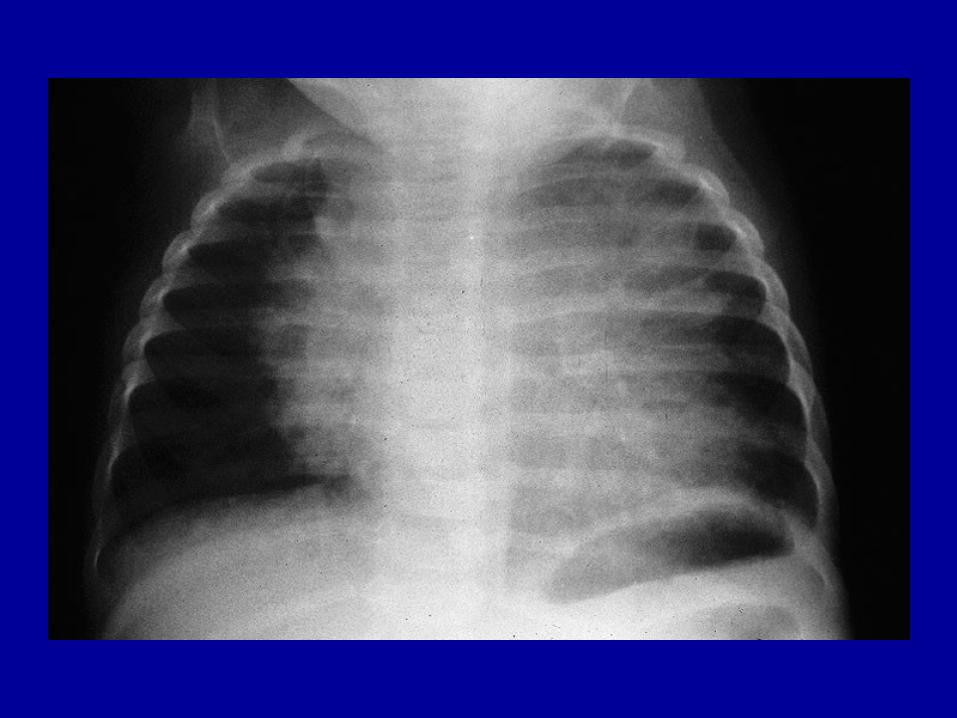
• pulmonary involvement (interstitial pattern pulmonary involvement (interstitial pattern -> “honeycombing”)-> “honeycombing”)
• marrow involvement (cytopenias)marrow involvement (cytopenias)• GI involvement (diarrhea, malabsorption)GI involvement (diarrhea, malabsorption)• endocrine involvement:endocrine involvement:
– diabetes insipidusdiabetes insipidus– growth failuregrowth failure– hypothyroidismhypothyroidism
Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Extent of disease at diagnosisExtent of disease at diagnosis
• single system / single sitesingle system / single site 33%33%
• single system / multiple sites15%
• multisystem involvement 52%

Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Diagnostic criteria Diagnostic criteria
(Histiocyte Society, 1987)(Histiocyte Society, 1987)• Presumptive diagnosisPresumptive diagnosis
– light morphologylight morphology
• Designated diagnosisDesignated diagnosis– light morphology, pluslight morphology, plus
– two or more positive stains for ATPase, S-100, a-D-two or more positive stains for ATPase, S-100, a-D-mannosidase, peanut lectinmannosidase, peanut lectin
• Definitive diagnosisDefinitive diagnosis– light morphology, plus light morphology, plus
– Birbeck granules and/or CD1a stainingBirbeck granules and/or CD1a staining

Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Natural historyNatural history
• isolated skin involvement (“Hashimoto-isolated skin involvement (“Hashimoto-Pritzker disease”): spontaneous resolutionPritzker disease”): spontaneous resolution
• eosinophilic granuloma: may resolve or eosinophilic granuloma: may resolve or progress; responds to biopsy, curettageprogress; responds to biopsy, curettage
• Hand-Schuller-Christian disease: usually Hand-Schuller-Christian disease: usually fatal if untreated due to DIfatal if untreated due to DI
• Letterer-Siwe disease: usually fatal if Letterer-Siwe disease: usually fatal if untreateduntreated

Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Therapeutic modalitiesTherapeutic modalities
• biopsy or curettagebiopsy or curettage
• radiation therapy (low dose)radiation therapy (low dose)
• topical steroidstopical steroids
• intralesional steroid injectionsintralesional steroid injections
• oral or intravenous steroidsoral or intravenous steroids
• oral or intravenous chemotherapyoral or intravenous chemotherapy– single agents (vinblastine, etoposide)single agents (vinblastine, etoposide)– combination chemotherapycombination chemotherapy

LCH-I: DesignLCH-I: Design
• first international clinical trial for LCHfirst international clinical trial for LCH
• compared vinblastine vs etoposide when compared vinblastine vs etoposide when given with steroidsgiven with steroids
• enrolled 447 pts from 1991-1995enrolled 447 pts from 1991-1995
• 143 randomized pts with multisystem 143 randomized pts with multisystem diseasedisease

LCH- ILCH- I

DAL HX-83 and HX-90 DAL HX-83 and HX-90 studies: Designstudies: Design
• two multi-center, non-randomized trials in two multi-center, non-randomized trials in Austria, Germany, Netherlands and Austria, Germany, Netherlands and Switzerland Switzerland
• risk-adapted assignment to treatmentrisk-adapted assignment to treatment
• intensive induction and continuation intensive induction and continuation therapy (much like leukemia therapy)therapy (much like leukemia therapy)
• total duration of therapy was 12 monthstotal duration of therapy was 12 months

LCH-IILCH-II
• compared vinblastine/prednisone +/- compared vinblastine/prednisone +/- etoposide as induction therapy etoposide as induction therapy
• continuation therapy: 6-MP, with pulses continuation therapy: 6-MP, with pulses of induction therapy agentsof induction therapy agents
• total duration of therapy was 24 weekstotal duration of therapy was 24 weeks
• enrolled 697 pts from 1996-2000 enrolled 697 pts from 1996-2000
• stratified patients on basis of riskstratified patients on basis of risk

LCH-II: Risk stratificationLCH-II: Risk stratification
• “Risk” patients: involvement of liver, spleen, lungs, bone marrow; age < 2 yrs
• “Low-risk” patients: none of the above

DAL HX, LCH-I and LCH-II: DAL HX, LCH-I and LCH-II: ConclusionsConclusions
• overall survival of multi-system patients overall survival of multi-system patients was about 80% on all studies was about 80% on all studies
• patients with lack of response at week 12 patients with lack of response at week 12 have a high risk of poor outcomehave a high risk of poor outcome
• 20% of patients do not respond to current 20% of patients do not respond to current therapy -> new treatments neededtherapy -> new treatments needed
• prolonged therapy has potential benefitprolonged therapy has potential benefit

LCH-III: Overall GoalsLCH-III: Overall Goals
• to deliver risk-adapted therapyto deliver risk-adapted therapy
• to evaluate response in various risk to evaluate response in various risk groupsgroups
• to assess morbidity in various risk groupsto assess morbidity in various risk groups

LCH-III: DesignLCH-III: Design
• adds methotrexate for “risk” patientsadds methotrexate for “risk” patients
• adds stratifications for multifocal bone adds stratifications for multifocal bone only patients and CNS patientsonly patients and CNS patients
• patients with involvement of facial bones patients with involvement of facial bones or middle cranial fossa have 3-fold risk or middle cranial fossa have 3-fold risk for DIfor DI

LCH in AdultsLCH in Adults
• most adults with LCH have pulmonary LCHmost adults with LCH have pulmonary LCH
• most are smokers most are smokers
• symptoms: cough, shortness of breath, chest symptoms: cough, shortness of breath, chest pain, sputum production, pneumothoracespain, sputum production, pneumothoraces
• CXR: diffuse bilateral infiltrates -> progress CXR: diffuse bilateral infiltrates -> progress to cyst formation and “honeycombing”to cyst formation and “honeycombing”
• Treatment: reports that 2-CdA is effectiveTreatment: reports that 2-CdA is effective

