Embed Size (px)
Citation preview

HOLZER
CENTER
FOR
CANCER
CARE

TABLE
OF
CONTENTS
PAGE
2PAGE
8
PAGE
4 PAGE
10
PAGE
14 PAGE
20 PAGE
30
PAGE
34 PAGE
24
PAGE
26 PAGE
38
PAGE
16
PAGE
18 PAGE
12PAGE
6
Cancer Liaison
Physician
Report
Cancer
Registry
Report
Holzer
Center for
Cancer
Care
Physicians
Community
Activity
Outreach
Report
Site of
Focus:
Lung
Cancer
Low-Dose
CT Screening
for Lung
Cancer
Palliative
Care
Cases
Diagnosed
in 2016
2016 Lung
Cases for
Holzer
2016 Clinical and Programmatic Goals
Financial Assistance Provided at HCCC
NurseNavigation
Cancer Program Practice Profile (CP3R)
2016 Quality of Care Studies and Improvements
HCCC Staff/ Cancer Committee

At Holzer Health System, thanks to prevention awareness, earlier detection,
advanced treatment, and supportive care, more patients in our Tri-State area are
surviving cancer than ever before. Unlike most rural cancer centers, Holzer Center
for Cancer Care (HCCC) is located in the center of our Tri-State area, allowing
patients to receive cutting-edge treatment closer to home.
One of our greatest successes in 2016 was the renewal of our 3-year
accreditation with the Commission on Cancer (CoC), a consortium of professional
organizations dedicated to improving survival and quality of life for cancer
patients. The CoC is responsible for establishing standards to ensure high
quality, multi-disciplinary, and comprehensive cancer care delivery in hospitals
throughout the United States, granting accreditation to only those facilities that
are committed to providing the best in cancer diagnosis and treatment.
Holzer takes great pride in this achievement and has received CoC accreditation
every three-year survey cycle since 1937. This success is possible through the
Holzer Cancer Committee, a diverse group of highly trained physicians and staff
dedicated to continually improving our cancer program.
Throughout 2016, the physicians, nurses and other team members of the cancer
center have made significant contributions to improving the health and well-
being of hundreds of area residents facing cancer. Our achievements include:
• Improving care and refining processes to improve our patients’ experiences.
• Creating innovative programs, like our survivor support groups, that focus on enhancing the long-term health and well-being of survivors and their families.
• Providing palliative care to all patients receiving treatment at HCCC.
• Increasing our clinical research and genetics activities.
• Providing our community with cancer screening services, like the Lung Low-Dose CT program and cancer prevention education.
• Educating the next generation of physicians, including our residents and medical students from Ohio University.
As we reflect on the outstanding accomplishments of the past year, it is exciting
to see the progress we have made, in our 80th year of achieving our mission:
Friendly Visits, Excellent Care; Every Patient, Every Time.
A YEAR OF
CANCER LIAISON PHYSICIAN REPORT
THANKS TO
PREVENTION
AWARENESS,
EARLIER
DETECTION,
ADVANCED
TREATMENT, AND
SUPPORTIVE
CARE, MORE
PATIENTS IN OUR
TRI-STATE AREA
ARE SURVIVING
CANCER THAN
EVER BEFORE
ALICE DACHOWSKI MD, FACS
Achievement & Advancement 3

As determined
each year by the
cancer committee
and under the
guidance of
Michelle Rankin,
RN and CC QI
Coordinator,
specific
clinical and
programmatic
goals were
established
in January 2016
to improve
our programs.
2016 PROGRAMMATIC GOAL:
To develop enhancements to the medical patient records and overall patient care that
increases accuracy and efficiency.
Procedures are as follows:The consults will be for any chemo patients with potential/active malnutrition. The protocol for nurses will be:
The changes include:A.
Chemo nurse will discuss concerns/options for nutrition consult with patient The physician
will put in order
Nurse discusses
scheduling preferences
Nutrition responds with an answer
Nurse will send task to
nutrition team and have front desk schedule
consult
Nutrition checks on insurance coverage
Created a template for psychosocial screenings
Designed new protocol of sending a task to nurse navigator and scheduling appointment when treatment completed
Developed more complete clinic notes to consolidate treatment information
Addition of Common Terminology Criteria for Adverse Events Assessment (CTCAE) to electronic chemo documentation
Updated chemo and infusion order set policy to state only provider to fill out order set as per ASCO/ONS chemo admin safety standards
Updated infusion order sets according to NCCN guidelines
Standardization of bar scanning meds and wristbands
Added 3 computers in infusion for increased accessibility
2016 CLINICAL GOAL:
Establish a dietary protocol to allow chemotherapy patients the option of receiving
the essential dietary guidance needed during treatment to extend care.
4 5
Nurse discusses results with patient
Patient sees nutritionist

2016 QUALITY
OF CARE
STUDIES AND
IMPROVEMENTS
A recent report created by the American Cancer Society and the
National Colorectal Cancer Round table states, “Community health
centers can do better with colorectal cancer screening rates. About
1 in 3 adults 50 to 75 years of age (23 million people) has never been
screened for colorectal cancer. ln community health centers (CHC),
which largely serve these populations, the national screening rate for
colorectal cancer in 2012 was 30.2%. CHCs have tremendous potential
to improve colorectal cancer screening rates and reduce colorectal
cancer morbidity and mortality in racially and ethnically diverse,
socioeconomically challenged communities across the country. Since
2012, the Federal Health Resources and Services Administration (HRSA)
has required CHCs to report colorectal cancer screening rates as a
standard performance measure as part of the Uniform Data System.”
Michelle Rankin researched Holzer’s current Adenoma Detection Rate
(ADR). There were a total of 152 colonoscopy procedures in the study.
The results were that adenomas were detected in 57% of the patients
who had a polyp removed. According to ASGE, ADR is reported at
10-40%. A higher ADR rate is associated with lower “postcolonoscopy”
colorectal cancer rate.
Again under the guidance of Michelle Rankin, the cancer center /cancer
committee established methods to consistently collect the withdrawal
time of the colonoscopies. Holzer wants to ensure, once the patient
commits to the expenses and prep for colorectal screening, that we are
providing the utmost quality and care.
The American Society for Gastrointestinal Endoscopy states, “Meticulous
inspection and longer withdrawal times are associated with higher
adenoma detection rates (ADR). A high ADR is essential to rendering
recommended intervals between screening and surveillance examinations
safe. Optimal technique is needed to ensure a high probability of
detecting dysplasia when present in inflammatory bowel disease. Finally,
technical expertise and experience will help prevent adverse events that
might offset the benefits of removing neoplastic lesions.”
Michelle researched Holzer’s current scope withdrawal times. She found
that the average withdrawal time was 10 minutes, with a range of 6 to 28
minutes. As stated earlier, the best practice time is 6 minutes or greater.
Overall, in 2014 our colorectal cancer screening rate was 60% for Medicare
patients, but we currently do not have an accurate way to measure
colorectal cancer screening rates for our overall population.
STUDY #1: Improving Baseline Colonoscopy Rates
STUDY #2: Quality of Colonoscopies
1. Require physician documentation to reflect best practices.
2. Monitor “mucosa/debris” collection rates. These patients should be rescheduled for a colonoscopy.
3. Establish a method to report colorectal cancer screening rates system-wide
4. Monitor rates to ensure the highest level of screenings are achieved.
All of the above suggestions are now in place and working well.
Recommendations for both studies include:
6 7

