Embed Size (px)
Citation preview
Brad Cutrell, MD
Assistant Professor
VA North Texas Healthcare System, Dallas, TX
University of Texas Southwestern, Dallas, TX
HIV and Cardiovascular Disease:
Practical Management Strategies
I have no relevant financial
disclosures or conflicts of interest and
will not be discussing non-FDA
approved drug uses.
Learning Objectives
By the end of this presentation, participants will be able to:
Explain contribution of traditional risk factors and ART to incidence of CVD in HIV
Describe two pathogenic mechanisms that lead to increased CVD in HIV
Apply JNC 8 guidelines to the management of hypertension
List four specific patient groups with an indication for statin therapy based on currentACC/AHA cholesterol guidelines
Outline
Summary Overviews
– CVD Epidemiology in HIV
– CVD Pathogenesis in HIV
– CVD Risk Prediction in HIV
Atherosclerotic CVD Primary and Secondary Prevention in HIV: Clinical Management Strategies
Topics Not Covered
Other Manifestations of Cardiac Disease
– Pericardial Disease
– Heart failure and Cardiomyopathy
– Arrhythmias and Sudden Cardiac Death
– Pulmonary HTN
Acute Management of ACS
CVD EPIDEMIOLOGY IN HIV
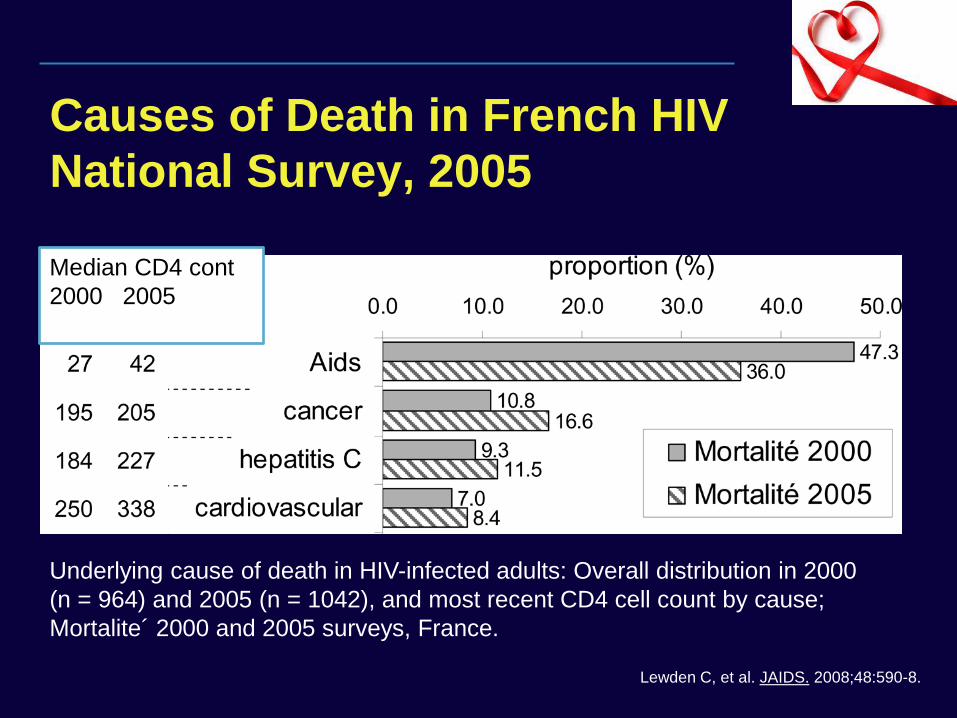
Causes of Death in French HIV
National Survey, 2005
Lewden C, et al. JAIDS. 2008;48:590-8.
Median CD4 cont
2000 2005
Underlying cause of death in HIV-infected adults: Overall distribution in 2000
(n = 964) and 2005 (n = 1042), and most recent CD4 cell count by cause;
Mortalite´ 2000 and 2005 surveys, France.
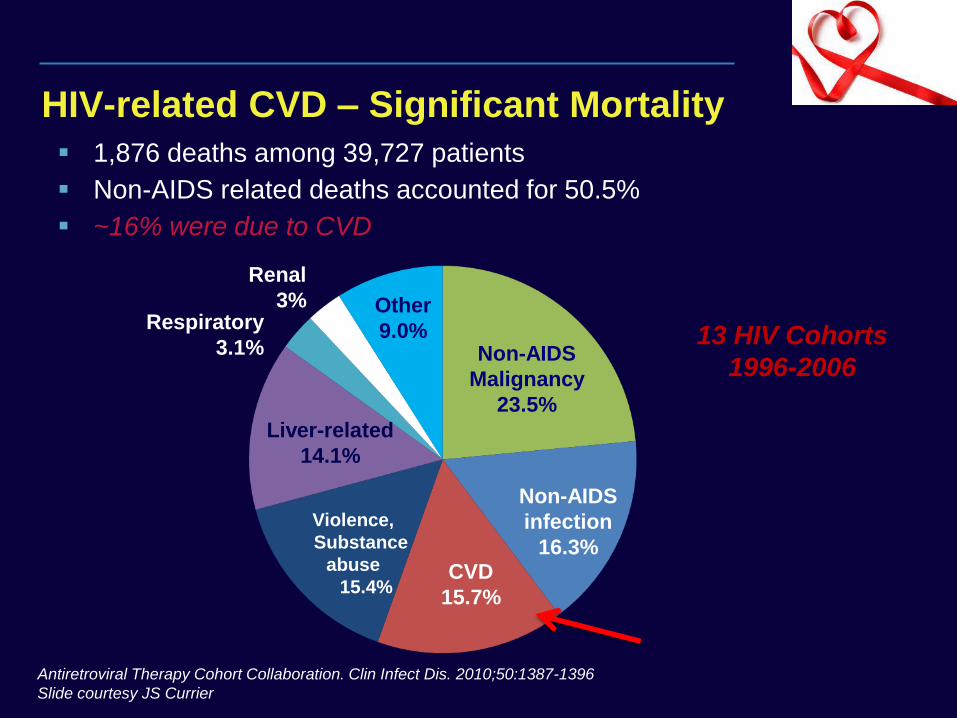
HIV-related CVD – Significant Mortality
1,876 deaths among 39,727 patients
Non-AIDS related deaths accounted for 50.5%
~16% were due to CVD
13 HIV Cohorts
1996-2006
CVD
15.7%
Non-AIDS
infection
16.3%
Non-AIDS
Malignancy
23.5%
Violence,
Substance
abuse
15.4%
Liver-related
14.1%
Other
9.0% Respiratory
3.1%
Renal
3%
Antiretroviral Therapy Cohort Collaboration. Clin Infect Dis. 2010;50:1387-1396
Slide courtesy JS Currier
CVD Incidence Rates in HIV
Increased CVD incidence in HIV-infected patients compared to uninfected controls1-3
– RR for MI and clinical CVD events: 1.5 - 2.0
– Significant even after controlling for traditional risk factors
– RR more pronounced in younger age groups
– Absolute risk remains low in most cohorts due to youth
Data limited by small event numbers and incomplete capture of other cardiac risk factors
1. Currier J, et al. JAIDS. 2003; 33:506-512. 2. Triant V, et al. J Clin Endocrinol Metab. 2007; 92:2506-12.
3. Klein D, et al. JAIDS. 2002; 30:471-77.
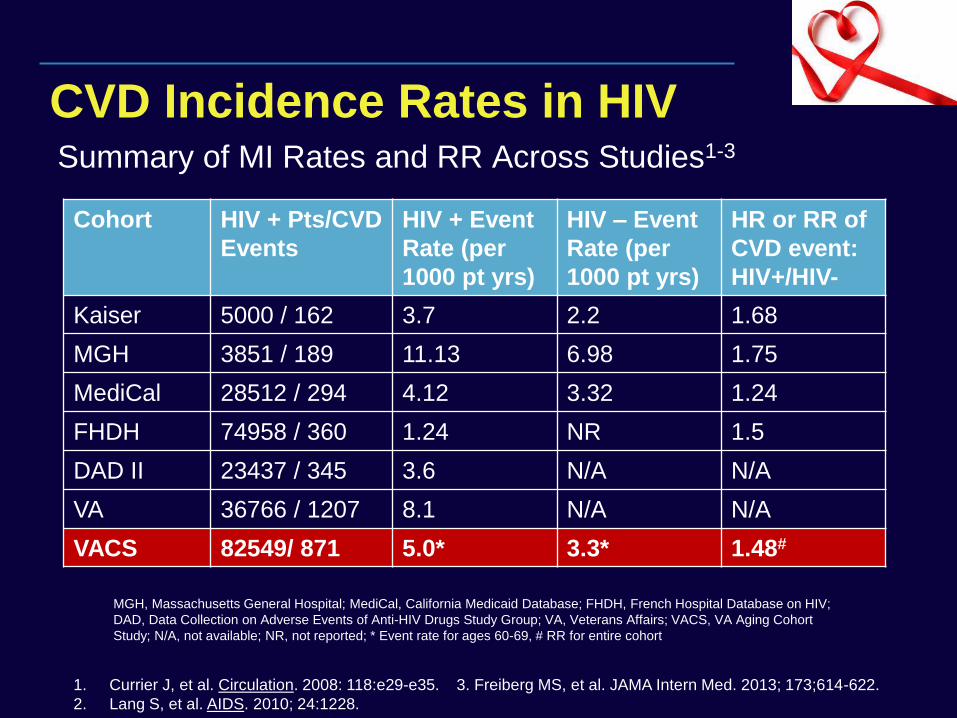
CVD Incidence Rates in HIV Summary of MI Rates and RR Across Studies1-3
Cohort HIV + Pts/CVD
Events
HIV + Event
Rate (per
1000 pt yrs)
HIV – Event
Rate (per
1000 pt yrs)
HR or RR of
CVD event:
HIV+/HIV-
Kaiser 5000 / 162 3.7 2.2 1.68
MGH 3851 / 189 11.13 6.98 1.75
MediCal 28512 / 294 4.12 3.32 1.24
FHDH 74958 / 360 1.24 NR 1.5
DAD II 23437 / 345 3.6 N/A N/A
VA 36766 / 1207 8.1 N/A N/A
VACS 82549/ 871 5.0* 3.3* 1.48#
1. Currier J, et al. Circulation. 2008: 118:e29-e35. 3. Freiberg MS, et al. JAMA Intern Med. 2013; 173;614-622.
2. Lang S, et al. AIDS. 2010; 24:1228.
MGH, Massachusetts General Hospital; MediCal, California Medicaid Database; FHDH, French Hospital Database on HIV;
DAD, Data Collection on Adverse Events of Anti-HIV Drugs Study Group; VA, Veterans Affairs; VACS, VA Aging Cohort
Study; N/A, not available; NR, not reported; * Event rate for ages 60-69, # RR for entire cohort
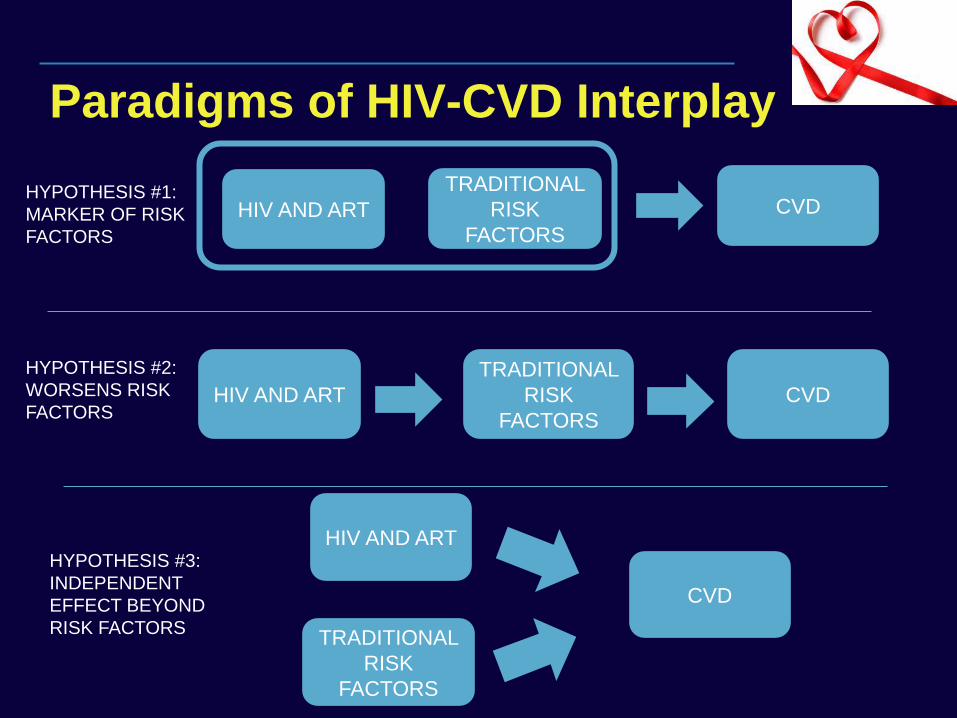
Paradigms of HIV-CVD Interplay
HIV AND ART
TRADITIONAL
RISK
FACTORS
CVD
TRADITIONAL
RISK
FACTORS
CVD HIV AND ART
HIV AND ART
TRADITIONAL
RISK
FACTORS
CVD
HYPOTHESIS #1:
MARKER OF RISK
FACTORS
HYPOTHESIS #2:
WORSENS RISK
FACTORS
HYPOTHESIS #3:
INDEPENDENT
EFFECT BEYOND
RISK FACTORS
CVD Risk Factors
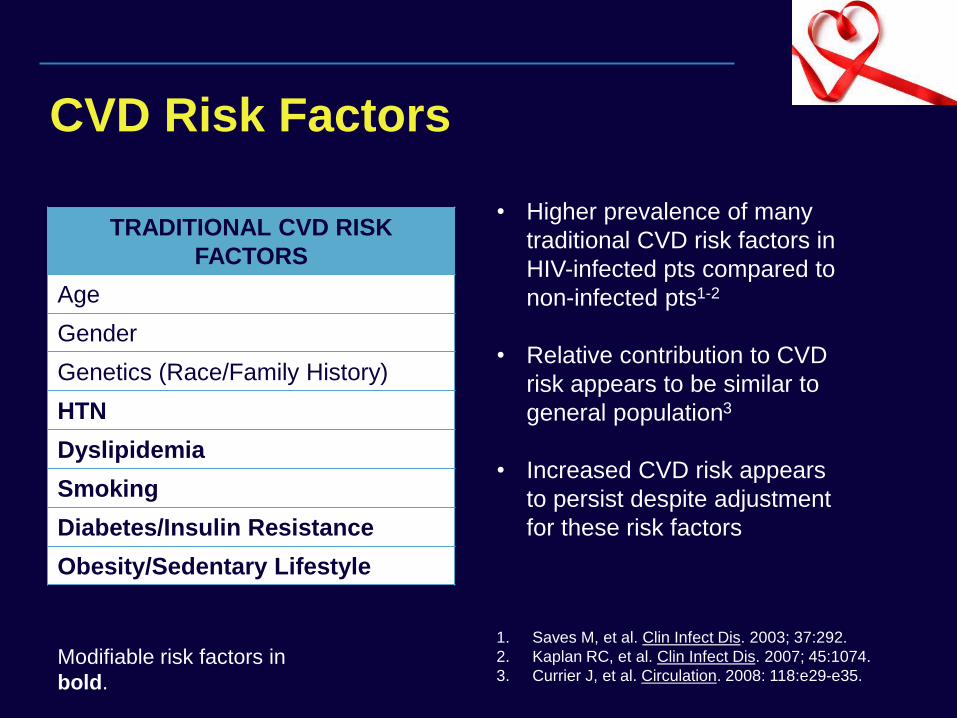
TRADITIONAL CVD RISK
FACTORS
Age
Gender
Genetics (Race/Family History)
HTN
Dyslipidemia
Smoking
Diabetes/Insulin Resistance
Obesity/Sedentary Lifestyle
Modifiable risk factors in
bold.