LCHLCHChildren vs AdultsChildren vs Adults
• AdultsAdults• Some lesions are not Some lesions are not
clonalclonal
• LC cells more LC cells more mature: CD86+mature: CD86+
• No IL-10 in No IL-10 in macrophagesmacrophages
• ChildrenChildren• All lesions are clonalAll lesions are clonal
• LC cells less LC cells less mature: CD86-mature: CD86-
• IL-10 expressed in IL-10 expressed in macrophagesmacrophages
Treatment Options for Treatment Options for Recurrent/Refractory LCHRecurrent/Refractory LCH
• Other chemo (Ara-C, methotrexate, cytoxan)Other chemo (Ara-C, methotrexate, cytoxan)
• cyclosporinecyclosporine
• interferoninterferon
• retinoic acid (France)retinoic acid (France)
• thalidomide (Texas Children’s Cancer Ctr)thalidomide (Texas Children’s Cancer Ctr)
• allogeneic bone marrow transplantationallogeneic bone marrow transplantation
• 2-chlorodeoxyadenosine (2-CdA) +/- Ara-C2-chlorodeoxyadenosine (2-CdA) +/- Ara-C

2-CdA for refractory LCH2-CdA for refractory LCH
• ReviewReview: 27 pts with refractory LCH were : 27 pts with refractory LCH were treated with 2CdA (23) or 2-DCF (4)treated with 2CdA (23) or 2-DCF (4)
• DosesDoses: 0.1 mg/kg/d - 13 mg/m2/day x 5-7 : 0.1 mg/kg/d - 13 mg/m2/day x 5-7 days for 1-6 coursesdays for 1-6 courses
• ResultsResults: 15 CR, 5 PR, 5 NR; no toxic deaths: 15 CR, 5 PR, 5 NR; no toxic deaths
• ToxicitiesToxicities: myelosuppression, prolonged : myelosuppression, prolonged thrombocytopenia, peripheral neuropathiesthrombocytopenia, peripheral neuropathies

LCH-S-98: Salvage trialLCH-S-98: Salvage trial
• for pts with relapsed or refractory LCHfor pts with relapsed or refractory LCH
• must have failed multi-agent therapy and must have failed multi-agent therapy and have high-risk diseasehave high-risk disease
• 2-CdA 5 mg/m2/day x 5 days q 3 wks x 6 2-CdA 5 mg/m2/day x 5 days q 3 wks x 6 coursescourses
• next salvage trial will add low-dose Ara-C to next salvage trial will add low-dose Ara-C to this dose of 2-CdAthis dose of 2-CdA

Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Why does it happen?Why does it happen?
• Epidemiologic study of possible risk Epidemiologic study of possible risk factors published in 1997factors published in 1997
• conducted in conjunction with HAAconducted in conjunction with HAA
• 22-page self-administered questionnaire 22-page self-administered questionnaire
• parents of 900 LCH patients in HAAparents of 900 LCH patients in HAA
• 63% response rate63% response rate
• 459 patients met all eligibility criteria459 patients met all eligibility criteria

Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Study of risk factorsStudy of risk factors
• Possible associations:Possible associations:– neonatal infections (cause or effect?)neonatal infections (cause or effect?)– exposure to solvents (acetone)exposure to solvents (acetone)– thyroid disease in family membersthyroid disease in family members
• No association:No association:– in utero exposure to cigarette smokein utero exposure to cigarette smoke– maternal infections or medicationsmaternal infections or medications

Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Challenges for the Future Challenges for the Future
• Better understanding of histiocyte biologyBetter understanding of histiocyte biology– differences between normal LC’s, LCHdifferences between normal LC’s, LCH– differences between localized, extensive LCHdifferences between localized, extensive LCH– differences between childhood, adult LCHdifferences between childhood, adult LCH
• Better understanding of LCH epidemiologyBetter understanding of LCH epidemiology– genetic and environmental factors genetic and environmental factors
Langerhans Cell Histiocytosis: Langerhans Cell Histiocytosis: Challenges for the Future Challenges for the Future
• New treatments for both newly diagnosed New treatments for both newly diagnosed and relapsed patientsand relapsed patients– more effectivemore effective– fewer side effectsfewer side effects– ““targeted” therapy (CD1a-linked radioisotope)targeted” therapy (CD1a-linked radioisotope)














![Title [原著]An Autopsy Case of Histiocytic Medullary ...okinawa-repo.lib.u-ryukyu.ac.jp/bitstream/20.500.12001/...The findings of this case were those of histiocytic medullary reticulosis,](https://img.pdfslide.net/doc/110x75/610486836382170066209593/title-ean-autopsy-case-of-histiocytic-medullary-okinawa-repolibu-.jpg)





![1 [Poster] Xanthogranuloma in the su- prasellar region: a](https://img.pdfslide.net/doc/110x75/62cdee8c07244125e8260f9d/1-poster-xanthogranuloma-in-the-su-prasellar-region-a-.jpg)