Our Oncologists treat all major adult
cancers and all adult hematological
disorders. The Medical Oncologists are
proficient in the delivery of routine IV
chemotherapy and oral chemotherapies,
as well as having extensive knowledge in
immunotherapy, targeted therapies, and
combined chemotherapy and radiation
therapies. Our Radiation Oncologist is
competent in the delivery of external
radiation therapy and stereotactic
radiation surgery. Working closely with
the Human Geneticists at The Ohio
State University Comprehensive Cancer
Center - James Cancer Hospital and
Solove Research Institute, they provide
the latest medical knowledge in human
oncology genetics. All oncologists also
refer qualifying patients for clinical trials
to optimize care and treatments.
HOLZER
CENTER
FOR
CANCER
CARE
PHYSICIANS
MEDICAL EDUCATIONBrody School of Medicine at
East Carolina University
Greenville, North Carolina
INTERNSHIPInternal Medicine
Pitt County Memorial Hospital -
Greenville, North Carolina
RESIDENCYRadiation Oncology
University of California - Irvine,
California
BOARD CERTIFICATION•American Board of
Radiology - Radiation
Oncology Certified
KHAWAJA K. HAMID, MD Hematology/Oncology
GHADA KUNTER, MD Hematology/Oncology
MELVA PINN-BINGHAM, MD Radiation Oncology
MEDICAL EDUCATIONSind Medical College
Karachi, Pakistan
RESIDENCY•St. Vincent’s Medical Center
Bridgeport, Connecticut
•St. Elizabeth’s Hospital
Utica, New York
FELLOWSHIPMedical Oncology
Providence Medical Center
Southfield, Michigan
BOARD CERTIFICATION•American Board of Internal
Medicine
•American Board of Medical
Oncology
•American Board of Medical
Specialists
RESIDENCYInternal Medicine
University of Kansas School of
Medicine, Wichita Center for
Graduate Medical Education
Wichita, Kansas
FELLOWSHIPS•Department of Adult
Hematology/Oncology
Winship Cancer Institute
Emory University School of
Medicine - Atlanta, Georgia
•Department of Blood and
Marrow Transplantation
Moffitt Cancer Center,
University of South Florida
Tampa, Florida
•Pediatric Hematology/
Oncology
Children’s Hospital in St. Louis
Washington University School
of Medicine
St. Louis, Missouri
BOARD CERTIFICATION•American Board of Internal
Medicine
•American Board of Pediatrics
•American Board of Pediatric
Hematology/Oncology
•American Board of Adult
Medical Oncology8 9

NURSE
NAVIGATION
Patient Navigators are trained,
culturally sensitive health care workers
who provide support and guidance
throughout the cancer care continuum.
They help people “navigate” through
the maze of doctors’ offices, clinics,
hospitals, outpatient centers, insurance
and payment systems, patient-support
organizations, and other components
of the health care system. Services are
designed to support timely delivery of
quality standard cancer care and ensure
that patients, survivors, and families are
satisfied with their encounters with the
cancer care system.
I. REFERRALS
II. COLLABORATION
III. TRACKING & DOCUMENTATION
IV. EDUCATION
Provides Access to Resources and Assesses Patients’ Current and Future Needs, and Financial Referrals
Develops Physician/Cancer Care
Team Relationships
Tracks Metrics, Quality Indicators; Documents Patient Interactions, Progression
Provides Patient Education, Provides Symptom Management Support
A.
A.
A.
A.
• Makes referrals for services based on patient/family needs – education, finances, psychosocial, survivorship, transportation, child care, lodging.
• Assesses for and assists with patient/family resources.
• Facilitates access to physicians and services.
• Assists with education, including disease state and treatment.
• Assesses for and mitigates barriers to care. Assists patients with access concerns (for screening, diagnosis, or treatment) and assists with paperwork and addressing access barriers as indicated.
• Facilitates appropriate medical record availability at scheduled appointments as needed.
• Facilitates transportation, lodging, and/or child/elder care and addresses any other practical needs.
• Facilitates linkages to follow-up services.
• Facilitates access to clinical trials.
• Creates and reviews Survivorship Care Plan with patients.
• Communicates and collaborates with involved physicians and staff members to facilitate individualized, holistic patient care plan.
• Facilitates communication between cancer care disciplines.
• Maintains communication with patients, survivors, families, and the health care providers to monitor patient satisfaction with the cancer care experience.
• Ensures that navigator functions are meeting physician expectations and that navigator activities remain within scope of defined role.
• Ensure timely documentation of all patient interactions into navigation tracking and documentation system(s).
• Assists with tracking, documentation and outcome reporting for navigation services.
• Assists with ongoing navigation program assessment and identification of process improvement opportunities.
• Assists with annual CoC Standard 3.1 activities related to community needs assessment and resulting program modifications related to needs; assists with program reporting to the Cancer Committee.
• Assists with coordinating appointments.
• Meets with patient by phone or in person prior to, during, and after treatment.
• Facilitates timely coordination of services between diagnosis and treatment.
• Provides telephone triage services (e.g., symptom management, emotional support, education, resource referral) for patients/families.
• Coordinates appointments for diagnostic testing, services, and with providers to ensure timely delivery of diagnostic and treatment services, providing clarification and literacy-level-appropriate education related to the visit.
10 11
Community Outreach
Coordination of Patient Care (coordinating/facilitating appointments, accompanying patients to appointments as needed) B.
B.
• Discusses physician visits with patients and families and answer questions.
• Provides and reinforces education re: treatment, care plan, symptom management and survivorship concerns.
• Empowers patients with education and knowledge to help improve patient outcomes and satisfaction.
• Conducts health promotion and awareness programs in community as appropriate.
• Provides community education presentations as appropriate.
• Coordinates patient care from diagnosis through survivorship or palliative care/hospice.