• Higher prevalence of many
traditional CVD risk factors in
HIV-infected pts compared to
non-infected pts1-2
• Relative contribution to CVD
risk appears to be similar to
general population3
• Increased CVD risk appears
to persist despite adjustment
for these risk factors
1. Saves M, et al. Clin Infect Dis. 2003; 37:292.
2. Kaplan RC, et al. Clin Infect Dis. 2007; 45:1074.
3. Currier J, et al. Circulation. 2008: 118:e29-e35.
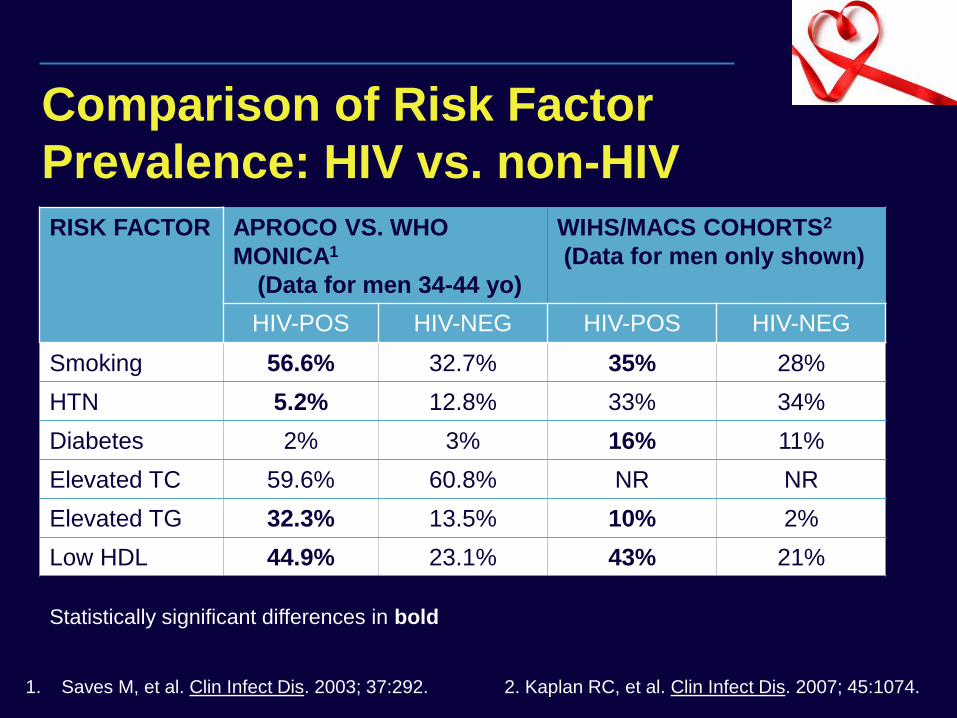
Comparison of Risk Factor
Prevalence: HIV vs. non-HIV
RISK FACTOR APROCO VS. WHO
MONICA1
(Data for men 34-44 yo)
WIHS/MACS COHORTS2
(Data for men only shown)
HIV-POS HIV-NEG HIV-POS HIV-NEG
Smoking 56.6% 32.7% 35% 28%
HTN 5.2% 12.8% 33% 34%
Diabetes 2% 3% 16% 11%
Elevated TC 59.6% 60.8% NR NR
Elevated TG 32.3% 13.5% 10% 2%
Low HDL 44.9% 23.1% 43% 21%
Statistically significant differences in bold
1. Saves M, et al. Clin Infect Dis. 2003; 37:292. 2. Kaplan RC, et al. Clin Infect Dis. 2007; 45:1074.
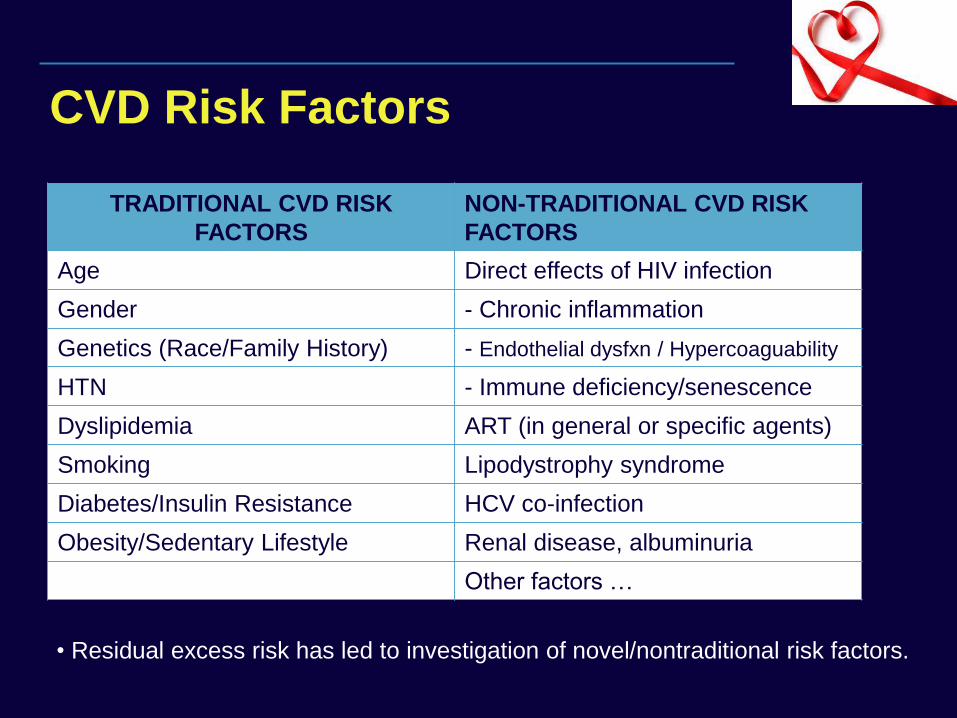
CVD Risk Factors
TRADITIONAL CVD RISK
FACTORS
Age
Gender
Genetics (Race/Family History)
HTN
Dyslipidemia
Smoking
Diabetes/Insulin Resistance
Obesity/Sedentary Lifestyle
NON-TRADITIONAL CVD RISK
FACTORS
Direct effects of HIV infection
- Chronic inflammation
- Endothelial dysfxn / Hypercoaguability
- Immune deficiency/senescence
ART (in general or specific agents)
Lipodystrophy syndrome
HCV co-infection
Renal disease, albuminuria
Other factors …
• Residual excess risk has led to investigation of novel/nontraditional risk factors.
HAART and the Heart
Association between ART exposure and increased CV events in most studies (except early large VA study) 1-3
Exposure to older protease inhibitors (e.g. lopinavir-ritonavir) most consistent association of risk, likely mediated by lipids; limited data but less concern with newer PIs1-2
Some but not all studies show association with recent use of abacavir; failure to account for confounding from CKD possible explanation4-5
ART interruption associated with higher rates of CV events in SMART study compared to continuous arm (1.3/100 py vs. 0.8/100 py) 6
1. DAD:Friis-Moller N, et al. N Engl J Med. 2007; 356:1723.
2. Mary-Krause M, et al. AIDS. 2003; 17:2479.
3. Bozzette SA, et al. N Engl J Med. 2003; 348:702.
4. DAD :Sabin CA, et al. Lancet. 2008; 371:1417.
5. Bedimo RJ, et al. Clin Infect Dis. 2011; 53:84.
6. SMART Study: El-Sadr WM, et al. N Engl J Med. 2006;
355:2283.
CVD Epidemiology Summary
Increased relative risk of CVD events in HIV-infected patients compared to uninfected patients
Higher prevalence of traditional CVD risk factors (such as smoking) partially explains increased risk
Select ART (primarily older PIs) are associated with increased risk, likely from worsening traditional risk factors
Benefits of HAART and CVD risk associated with treatment interruption outweigh CVD risks of treatment
CVD PATHOGENESIS IN HIV
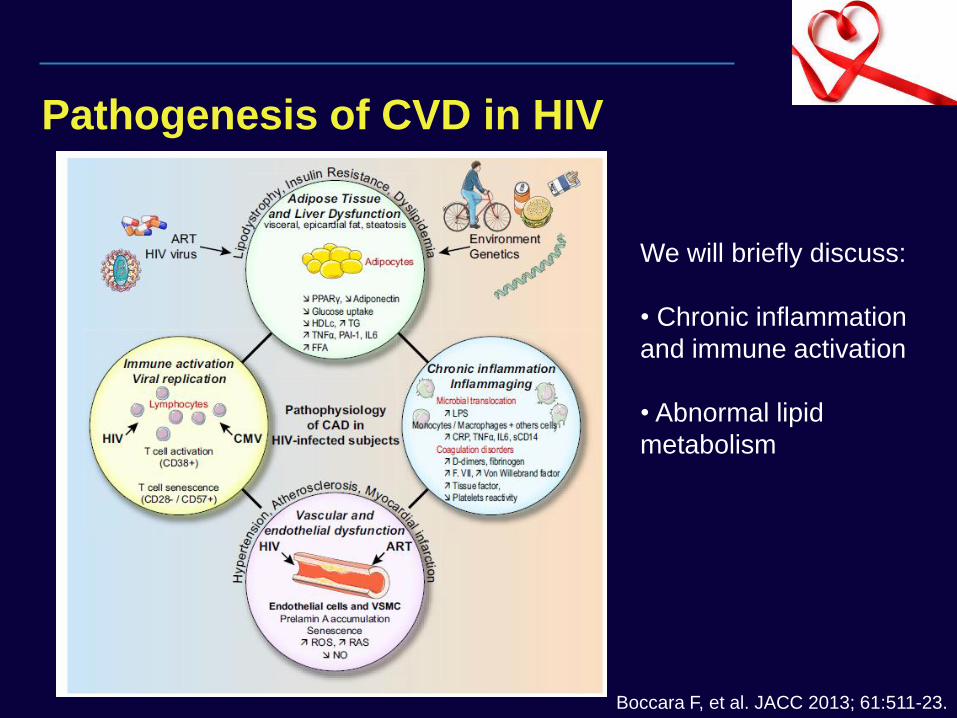
Pathogenesis of CVD in HIV
Boccara F, et al. JACC 2013; 61:511-23.
We will briefly discuss:
• Chronic inflammation
and immune activation
• Abnormal lipid
metabolism
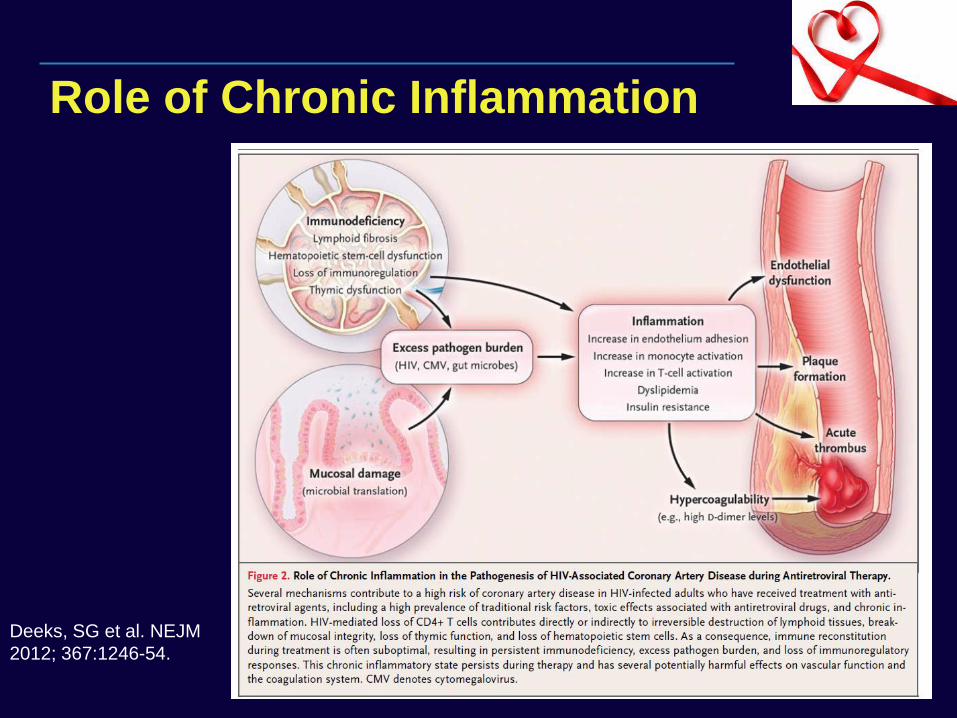
Deeks, SG et al. NEJM
2012; 367:1246-54.
Role of Chronic Inflammation
clinicaloptions.com/hiv
The Challenges of Managing the Aging HIV-Infected Patient
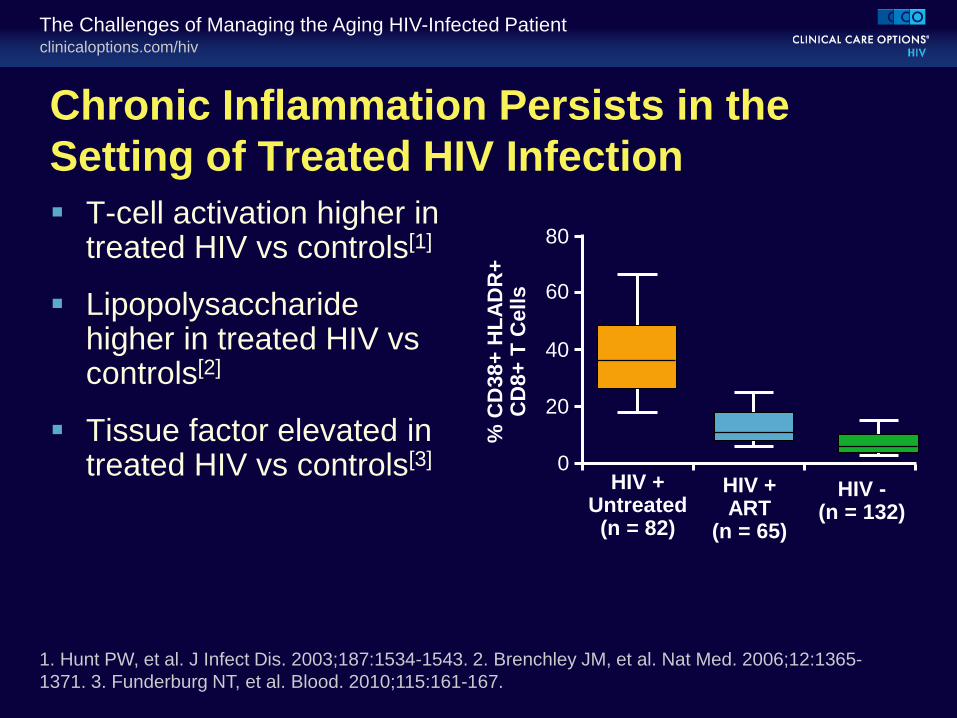
Chronic Inflammation Persists in the
Setting of Treated HIV Infection
T-cell activation higher in treated HIV vs controls[1]
Lipopolysaccharide higher in treated HIV vs controls[2]
Tissue factor elevated in treated HIV vs controls[3]
1. Hunt PW, et al. J Infect Dis. 2003;187:1534-1543. 2. Brenchley JM, et al. Nat Med. 2006;12:1365-
1371. 3. Funderburg NT, et al. Blood. 2010;115:161-167.
