Embed Size (px)
Citation preview

HIV Management 2011
John K. Midturi
April 16, 2011

Objectives
• Recognize HIV/AIDS prevalence rates in USA
• Recognize populations at highest risk for HIV infections
• Understand rationale for CDC recommendations on routine testing
• Be able to decide when to initiate HAART• Be able to select initial antiretroviral regimen

Epidemiology
• Reported 25 yrs ago
• Industrialized nations– Chronic manageable disease
• Developing world– Devastating effects on individuals, family
units, general community– High mortality and morbidity rates

Quarter-Year
Nu
mb
er
of
Case
s/D
eath
s
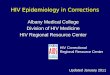
*Adjusted for reporting delays
1985198619871988198919901991199219931994199519961997199819990
5,000
10,000
15,000
20,000
25,0001993 definitionimplementationDeaths
Prevalence
AIDS
0
150,000
100,000
50,000
200,000
250,000
300,000
350,000
Estimated Incidence of AIDS, Deaths, and Prevalence by Quarter-Year of Diagnosis/Death,
United States, 1985-1999*
Pre
vale
nce


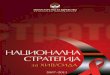
Estimated Rates for Adults and Adolescents Living With HIV Infection (not AIDS)34 States and 5 U.S. Dependent Areas, 2007
Estimated HIV Rateper 100,000
Confidential name-basedHIV infection reporting not implemented as of 2003
2.2 – 51.7
51.8 – 103.8
103.9 – 170.5
170.6 – 282.0Data classed using quartilesTotal rate: 154.2 per 100,000
Note: Rates have been adjusted for reporting delays. Inset maps not to scale. HIV/AIDS Surveillance Report, 2007. Vol 19, table 11.
U.S. Virgin Islands
AKHI
Puerto Rico
American Samoa
NorthernMarianaIslands
Guam
DC
6

7
Awareness of HIV Status in the US
1CDC. HIV prevalence estimate—United States, 2006. MMWR. 2008;57(39):1073-1076.2Hall HI, et al. Estimation of HIV incidence in the United States of America. JAMA. 2008;300:520-529.
3CDC. HIV/AIDS surveillance report—cases of HIV infection and AIDS in the United States and dependent areas, 2007;19.http://www.cdc.gov/hiv/topics/surveillance/resources/reports/2007report/default.htm. Accessed July 23, 2009.
HIV estimated prevalence1 1,056,400 - 1,156,400
Undiagnosed1 232,700
Estimated newannual infections (2006)2
56,300
• From 2004 to 2007, the estimated number of newly diagnosed HIV/AIDS cases increased 15%3

8
US Population Demographics: Total Population and HIV/AIDS Cases by Race/Ethnicity
White71%
Other4%
Black12%
Hispanic13%
Total US Population (2006)(N = 247.1 million)1
Campsmith M, Rhodes P, Hall HI. 16th CROI; 2009; Montreal. Abstract #1036.
Estimated HIV/AIDS Prevalence by Race/Ethnicity (2006)
(N = 1,106,400)2
Black46%
White35%
Hispanic/Latino18%
Other<2%

9
Estimated HIV/AIDS Prevalence and New Infections by Transmission Category in the US (2006)
MSM48%
High-Risk Heterosexual
Contact (Male)9%
IDU (Male)12%
MSM + IDU5%
High-Risk Heterosexual
Contact (Female)
18%
IDU (Female)
7%
Other1%
CDC. HIV Incidence. Available at http://www.cdc.gov/hiv/topics/surveillance/incidence.htm.
MSM53%
High-Risk Heterosexual
Contact31%
IDU12%
MSM + IDU4%
Estimated New HIV DiagnosesEstimated Prevalence of HIV/AIDS



A global view of HIV infection33 million people [30–36 million] living with HIV, 2007

Pathophysiology and Natural History
• Family of Retroviruses– Subfamilies– Oncoviruses– Lentiviruses- slow viruses
• HIV- long replication periods prior to clinical manifestations
– Spumaviruses- not associated with human disease

• HIV genome consists of three structural genes
• gag- codes for viral capsid proteins, p15, p17, p24
• pol- codes for proteins responsible for viral replication, and reverse transciptase
• env- codes for envelope proteins gp120, gp41

Ontogeny of HIV• Simian immunodeficiency virus (SIV) is
evolutionarily adapted to its natural hosts, chimpanzees and sooty mangeby monkeys
• Inoculation of SIV into other primates typically produces an HIV-like disease
• SIV is the closest known relative of HIV-1 and 2• These findings suggest that the HIV pandemic
began with infection of humans by SIV variants• Phylogenetic analysis suggests that HIV became
established in humans early in the 20th century

