Embed Size (px)
Citation preview

VIEWS & REVIEWS
HIV phenotypes - gaining importance as surrogate markers in AIDS
-Tracey Taylor-
A key issue that emerged at the VIIIth International AIDS Conference was the relationship between different phenotypes of "IV, the emergence of drug resistance and the onset of progression to AIDS.
To date, the most frequently used surrogate marker for HIV infection progression has been circulating CD4+ T lymphocyte counts. As HIV infection progresses, CD4 (the prime receptor target for HIV attack) levels decrease. However, there are a number of problems with this marker: • The level of circulating HIV-infected CD4+ T
lymphocytes only represents a minor proportion of the total body count. Other organs and, in particular, lymph nodes house the bulk of HIV-infected CD4+ lymphocytes.
• CD4 count decline in HIV-infected patients is not accurately represented by the classical curve usually described [see diagram]. Natural variations, including increases in CD4 counts, occur in HIV-infected and noninfected populations.
• CD4+ cell levels are not always reliable predictors of treatment effect. Similarly, very little of the treatment effect is explained by changes in antigen load. Therefore, there is an immediate need for a more
accurate means of determining when to initiate or change treatment regimens in HIV-infected patients.
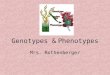
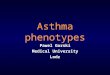
Relationships in AIDS progression
Envelope mulaUons NSI --------~------------ SI
• Low levels 01 HIV repheal,on
• Slow developmenr of z,dovud,ne·res,slanl mUlal,ons
• MT2 ooillrop,sm negat,ve (d,agnoShe)
HIV load
CD4 count
• Increased HIV rephcal,on
• Increased developmenl of z,dovudone·res,slanl muta"ons
• MT2 cell Irop,sm pos",ve (d,agnosl,el
The answer may lie in the different phenotypes ofIDv.
It appears that the emergence of drug resistance and disease progression are closely linked to the predominant circulating HIV phenotype.
The 2 differential phenotypes are nonsyncytium-inducing (NSI) HIV and syncytium-inducing (SI) HIY. It seems that SI HIV is the cytopathic version of the virus, which emerges in approximately 50% of patients during progression to AIDS. On the other hand, patients infected with the NSI phenotype are largely asymptomatic. An increase in viral load is preceded
ISSN 0156-270319210815-0031$1.00'" Adls International Ltd
by the emergence of the cytopathic (SI) virus, which may also herald the onset of drug resistance. It has also been observed that CD4+ cell counts decrease 3- to 5-fold more rapidly after the emergence of SI virus.
In a study conducted in HIV-infected homosexual males in Amsterdam, 67% of SI- and 16% of NSI-infected patients progressed to AIDS within 30 months.
What are the therapeutic implications of SI and NSI lHV?
It appears that while zidovudine does interfere with progression to AIDS in patients harbouring the NSI virus, this effect is not seen in patients with SI HIY.
Unfortunately, zidovudine does not impede the 'switch' from NSI to SI phenotype. According to Dr. Frank Miedema, this implies that zidovudine monotherapy is only useful in asymptomatic patients with NSI HIV, and that combination therapy or substitution with another agent should be initiated in patients who are in the SI stage of disease.
'Anyone with CD4 counts of 300 or less who has been on zidovudine for 16 weeks
should change to didanosine. ' James Kahil.
Preliminary results from the ACTG 116b/ll7 trial. conducted by Dr. James Kahn and colleagues, supported Dr. Miedema's view.
The 913 patients enrolled had CD4 counts less than 300 (less than 200 if they were asymptomatic) and had received a minimum of 16 weeks' zidovudine therapy. They were randomised in a double-blind protocol to treatment with didanosine 500 or 750mg or zidovudine 500mg.
No difference in overall survival was seen between recipients of didanosine 500 or 750mg or zidovudine 500mg. However, didanosine recipients had consistently higher CD4 counts and experienced less haematological toxicity than zidovudine recipients. Patients who received didanosine 500mg were also less likely to progress to the study endpoints, which were the development of AIDS or a new AIDS-defining event or death.
No differences in the incidence of peripheral neuropathy were observed between groups. Didanosine 750mg, but not 500mg, recipients experienced significantly more pancreatitis than zidovudine recipients.
How practical is the use of phenotypic data? According to a number of leading researchers,
obtaining phenotypic data is simple and practical. The diagnostic assay to determine levels of SI and NSI HIV involves the presence or absence of MT2 cell tropism, respectively. However, standardisation is required before it becomes a recognised procedure.
SOOl510C1i1
INPHARMA~ 15 Augl992
3