% C
D38+
HL
AD
R+
C
D8+
T C
ells
80
60
40
20
0 HIV +
Untreated (n = 82)
HIV + ART
(n = 65)
HIV - (n = 132)
clinicaloptions.com/hiv
The Challenges of Managing the Aging HIV-Infected Patient
Low CD4+ Count Associated With CVD
Nadir CD4+ cell count ≤ 200 cells/mm³ independently associated with carotid IMT[1,2]
Proximal CD4+ cell count during therapy associated with incident CVD and AMI[3]
Kaiser study: higher risk of CHD seen only in treated HIV+ pts with either recent or lowest CD4+ cell count ≤ 200 cells/mm3[4]
Nadir CD4+ cell count < 350 cells/mm3 independently associated with worsened arterial stiffness and endothelial function[5,6]
Will there be a CV benefit in earlier initiation of antiretroviral therapy?
1. Hsue PY, et al. Circulation. 2004;109:1603-1608. 2. Triant VA, et al. J Acquir Immune Defic Syndr.
2010;55:615-619. 3. Lichtenstein KA, et al. Clin Infect Dis. 2010;51:435-447. 4. Klein D, et al. CROI 2011.
Abstract 810. 5. Ho JE, et al. AIDS. 2010;24:1897-1905. 6. Ho E, et al. AIDS. 2012;26:1115-1120.
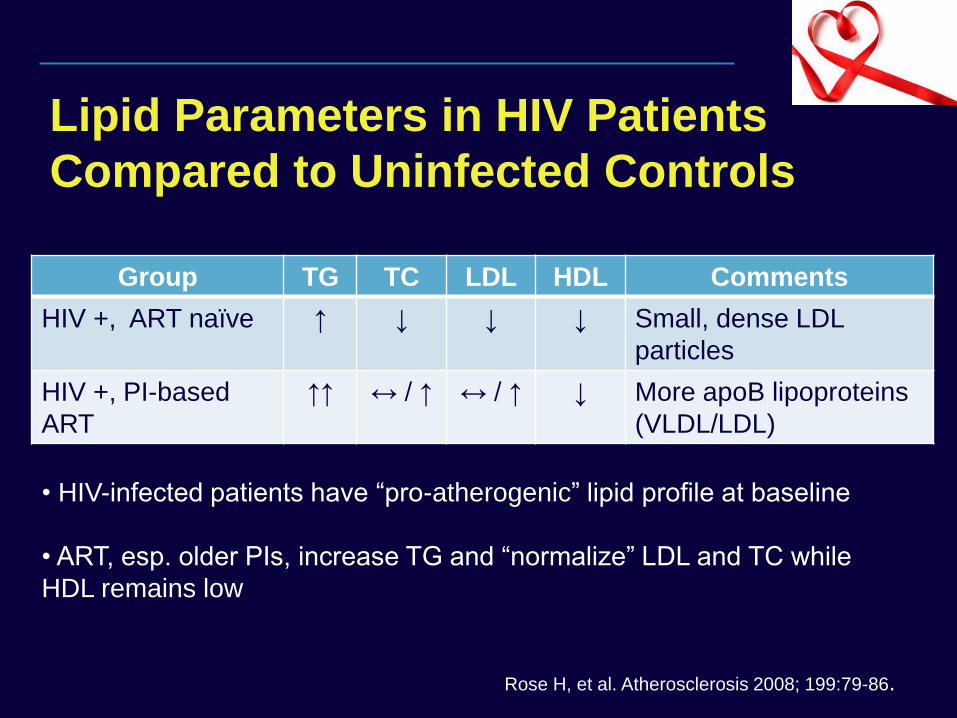
Lipid Parameters in HIV Patients
Compared to Uninfected Controls
Group TG TC LDL HDL Comments
HIV +, ART naïve ↑ ↓ ↓ ↓ Small, dense LDL
particles
HIV +, PI-based
ART
↑↑ ↔ / ↑ ↔ / ↑ ↓ More apoB lipoproteins
(VLDL/LDL)
Rose H, et al. Atherosclerosis 2008; 199:79-86.
• HIV-infected patients have “pro-atherogenic” lipid profile at baseline
• ART, esp. older PIs, increase TG and “normalize” LDL and TC while
HDL remains low
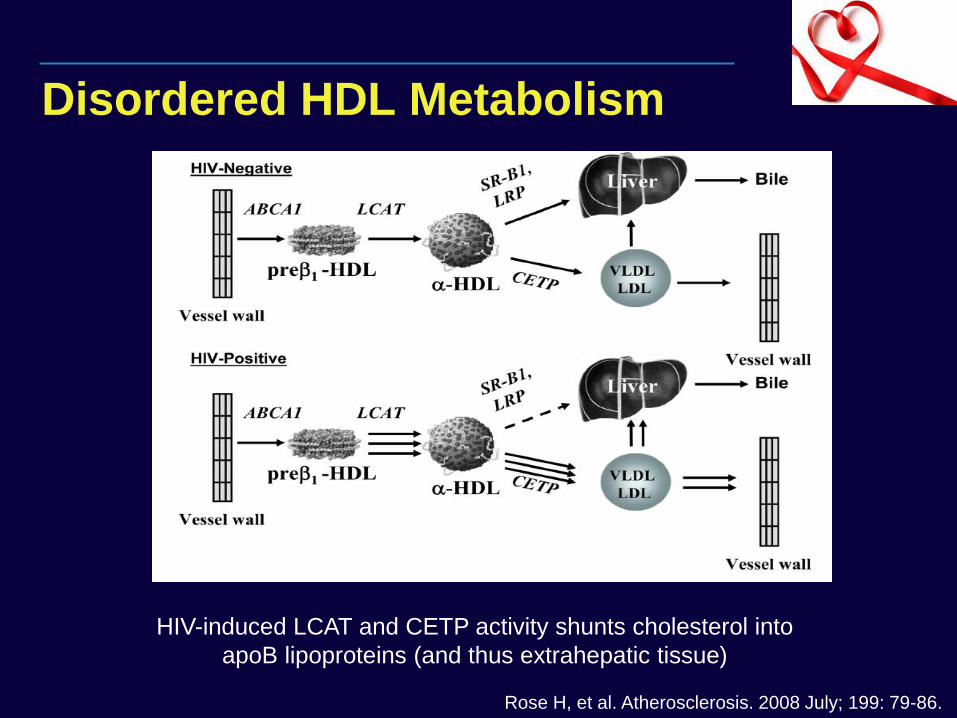
Disordered HDL Metabolism
Rose H, et al. Atherosclerosis. 2008 July; 199: 79-86.
HIV-induced LCAT and CETP activity shunts cholesterol into
apoB lipoproteins (and thus extrahepatic tissue)
CVD RISK PREDICTION IN HIV
CVD Risk Prediction
Goal is to match the intensity of CV risk factor modification to the predicted
risk of CVD?
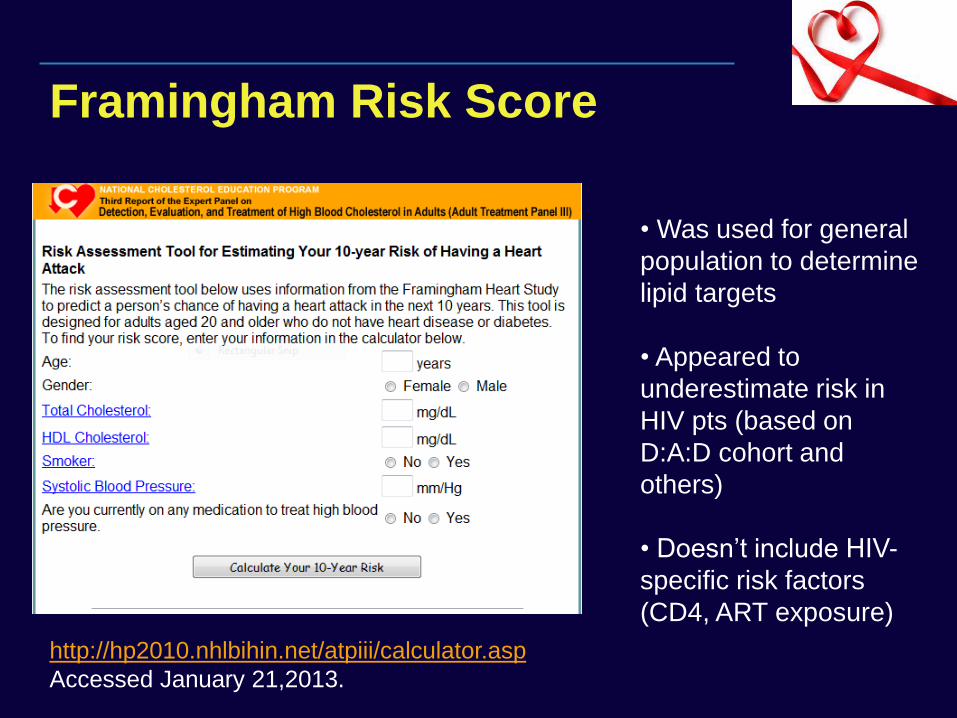
Framingham Risk Score
http://hp2010.nhlbihin.net/atpiii/calculator.asp
Accessed January 21,2013.
• Was used for general
population to determine
lipid targets
• Appeared to
underestimate risk in
HIV pts (based on
D:A:D cohort and
others)
• Doesn’t include HIV-
specific risk factors
(CD4, ART exposure)
clinicaloptions.com/hiv
Clinical Impact of New Data From ICAAC, IDWeek, and EACS 2013
D:A:D Updated Models of Global CVD
Risk/Comparison With Framingham
Retrospective analysis of 32,663 HIV+ persons from 20 countries in Europe and Australia with
– No CVD disease at entry to study, and
– Data on CVD risk factors
1010 CVD events in 186,364.5 PY → overall rate of 5.42/1000 PY (95% CI: 5.09-5.76)
– Includes MI (n = 493); stroke (n = 295); angioplasty (n = 129); bypass (n = 44); other CVD death (n = 36); carotid endarterectomy (n = 13)
– 2 D:A:D models used (1 including exposure to certain ARV agents) and compared with Framingham model
Friis-Møller N, et al. EACS 2013. Abstract PS1/3.
clinicaloptions.com/hiv
Clinical Impact of New Data From ICAAC, IDWeek, and EACS 2013
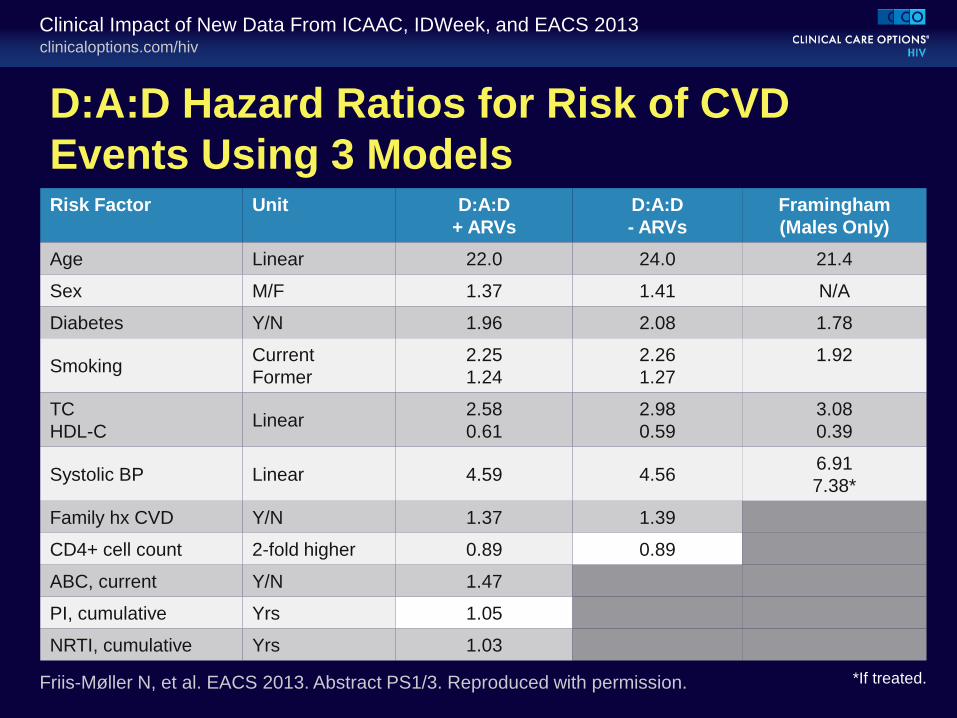
D:A:D Hazard Ratios for Risk of CVD
Events Using 3 Models
*If treated. Friis-Møller N, et al. EACS 2013. Abstract PS1/3. Reproduced with permission.
Risk Factor Unit D:A:D
+ ARVs
D:A:D
- ARVs
Framingham
(Males Only)
Age Linear 22.0 24.0 21.4
Sex M/F 1.37 1.41 N/A
Diabetes Y/N 1.96 2.08 1.78
Smoking Current
Former
2.25
1.24
2.26
1.27
1.92
TC
HDL-C Linear
2.58
0.61
2.98
0.59
3.08
0.39
Systolic BP Linear 4.59 4.56 6.91
7.38*
Family hx CVD Y/N 1.37 1.39
CD4+ cell count 2-fold higher 0.89 0.89
ABC, current Y/N 1.47
PI, cumulative Yrs 1.05
NRTI, cumulative Yrs 1.03
clinicaloptions.com/hiv
Clinical Impact of New Data From ICAAC, IDWeek, and EACS 2013
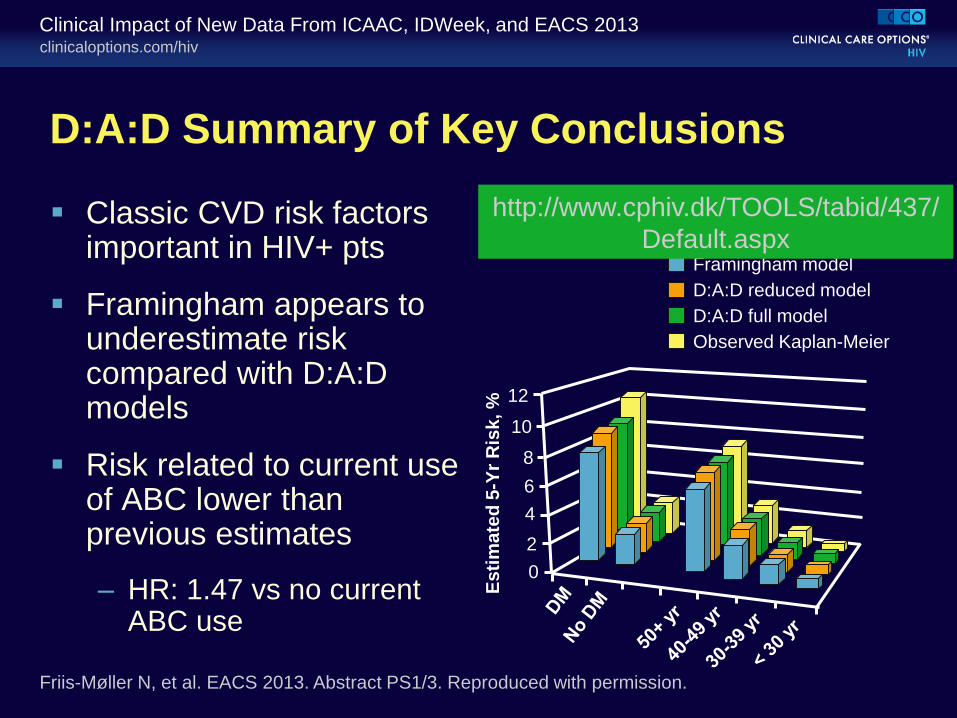
D:A:D Summary of Key Conclusions
Classic CVD risk factors important in HIV+ pts
Framingham appears to underestimate risk compared with D:A:D models
Risk related to current use of ABC lower than previous estimates
– HR: 1.47 vs no current ABC use
Framingham model
D:A:D reduced model
D:A:D full model
Observed Kaplan-Meier
5-Yr CVD Risk by Age and Diabetes Status
Es
tim
ate
d 5
-Yr
Ris
k, %
12
10
8
6
4
2
0
Friis-Møller N, et al. EACS 2013. Abstract PS1/3. Reproduced with permission.
http://www.cphiv.dk/TOOLS/tabid/437/
Default.aspx
CVD PREVENTION IN THE HIV
CLINIC
CVD Primary Prevention
To prevent CVD, first provider has to CONSIDER THE PATIENT AT RISK!