HIV Types 1 and 2• Geographic distribution
• HIV-1: Global• HIV-2: West Africa
• Transmission• Identical for the two virus types
• Pathogenicity• HIV-2 appears to be less pathogenic
than HIV-1

HIV-1 Classification System
• Group M (main)• Subtypes (clades) A to D, F, G, H to K• Recombinant forms
• Group O (outlier)
• Group N (non-M/non-O)

Subtype, circulating recombinant forms

HIV-1 Subtypes: Implications for Diagnosis and Treatment
• Several studies suggest differential rates of HIV disease progression and transmission by subtype
• There may be differential rates of emergence of resistance to ARVs by subtype

Transmission
• Probability of infection– Blood transfusion/ transplant
95%-100%– MTCT with ART: ~25%– Needle Sharing: 1/150,
~0.6%– Occupational needle stick,
1/300, ~0.3%– Sexual contact (single event):
0.2%
Un.org
Medipulse.com
Brandonyeoh.com

HIV Life Cycle
Maturation2. Membrane
fusion & entry
9. Budding
3. Uncoating & reverse
transcription
4. Nuclearuptake 5. Integration
6. Transcription & RNA processing
7. Nuclearexport 8. Translation
& Assembly
1. Receptorbinding

Immunopathogenesis of HIV
• CD4+ cells are the principle targets of HIV in the host• Helper/inducer T-lymphocytes• Fetal thymocytes• Macrophages/monocytes• Dendritic cells• Microglia• Placental trophoblast cells

Clinical Presentation

Acute infection
• 40-90% of primary infections develop mononucleosis like syndrome– 2-6 weeks after exposure– Acute retroviral syndrome– Signs/symptoms
• Fever 96%, LAD 74%, Exudative pharyngitis 70%, myalgia's/arthralgia 54%, diarrhea 32%, headache 32%
– Duration of illness is <2weeks– Diagnosis
• HIV RNA viral load (high) and HIV antibody (+/-)

• Progressive loss of CD4 lymphocytes– 50-80 CD4 cells/uL
per year– Infection to
development of AIDS- 6-8years
– Dependent on viral load, CD4 count, age, socioeconomic status, host genetics
• Rapid progressor• Long term non-
progressors• Elite controllers
(viral load <48copies w/o therapy)
Chronic Infection

WHO HIV clinical stages

Definitions for AIDS
1993 Centers for Disease Control and Prevention Revised Surveillance Definitions of AIDS
A CD4+ T-cell count below 200 cells/μL or a CD4+ T-cell percentage of total lymphocytes of ≤ 14% and/or the following AIDS-defining infections:
Candidiasis of bronchi, trachea, or lungs
Esophageal Candida
Coccidioidomycosis, disseminated or extrapulmonary
Cryptococcosis, extrapulmonary
Cryptosporidiosis, chronic intestinal for > 1 mo
Cytomegalovirus disease (other than liver, spleen, or lymph nodes)
Encephalopathy (HIV-related)
Herpes simplex: chronic ulcer(s) for > 1 mo; or bronchitis, pneumonitis, or esophagitis
Histoplasmosis, disseminated or extrapulmonary
Isosporiasis chronic intestinal (for > 1 mo)
Mycobacterium avium complex
Mycobacterium, other species, disseminated or extrapulmonary
Pneumocystis jiroveci (formerly carinii) pneumonia
Pneumonia recurrent (> 1 recurrent episode in a 12-mo period)
Progressive multifocal leukoencephalopathy
Salmonella septicaemiae (recurrent)
Toxoplasmosis of the brain
Tuberculosis
Wasting syndrome due to HIV
And/or the following AIDS-defining malignancies:
Cervical cancer (invasive)
Lymphoma: Burkitt's, immunoblastic or primary brain
Kaposi's sarcoma
Wikimedia.com
Emedicine.com
www.brown.edu
www.bmj.com

Screening and Diagnosis
• CDC recommendations – 13-64 years of age– Routine HIV testing in all health care settings– Informed to opt out, no written consent required– Must screen for HIV
• TB treatment• STD treatment
– High risk behavior• IV drug users• Exchange sex for money• Sex partners of HIV infected person• Men who have sex with men• Heterosexual persons or partners with more than one partner since
last test
www.stdexpress.com

Routine HIV Testing: Who to Test
Which patients should be offered routine HIV testing? What guidelines and recommendations exist regarding routine HIV testing?Short answer: All individuals between the ages of 13 and 64 yrs should be routinely screened for HIV infection in healthcare settings.