The Commission on Cancer (CoC)
tracks each case submitted by our
hospital. Those cases that meet the
criteria for the described measures are
reviewed to ensure quality treatment
is met. With the new Rapid Quality
Reporting System, cases are sent
to the CoC on a monthly basis, with
results of the measures given each
month. This proactive system confirms
that the most valuable treatment is
being given on a timely basis.
Image or palpation-guided needle (core or FNA) of the primary site is performed to establish diagnosis of breast cancer
Tamoxifen or third generation aromotase inhibitor is considered or administered within 1 year of diagnosis for women with AJCC T1c or stage IB-III hormone receptor positive breast cancer
Radiation therapy is considered or administered following any mastectomy within 1 year of diagnosis of breast cancer for women with >= 4 positive regional lymph nodes
Radiation is administered within 1 year of diagnosis for women under the age of 70 receiving breast conservation surgery for breast cancer
Combination chemotherapy is considered or administered within 4 months of diagnosis for women under 70 with AJCC T1cN0, or stage IB - III hormone receptor negative breast cancer
Adjuvant chemotherapy is considered or administered within 4 months of diagnosis for patients under the age of 80 with AJCC stage III colon cancer
Endoscopic, laparoscopic, or robotic surgeries performed for all Endometrial cancer for all stages except stage IV
Use of brachytherapy in patients treated with primary radiation with curative intent in any stage of cervical cancer.
Surgery is not the first course of treatment for stage cN2 M0 lung cases
Systemic chemotherapy is administered within 4 months preoperatively to 6 months postoperatively or it is considered for surgically resected cases with pathologic positive lymph nodes for Non-Squamous Cell Lung Cancer
80%
90%
90%
90%
90%
90%
Not applicable
Not applicable
Not applicable
Not applicable
92.3%
100%
100%
100%
100%
100%
100%
100%
100%
100%
Quality Measures
for Breast, Colon,
Endometrium, and
Lung Cancers
CANCER
PROGRAM
PROFILE
REPORTS
(CP3R)
CoC MeasureStandard to Meet
HCCC Rate
12 13

WHAT IS THE CANCER REGISTRY?
Cancer is a reportable disease in every state in the United States. For every patient
diagnosed with this disease, all physicians, dentists, laboratories, and other health
care providers must collect, process, and report each malignant case through a
certified tumor registrar (CTR). The Holzer Center for Cancer Care CTR, Robin Lyles,
operates under the direction and guidance of Holzer’s Cancer Committee.
Holzer Center for Cancer Care’s (HCCC) Cancer Committee is a diverse group of
individuals within the System, designated to provide leadership in the planning,
initiation, stimulation, and assessment of Holzer’s cancer care services and activities,
in accordance with the American College of Surgeons’ Commission on Cancer (CoC)
requirements. The Committee includes representatives from Surgery, Radiology,
Medical Oncology, Radiation Oncology, Pathology, Administration, Nursing,
Navigation, Palliative Care, Community Wellness, Pharmacy, Social Work, Nutrition,
Rehabilitation, Marketing, Pastoral Care, and Genetics, as well as an American
Cancer Society representative.
WHAT IS THE CANCER REGISTRY USED FOR?
Cancer Registry data is used by the Department of Health, county and local health
departments, patient and public interest groups, researchers, and the public for
health planning and evaluation, as well as for research, incidence patterns, and
trends for southeast Ohio.
The Cancer Registry plays an important role in research to identify the causes of
cancer. Researchers often use the data collected by the registry to identify higher
incidences of cancer with specific exposures and/or particular geographical areas.
HOW DOES THE REGISTRY PROTECT PRIVACY?
All information reported to the Ohio Department of Health and the National Cancer
Data Base is confidential and strict procedures are enforced to protect patient
privacy. For all records sent to the state and national organizations, all patient
indicators have been removed.
WHAT IS A CANCER
CONFERENCE?
HCCC offers a cancer conference each month at
Holzer Health System, allowing multidisciplinary
physicians to determine the most effective care
for the most challenging cancer cases, as well
as providing education for all in attendance. It is
monitored by one of our clinical pathologists and
Cancer Conference Coordinator, Dr. Raul Gagucas,
to ensure these conferences meet the CoC goals.
All in attendance receive 1 CME for each conference.
WHAT INFORMATION IS
COLLECTED ABOUT PATIENTS
WITH CANCER?
The cancer registry collects data on the
demographics, anatomic sites and sizes of tumors,
the stages of diagnosis, the cell types of cancer,
treatment information, and annual follow up. All
malignant cancers are reported except Squamous
and Basal Cell Carcinomas and in situ malignant
tumors from the cervix, prostate, vulva, vagina, and
anus. All brain and nervous system tumors are also
collected, even those that are benign.
HOW LONG HAS HOLZER’S
CANCER REGISTRY BEEN
COLLECTING AND REPORTING
CANCER DATA?
Holzer Center for Cancer Care has been accredited
with the CoC every three-year survey cycle since
1937 and the registry has 12,600 cases on file.
Holzer Medical Center established the cancer
registry in 1977 and has been collecting all required
data since that time.
The commission on Cancer requires that registrars follow all cancer patients in their registry that have received first-course treatment for their lifetime. This information assists physicians when accessing patients who may return for check-ups, aids in early identification of recurrences, and helps to determine treatment. The overall successful followup rate since 2001 at Holzer Center for Cancer Care for 2016 was 90.68% (required minimum is 80%). The successful followup rate for the last 5 years was 94.14% (required minimum is 90%).
Since 2001
4,021
1,646
1,499
293
At least 80%
90.68%
Total new patients in the registry
Less deceased
Number living
Patients lost to follow up
Percentage of Successful Follow Up Rate
HCCC Rate as of December 31, 2015
The last 5 years
1,438
392
752
67
At least 90%
94.14%
CANCER
REGISTRY
REPORT
ONCOLOGY QUALITY/DATA SPECIALIST
Robin Lyles, CTR, MEd
As Cancer Registrar, Robin’s responsibilities are as follows:
Other aspects of Robin’s position includes duties as the Quality/Data Specialist, such as:
• Identifies all patients having the diagnosis and/or treatment of cancer within Holzer Health System and enters each case into the cancer software system.
• Assigns codes for cancer diagnoses utilizing ICD-9, ICD-10, and ICD-O coding and enters diagnostic, demographic, and registry data into the cancer registry software program.
• Prepares the agenda and records minutes for the monthly Tumor Board conferences and quarterly Cancer Committee meetings.
• Performs TNM staging classifications.
• Compiles registry reports utilizing the hospital’s database and national and state statistics.
• Provides patient care evaluation studies each year and presents to the Committee.
• Assists oncology leadership in the development, measurement, and reporting of quality cancer data.
• Participates in educational events annually to maintain certification status, including attendance to regional and national conferences.
• Follows cancer patients treated at HCCC for their lifetime.
• Coordination and management of the Cancer Committee meetings, including review of the 34 CoC standards for accreditation.
• Working closely with all 6 CoC coordinators to originate and implement services and write annual summaries.
• Submission and maintenance of all documentation for the CoC and upload of completed information.
• Performing research studies, workload statistics, and projects, including solution proposals and actions for resolution.
• Identifying methods of utilizing registry data through patient care evaluation audits and special research studies.
• Assistance in the development
of the annual reports.
• Responsible for all aspects of maintaining the system’s oncology program in compliance with the CoC.
• Participating in marketing initiatives, including cancer prevention programs, screenings, and wellness fairs.
• Advising Cancer Committee on changes in cancer patient population, referral patterns, trends in treatment modalities, evaluation of patient care, and other topics of interest to the Committee.
• Robin is also a member of the National Cancer Registrar’s Association, Ohio Cancer Registrars Association, and Cancer Registry Association of Central Ohio.
FOLLOW UP RATES FOR 2016
14 15