HIV guidelines generally follow those for general public with special consideration of drug-drug interactions and metabolic effects of ART
Suggested Approaches:
– Have Systematic Approach to assessing CV risk factors
– Design workflow to make it “easy” to follow guidelines
– Understand and maximize non-physician resources
– Consider dedicated “Metabolic” visit (in stable pts)
– Evaluate your practice as part of QI process
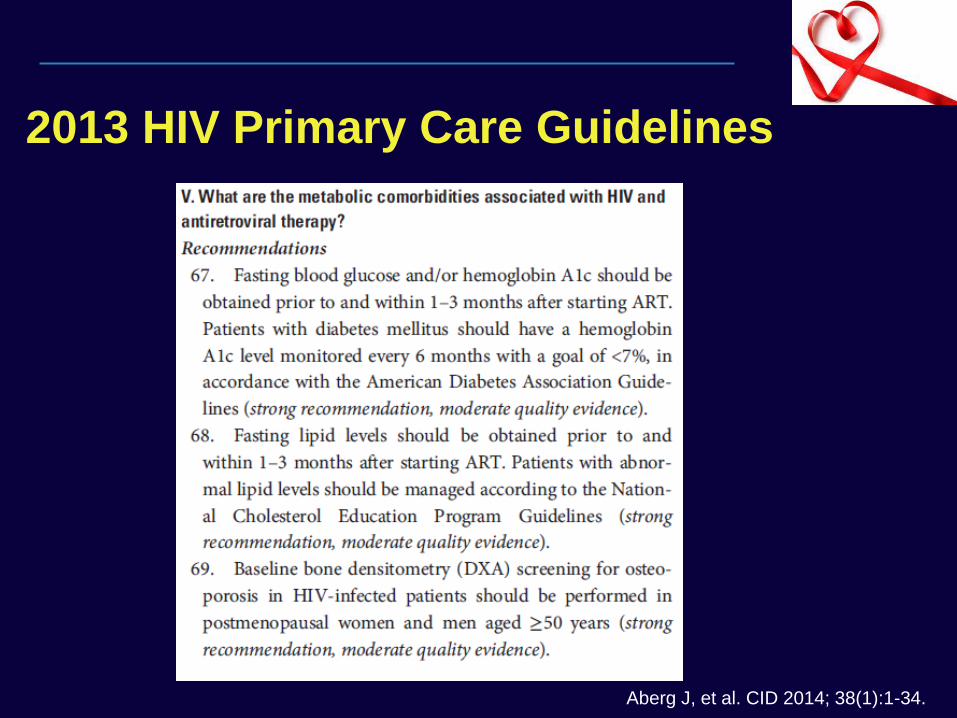
2013 HIV Primary Care Guidelines
Aberg J, et al. CID 2014; 38(1):1-34.
Clinical Inertia in CVD Prevention
Retrospective study of 90 pts in UAB HIV clinic not at LDL goal showed 44% of patients failed to have appropriate intervention over 12-month span1
– Women and pts in highest CVD risk category most likely affected by inertia, higher absolute LDL less likely
Same clinic reported study of 397 patients qualifying for ASA for primary prevention based on USPSTF guidelines, found that only 66 (17%) patients received therapy2
– OR of receipt of ASA doubled for each additional CVD risk factor
Conclusions: Clinical inertia major issue in CVD prevention in HIV clinic and clinicians tend to rely on clinical impression rather than practice guidelines
1. Willig JH, et al. Clin Infect Dis. 2008; 46:1315.
2. Burkholder GA, et al. Clin Infect Dis. 2012; 55:1550.
ABCs of CVD Prevention Aspirin
Blood pressure
Cholesterol
Diet
Exercise
Fumes (smoking)
Glucose (DM/insulin resistance)
HAART
Maximize
non-MD
resources
Utilize
pharmacist and
specialist
expertise in
complex cases
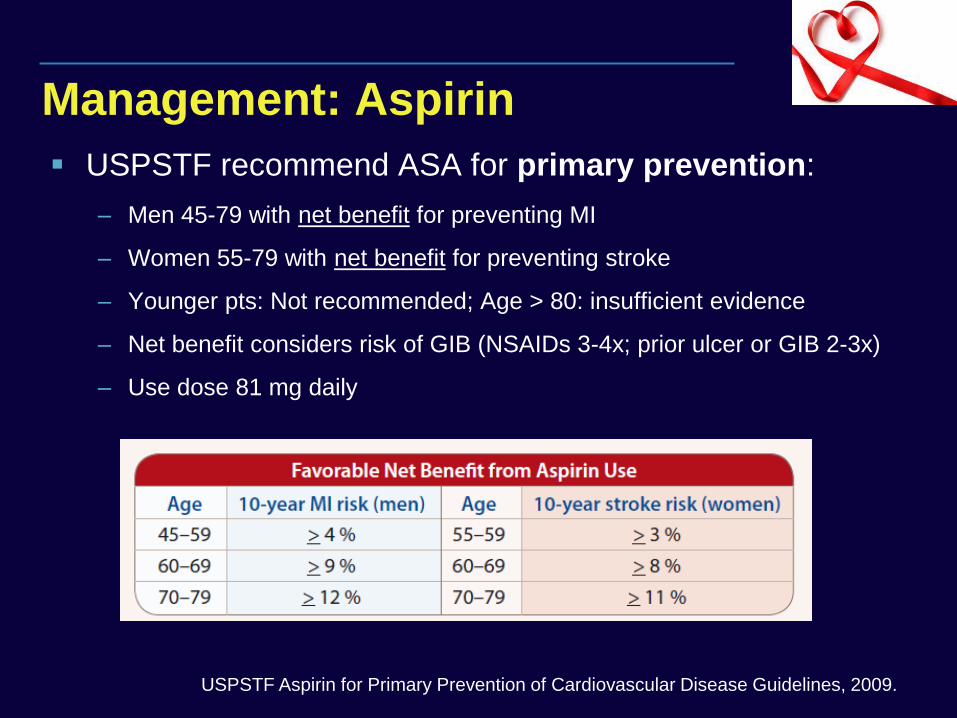
Management: Aspirin
USPSTF recommend ASA for primary prevention:
– Men 45-79 with net benefit for preventing MI
– Women 55-79 with net benefit for preventing stroke
– Younger pts: Not recommended; Age > 80: insufficient evidence
– Net benefit considers risk of GIB (NSAIDs 3-4x; prior ulcer or GIB 2-3x)
– Use dose 81 mg daily
USPSTF Aspirin for Primary Prevention of Cardiovascular Disease Guidelines, 2009.
Recent CV Guideline Changes
Updated Guidelines in late 2013:
– JNC 8: Hypertension
– ACC/AHA Management of Blood Cholesterol
– ACC/AHA Lifestyle Management
– ACC/AHA Cardiovascular Risk Assessment
– ACC/AHA Management of Obesity
Intended to apply RCT evidence to specific clinical research questions, NOT comprehensive guidelines
Controversial from outset of publication (HTN and Chol)
Management: Blood Pressure
Definition of HTN and prehypertension not addressed
Key Changes from JNC-7:
– Goal BP: < 140/90 (age 18-60), < 150/90 (age ≥ 60)
– Goal BP in diabetes/CKD: < 140/90 regardless of age
– Recommended drug classes: thiazide diuretics, ACE-I, ARB or CCB (except in AA and pts with CKD)
– 3 drug treatment titration strategies suggested
JNC 8 Guidelines for Mgmt of HTN. JAMA. Published online 12/18/13.
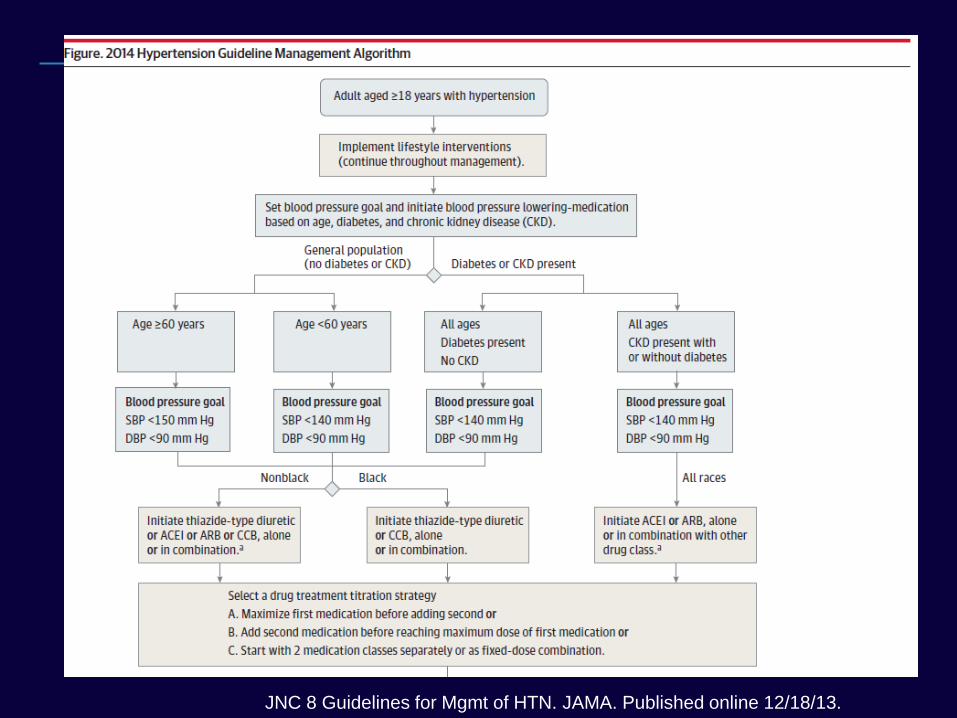
JNC 8 Guidelines for Mgmt of HTN. JAMA. Published online 12/18/13.
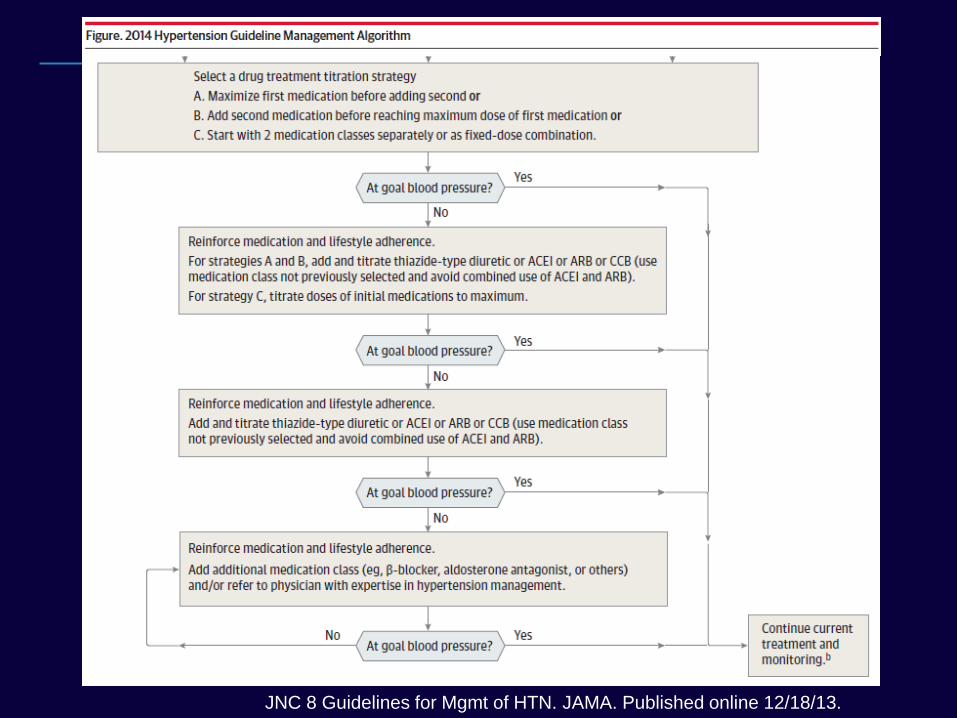
JNC 8 Guidelines for Mgmt of HTN. JAMA. Published online 12/18/13.