CDC Recommendations for Routine HIV Testing
• Routine, voluntary HIV screening in healthcare settings recommended for all patients 13-64 yrs of age– Except in populations with documented prevalence of
undiagnosed HIV infection < 0.1%– Without prevalence data, voluntary HIV screening
appropriate until diagnostic yield < 1/1000 patients screened is established
• Separate written consent not recommended• Pre- or post-test prevention counseling should not be
required with testing or screening programs
Branson BM, et al. MMWR Recomm Rep. 2006;55:1-17.

USPSTF HIV Testing Recommendations
• Screening strongly recommended for all adolescents and adults at increased risk for HIV and all pregnant womenIncreased risk defined as individuals with ≥ 1 risk individual factor or
individuals receiving healthcare in a high-prevalence or high-risk clinical setting
Individual Risk Factors High-Prevalence or High-Risk Settings
Men who have had sex with men after 1975 Men and women having unprotected sex with multiple partners Past or present IDUsMen and women who exchange sex for money or drugs or have sex partners who doIndividuals whose past or present sex partners were HIV infected, bisexual, or IDUs Persons being treated for STDs Persons with a history of blood transfusion between 1978 and 1985Persons who request an HIV test despite reporting no individual risk factors may be considered at increased risk
STD clinics Correctional facilities Homeless shelters Tuberculosis clinicsClinics serving men who have sex with menAdolescent health clinics with a high prevalence of STDsAny clinical setting with a known HIV prevalence ≥ 1% among the patient population being served
USPSTF recommendations. July 2005.

Diagnosis
• Enzyme linked immunosorbent assay (ELISA) followed by confirmatory Western blot assay if ELISA positive
• ELISA 99% specific, 98.5% sensitive• Western blot 100% sensitive, and 100%
specific for chronically infected– Detects antibodies to HIV proteins– Core (p17, p24, p55)– Polymerase (p31, p51, p66)– Envelope (gp41, gp120, gp160)
Oraquick

Western Blot
• CDC criteria 1– p160, p120 AND p41
• CDC criteria 2– p160, p120 OR p41 PLUS p24
– Positive= reactive to gp120 and either gp41, p24
– Negative= non reactive– Indeterminate= presence of other band
pattern not positive
p160 p120 p41 p68 p53 p32 p55 p40 p24 p18G
AG
PO
L
EN
V

Diagnosis
• HIV antibodies appear in circulation 2-12 weeks after exposure
• Window period- serologic testing is negative– Repeat test in 6 weeks to 3 months
• Rapid serologic tests results in 20 minutes– Sensitivity and specificity 99%

Management
• H&P• Social support system• Reaction to HIV infection
– Anxiety, depression, adjustment disorders
• Lab– Baseline- assessment of liver, bone marrow,
and kidney function, lipids• Cd4, viral load, CBC with diff, LFTs, lipid, hep Bs
antigen and antibody, hep c antibody, Toxoplas IgG, cmv IgG, tst, rpr, pap smear, g6pd level, genotype

Preventative measures
• Routine immunizations
• Cervical cancer screening
• Medication for primary or secondary prophylaxis

Immunizations
• Pneumococcal vaccine– Every 5 years x 2 doses
• Hepatitis A and B• Give when CD4 above 200cell/uL• TST/T-Spot
– Annually– >5mm considered positive
• CXR and if no symptoms and CXR clear therapy for LTBI

Women & HIV
• Women– Increased incidence of cervical dysplasia and
invasive cervical carcinoma• More frequent Pap smear screenings• 2 Pap smears 6 months apart and then annually if
results are normal• Abnormality- colposcopy
– HSV- suppressive therapy indicated for frequent anogenital outbreaks
Kasheun.com

Care of Pregnant HIV-Infected Women
• The current recommendations focus on use of HAART by known HIV-infected pregnant women, regardless of maternal health needs– reduce the risk of mother-to-child
transmission
• Perinatal transmission rates—to less than 2%—in the United States.– Identifying HIV infection in pregnant women
with previously undiagnosed or newly acquired HIV infections
– Preventing HIV transmission to infants through the use of chemoprophylaxis antiretroviral therapy
– Avoiding breastfeedinghttp://www.hiv.gov.gy/ads/pstr_protectbaby.jpg



Antiretroviral Therapy During Pregnancy
• HAART should be initiated in all HIV-infected pregnant women regardless of CD4+ cell count or HIV-1 RNA level. – Antiretroviral resistance testing before initiating HAART– CBC & CMP testing before treatment initiation. – OI prophylaxis-based on current CD4+ cell count.
• HAART (2 NRTIs and either a PI with ritonavir boosting or a NNRTI) – Efficacy of antiretroviral therapy in preventing maternal to fetal
transmission is primarily through lowering plasma HIV-1 RNA.
• Transmission can occur at any plasma HIV-1 RNA level, including undetectable plasma HIV-1 RNA– All HIV-infected pregnant women should be offered HAART.