FINANCIAL
ASSISTANCE
PROVIDED
AT HCCC
In addition to facing the physical
suffering of cancer treatment, these
procedures can also present serious
financial difficulties for patients and
their families, even for those with health
insurance. With the costs of cancer care
clearly increasing and cancer patients
now living longer than ever before,
many insurance companies transfer
more and more of the costs to the
patients. These additional burdens can
have negative effects on healing, both
mentally and physically.
Today there are many support services
available for patients with cancer.
However, the majority of patients and
even the healthcare providers are
unaware of these services. To help
patients pay for their cancer care,
many drug companies, as well as non-
profit organizations and foundations,
have developed financial assistance
programs to offset the high cost of
cancer care for patients. These financial
assistance programs are designed
specifically to help patients pay for
medications, medical bills, and other
expenses related to cancer care, such
as travel to a cancer facility and hotel
stays during treatment.
HCCC’s Revenue Cycle
Specialist, Ashley
Foster, is certified
through the Association
of Community of
Cancer Care (ACCC).
She assists each patient
in finding alternate
funding to ease this
financial burden prior
to a patient starting their cancer
treatment. Ashley verifies insurance
benefits and determines an estimated
out-of-pocket cost for the planned
cancer treatment. Based on the
diagnosis and medications ordered,
Ashley finds available assistance
programs, grants, or foundations
that the patient would qualify for
and assists them in the application
process. Once approved, she will
continue to work with the programs
to ensure payment is received for
each treatment, taking a huge
financial burden off of our patients.
16 17

18 19
CANCER COMMITTEE
Our strongest asset at Holzer Center for Cancer Care is our staff. Our specialists blend their expertise together to provide a unified approach to optimal treatment and provide the very best comprehensive cancer care available anywhere.
NAME MEMBER STATUS DEPARTMENT NAME MEMBER STATUS DEPARTMENT
Alice Dachowski, MD Appointee SURGERY/COMMITTEE CHAIR/CLP
Amy Bokal, MD Appointee DX RADIOLOGY
Ghada Kunter, MD Appointee MEDICAL ONCOLOGY
Khawaja Hamid, MD Alternate MEDICAL ONCOLOGY
Subhash Khosla, MD Appointee RADIATION ONCOLOGY
Raul Gagucas, MD Appointee PATHOLOGY/CANCER CONFERENCE COORD
Sarah Harrigan, RN, MSN, OCN Appointee CANCER PROGRAM ADMINISTRATOR
Robin Lyles, CTR, MEd Appointee CERTIFIED TUMOR REGISTRAR & CANCER REGISTRY QUALITY COORD
Amity Wamsley, LPN Appointee CLINICAL RESEARCH COORD
MarJean Kennedy, MBA, PCM Appointee COMMUNITY WELLNESS
Melissa Burris, RN Appointee NURSING
Michelle Rankin, RN, MSN Appointee QUALITY IMPROVEMENT/ MANAGEMENT COORD
Teresa Stewart, RN, CHPN Appointee PSYCHOLOGICAL SERVICES COORD
Ryan Ramsburg, RT Additional Member DOSIMETRIST
Stella Barrett, OTR/L Additional Member REHABILITATION
Hilary Nichols Additional Member AMERICAN CANCER SOCIETY
Fred Williams, PhD Additional Member PASTORAL CARE
Jared Vernon, RPh Additional Member PHARMACY
Sarah Ramsburg, LD, RD Additional Member NUTRITION SERVICES
Amity Wamsley, LPN Additional Member LPN/GENETICS ASSISTANT

COMMUNITY
OUTREACH
ACTIVITY
REPORT
2016 DIETARY COMMUNITY OUTREACH ACTIVITIES provided by Holzer Nutritional Services/Registered Dieticians
and Health and Wellness
As a Commission on Cancer
accredited facility, the Holzer Center
for Cancer Care is committed to
community outreach and support
services for cancer care. Community
outreach services increase the
public awareness of prevention
activities, promote the benefits
of early detection and encourage
participation in screening programs.
Holzer Health System, a not-
for-profit entity, conducts a
comprehensive Community
Health Needs Assessment
(CHNA) and Implementation
Strategy in cooperation with
local health departments and
regional health partners every
three years. Holzer completed
its most recent assessment on
June 30, 2016, and subsequent
implementation strategy on
November 15, 2016.
Assessment results of the seven-
county area studied indicate
that obesity, poor nutrition,
and lack of physical activity
remains one of the region’s
most important health issues
leading to chronic disease states
including increased incidence
of cancer. Holzer continued
nutrition efforts to reduce
obesity and increase healthy
eating in 2016 and opened
a new Wellness Center on
November 3, 2016 to encourage
and support healthy lifestyle
behaviors.
DATE EVENT TIME
01/05/16 Diabetes Class - Gallipolis 3 hours
01/29/16 Assessments for Homestead 20 hours
02/09/16 Diabetes Class - Gallipolis 3 hours
02/10/16 Go Red Luncheon 1 hour
02/27/16 Cardiac Symposium 4 hours
03/03/16 Kids Cooking Class 3 hours
03/08/16 Senior Citizen Center presentation 1 hour
03/08/16 Athens Nutrition Month presentation 1 hour
03/10/16 Kids Cooking Class 3 hours
03/15/16 Jackson Diabetes Class 1 hour
03/17/16 Kids Cooking Class 3 hours
03/24/16 Kids Cooking Class 3 hours
03/31/16 Kids Cooking Class 3 hours
04/05/16 Diabetes Class 3 hours
04/13/16 Woodlands presentation 1.5 hours
04/22/16 Rio Grande University Health Fair 5 hours
04/25/16 TOPS presentation - low sodium 3 hours
04/10/16 MNT assessments for Victory House/Homestead 10 hours
05/06/16 GAMS - Middle School Health Fair 2 hours
05/10/16 Diabetes Class - Gallipolis 3 hours
05/10/16 Truancy Class 1 hour
05/12/16 Homestead Menus 6 hours
05/18/16 Breastfeeding Coalition 2 hours
05/24/16 Diabetes Class – Jackson 3 hours
06/16/16 Homestead assessments 8 hours
06/21/16 Cooking Demo Jackosn Library 1 hour
06/24/16 Rocky Boots Health Fair 5 hours
07/07/16 DM Support Group 1 hour
07/12/16 DM class - Gallipolis 3 hours
07/12/16 Children’s Library program - Gallipolis 3 hours
07/14/16 Teen’s Library Program - Gallipolis 3 hours
07/26/16 DM class - Jackson 3 hours
08/09/16 DM Class – Gallipolis 3 hours
08/13/16 Buckeye Rural Health Fair 4 hours
09/08/16 Homestead Assessments 8 hours
09/13/16 Diabetes Class - Gallipolis 3 hours
09/14/16 Gallia High School Career Day 2.5 hours
10/03/16 Diabetes class - Jackson 3 hours
10/06/16 Healthy Men Cooking Demo - with James Center 4 hours
10/11/16 Diabetes Class - Jackson 3 hours
10/11/16 OU Hockey team presentation 1 hour
10/12/16 OVB Health Fair 6 hours
10/17/16 Diabetes class at Woodlands 2 hours20 21