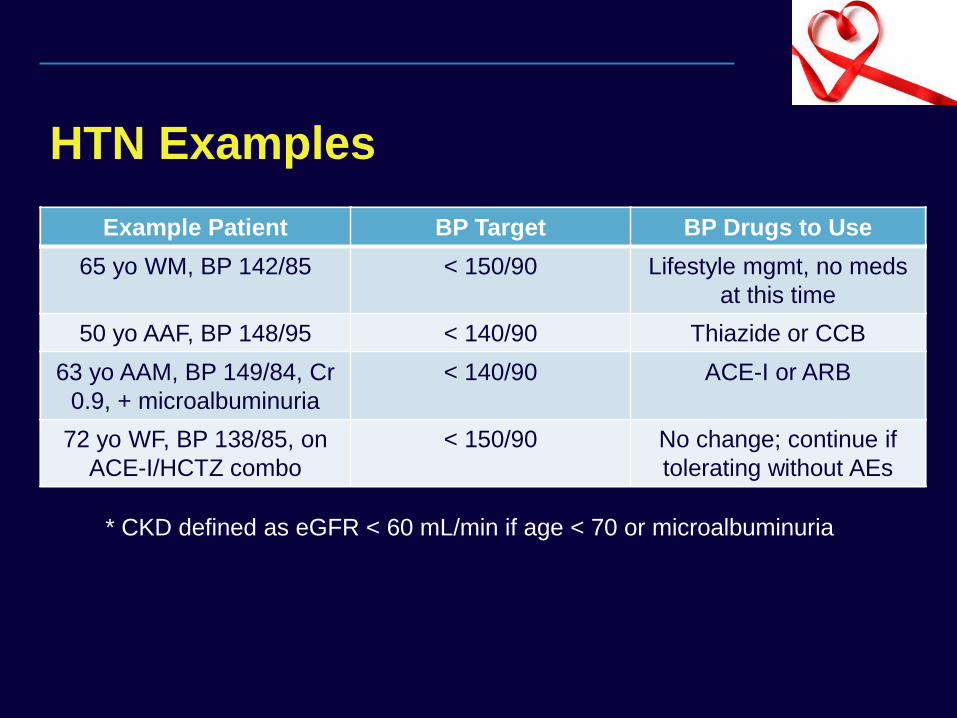
HTN Examples
Example Patient BP Target BP Drugs to Use
65 yo WM, BP 142/85
50 yo AAF, BP 148/95
63 yo AAM, BP 149/84, Cr
0.9, + microalbuminuria
72 yo WF, BP 138/85, on
ACE-I/HCTZ combo
* CKD defined as eGFR < 60 mL/min if age < 70 or microalbuminuria
Example Patient BP Target BP Drugs to Use
65 yo WM, BP 142/85 < 150/90 Lifestyle mgmt, no meds
at this time
50 yo AAF, BP 148/95
63 yo AAM, BP 149/84, Cr
0.9, + microalbuminuria
72 yo WF, BP 138/85, on
ACE-I/HCTZ combo
Example Patient BP Target BP Drugs to Use
65 yo WM, BP 142/85 < 150/90 Lifestyle mgmt, no meds
at this time
50 yo AAF, BP 148/95 < 140/90 Thiazide or CCB
63 yo AAM, BP 149/84, Cr
0.9, + microalbuminuria
72 yo WF, BP 138/85, on
ACE-I/HCTZ combo
Example Patient BP Target BP Drugs to Use
65 yo WM, BP 142/85 < 150/90 Lifestyle mgmt, no meds
at this time
50 yo AAF, BP 148/95 < 140/90 Thiazide or CCB
63 yo AAM, BP 149/84, Cr
0.9, + microalbuminuria
< 140/90 ACE-I or ARB
72 yo WF, BP 138/85, on
ACE-I/HCTZ combo
Example Patient BP Target BP Drugs to Use
65 yo WM, BP 142/85 < 150/90 Lifestyle mgmt, no meds
at this time
50 yo AAF, BP 148/95 < 140/90 Thiazide or CCB
63 yo AAM, BP 149/84, Cr
0.9, + microalbuminuria
< 140/90 ACE-I or ARB
72 yo WF, BP 138/85, on
ACE-I/HCTZ combo
< 150/90 No change; continue if
tolerating without AEs
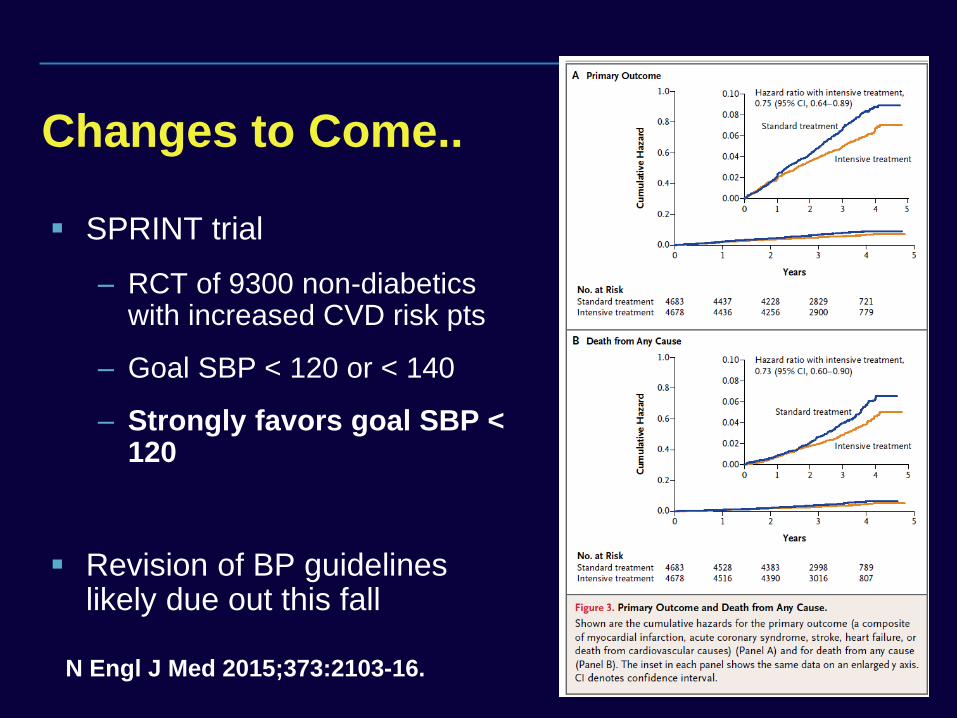
Changes to Come..
SPRINT trial
– RCT of 9300 non-diabetics with increased CVD risk pts
– Goal SBP < 120 or < 140
– Strongly favors goal SBP < 120
Revision of BP guidelines likely due out this fall
N Engl J Med 2015;373:2103-16.
Management: Cholesterol
Key Changes from New Lipid Guidelines:
– Highlights 4 groups most likely to benefit from statins
– Focus on statin intensity, NOT treatment to specific LDL or non-HDL targets
– New Pooled Risk Equation to predict 10-year ASCVD risk
– No “routine role” for non-statin therapy
– Emphasis on “patient-centered” approach with discussion of individual risk/benefits of therapy
ACC/AHA Guidelines for Mgmt of Blood Cholesterol. Stone NJ, et al. JACC. 2013
4 ASCVD Statin Benefit Groups
4 Patient Groups which benefit from statins:
– Clinical ASCVD (includes CAD, CVA/TIA, PVD)
– LDL≥ 190 mg/dL
– Diabetes age 40-75 with LDL 70-189 mg/dL
– 10-year ASCVD est. risk ≥ 7.5% with LDL 70-189 mg/dL
For NYHA II-IV heart failure and hemodialysis pts, no recommendation made due to lack of evidence proving efficacy in these populations
ACC/AHA Guidelines for Mgmt of Blood Cholesterol. Stone NJ, et al. JACC. 2013
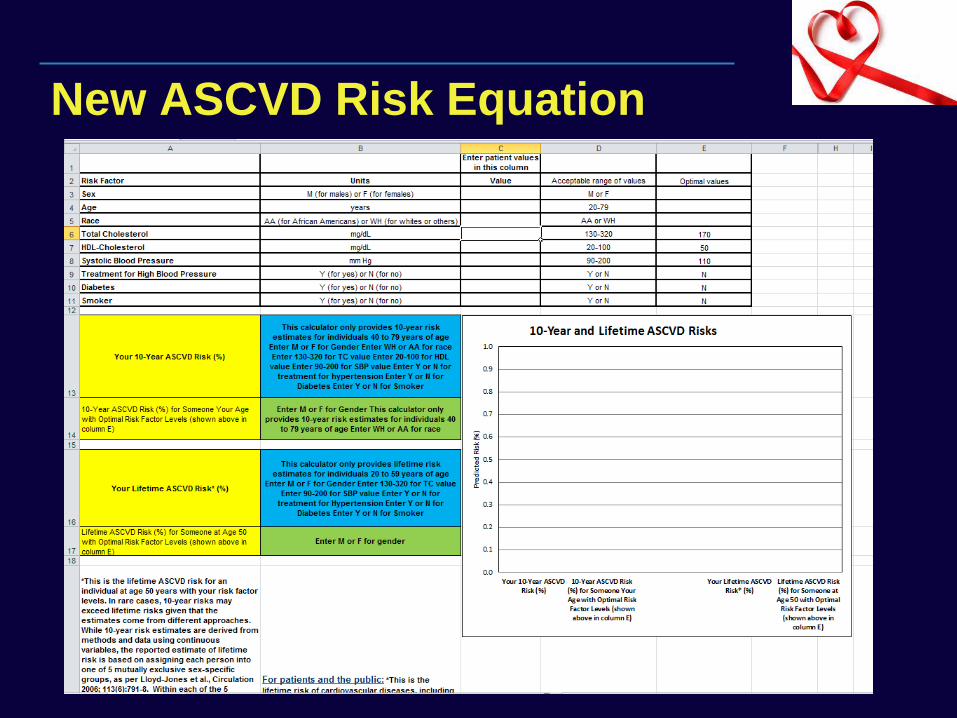
New ASCVD Risk Equation
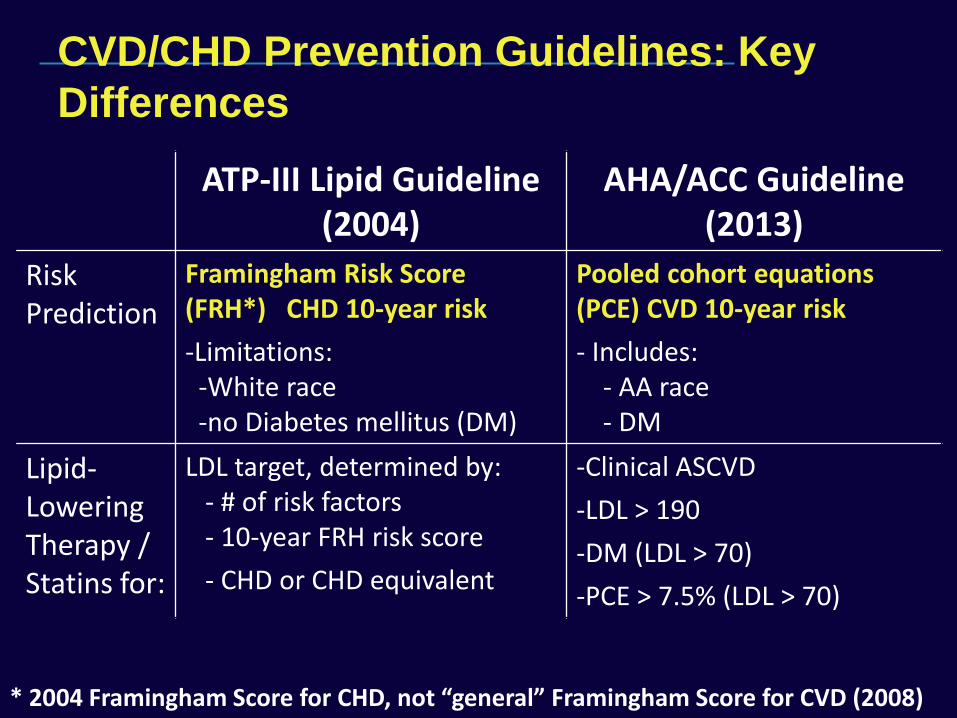
CVD/CHD Prevention Guidelines: Key
Differences
ATP-III Lipid Guideline (2004)
AHA/ACC Guideline (2013)
Risk Prediction
Framingham Risk Score (FRH*) CHD 10-year risk
-Limitations: -White race -no Diabetes mellitus (DM)
Pooled cohort equations (PCE) CVD 10-year risk
- Includes: - AA race - DM
Lipid-Lowering Therapy / Statins for:
LDL target, determined by: - # of risk factors - 10-year FRH risk score
- CHD or CHD equivalent
-Clinical ASCVD
-LDL > 190
-DM (LDL > 70)
-PCE > 7.5% (LDL > 70)
* 2004 Framingham Score for CHD, not “general” Framingham Score for CVD (2008)
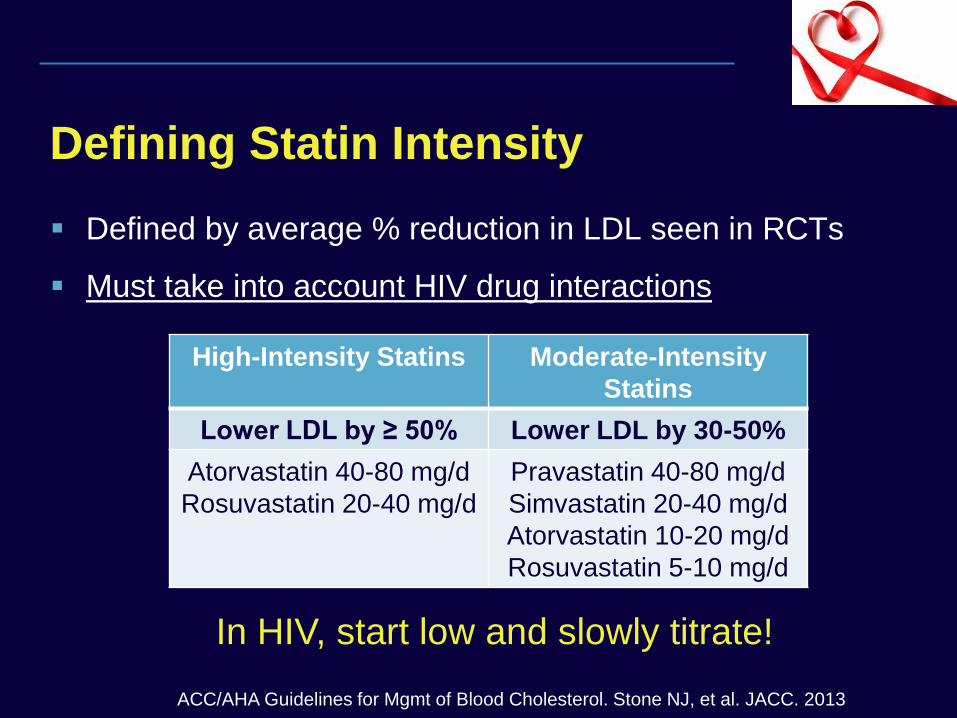
Defining Statin Intensity
Defined by average % reduction in LDL seen in RCTs
Must take into account HIV drug interactions
High-Intensity Statins Moderate-Intensity
Statins
Lower LDL by ≥ 50% Lower LDL by 30-50%
Atorvastatin 40-80 mg/d
Rosuvastatin 20-40 mg/d
Pravastatin 40-80 mg/d
Simvastatin 20-40 mg/d
Atorvastatin 10-20 mg/d
Rosuvastatin 5-10 mg/d
In HIV, start low and slowly titrate!
ACC/AHA Guidelines for Mgmt of Blood Cholesterol. Stone NJ, et al. JACC. 2013
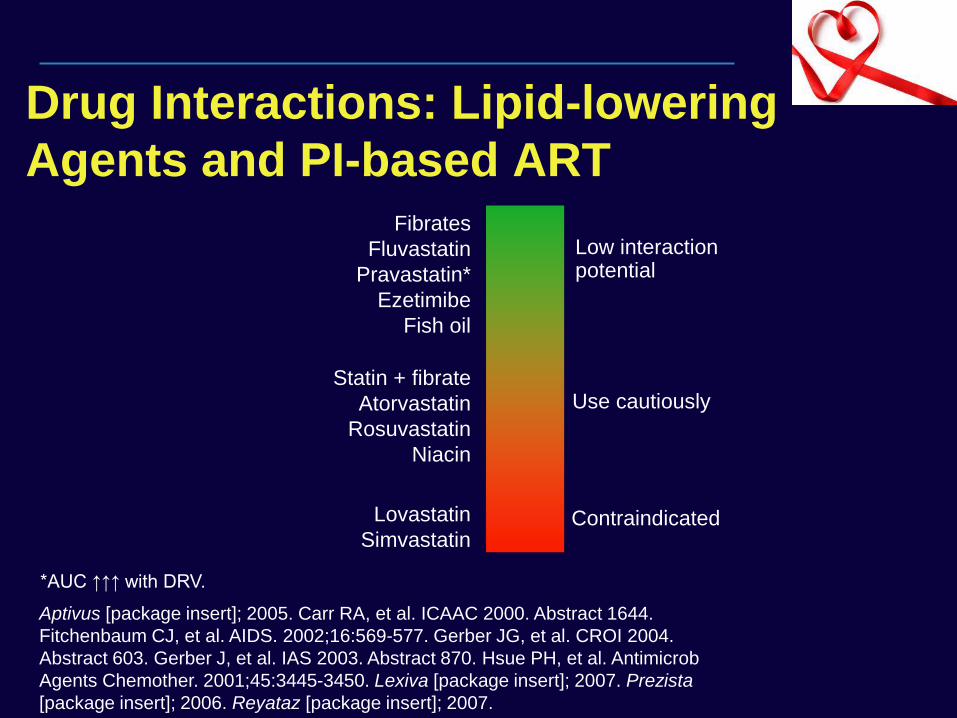
Drug Interactions: Lipid-lowering
Agents and PI-based ART
*AUC ↑↑↑ with DRV.
Fibrates
Fluvastatin
Pravastatin*
Ezetimibe
Fish oil
Use cautiously Statin + fibrate
Atorvastatin
Rosuvastatin
Niacin
Lovastatin
Simvastatin Contraindicated
Low interaction potential
Aptivus [package insert]; 2005. Carr RA, et al. ICAAC 2000. Abstract 1644.
