Embed Size (px)
Citation preview
Hodgkin ’s Disease in Married Couples
THOMAS D. FOGEL, MD,’ RICHARD E. PESCHEL, MD, PHD,* AND ROSE PAPAC, MDt
l h e case of a husband and wife who both developed Hodgkin’s disease of the same cellular subtype is reported. This represents only the fifth reported case of marital Hodgkin’s disease that is well- documented histiologically. The relevant literature and potential implications are reviewed.
Cancer 52495-2497, 1985.
‘HE ETIOLOGY of Hodgkin’s disease (HD) remains T unknown. Immunologic, infectious, environmental, and genetic factors have all been impli~ated.’-~ Cases of familial HD give some support for an immunologic or genetic e t i ~ l o g y , ~ , ~ , ~ - ’ ~ and the clustering of cases in certain groups and communities has encouraged specu- lation that the disease may be induced by or transmitted by an infectious agent such as a Our current understanding of Burkitt’s lymphoma, nonhuman leu- kemias, and the retrovirus associated adult T-cell lym- phoma encourages further speculation for the potential role of a virus in the pathogenesis of HD.I2
The occurrence of HD in married couples is We report here the case of a husband and
wife who developed HD of the same cellular subtype. The relevant literature and potential implications will be discussed.
rare ,2,4.7.8. I0
Case Reports
CUSC? I A single 19-year-old white man presented with epigastric
pain in 1968. A gastrointestinal (GI) workup was normal but a routine chest x-ray disclosed a right superior mediastinal mass. Physical examination was unremarkable except for the presence of several small movable lymph nodes in the left axilla and some shotty adenopathy in the right inguinal region, none of which were believed to be significant. An open thoracotomy was performed. A biopsy specimen of an abnormal mediastinal lymph node revealed HD, nodular sclerosing type. A lymphangiogram was read as highly suspicious in the right and left para-aortic lymph node region. A bone marrow biopsy specimen was negative for tumor. Routine blood chemistries
* Department of Therapeutic Radiology, Yale University School of Medicine, New Haven, Connecticut 065 10.
t Chief of Hematology and Oncology Section, Veteran’s Adrninis- tratioin Hospital. West Haven, Connecticut 065 16.
Address for repnnts: Richard E. Peschel, MD, PhD, Department of Therapeutic Radiology. Yale University School of Medicine, 333 Cedar Street, New Haven, CT 06510.
Accepted for publication May 30, 1984.
and an intravenous pyelogram were normal. The patient denied any “B symptoms.” The patient was, therefore, staged as a clinical Stage IIIA. No staging laparotomy was performed. The patient received total nodal irradiation (4000 rad to a mantle field, 4000 rad to a para-aortic plus spleen field. and 3600 rad to a pelvic and bilateral inguinal field) from June through October of 1968. Following treatment, the patient was in complete remission. In 1972, 4 years after his total nodal irradiation, the patient was married to a 24-year-old white woman who is discussed in Case 2. The patient has remained free of recurrent disease for 17 years with his last follow-up visit in January of 1985.
Case 2
This woman was 24 years old when she married the patient discussed in Case 1 in 1972. Her husband had received total nodal irradiation in 1968 for HD, clinical Stage IIIA, and he was in complete remission at the time of their mamage. Nine years later, in August of 1981, this woman, now 33 years old, developed left neck adenopathy. The rest of her physical examination was normal. A biopsy specimen of the left neck adenopathy documented HD. nodular sclerosing type. Clinical staging included a chest x-ray, lymphangiogram, liver/spleen scan, bone marrow biopsy, and intravenous pyelogram which were all within normal limits. A staging laparotomy with splenectomy, open liver biopsy, and random lymph node sampling was entirely unremarkable. The patient denied any “B symptoms” and she was, therefore, a pathologic Stage IA. The patient received subtotal nodal irradiation including Wal- deyer’s ring (4000 rad to a mantle field, 3600 rad to Waldeyer’s ring, 3600 rad to a para-aortic and splenic pedicle field) from November 1981 to February 1982. This patient remains without evidence of recurrent disease at her last clinic visit in January of 1985.