22 23
BREAST AND COLORECTAL CANCER
As part of its Healthy People 2020
initiative, the U.S. Department of Health
and Human Services identified breast
and colorectal cancer screening as
leading health indicators setting a
target of increasing screening rates to
81.1 and 70.5 percent respectively by
the year 2020. These indicators are
relevant because engaging in preventive
behaviors allows for early detection
and treatment of health problems.
This indicator can also highlight a lack
of access to preventive care, a lack of
health knowledge, insufficient provider
outreach, and social barriers preventing
utilization of services. The system’s
CHNA revealed that screening rates
within each of the counties served fall
below HHS targets. Holzer increased its
educational efforts surrounding these
topics, conducted preventative awareness
events in the community and initiated
targeted screening reminder programs
through both face-to-face provider
communication and in-home messaging.
A Colorectal Prevention and Awareness
Event was held on March 29, 2016, in
the Bossard Library Riverside Room in
Gallipolis, OH. Medical Oncologist Dr.
Ghada Kunter provided a presentation
on preventative measures, risk factors,
the importance of screenings, as well
as treatment options after diagnosis.
Holzer chef, Tommy Fallon provided a
healthy eating cooking demonstration
and all in attendance were given a variety
of sample appetizers to enjoy. Sarah
Ramsburg, staff nutritionist, discussed the
importance of healthy eating as a primary
prevention measure. Dr. Kunter asked for
a show of hands to see if the presentation
increased their knowledge about colon
cancer and prevention of the disease. All
acknowledged that their knowledge had
increased as a result of the presentation.
Additionally, two in attendance stated
they had recent colonoscopies, while
five others agreed they would ask their
physicians about scheduling a screening
colonoscopy. Social media activities
surrounding the event resulted in an
additional reach of 809 individuals with
24 actively engaged with the educational
materials.
Holzer staff, in collaboration with the OSU
James Cancer Center, participated in the
annual Komen Race for the Cure event
held in Athens, Ohio on October 23, 2016.
Holzer targeted awareness surrounding
the event resulted in a reach of 1721
individuals with 187 actively engaged in
the educational materials. Additionally,
a targeted breast cancer awareness
article with attached quiz reached 763
individuals with 14 actively engaged
and three taking the quiz to test their
personal knowledge.
LUNG CANCER
Additional primary areas of concern
identified in the CHNA are access to care
and substance abuse including tobacco.
Holzer continues to provide financial
assistance programs as well as low dose
lung CT screenings for high-risk patients.
Holzer completed 100 low-dose lung
CT screenings in 2016 resulting in the
following results:
• HIGHLY SUSPICIOUS: 7 -
Recommendation PET Scan & CT
Guided Biopsy
• SUSPICIOUS: 4 – 1 or more Nodule –
Return in 3 Months
• 1 OR MORE SMALL NODULE: 16 –
Return in 6 Months
• NODULES BUT NOT CONSIDERED
SUSPICIOUS: 34 – Return in 1 Year
• NORMAL: 39 -
25 of screenings were Grant-Funded for
individuals with an inability to pay.
Holzer’s lung cancer coordinator
conducted a feature interview on the
local NBC news, WSAZ Channel 3, on
October 19, 2016, providing awareness,
prevention, and screening information
reaching 68,000 viewers. Social media
awareness during October and November
reached an additional 1905 with 93
actively engaged with the educational
materials. Additionally, a Shine the Light
event to increase awareness of the
dangers of cigarette smoking was held
at the Holzer Center for Cancer Care on
October 12, 2016, with 30 individuals in
attendance.
SKIN CANCER
The Cancer Committee chose skin as the
screening site focus for 2016 as a result
of an increase in Melanoma in the region
and community interest gained from
the CHNA process. Awareness activities
and a skin screening event was held on
November 3, 2016, as part of the grand
opening ceremony of the system’s new
Wellness Center.
19 studies were performed resulting in the
following:
• 4 with at least one seborrheic
keratosis.
• 3 with at least one actinic keratosis.
• 6 with at least one dysplastic nevus.
• 8 biopsies recommended.
• 10 skin cancer pre-tests taken. All
answered the six questions correctly.
Nursing staff conducted followed-up
on the eight recommended biopsies.
Targeted social media awareness in
conjunction with this event reached an
additional 242 individuals with 14 of those
engaged with the related educational
materials.
HOLZER COMMUNITY HEALTH & WELLNESS SCREENING EVENTS
EVENT DATE
Drug Prevention and Resources Monthly Meeting 01/11/16
Wellston High School Health Fair 01/13/16
Vein Screening Event 01/19/16
Vein Screening Event 01/25/16
Holzer Family Pharmacy Wellness Events (all locations) 02/03/16
Drug Prevention and Resources Monthly Meeting 02/08/16
Vein Screening Event 02/09/16
Red Dress Event - Gallipolis 02/11/16
Cardiac Symposium 02/27/16
Drug Prevention and Resources Monthly Meeting 03/07/16
Vein Screening Event 03/08/16
Vein Screening Event 03/08/16
Vein Screening Event 03/08/16
Spring Showcase - Jackson 03/18/16
Colorectal Cancer Event 03/29/16
Meigs Agricultural Society 04/08/16
Vein Screening Event 04/12/16
URG Health Fair 04/22/16
Drug Prevention and Resources Monthly Meeting 05/02/16
Gallia Academy Middle School Health Fair 05/06/16
Vein Screening Event 05/10/16
Drug Prevention and Resources Monthly Meeting 05/30/16
Vein Screening Event 06/14/16
Athens Health Fair 06/17/16
Rocky Boots Health Fair 06/24/16
Drug Prevention and Resources Monthly Meeting 06/27/16
Vein Screening Event 07/12/16
Jackson County Fair 07/18-22/16
Drug Prevention and Resources Monthly Meeting 07/25/16
Gallia County Junior Fair 08/1-5/16
Mason County Fair 08/8-12/16
Buckeye Rural Annual Meeting Health Fair 08/13/16
Meigs County Fair 08/15-19/16
Drug Prevention and Resources Monthly Meeting 08/22/16
Vein Screening Event 09/13/16
Emancipation Celebration 09/18-19/16
Drug Prevention and Resources Monthly Meeting 09/19/16
Apple Festival 09/20-24/16
Athens Kid and Safety Fair 10/01/16
OVB Health Fair 10/12/16
Drug Prevention and Resources Monthly Meeting 10/17/16
Skin Cancer Screening - Wellness Center Opening 11/03/16
Drug Prevention and Resources Monthly Meeting 11/14/16
Drug Prevention and Resources Monthly Meeting 12/12/16