Fitchenbaum CJ, et al. AIDS. 2002;16:569-577. Gerber JG, et al. CROI 2004.
Abstract 603. Gerber J, et al. IAS 2003. Abstract 870. Hsue PH, et al. Antimicrob
Agents Chemother. 2001;45:3445-3450. Lexiva [package insert]; 2007. Prezista
[package insert]; 2006. Reyataz [package insert]; 2007.
ACC/AHA Guidelines for Mgmt of Blood Cholesterol. Stone NJ, et al. JACC. 2013
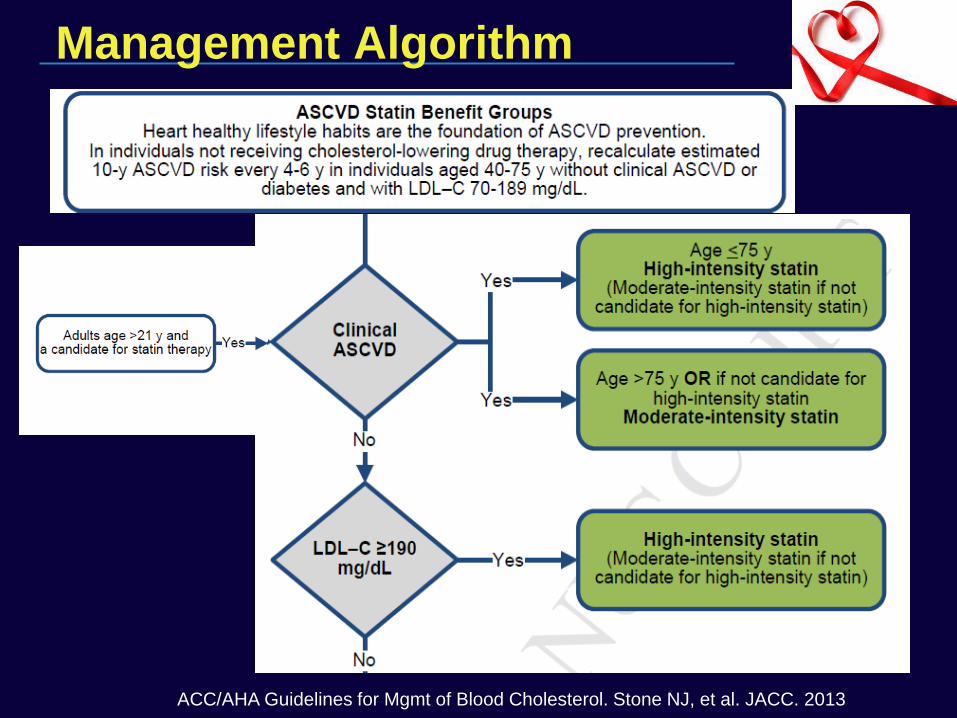
Management Algorithm
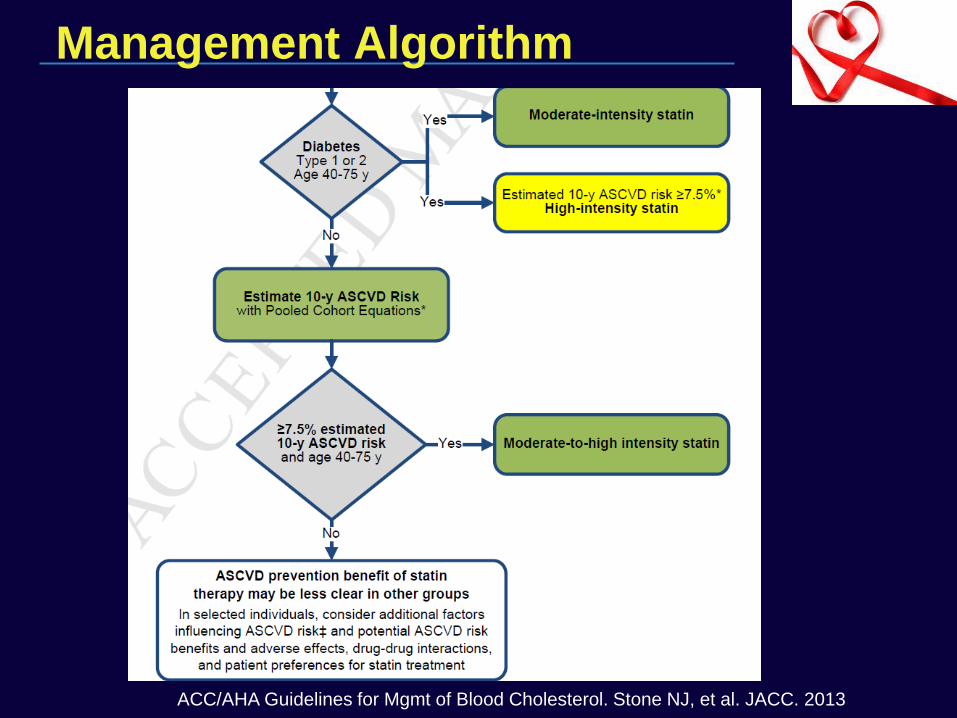
ACC/AHA Guidelines for Mgmt of Blood Cholesterol. Stone NJ, et al. JACC. 2013
Management Algorithm
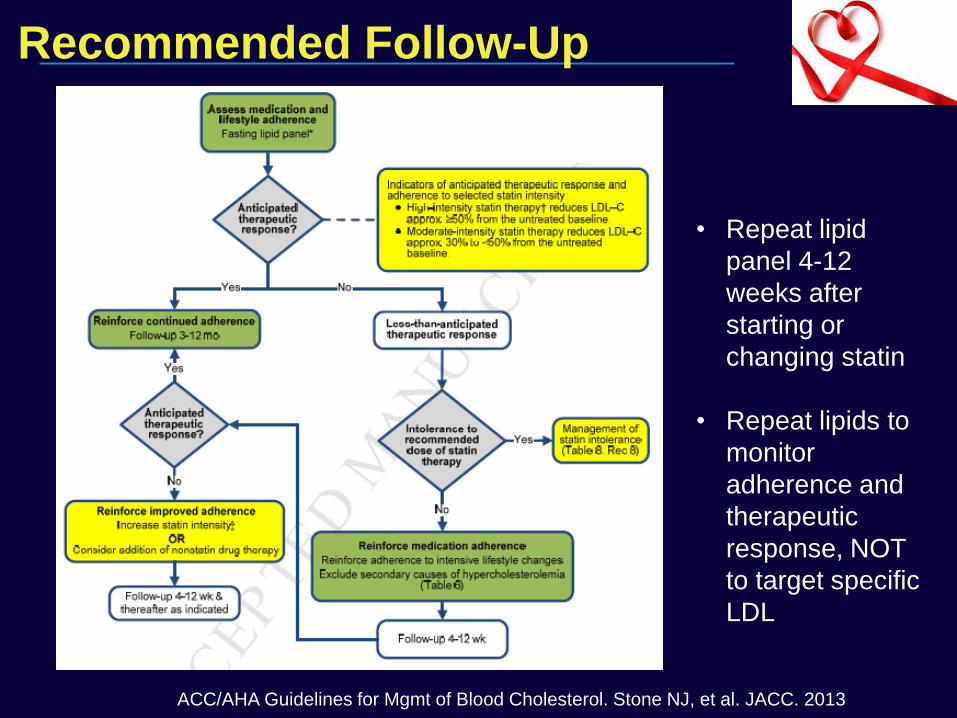
Recommended Follow-Up
ACC/AHA Guidelines for Mgmt of Blood Cholesterol. Stone NJ, et al. JACC. 2013
• Repeat lipid
panel 4-12
weeks after
starting or
changing statin
• Repeat lipids to
monitor
adherence and
therapeutic
response, NOT
to target specific
LDL
Do these guidelines apply to HIV
patients?
“Clinician judgment is especially important for several patient groups for whom the RCT evidence is insufficient for guiding clinical recommendations. These patient groups
include … those with serious comorbidities and increased ASCVD risk (e.g., individuals
with HIV, etc.)”
ACC/AHA Guidelines for Mgmt of Blood Cholesterol. Stone NJ, et al. JACC. 2013
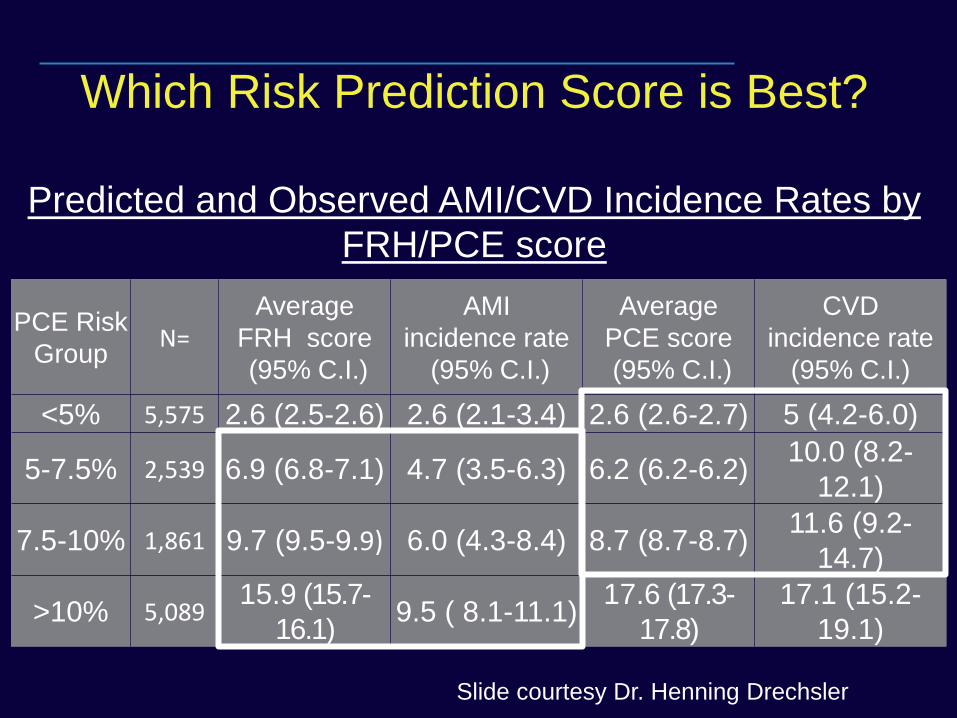
PCE Risk
Group N=
Average
FRH score
(95% C.I.)
AMI
incidence rate
(95% C.I.)
Average
PCE score
(95% C.I.)
CVD
incidence rate
(95% C.I.)
<5% 5,575 2.6 (2.5-2.6) 2.6 (2.1-3.4) 2.6 (2.6-2.7) 5 (4.2-6.0)
5-7.5% 2,539 6.9 (6.8-7.1) 4.7 (3.5-6.3) 6.2 (6.2-6.2) 10.0 (8.2-
12.1)
7.5-10% 1,861 9.7 (9.5-9.9) 6.0 (4.3-8.4) 8.7 (8.7-8.7) 11.6 (9.2-
14.7)
>10% 5,089 15.9 (15.7-
16.1) 9.5 ( 8.1-11.1)
17.6 (17.3-
17.8) 17.1 (15.2-
19.1)
Which Risk Prediction Score is Best?
Predicted and Observed AMI/CVD Incidence Rates by
FRH/PCE score
Slide courtesy Dr. Henning Drechsler
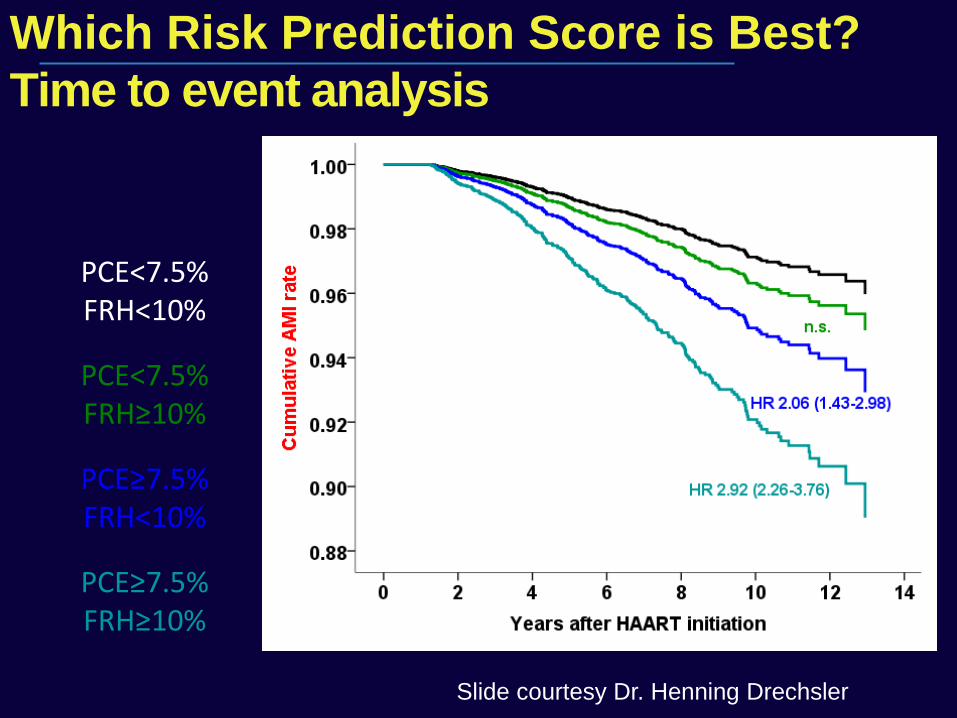
patients CVD
events AMI
events
PCE<7.5% FRH<10%
7,383 263 122
PCE<7.5% FRH≥10%
731 27 13
PCE≥7.5% FRH<10%
1,511 95 48
PCE≥7.5% FRH≥10%
5,439 416 219
Which Risk Prediction Score is Best?
Time to event analysis
Slide courtesy Dr. Henning Drechsler
Statin Therapy in HIV:
Other Benefits?
ALLRT cohort (3601 subjects) evaluated statin use and non-accidental death or non-AIDS defining complications1
– Adjusted HR for death 0.81 [.53-1.24], for non-AIDS malignancy 0.43 [.19-.94]
Hopkins cohort of 1538 virologically-suppressed pts2
– HR for death of 0.33 [0.14-0.76] associated with statin use in multivariate analysis controlling for demographic and clinical factors
VA HIV cohort from 1995-2009 including > 25k patients and 6435 deaths3
– Significant reduction in all-cause mortality per year of cumulative statin exposure
– Any statin: HR 0.95 [0.93-0.98]; Potent statin: HR 0.86 [0.81-0.93]
1. Overton ET, et al. CID 2013; 56:1471-1479; 2. Moore RD, et al. PLoS One 2011;
3. Drechsler H, et al. CROI 2013 Abstract 765.
Carr A, et al. AIDS. 2001;15:1811-1822. Moyle G, et al. AIDS. 2001;15:1503-1508. Miller J, et al. AIDS. 2002;16:2195-2200.
Doser N, et al. AIDS. 2002;16:1982-1983. Aberg JA, et al. AIDS Res Hum Retroviruses. 2005;21:757-767. Calza L, et al.
AIDS. 2005;19:1051-1058.