Discussion
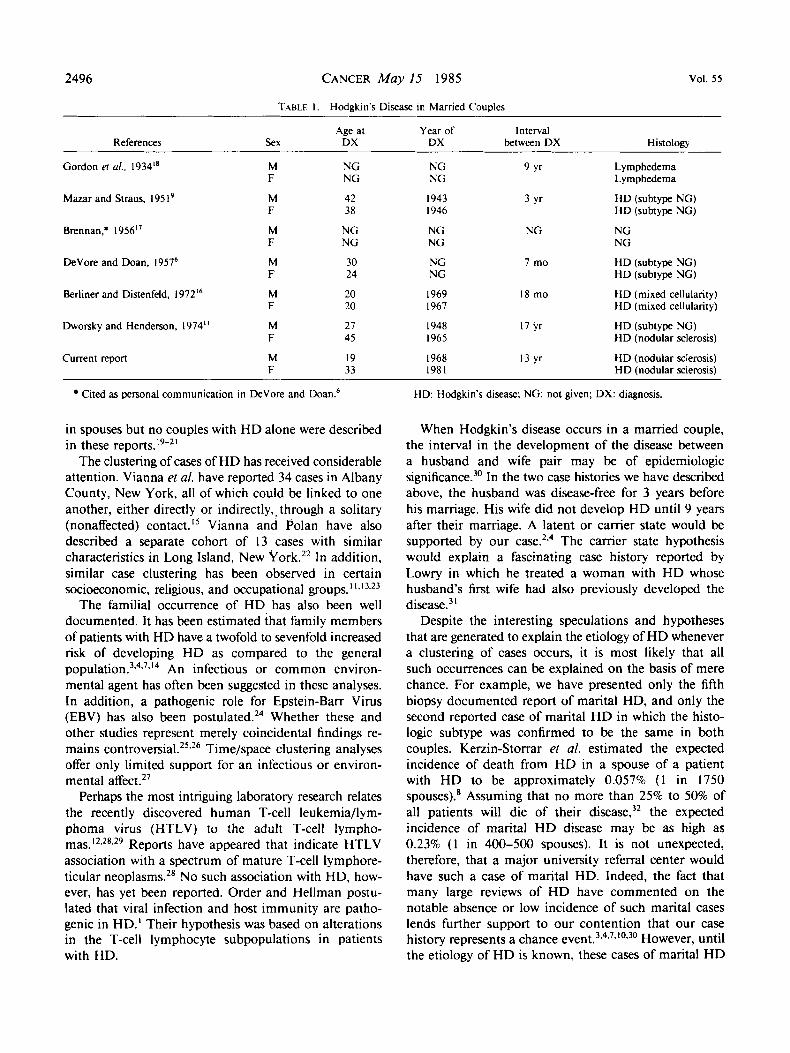
The appearance of HD in spouses is rare. Only six other couples have been reported of which only four are well-documented histologically.6~9~’1~’6~18 Th e relevant data on all reported cases are summarized in Table 1. Other authors have reported “lymphoreticular disorders”
2495
2496 CANCER May I5 1985 Vol. 5 5
TABLE I . Hodgkin’s Disease in Mamed Couples
Age at Year of Interval References Sex DX DX between DX Histology
Gordon er al., 1934” M NG NG 9 Yr Lymphedema F NG NG Lymphedema
M a r and Straus, I95 l 9 M 42 I943 3 Yr €1D (subtype NG) F 38 I946 €ID (subtype NG)
Brennan,. 1956” M NG NG NG NG F NG NG NG
DeVore and Doan, 19576 M 30 NG 7 mo HD (subtype NG) F 24 NG HD (subtype NG)
Berliner and Distenfeld, 197216 M 20 1969 18 mo )ID (mixed cellularity) F 20 1967 €ID (mixed cellularity)
Dworsky and Henderson, 1974” M 21 I948 17 yr H D (subtype NG) F 45 1965 €ID (nodular sclerosis)
Current report M 19 1968 13 yr HD (nodular sclerosis) F 33 1981 HD (nodular sclerosis)
Cited as personal communication in DeVore and Doan.6
in spouses but no couples with HD alone were described in these
The clustering of cases of HD has received considerable attention. Vianna et a/. have reported 34 cases in Albany County, New York, all of which could be linked to one another, either directly or indirectly,, through a solitary (nonaffected) contact.” Vianna and Polan have also described a separate cohort of 13 cases with similar characteristics in Long Island, New York.22 In addition, similar case clustering has been observed in certain socioeconomic, religious, and occupational groups. ’ 1 9 1 3 . 2 3
The familial occurrence of HD has also been well documented. It has been estimated that family members of patients with HD have a twofold to sevenfold increased risk of developing HD as compared to the general p ~ p u l a t i o n . ~ , ~ . ~ . ’ ~ An infectious or common environ- mental agent has often been suggested in these analyses. In addition, a pathogenic role for Epstein-Barr Virus (EBV) has also been p ~ s t u l a t e d . ~ ~ Whether these and other studies represent merely coincidental findings re- mains c o n t r o v e r ~ i a l . ~ ~ . ~ ~ Time/space clustering analyses offer only limited support for an infectious or environ- mental affect.27
Perhaps the most intriguing laboratory research relates the recently discovered human T-cell leukemia/lym- phoma virus (HTLV) to the adult T-cell lympho- mas. ‘ 2 * 2 8 3 2 9 Reports have appeared that indicate HTLV association with a spectrum of mature T-cell lymphore- ticular neoplasms.28 No such association with HD, how- ever, has yet been reported. Order and Hellman postu- lated that viral infection and host immunity are patho- genic in HD.’ Their hypothesis was based on alterations in the T-cell lymphocyte subpopulations in patients with HD.