PALLIATIVE
CARE
Palliative Care focuses on relieving and
preventing the suffering of patients.
Palliative care specializes in the relief
of the pain, symptoms and stress of
serious illness.
Palliative care is given to improve the
quality of life of patients who have a
serious or life-threatening disease, such
as cancer. The goal of palliative care is
to prevent or treat, as early as possible,
the symptoms and side effects of the
disease and its treatment, in addition
to the related psychological, social,
and spiritual problems. The goal is not
to cure. Palliative care is also called
comfort care, supportive care, and
symptom management.
Palliative medicine
is appropriate for
patients in all disease
stages, including
those undergoing
treatment for curable
illnesses and those
living with chronic
diseases, as well as
patients nearing the end of life.
This can include treating nausea related to
chemotherapy, morphine to treat the pain
of broken leg, or ibuprofen to treat aching
related to an influenza (flu) infection.
Palliative medicine at Holzer utilizes a
multidisciplinary approach to patient
care, relying on input throughout our
healthcare system, including physicians,
pharmacists, nurses, chaplains, social
workers, and Hospice to create a plan of
care to relieve suffering in all areas of life.
This multidisciplinary approach allows the
palliative care team to address physical,
emotional, spiritual and social concerns
that arise with advanced illness.
The Palliative Care Team plans to provide
both effective inpatient and outpatient
management of patients with serious,
potentially life threatening illness
independent of curative or life-prolonging
care. The primary focus is placed on
pain and symptom control, psychosocial
distress, spiritual issues and practical
needs. Additionally, our desire is to be
very informative so that patients and their
families can fully understand the illness,
prognosis and treatment options and then
work from that knowledge in establishing
goals of care. Knowledge, understanding
and compassion are key foundational
concepts for the success of Palliative Care.
HOW DO I KNOW IF PALLIATIVE CARE IS RIGHT FOR ME?
Palliative care may be right for you if
you suffer from pain or other symptoms
due to a serious illness. Serious illnesses
include but are not limited to:
• Cancer
• Cardiac disease
• Respiratory disease
• Kidney failure
• Alzheimer’s
• AIDS
• Amyotrophic Lateral Sclerosis
(ALS)
• Multiple Sclerosis
Palliative care can be utilized at any stage
of illness and alongside curative treatment.
WHAT CAN I EXPECT FROM PALLIATIVE CARE?
When you receive palliative care you can
expect relief from distressing symptoms
such as pain, shortness of breath, fatigue,
constipation, nausea, loss of appetite
and difficulty sleeping. Palliative care
improves your ability to carry on with
your daily life. It improves your ability to
tolerate medical treatments and helps
you to better understand your condition
and your choices for medical care. In
short, you can expect the best possible
quality of life.
COMMON INDICATIONS FOR PALLIATIVE CARE
Some of the more common indications
for palliative care consultation include:
• Intractable symptom (pain,
nausea, depression, etc.)
management associated with
end stage or serious illness,
• Discussing goals of treatment/care
and prognosis, and assistance with
coordination of care,
• Patients who have frequent
readmissions to the acute care
setting can often benefit from
palliative care consultation
especially when a progressing
illness such as COPD, CHF or
advanced renal disease are the
culprit. Complex family system
dynamics often create situations
in which palliative care can be
beneficial as well.
PALLIATIVE CARE & CANCER
Palliative care is given throughout a
patient’s experience with cancer. Our
palliative care nurse, Teresa Stewart,
RN, CHPN, meets with each patient at
diagnosis and continues through treatment,
follow-up care, and the end of life.
Palliative care is provided in addition
to cancer treatment. However, when
a patient reaches a point at which
treatment to destroy the cancer is no
longer warranted, palliative care becomes
the total focus of care. Palliative care will
be continued to alleviate the symptoms
and emotional issues of cancer. Palliative
care providers can help ease the
transition to end-of-life care.
PALLIATIVE CARE & CANCERFAMILY CARE
It’s common for family members to
become overwhelmed by the extra
responsibilities placed upon them.
Palliative care can help families and
friends cope with these issues and
provide the support needed.
24 25

26 27
CASES DIAGNOSED IN 2016: Description of top sites compared to Ohio & National
HCCC PERCENTAGE OHIO PERCENTAGE NATIONAL PERCENTAGE
Lung/Bronchus 62 20.8% 10,550 16.0% 224,390 13.5%
Breast 45 15.1% 9,390 14.2% 246,660 14.8%
Colorectal 31 10.8% 5,430 8.2% 134,490 8.1%
Prostate 22 7.4% 6,760 10.2% 180,890 10.9%
Uterine Corpus 21 7.0% 2,640 4.0% 60,050 3.6%
Leukemia 18 6.0% 2,140 3.3% 60,140 3.6%
Lymphoma 13 4.3% 2,820 4.2% 72,580 4.4%
Bladder 11 3.6% 3,180 4.8% 76,960 4.7%
Melanoma of Skin 10 3.3% 2,880 4.4% 76,380 4.6%
Uterine Cervix 5 1.7% 470 0.7% 12,990 0.8%
All Others 60 20.0% 19,760 30.0% 512,680 31.0%
TOTALS: 300 100.0% 66,020 100.0% 1,658,210 100.0%
An estimated 1,658,210 new cancer cases have occurred nationally in 2016. The state of Ohio is estimated at 66,020. Holzer
Center for Cancer Care (HCCC) had 300 cases for the year. The incidence rate continues to decline for men and is about the
same among women after a long period of increase. Holzer was 7.3% above the national level for lung, our top site, and about
the same as national for breast, our second-highest site. The other selected sites were relatively comparable to the state and
national averages. Prostate was 3% below the national average, Leukemia was 2.4% above the national average, Uterine was
3.4% above the national average, and colorectal was 2.7% above the national average.
HCCC SITE DISTRIBUTION DATA ILLUSTRATION FOR DIAGNOSIS: YEAR 2016
Other Head & Neck: 5.4%
Brain: 1.0% Brain: 0%
Lung & Bronchus: 25.2%
Breast: 2.2%
Digestive System: 23.6%
Urinary System: 6.1%
Reproductive System: 19.1%
Lymph Nodes: 3.8%
Melanoma of the Skin: 3.8%
Blood/Bone Marrow: 7.6%
All Other Sites: 2.2%
TOTAL: 131 Cases
Lung & Bronchus: 19.2%
Breast: 25.1%
Digestive System: 13.8%
Urinary System: 5.9%
Reproductive System: 18.0%
Lymph Nodes: 4.8%
Melanoma of the Skin: 3.0%
Blood/Bone Marrow: 4.8%
All Other Sites: 1.2%
TOTAL: 169 Cases
Other Head & Neck: 3.6%