Viral Load and Transmission
00
16.616.6
21.321.3
30.930.9
40.640.6
HIV-1 RNAHIV-1 RNA Transmission %Transmission %
<1000 copies/mL<1000 copies/mL
1000 - 10,0001000 - 10,000
10,001- 50,00010,001- 50,000
50,001-100,00050,001-100,000
>100,000>100,000
NN
0/570/57
32/19332/193
39/18339/183
17/5417/54
26/6426/64
Women & Infants Transmission Study (WITS) Garcia, et al, NEJM 1999

Mode of Delivery • HIV-1 RNA remains > 1000 copies/mL- caesarian section
– Scheduled for 38-39 weeks gestation• Intravenous zidovudine infusion initiated 4 hours before the caesarian delivery
(2 mg/kg over 1-hour loading dose, then 1 mg/kg/hour continuous infusion until delivery, ie, umbilical cord ligated)
– Caesarian section delivery probably confers little added benefit in women with plasma HIV-1 RNA < 1000 copies/mL (Management Guidelines).[DHHS Perinatal]
• HIV-1 RNA is < 1000 copies/mL, a vaginal delivery – Induction of labor at 38-39 weeks. – Invasive fetal monitoring or operative delivery with vacuum devices or forceps
should be avoided in HIV-infected women• increase risk of transmission.[Mofenson 1999; Shapiro 1999]
– Artificial or prolonged rupture of membranes should be avoided• caesarian delivery if labor does not progress 4 hours after membranes have
ruptured– Intravenous infusion with zidovudine should be initiated at the onset of labor
• Intravenous zidovudine (2 mg/kg over 1-hour loading dose, then 1 mg/kg/hour continuous infusion until delivery, ie, umbilical cord ligated)

Prophylaxis
• CD4 cell count is an indicator of immune competence– CD4 <200, CD4% <14%, recurrent
candidiasis, persistent fever, previous PCP: Pneumocystis jirovecii pneumonia
• TMP/SMX• Dapsone• Atovaquone• Pentamidine (aerosolized)

Prophylaxis
• CD4 <100 and positive IgG Toxo titer:– Toxoplasmosis:
• TMP/SMX• Dapsone• Pyrimethamine• Leucovorin
• CD4 <50– MAC
• Azithromycin• Clarithromycin• Rifabutin

Discontinuation of Prophylaxis
• Discontinue primary and secondary prophylaxis for certain OI if sustained rise in CD4 cell count above threshold for prophylaxis initiation
• PJP (>200)• Toxoplasmosis (>100)• MAC (>50)• Secondary prophylaxis
– Cytomegalovirus (>150)
• Re-initiate prophylaxis if CD4 decreased below threshold

Treatment
• Goal: – prolong life– avoid destruction of immune system– allow reconstitution of immune system– prevent OI– provide improved quality of life by reduction HIV-related
symptoms
• Effective therapy: <50copies/ml– Improve prognosis, minimize the development of
resistance, and prolong duration of antiretroviral response
www.abc.net.au



Antiretroviral Agents - 1
• Nucleoside / nucleotide analogues (NRTIs)Abacavir C – No studies. Concern for
hypersensitivityDidanosine B – Concern for lactic acidosis (do not use
w/ d4T)Emtricitabine B – No studies.Lamivudine C – Well tolerated. Widely used.Stavudine C – Concern for lactic acidosis (do not use
w/ ddI)Tenofovir B – No studies. Animal reports of bone
abnlsZalcitabine C – No studies. Teratogenic in animals.Zidovudine C – Well tolerated. The most experience.

Antiretroviral Agents - 2
• Non-nucleoside RT inhibitors (NNRTIs)Delavirdine C – No studies.Efavirenz D – Teratogenic. 4/142 birth
defects. Avoid in 1st trimesterNevirapine C – Well tolerated. Avoid initiating if CD4
>250 cells/mm3.