HD: Hodgkin’s disease; NG: not given; DX: diagnosis.
When Hodgkin’s disease occurs in a mamed couple, the interval in the development of the disease between a husband and wife pair may be of epidemiologic significance.m In the two case histories we have described above, the husband was disease-free for 3 years before his marriage. His wife did not develop HD until 9 years after their marriage. A latent or camer state would be supported by our ~ a s e . ~ . ~ The camer state hypothesis would explain a fascinating case history reported by Lowry in which he treated a woman with HD whose husband’s first wife had also previously developed the d i sea~e .~
Despite the interesting speculations and hypotheses that are generated to explain the etiology of HD whenever a clustering of cases occurs, it is most likely that all such occurrences can be explained on the basis of mere chance. For example, we have presented only the fifth biopsy documented report of marital HD, and only the second reported case of marital H D in which the histo- logic subtype was confirmed to be the same in both couples. Kerzin-Storrar el af. estimated the expected incidence of death from HD in a spouse of a patient with HD to be approximately 0.057% ( 1 in 1750 spouses).8 Assuming that no more than 25% to 50% of all patients will die of their disease,32 the expected incidence of marital HD disease may be as high as 0.23% ( 1 in 400-500 spouses). It is not unexpected, therefore, that a major university referral center would have such a case of marital HD. Indeed, the fact that many large reviews of HD have commented on the notable absence or low incidence of such marital cases lends further support to our contention that our case history represents a chance event.3v4-7,’0*30 However, until the etiology of H D is known, these cases of marital HD
No. 10 HODGKIN’S DISEASE IN MARRIED COUPLES Fogel er al. 2497
remain an obvious source of fascination, speculation, and potential importance.
REFERENCES
I . Order SE, Hellman S. Pathogenesis of Hodgkin’s disease. Lancet
2. Vianna NJ, Greenwald P, Davies JNP. Hodglan’s disease: An infectious disease? In: Lacher MJ, ed. Hodglun’s Disease. New York: John Wiley & Sons, 1979; 405-415.
3. Cirufferman S, Cole P, Smith PG, Lukes RJ. Hodgkin’s disease in siblings. N Engl J Med 1977; 296:248-250.
4. Gruffeman S. Clustering and aggregation of exposures in Hodg- kin’s disease. Cancer 1977; 39: 1829-1833.
5 . Henderson BE, Dworsky R, Menck H et a / . Case-control study of Hodgkin’s disease: 11. Herpes virus group antibody titers and HL-A type. J Nut1 Cancer Inst 1973; 51:1443-1447.
6. DeVore JW, Doan CA. Studies in Hodgkm’s syndrome: XII. Hereditary and epidemiologic aspects. Ann Intern Med 1957; 47:300- 316.
7. Fraumeni JF Jr. Family studies on Hodglun’s disease. Cancer Res 1974; 34:1164-1165.
8 . Kerzin-Storrar L, Faed MJW, MacGillirray JB, Smith PG. Inci- dence of familial Hodgkin’s disease. Br J Cancer 1983: 47:707-712.