2016 NATIONAL
COMPARISON
OF ESTIMATED
TOP CANCER
SITES
PRIMARY SITE CASES PERCENT
Bronchus & Lung 30 35.7%
Prostate 22 26.2%
Colorectal 15 17.9%
Blood / Bone Marrow
10 11.9%
Esophagus 7 8.3%
Total 84 100%
PRIMARY SITE CASES PERCENT
Breast 42 30.9%
Bronchus & Lung 32 23.5%
Reproductive Sites 30 22.1%
Colorectal 16 11.7%
Blood/BM 8 5.9%
Lymph Nodes 8 5.9%
Total 120 100%
TOP SITES FOR MEN TOP SITES FOR WOMEN
28 29

Lung cancer was the leading cause
of cancer death in Ohio in 2013,
representing 29.1 % of all cancer
deaths, followed by colorectal
(9.0%), breast cancer (7.2%) and
pancreatic cancer (6.2%). The good
news is that the lung and bronchus
cancer incidence rate for Ohio males
declined 19% and mortality rates
declined 21% from 2004 to 2013. The
lung and bronchus cancer incidence
rate among Ohio females declined 5%
from 2004 to 2013 In Ohio, between
2008 and 2014, 95% of individuals
who developed lung and bronchus
cancer were age 50 and over.
African American men are about
20% more likely to develop and die
from lung cancer than white men,
even though their overall exposure to
cigarette smoke, the primary risk factor
for lung cancer, is lower. About 50% of
Ohio lung and bronchus cancer cases
were diagnosed at a distant stage
in Ohio in 2013, where the five-year
relative survival probability is only 4%.
It is estimated that approximately $10.3
billion per year is spent in the United
States on lung cancer treatment with
an estimated number of lung cancer
deaths at 160,000 for 2014.
One reason malignant tumors are
dangerous is because they grow
uncontrollably. When the cancer cells
grow too fast, they prevent organs
of the body from working well. For
example, if cancer affects the lungs,
the tumor may grow so large it blocks
a major airway so that part of the lung
can’t breathe.
Another reason a cancerous tumor
is dangerous is because it can
spread to different parts of the body.
Sometimes a cancerous tumor sheds
cells. These cells can be carried to
other parts of the body through the
blood or the natural fluid around the
lung tissue called lymph. The cells
can begin to grow uncontrollably in
the new location and cause problems
that keep that part of the body from
working properly.
There are two main types of lung
cancer: small cell lung cancer (SCLC)
and non-small cell lung cancer
(NSCLC). Non-small cell lung cancer
is more common. It makes up about
80% of lung cancer cases. This type of
cancer usually grows and spreads to
other parts of the body more slowly
than small cell lung cancer does. There
are three different types of non-small
cell lung cancer: adenocarcinoma,
squamous cell carcinoma and large cell
carcinoma. Each type is different, but
they are grouped together because
they are treated similarly. Small cell
lung cancer is almost always associated
with cigarette smoking. It is important
to know the type of lung cancer you
have because it helps determine what
treatment options are available.
The five-year survival rate for lung
cancer is 53.5% for cases detected
when the disease is still localized
(within the lungs). However, only 15% of
lung cancer cases are diagnosed at an
early stage. For distant tumors (spread
to other organs) the five-year survival
rate is only 3.9%.
TREATMENT OVERVIEW FOR NON-SMALL CELL LUNG CANCER (NSCLC)
In cancer care, different types of
doctors often work together to
create a patient’s overall treatment
plan that combines different types
of treatments. Cancer care teams
include a variety of other health
care professionals, such as physician
assistants, oncology nurses, social
workers, pharmacists, counselors,
dietitians, and others.
There are 5 basic ways to treat NSCLC:• Surgery• Radiation therapy• Chemotherapy• Targeted therapy• lmmunotherapy
Treatment options and
recommendations depend on several
factors, including the type and stage
of cancer, possible side effects, and the
patient’s preferences and overall health.
SURGERY
A thoracic surgeon is specially trained
to perform lung cancer surgery. The
goal of surgery is to completely remove
the lung tumor and the nearby lymph
nodes in the chest. The tumor must be
removed with a surrounding border or
margin of healthy lung tissue.
The following types of surgery may be
used for NSCLC:• LOBECTOMY. The lungs have 5
lobes, 3 in the right lung and 2
in the left lung. The removal of
an entire lobe of the lung in a
procedure called a lobectomy is
currently thought to be the most
effective type of surgery, even when
the lung tumor is very small.
SITE OF
FOCUS
Lung Cancer
Currently, a man living in the U.S. has a
1 in 15 lifetime risk of developing invasive
lung and bronchus cancer, and a woman
has a 1 in 18 lifetime risk of developing
invasive lung and bronchus cancer
(ACS’ Cancer in Ohio 2016). Lung and
bronchus cancer was the leading cause
of cancer incidence in Ohio in 2016,
representing 15.2% of all new invasive
cancer cases, followed by breast cancer
(14.7%), prostate cancer (11.0%), and
colon and rectum cancer (9.0%).
30 31