Antiretroviral Agents - 3
• Protease inhibitors (PIs)Amprenavir C – No studies. Oral solution contraindicated.Atazanvir B – No studies. Concern hyperbilirubinemiaFosamprenavir C – No studiesIndinavir C – Unboosted: poor blood levels in pregLopinavir/ritonavirC – No studiesNelfinavir B – Registry data shows no incr in birth defRitonavir B –Not used alone due to GI side effectsSaquinavir B – Well tolerated, used boostedTripanavir C – No studies

Antiretroviral Agents- 4
• Integrase Inhibitors (INSTI)– Raltegravir C-No studies

Antiretroviral Agents- 5
• Entry Inhibitors– Maraviroc B- No studies, requires Tropism
test– Enfuvirtide B- No studies, subcut injection

0
200
400
600
800
1,000
1,200
1,400
HIV Infected Diagnosed In Care On ART
Pa
tie
nts
in
00
0s
1,056 – 1,156
835 – 915
560
~79%
~83%675~75%
Sources:* February, 2009 CDC estimates as of the end of 2006** Synovate Healthcare U.S. HIV Monitor Q3 2008
Significant Numbers of People with HIVin the US Are Not on Antiretroviral Therapy

FACTOR RECOMMENDATION FOR TREATMENT
AIDS Treat Treat Treat Treat Treat
CD4 <500
• Treat <200
• Offer <350
• Indiv. >350
•Treat <350
• Risks/ Benefits if >350
Viral Load >20,000 >55,000 > 100,000No specific viral
load
Other Factors
• Pregnant women
• HBV co-infected
• HIVAN DHHS Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents, 1998 – 2008.
When to Treat: History of DHHS Recommendations
1998 2001 2002 2004 2008

Recommendations for Initiation of Therapy in Antiretroviral Naïve HIV-infected PatientsCondition Recommendation
In presence of
• AIDS-defining illness
• Pregnancy
• HIV-associated nephropathy
• HBV co-infection when HBV therapy is indicated
and/or
• CD4 count <350 cells/mm3
Start ART
CD4 count
350-500 cells/mm3
ART is recommended
• 55% of Panel members strongly recommended starting ART
• 45% moderately recommended starting ART
CD4 count
>500 cells/mm3
ART is recommended or optional
• 50% recommended starting ART
• 50% viewed starting ART as optional
DHHS 2009 Guidelines
DHHS Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. December 1, 2009. Available at: http://www.aidsinfo.nih.gov.

Recommendations for Initiation of Therapy in Antiretroviral Naïve HIV-infected Patients
• Patients initiating antiretroviral therapy should be willing and able to commit to lifelong treatment and should understand the benefits and risks of therapy and the importance of adherence
• Patients may choose to postpone therapy, and providers may elect to defer therapy, based on clinical and/or psychosocial factors on a case-by-case basis
DHHS 2009 Guidelines
DHHS Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. December 1, 2009. Available at: http://www.aidsinfo.nih.gov.

60
Recommendations for Earlier ART Initiation: Summary of Benefits and Limitations
Benefits Potential Limitations• Reduction in mortality and/or AIDS-
associated morbidity
• Improved outcomes in patients with certain co-morbidities, including HIVAN and HIV/HBV co-infection
• Potential to reduce risk of endothelial dysfunction and cardiovascular disease
• Reduced risk of AIDS-defining and non-AIDS-defining malignancies
• More robust immunologic response when treatment is initiated at a younger age
• Prevention of HIV transmission
• Fewer long-term safety data on newer ARVs
• Concerns for some unknown adverse consequences / complications of lifelong ART
• Potential for reduced quality of life associated with side effects in some patients, particularly those who are asymptomatic at the time of ART initiation
• Earlier emergent drug resistance, particularly in nonadherent patients, resulting in loss of drugs and drug classes and transmission of drug-resistant HIV
• Annual cost of medication
DHHS 2009 Guidelines
DHHS Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. December 1, 2009. Available at: http://www.aidsinfo.nih.gov.

0
15
30
45
60
75
90
105
120
135
150
Med
ian
CD
4 In
crea
se
97
119 120 121127 125
150Median CD4 increase
Treatment Responses in 1st Year of HAARTImproving Over Time
• 4143 subjects from 5 clinic cohorts in Europe and Canada• Treatment-naive; started HAART from 1996-2002 risk of virologic failure, med. CD4 count increase in later years
– Most “failure” now due to loss to follow-up or treatment discontinuation
Lampe F, et al. CROI 2005. Abstract 593
24.8 23.017.3
12.4 10 8 8.4
0
10
20
30
40
50
1996 1997 1998 1999 2000 2001 2002
% with VL > 500 c/mL
60
70
80
90
100
% W
ith
VL
>50
0 o
n A
RT