9. klazar SA, Straus B. Marital Hodgkin’s disease: A review of the familial incidence and of etiological factors. .4rch Intern Med 195 1;
10. Kazis DV, Diamond HD, Craver LF. Familial Hodgkin’s disease: Its significance and implications. Ann Intern Med 1959; 51:933-971.
1 I . lDworsky RL, Henderson BE. Hodgkin’s disease clustering in families and communities. Cancer Res 1974; 341 161-1 163.
12. Gallo RC, Gelmann EP. In search of a Hodgkm’s disease virus. N Engl J Med 198 1 ; 304: 169- 170.
13. Gutensohn N, Cole P. Childhood social environment and Hodgkin’s disease. N Engl J Med 198 1 ; 304: 135- 140.
14. Schimpff SC, Schimpff CR, Brager DM, Wiernik PH. Leukemia and lymphoma patients interlinked by prior social contact. Lancet
15. ’v‘ianna NJ, Greenwald P, Brady J et a/ . Hodgkin’s disease: Cases with features of a community outbreak. Ann Intern Med 1972;
1972; 11571-573.
88:819-830.
1975; I : 124-129.
77: 169-1 80.
16. Berliner AD, Distenfeld A. Hodglun’s disease in a married couple. JAMA 1972; 221:703-704.
17. Brennan MJ. 1956. Cited as personal communication by DeVore and Doan.6
18. Gordon MH, Cow AC, Levitt WM, Weber FP. Recent advances in the pathology and treatment of lymphadenoma. Proc R Sac Med
19. Hazen PG, Michel B. Hodglan’s disease and mycosis fungoides in a married couple. Dermatologica 1977; 154:257-260.
20. Stephens RL, Larsen WE, Holmes FF, Clark GM. Connubial lymphoproliferative malignancies: A report of nine couples. Med Pediatr Oncol 1977; 3:35 1-358.
21. Takats W, Csapo ZS. Malignant lymphomas occurring in marital partners: Case reports on two couples. Br J Cancer 1968; 22:
22. Vianna NJ, Polan AK. Epidemiologic evidence for transmission of Hodgkin’s disease. N Engl J Med 1973; 289:499-502.
23. Vianna NJ, Polan AK, Keogh MD, Greenwald P. Hodglan’s disease mortality among physicians. Lancet 1974; 2: 13 1- 133.
24. Veltri RW, Shah SH, McClung JE et al. Epstein-Barr virus, fatal infectious mononucleosis, and Hodgkin’s disease in siblings. Cancer 1983; 51:509-520.
25. Pike MC, Henderson BE, Casagrande J et a/. Infectious aspects of Hodglun’s disease (letter). N Engl J Med 1974; 290:34 I .
26. Smith PG, Pike MC. Case clustering in Hodgkin’s disease: A brief review of the present position and report of current work in Oxford. Cancer Res 1974; 34: 1 156- I 160.
27. Greenberg RS, Gruffeman S, Cole P. An evaluation of space- time clustering in Hodgkin’s disease. J Chronic Dis 1983; 36:257-262.
28. Blattner WA, Blayney DW, Robert-Guroff M ef al. Epidemiology of human T-cell leukemia/lymphoma virus. J Infict Dis 1983; 147:
29. Bunn PA, Schechter GP, Jaffe E et al. Clinical course of retrovirus-associated adult T-cell lymphoma in the United States. N Engl J Med 1983; 309:257-264.
30. Vianna NJ, Davies JNP, Polan AK, Wolfgang P. Familial Hodgkin’s disease: An environmental and genetic disorder. Lancet
31. Lowry WS. Infectious aspects of Hodgkm’s disease (letter). N Engl J Med 1974; 290:341-342.
32. Prosnitz LR, Farber LR, Kapp DS et al. Combined modality therapy for advanced Hodgkin’s disease. Long-term follow-up data. Cancer Treat Rep 1982; 66:871-879.
1934; 27: 1035-1050.
173-175.
406-4 12.
1974; 2~854-857.



![REGISTRATION FORM Married Couples Retreat … their own experience of married life as well as their ex- ... REGISTRATION FORM [MARRIED COUPLES RETREAT-2017] ... “Pick up” Supper](https://img.pdfslide.net/doc/110x75/5b09d2e17f8b9ac7678b6821/registration-form-married-couples-retreat-their-own-experience-of-married-life-as.jpg)

