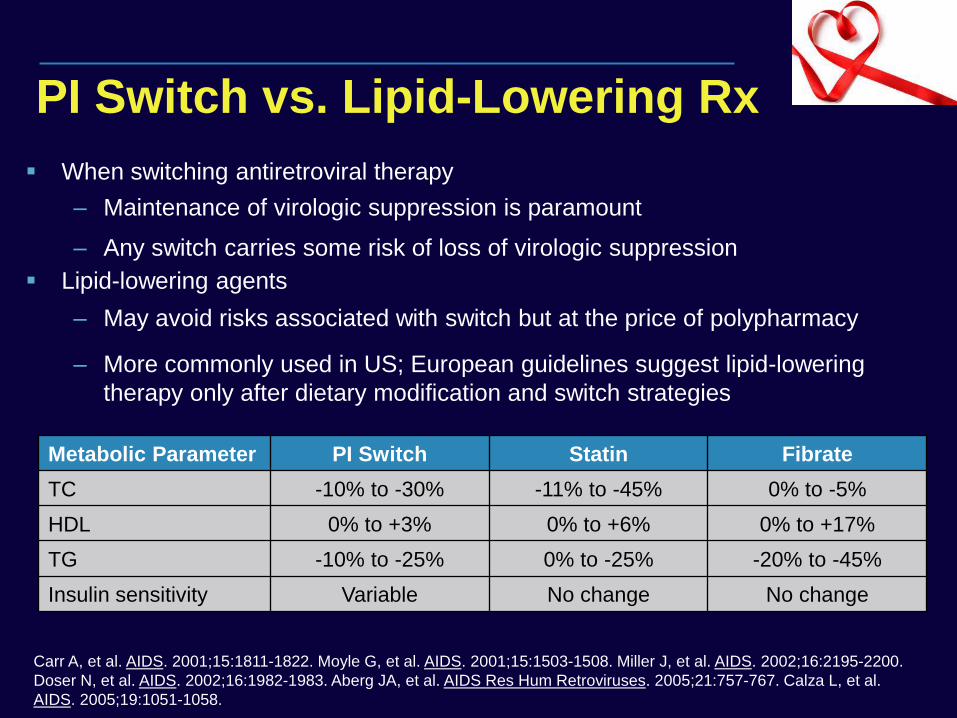
PI Switch vs. Lipid-Lowering Rx
Metabolic Parameter PI Switch Statin Fibrate
TC -10% to -30% -11% to -45% 0% to -5%
HDL 0% to +3% 0% to +6% 0% to +17%
TG -10% to -25% 0% to -25% -20% to -45%
Insulin sensitivity Variable No change No change
When switching antiretroviral therapy
– Maintenance of virologic suppression is paramount
– Any switch carries some risk of loss of virologic suppression
Lipid-lowering agents
– May avoid risks associated with switch but at the price of polypharmacy
– More commonly used in US; European guidelines suggest lipid-lowering
therapy only after dietary modification and switch strategies
Cholesterol Conclusions (Tentative)
Follow guidelines for pts with clinical ASCVD, LDL > 190 mg/dL, and diabetics
Consider “individualized” risk/benefit ratio of statin Rx in others (with predicted 10-year ASCVD risk as only one component)
Start lower dose statin and slowly titrate to achieve % LDL reduction goals (rather than a specific LDL)
Reserve non-statin therapy for statin intolerance or ↑↑ triglycerides
Consider more “lipid-friendly” ART if viral suppression possible
Need validation of risk calculators in HIV patients and RCT data on statins in HIV patients w/o clinical ASCVD (REPRIEVE trial)
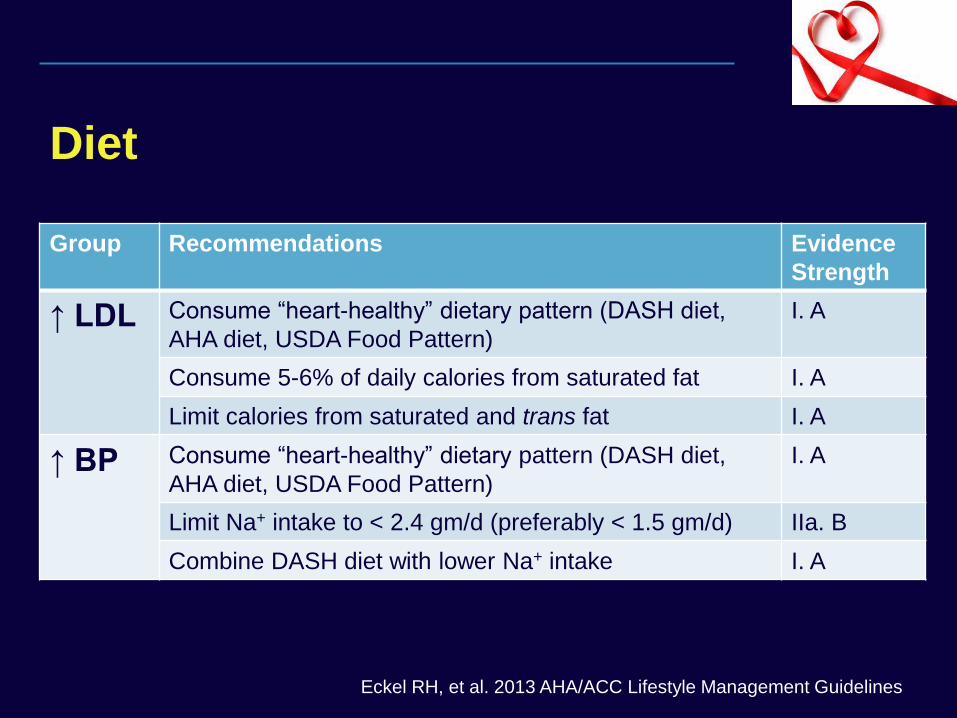
Diet
Group Recommendations Evidence
Strength
↑ LDL Consume “heart-healthy” dietary pattern (DASH diet,
AHA diet, USDA Food Pattern)
I. A
Consume 5-6% of daily calories from saturated fat I. A
Limit calories from saturated and trans fat I. A
↑ BP
Consume “heart-healthy” dietary pattern (DASH diet,
AHA diet, USDA Food Pattern)
I. A
Limit Na+ intake to < 2.4 gm/d (preferably < 1.5 gm/d) IIa. B
Combine DASH diet with lower Na+ intake I. A
Eckel RH, et al. 2013 AHA/ACC Lifestyle Management Guidelines
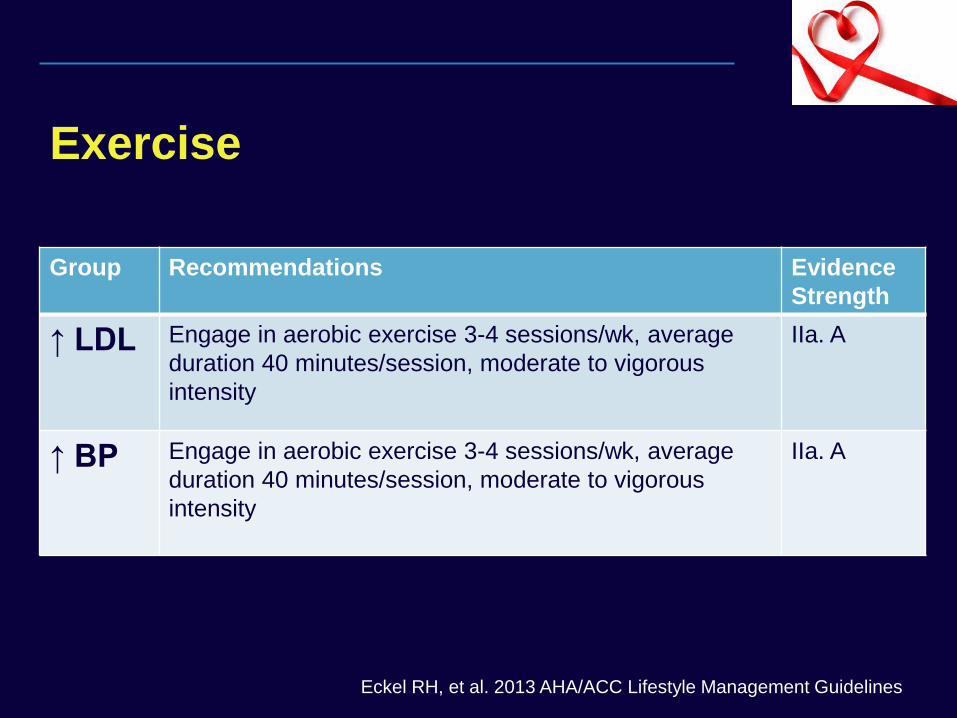
Exercise
Group Recommendations Evidence
Strength
↑ LDL Engage in aerobic exercise 3-4 sessions/wk, average
duration 40 minutes/session, moderate to vigorous
intensity
IIa. A
↑ BP
Engage in aerobic exercise 3-4 sessions/wk, average
duration 40 minutes/session, moderate to vigorous
intensity
IIa. A
Eckel RH, et al. 2013 AHA/ACC Lifestyle Management Guidelines
SMOKING CESSATION
Smoking cessation has GREATEST impact (≈ 50%) on CVD risk reduction of any single intervention
DHHS guidelines recommend pharmacotherapy for all patients except those with medical contraindications
– Approved agents: Nicotine patch, gum, inhaler, nasal spray, bupropion and varenicline
– No drug interactions with varenicline; caution with bupropion and boosted PIs
More intensive counseling interventions with better results in HIV+ patients, particularly when initiated by MD
Vidrine DJ, et al. AIDS. 2006; 20:253.
Insulin Resistance / Diabetes
Definitions of Diabetes: 2013 ADA Guidelines
– HbA1c ≥ 6.5%* or
– Fasting plasma glucose (FPG) ≥ 126 mg/dL* or
– Plasma glucose ≥ 200 mg/dL after 2 hrs during OGTT* or
– Random plasma glucose ≥ 200 mg/dL with symptoms
* Should be confirmed on repeat testing
Screening Frequency:
– Prior to and 1-3 months after starting HAART
– FPG or HbA1c in all patients every 6-12 months
Aberg J, et al. CID 2014; 38(1):1-34.
clinicaloptions.com/hiv
The Challenges of Managing the Aging HIV-Infected Patient
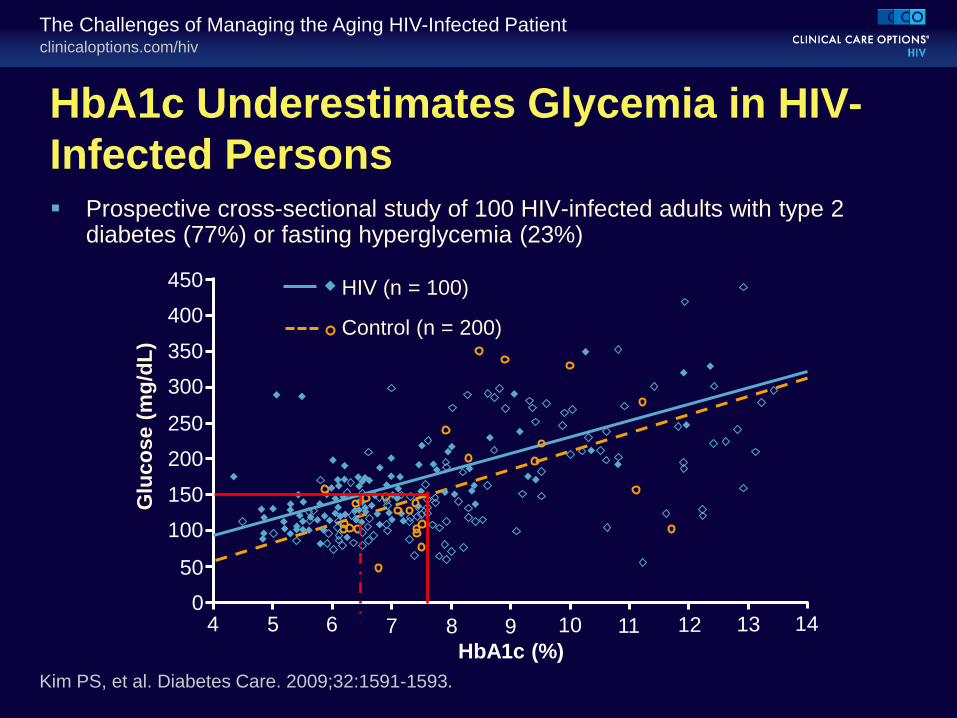
HbA1c Underestimates Glycemia in HIV-
Infected Persons
HIV (n = 100)
Control (n = 200)
Glu
co
se (
mg
/dL
)
Kim PS, et al. Diabetes Care. 2009;32:1591-1593.
450
400
350
300
250
200
150
100
50
0 4 5 6 7 8 9 10 11 12 13 14
HbA1c (%)
Prospective cross-sectional study of 100 HIV-infected adults with type 2 diabetes (77%) or fasting hyperglycemia (23%)
clinicaloptions.com/hiv
The Challenges of Managing the Aging HIV-Infected Patient
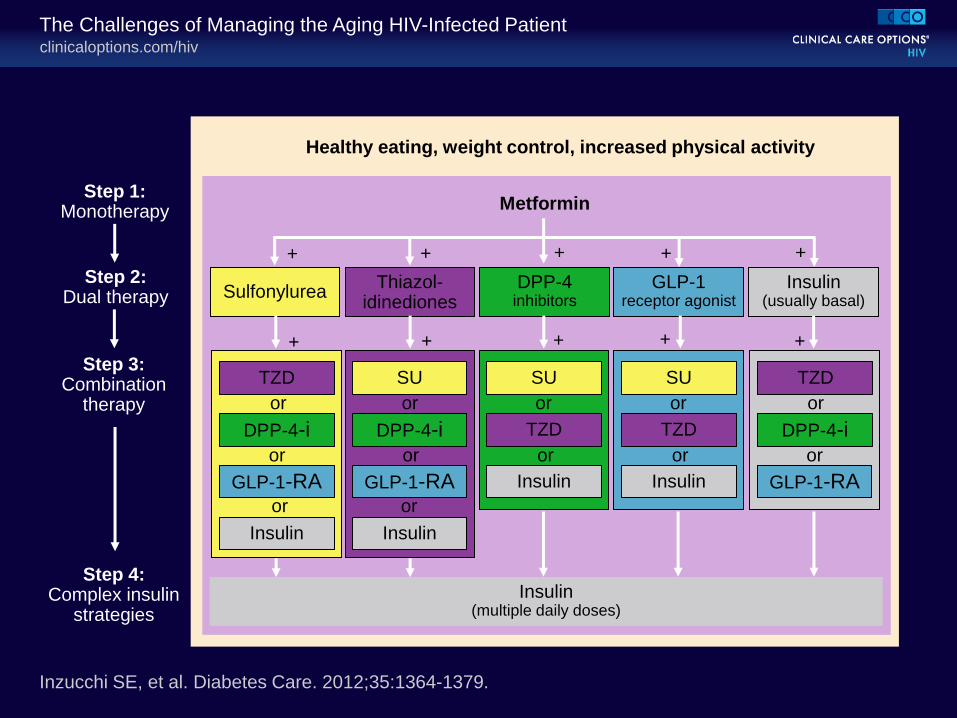
Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379.
Step 1: Monotherapy
Step 2: Dual therapy
Step 3: Combination
therapy
Step 4: Complex insulin
strategies
Insulin (multiple daily doses)
Insulin (usually basal)
GLP-1 receptor agonist
DPP-4 inhibitors
Thiazol- idinediones
Sulfonylurea
Healthy eating, weight control, increased physical activity
Metformin
TZD
TZD TZD
TZD
DPP-4-i DPP-4-i DPP-4-i
GLP-1-RA GLP-1-RA GLP-1-RA
Insulin Insulin
Insulin Insulin
SU SU SU
+ + + + +
+ + + + +
or
or
or
or
or
or
or
or
or
or
or
or
clinicaloptions.com/hiv
The Challenges of Managing the Aging HIV-Infected Patient
HbA1c Goal for the Prevention of Diabetes
Complications
< 7% Individualization is key:
Tighter control (HbA1c 6.0% to 6.5%): younger, healthier
Looser control (HbA1c 7.5% to 8.0%+): older, hypoglycemia prone, comorbidities
Should HbA1c goal be lower in HIV-positive patient if it underestimates glycemia?
Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379.
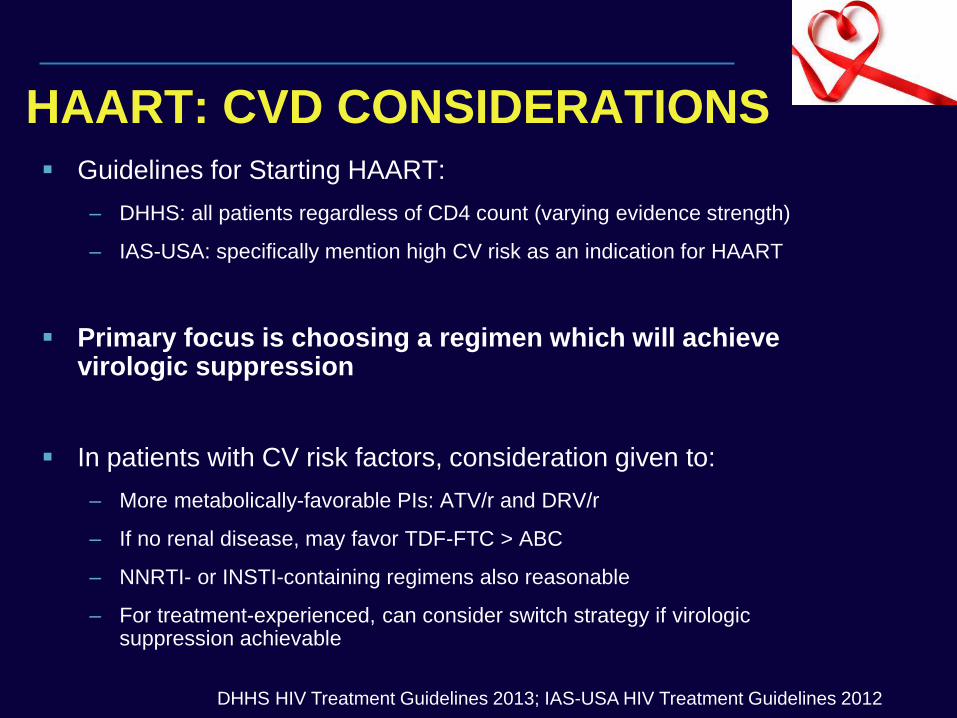
HAART: CVD CONSIDERATIONS Guidelines for Starting HAART:
– DHHS: all patients regardless of CD4 count (varying evidence strength)
– IAS-USA: specifically mention high CV risk as an indication for HAART
Primary focus is choosing a regimen which will achieve virologic suppression
In patients with CV risk factors, consideration given to:
– More metabolically-favorable PIs: ATV/r and DRV/r
– If no renal disease, may favor TDF-FTC > ABC
– NNRTI- or INSTI-containing regimens also reasonable
– For treatment-experienced, can consider switch strategy if virologic suppression achievable
DHHS HIV Treatment Guidelines 2013; IAS-USA HIV Treatment Guidelines 2012
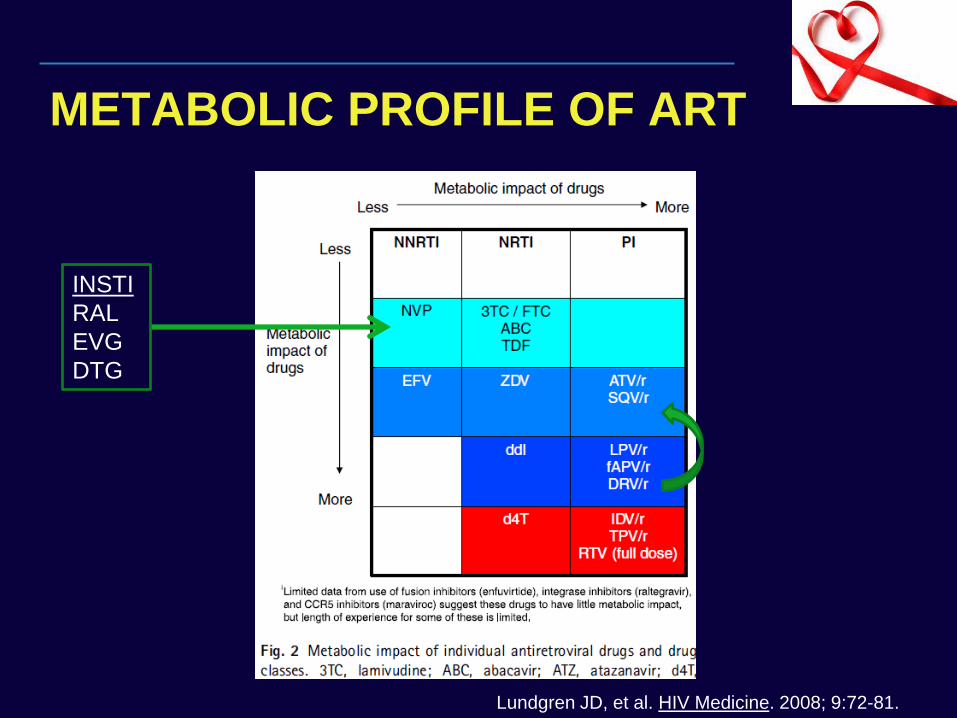
METABOLIC PROFILE OF ART
Lundgren JD, et al. HIV Medicine. 2008; 9:72-81.
INSTI
RAL
EVG
DTG
Conclusions
CVD is prevalent among HIV patients with significant morbidity and mortality
Pathogenesis of CVD in HIV is multifactorial including chronic inflammation/immune activation and abnormal lipid metabolism
Consistent delivery of CVD prevention strategies require a systematic, multi-disciplinary approach
Applicability of CVD guideline changes to HIV patients is unclear
Improved CV risk prediction and validated guidelines specific for HIV patients are urgently needed
The End
Mortality Trends in HIV
Introduction of HAART in 1996 led to dramatic reductions in AIDS-related morbidity and mortality1
Non-AIDS related causes of morbidity and mortality of increasing importance, with 3 dominant players2
– Cardiovascular Disease (CVD)
– Chronic liver disease, primarily from viral hepatitis
– Non-AIDS defining malignancies
1. Pallela FJ, et al. N Engl J Med. 1998; 338:853.
2. Neuhaus J, et al. AIDS. 2010; 24:697.
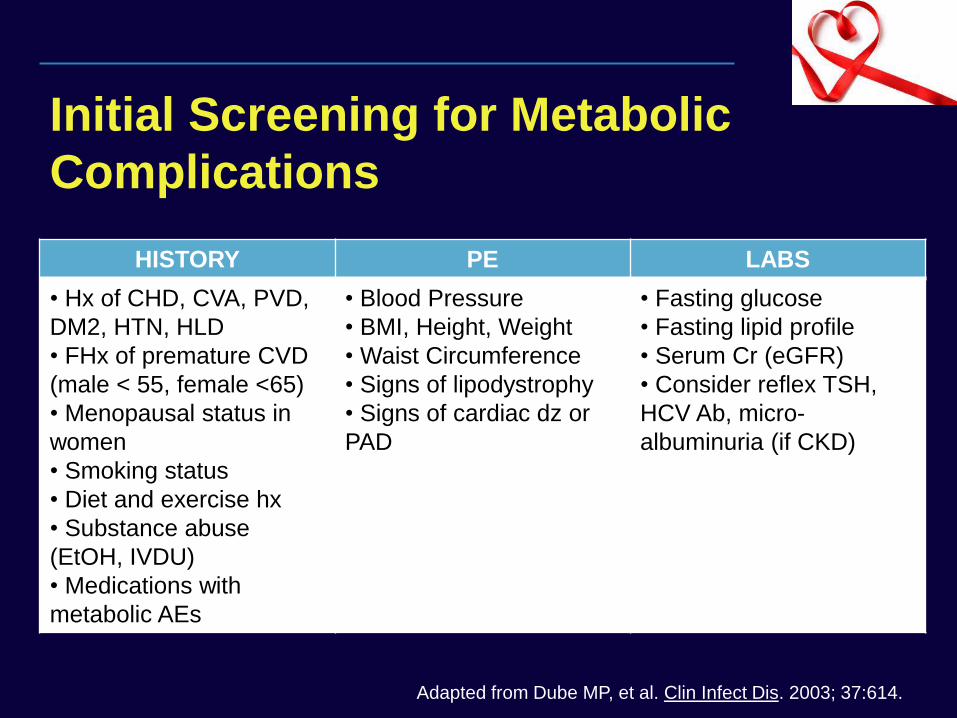
Initial Screening for Metabolic
Complications
HISTORY PE LABS
• Hx of CHD, CVA, PVD,
DM2, HTN, HLD
• FHx of premature CVD
(male < 55, female <65)
• Menopausal status in
women
• Smoking status
• Diet and exercise hx
• Substance abuse
(EtOH, IVDU)
• Medications with
metabolic AEs
• Blood Pressure
• BMI, Height, Weight
• Waist Circumference
• Signs of lipodystrophy
• Signs of cardiac dz or
PAD
• Fasting glucose
• Fasting lipid profile
• Serum Cr (eGFR)
• Consider reflex TSH,
HCV Ab, micro-
albuminuria (if CKD)
Adapted from Dube MP, et al. Clin Infect Dis. 2003; 37:614.
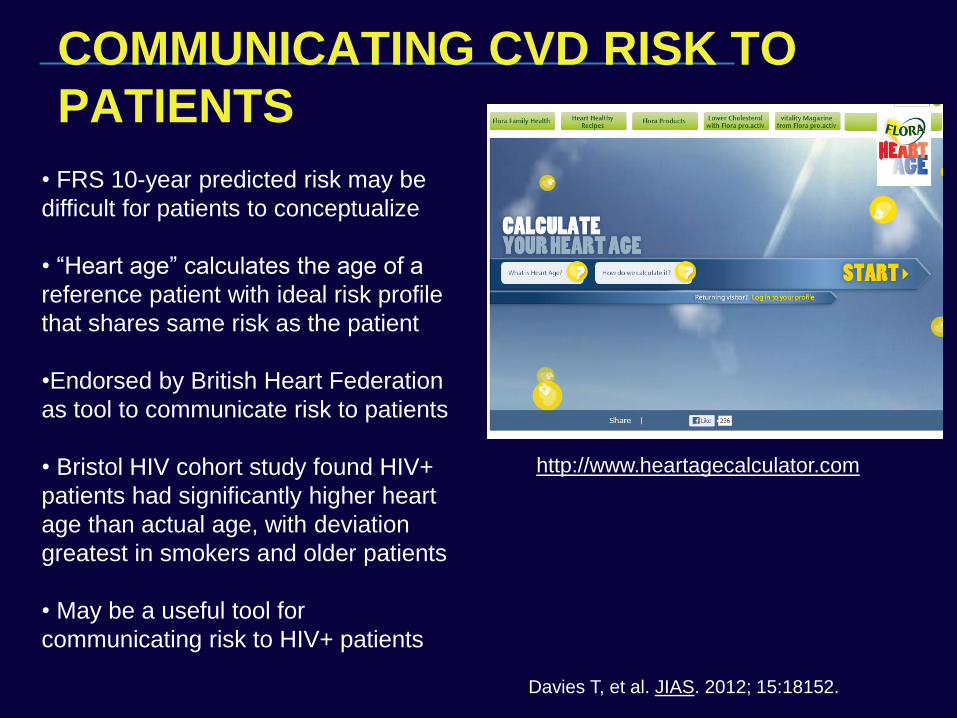
COMMUNICATING CVD RISK TO
PATIENTS
http://www.heartagecalculator.com
• FRS 10-year predicted risk may be
difficult for patients to conceptualize
• “Heart age” calculates the age of a
reference patient with ideal risk profile
that shares same risk as the patient
•Endorsed by British Heart Federation
as tool to communicate risk to patients
• Bristol HIV cohort study found HIV+
patients had significantly higher heart
age than actual age, with deviation
greatest in smokers and older patients
• May be a useful tool for
communicating risk to HIV+ patients
Davies T, et al. JIAS. 2012; 15:18152.
clinicaloptions.com/hiv
The Challenges of Managing the Aging HIV-Infected Patient
CV Risk Persists in Treated HIV Infection;
Inflammation Predictive of This Risk
ART-treated/virologically suppressed HIV-infected patients have greater carotid IMT vs controls[1,2]
– hsCRP strongly associated with IMT in bifurcation region[2]
HIV-infected patients with well-controlled disease have greater arterial inflammation (using FDG-PET)
– Associated with sCD163 but not CRP or D-dimer[3]
1. Hsue PY, et al. AIDS. 2009;23:1059-1067. 2. Hsue PY, et al. J Am Heart Assoc. 2012;1:pii: jah3-
e000422. 3. Subramanian S, et al. JAMA. 2012;308:379-386.
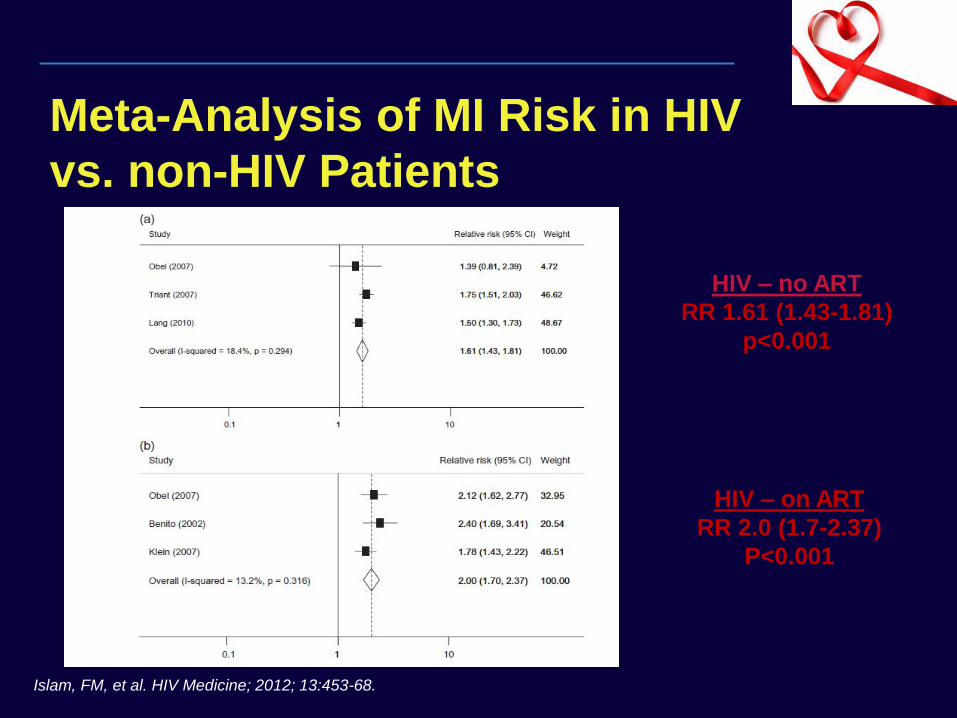
Meta-Analysis of MI Risk in HIV
vs. non-HIV Patients
HIV – no ART
RR 1.61 (1.43-1.81)
p<0.001
HIV – on ART
RR 2.0 (1.7-2.37)
P<0.001
Islam, FM, et al. HIV Medicine; 2012; 13:453-68.














![Cardiovascular disease [autosaved]](https://img.pdfslide.net/doc/110x75/554b2ab7b4c905d3088b4ab0/cardiovascular-disease-autosaved.jpg)