Magnitude of increase in CD4 cell count greatest if therapy started at low CD4 cell counts, but greater likelihood of CD4 cell
count normalization with earlier therapyKeruly J, et al. Clin Infect Dis. 2007;44(3):441-446. Gras L, et al. J Acquir Immune Defic Syndr. 2007;45(2):183-192.
Likelihood of Achieving a Normal CD4 Cell Count Dependent on CD4 at Initiation of
Therapy
1000
800
600
400
200
00 48 96 144 192 240 288 336
ATHENA National Cohort
Weeks from Starting ART
>500350-500200-35050-200<50
Years on ART
Johns Hopkins HIV Clinical Cohort
Mea
n C
D4
Cel
l C
ou
nt
(cel
ls/m
m3)
2 3 4 6
200
400
600
800
0
1000
>350200-350<200
510


Initial Treatment: Preferred
NNRTI based •EFV/TDF/FTC1,2
PI based •ATV/r + TDF/FTC²•DRV/r (QD) + TDF/FTC²
II based •RAL + TDF/FTC²
Pregnant Women •LPV/r (BID)³ + ZDV/3TC
1. EFV should not be used during the first trimester of pregnancy or in women trying to conceive or not using effective and consistent contraception. 2. 3TC can be used in place of FTC and vice versa.

Initial Treatment: AlternativesNNRTI based •EFV¹ + (ABC/3TC) or (ZDV/3TC)²
•NVP4 + ZDV/3TC
PI based •ATV/r + (ABC/3TC) or (ZDV/3TC)2,3
•FPV/r (QD or BID) + (ABC/3TC) or (ZDV/3TC) or (TDF/FTC)2,3
•LPV/r (QD or BID) + (ABC/3TC) or (ZDV/3TC) or (TDF/FTC)2,3
•SQV/r + TDF/FTC2
1. EFV should not be used during the first trimester of pregnancy or in women trying to conceive or not using effective and consistent contraception. 2. 3TC can be used in place of FTC and vice versa.3. ABC should not be used in patients who test positive for HLA B*5701; caution if HIV RNA >100,000 copies/mL, or if high risk of cardiovascular disease.4. NVP should not be started if pre-ARV CD4 >250 in women or >400 in men.

ARVs Not Recommended inInitial Treatment
High rate of early virologic failure
• ddI + TDF
Inferior virologic efficacy
• ABC + 3TC + ZDV as 3-NRTI regimen• ABC + 3TC + ZDV + TDF as 4-NRTI regimen• DLV• NFV• SQV as sole PI (unboosted)• TPV/r
High incidence of toxicities
• d4T + 3TC• IDV/r• RTV as sole PI

Questions

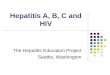
HIV Entry Is Triggered by Receptor Engagement
Attachmentto CD4+ cell
Triggered by coreceptor
Membranefusion
1 2 3
Maraviroc Enfuvirtide
Licensed entry inhibitors

Co-receptor antagonists
• Block major entry step by binding to chemokine receptors (CCR5 or CXC4)

What Are Viral Coreceptors?
• There are 2 viral coreceptors that matter– CCR5 and CXCR4– Both are chemokine
receptors• Most viruses can use only
CCR5: R5 viruses• Many can use both
coreceptors: R5/X4 (D/M)• A few can use only CXCR4: X4
viruses
352
C
LAD
TF
F
H
LL
S
PL
A
F
NY
I
VL
W
L
LF
I
G
FG
F
L
IL
I
LI
L
F
IT
F
YG
T
S
STV
LI
F
T
IT
V
GS
F
V
VV
W
PA
I
A
GCM
VL
L
I
YI
V
GL
V
L
SL
I
LP
I
V
TI
L
F
YV
W
L
MF
Y
IP
L
F
II
V
NA
L
LMV
I
F
YP
V
GL
G
L
S
L
F
NV
F
I
L
L
I
LIN
IN
F
C
TV
M
A
PY
C
V
TL
M
T
IA
I
G
EG
Q
H
EID
L
KR M
T
K S
Y
TMCQ
NF G
RYLAVV
A F A K ARTVTF
VG
HV L
SQK
EGLHY
TCS
YS Q Y Q F
WKNFQ
H
PF
S
KTLL
V
HR
KKENRCR
NTFQEFFGL N N C
SSSNR
DQ
L
CK
K
FFR N
YL L
V
HIAKRF
F
QK
ACC S I
F Q Q
SVYTRST
G
E
PE
RASEQE
AA
AQ
AAI
QKVNI K Q C
PES
TYYNIDYIPSS V Q Y D M - NH2
- COOH
R31-
-57 67-
-89 102-
-125 146-
-168 -197
219- -235
-258
303-
TL
RA
I S V G L
R
PL
D
K
R
277-
Acidic
Basic
CCR5 = CXCR4
CCR5DW
CCR5
Q
LSD
TF
F
LR
A
PI
A
L
HY
V
LV
W
L
FI
L
S
TV
L
A
LI
V
IV
V
Y
AS
L
YN
H
S
YVP
IF
L
A
GV
I
DT
F
L
VV
W
PL
I
A
ICI
IV
G
H
YI
L
GL
I
I
CI
S
LP
M
V
IL
T
F
YG
W
I
IV
F
IP
S
C
LT
A
YL
I
AGV
I
T
YP
I
I
GL
G
L
TS
F
F
NV
I
V
II
L
L
M G Y
LN
F
C
AI
F
W
PY
C
L
TL
I
F
IA
L
G
GA
S
H
AKD
L
KK M
T
R S
D
FLCK
NY F G
DRYLAIV
N S R PRKLLA
KE
H T Q
VSE
ADDRYI
CD
N D L W VVVFQFQ
FP
Y
R
SKLS
KLAKRKQHGKS
H
DSFILLEII K Q G C E
FENT
HK
V
LK
K
LFK T
S AQ H
VSRGSS
A
TS
GIL S K
G K R
TESESSS
F
GHSSVSH
S S
VA
ANW
KNF
NANE E R F C
PEKM
SDYD
GSGMEETYND S
T Y I S I G E M - NH2
Ser/Thr rich
*
*
*
N
Cytoplasmic
39-
-65 75-
-97 110-
-133 154-
-176 -202
224- -239
-262-282
308-
-352
F
CXCR-4
A
= Predicted G-protein binding domains
CXCR4

Summary: Appropriate Use of CCR5 Antagonists
• CCR5 inhibitors beneficial when used in treatment-experienced patients with no detectable D/M or X4 virus at BL
• In antiretroviral-naive patients with R5-only virus, CCR5 antagonist plus 2 NRTIs showed substantial activity, though not noninferior vs efavirenz plus 2 NRTIs
• Phenotyping tests likely to be used to identify tropism of patient’s viral population having detectable X4 or D/M virus– Clinician can then determine if patient is appropriate
candidate for CCR5 inhibitor therapy

Adverse Effects: CCR5 Antagonist
• MVC – Drug-drug interactions– Abdominal pain– Upper respiratory tract infections– Cough– Hepatotoxicity– Musculoskeletal symptoms– Rash– Orthostatic hypotension

Fusion Inhibitors
• Impair membrane fusion of HIV to T cells
• Subcutaneous injection twice daily

Adverse Effects: Fusion Inhibitor
• ENF – Injection-site reactions– Hypersensitivity reaction– Increased risk of bacterial pneumonia

Co-receptors-Conclusion
• HIV entry process offers several opportunities for therapeutic intervention
• Understanding Env protein is key to development and use of entry inhibitors
• Coreceptor binding offers important target to disrupt HIV infection
• Coreceptors are evolving target for inhibitors– Development of resistance likely and will pose
challenges in how to use therapies• Effective use of entry inhibitors will require careful use of
phenotypic coreceptor tropism assays

Summary: Viral Envelope and Coreceptor Use
• HIV binds to CD4 and a coreceptor
– R5 viruses use CCR5 and are common
– X4 viruses use only CXCR4 and are rare
– D/M viruses can use both coreceptors and are common in later-stage patients
• Coreceptor use largely defines HIV tropism
• New infections almost always due to R5 viruses
• In some patients, D/M and/or X4 viruses emerge years after infection
• Coreceptor switch associated with faster progression

Nucleoside/Nucleotide reverse transcriptase inhibitors (NTRI)
• Nucleoside and nucleotide analogues
• Impair transcription of viral RNA into DNA

Adverse Effects: NRTIs
• All NRTIs: – Lactic acidosis and hepatic steatosis (highest
incidence with d4T, then ddI and ZDV, lower with TDF, ABC, 3TC, and FTC)
– Lipodystrophy(higher incidence with d4T)

Adverse Effects: NRTIs (2)
• ABC– HSR*
– Rash
– Possible ↑ risk of MI
• ddI – GI intolerance
– Peripheral neuropathy
– Pancreatitis
– Possible noncirrhotic portal hypertension
* Screen for HLA-B*5709 before treatment with ABC; ABC should not be given to patients who test positive for HLA-B*5709.

Adverse Effects: NRTIs (3)• d4T
– Peripheral neuropathy– Pancreatitis
• TDF– Renal impairment – Possible decrease in bone mineral density– Headache– GI intolerance
• ZDV
– Headache– GI intolerance– Bone marrow suppression

Non-nucleoside reverse transciptase inhibitors (NNRTI)
• Inhibit reverse transciptase by binding to the enzyme

ARV Components in Initial Therapy: NNRTIs
ADVANTAGES• Long half-lives• Less metabolic toxicity
(dyslipidemia, insulin resistance) than with some PIs
• PIs and II preserved for future use
DISADVANTAGES• Low genetic barrier to
resistance – single mutation
• Cross-resistance among most NNRTIs
• Rash; hepatotoxicity• Potential drug interactions
(CYP450)• Transmitted resistance to
NNRTIs more common than resistance to PIs

Adverse Effects: NNRTIs
• All NNRTIs:– Rash, including Stevens-Johnson syndrome– Drug-drug interactions
• EFV– Neuropsychiatric– Teratogenic in nonhuman primates + cases of neural tube defects in
human infants after first trimester exposure
• NVP– Higher rate of rash – Hepatotoxicity (may be severe and life-threatening;
risk higher in patients with higher CD4 counts at the time they start NVP)

Protease Inhibitors (PI)
• Impair the packaging of viral particles into mature virus capable of budding from the cell

ARV Components in Initial Therapy: PIs
ADVANTAGES• Higher genetic barrier
to resistance• PI resistance
uncommon with failure (boosted PI)
• NNRTIs and II preserved for future use
DISADVANTAGES• Metabolic complications
(fat maldistribution, dyslipidemia, insulin resistance)
• GI intolerance
• Potential for drug interactions (CYP450), especially with RTV

Adverse Effects: PIs
• All PIs: – Hyperlipidemia – Insulin resistance and diabetes– Lipodystrophy – Elevated LFTs– Possibility of increased bleeding risk
for hemophiliacs– Drug-drug interactions

Adverse Effects: PIs (2)
• ATV– Hyperbilirubinemia– PR prolongation– Nephrolithiasis
• DRV – Rash– Liver toxicity
• FPV– GI intolerance– Rash– Possible increased risk of MI

Adverse Effects: PIs (3)
• IDV– Nephrolithiasis– GI intolerance
• LPV/r – GI intolerance– Possible increased risk of MI– PR and QT prolongation
• NFV – Diarrhea

Adverse Effects: PIs (4)
• RTV
– GI intolerance– Hepatitis
• SQV – GI intolerance
• TPV – GI intolerance– Rash– Hyperlipidemia– Liver toxicity– Cases of intracranial hemorrhage

Integrase Inhibitors
• Prevent incorporation of viral DNA into host cell genome

ARV Components in Initial Therapy: II (Raltegravir)
ADVANTAGES• Virologic response
noninferior to EFV• Fewer adverse events
than with EFV• Fewer drug-drug
interactions than with PIs or NNRTIs
• NNRTIs and PIs preserved for future use
DISADVANTAGES• Less experience with IIs,
limited data• Twice-daily dosing• Lower genetic barrier to
resistance than PIs• No data with NRTIs other
than TDF/FTC in initial therapy

Adverse Effects: II• RAL
– Nausea– Headache– Diarrhea– CPK elevation

Integrase Enzyme• Viral enzyme essential to replication of
both HIV-1 and HIV-2
• Integration– Follows reverse transcription, which
synthesizes double-stranded DNA copy of HIV-1 RNA after infection
– Essential step before viral DNA can be transcribed back into viral RNA
– Incorporates or “integrates” viral DNA into host cell’s DNA

Integrase Strand Transfer Inhibitors
• Raltegravir (pyrimidinone analogue, formerly known as MK-0518)[1]
– First approved integrase inhibitor
– Originally approved for use in treatment-experienced patients; recently approved for treatment-naive patients
• Elvitegravir (diketoacid derivative of dihydroquinoline-3-carboxylic acid, formerly known as GS-9137)[2]
– Currently in phase III clinical trials
• S/GSK1349572[3]
– New integrase inhibitor active against raltegravir- and elvitegravir-resistant isolates in vitro
– Currently in phase IIb clinical trials1. Markowitz M, et al. J Acquir Immune Defic Syndr. 2006;43:509-515. 2. DeJesus E, et al. J Acquir Immune Defic Syndr. 2006;43:1-5. 3. Lalezari J, et al. IAS 2009. Abstract TUAB105.