intravenous (IV) tube placed into a vein
using a needle or in a pill or capsule
that is swallowed (orally). Most types of
chemotherapy used for lung cancer are
given by IV injection.
A chemotherapy regimen , or schedule,
usually consists of a specific number of
cycles given over a set period of time.
The type of lung cancer you have, such
as adenocarcinoma or squamous cell
carcinoma, affects which drugs are
used for chemotherapy.
Chemotherapy may also damage
healthy cells in the body, including
blood cells, skin cells, and nerve cells.
The side effects of chemotherapy
depend on the individual and the dose
used, but they can include fatigue,
low numbers of blood cells, risk of
infection, mouth sores, nausea and
vomiting, loss of appetite, diarrhea,
numbness and tingling in the hands
and feet, and hair loss. Your medical
oncologist can often prescribe drugs
to help relieve many of these side
effects. Hormone injections are
used to prevent white and red blood
cell counts from becoming too low.
Nausea and vomiting are also often
avoidable. These side effects usually
go away after treatment is finished.
TARGETED THERAPY
Targeted therapy is a treatment that
targets the cancer’s specific genes,
proteins, or the tissue environment
that contributes to cancer growth and
survival. This type of treatment blocks
the growth and spread of cancer cells
while limiting damage to healthy cells.
Recent studies show that not all tumors
have the same targets. For some lung
cancers, abnormal proteins are found
in unusually large amounts in the
cancer cells. This helps doctors better
match each patient with the most
effective treatment whenever possible.
In addition, many research studies
are taking place now to find out more
about specific molecular targets and
new treatments directed at them.
For NSCLC, the following types
of targeted therapy may be used,
particularly in clinical trials. Talk with
your doctor about possible side effects
for a specific medication and how they
can be managed.
• ANTI-ANGIOGENESIS THERAPY.
Anti-angiogenesis therapy is
focused on stopping angiogenesis,
which is the process of making new
blood vessels. Because a tumor
needs the nutrients delivered by
blood vessels to grow and spread,
the goal of anti-angiogenesis
therapies is to “starve” the tumor.
• EPIDERMAL GROWTH FACTOR
RECEPTOR (EGFR) INHIBITORS.
Researchers have found that drugs
that block EGFR may be effective
for stopping or slowing the growth
of lung cancer.
• DRUGS THAT TARGET OTHER
GENETIC CHANGES. Researchers
have found that targeting other
genetic changes in lung tumors
may help stop or slow the growth
of NSCLC. An example is anaplastic
lymphoma kinase (ALK) inhibitors.
Mutations in the ALK gene are
found in about 5% of patients with
NSCLC. Another example are drugs
that target changes in a gene called
ROS1.
IMMUNOTHERAPY
lmmunotherapy is designed to boost
the body’s natural defenses to fight the
cancer. It uses materials made either by
the body or in a laboratory to improve,
target, or restore immune system
function.
GETTING CARE FOR SYMPTOMS AND SIDE EFFECTS
Cancer and its treatment often
cause side effects. In addition to
treatments intended to slow, stop, or
eliminate the cancer, an important
part of cancer care is relieving a
person’s symptoms and side effects.
This approach is called palliative
or supportive care, and it includes
supporting the patient with his or her
physical, emotional, and social needs.
Palliative care is any treatment that
focuses on reducing symptoms,
improving quality of life, and
supporting patients and their families.
Any person, regardless of age or type
and stage of cancer, may receive
palliative care. It works best when
palliative care is started as early
as needed in the cancer treatment
process. People often receive
treatment for the cancer at the same
time that they receive treatment to
ease side effects. In fact, patients who
receive both at the same time often
have less severe symptoms, better
quality of life, and report they are
more satisfied with treatment.
• A WEDGE RESECTION. If the
surgeon cannot remove an entire
lobe of the lung, the surgeon can
remove the tumor, surrounded by a
margin of healthy lung.
• SEGMENTECTOMY. This is another
way to remove the cancer when an
entire lobe of the lung cannot be
removed. In a segmentectomy, the
surgeon removes the portion of the
lung where the cancer developed.
• PNEUMONECTOMY. If the tumor is
close to the center of the chest, the
surgeon may have to remove the
entire lung.
ADJUVANT THERAPY
“Adjuvant therapy” is treatment that
is given after surgery to lower the risk
of the lung cancer returning. Adjuvant
therapy may include radiation therapy,
chemotherapy, targeted therapy,
or immunotherapy. Each therapy is
described below. It is intended to get
rid of any lung cancer cells that may
still be in the body after surgery. It
also helps lower the risk of recurrence,
though there is always some risk that
the cancer will come back.
RADIATION THERAPY
Radiation therapy is the use of high
energy x-rays or other particles to
destroy cancer cells. If you need
radiation therapy, you will be asked
to see a specialist called a radiation
oncologist. A radiation oncologist is
the doctor who specializes in giving
radiation therapy to treat cancer.
The most common type of radiation
treatment is called external-beam
radiation therapy, which is radiation
given from a machine outside the
body. A radiation therapy regimen, or
schedule, usually consists of a specific
number of treatments given over a
set period of time. This can vary from
just a few days of treatment to several
weeks.
Like surgery, radiation therapy cannot
be used to treat widespread cancer.
Radiation therapy only destroys
cancer cells directly in the path of
the radiation beam. It also damages
the healthy cells in its path. For this
reason, it cannot be used to treat
large areas of the body.
SIDE EFFECTS OF RADIATION THERAPY
Patients with lung cancer who receive
radiation therapy often experience
fatigue and loss of appetite. If radiation
therapy is given to the neck or center of
the chest, patients may develop a sore
throat and have difficulty swallowing.
Patients may notice skin irritation,
similar to sunburn, where the radiation
therapy was directed. Most side effects
go away soon after treatment is
finished.
If the radiation therapy irritates or
inflames the lung, patients may develop
a cough, fever, or shortness of breath
months and sometimes years after
the radiation therapy ends. About 15%
of patients develop this condition,
called radiation pneumonitis. If it is
mild, radiation pneumonitis does not
need treatment and goes away on its
own. If it is severe, a patient may need
treatment for radiation pneumonitis
with steroid medications.
CHEMOTHERAPY
Chemotherapy is the use of drugs to
destroy cancer cells, usually by ending
the cancer cells’ ability to grow and
divide. It has been shown to improve
both the length and quality of life for
people with lung cancer of all stages.
Chemotherapy is given by a medical
oncologist, a doctor who specializes in
treating cancer with medication.
Systemic chemotherapy gets into the
bloodstream to reach cancer cells
throughout the body. Common ways
to give chemotherapy include an
33

LOW-DOSE CT
SCREENING
FOR
LUNG CANCER
While cigarette smoking rates in the
United States have steadily decreased
over the past 50 years, lung cancer still
remains the leading cause of cancer
deaths in both men and women,
especially in our tristate area. Every
year we lose more people to lung
cancer than breast, colon and prostate
cancers combined. BUT, we at Holzer are
changing all of that!
REQUIREMENTS FOR
THE LOW-DOSE CT
LUNG CANCER
SCREENING:
Individuals must be
55-77 years old
Individuals must be a
current smoker with a
history of smoking 2
packs per day for 15
years or one pack per
day for 30 years
or
Individuals must be
an ex-smoker who has
quit smoking within
the past 15 years
Holzer Health System now offers a service called Low-Dose CT Screening
for Lung Cancer. Low-Dose CT Screening is basically a CAT Scan using
a lower dosage of radiation to look for nodules in the lungs. It’s a test to
check for disease in someone who does not have any symptoms. According
to the National Cancer Institute, scientists have found a 20% reduction in
deaths from lung cancer among current or former heavy smokers when
screened with Low-Dose CT versus those screened by chest x-ray. CT
Scanning provides detailed, cross-sectional pictures of the lungs that let us
see very small nodules very closely.
The criteria to be eligible for screening are: Patients between the ages of 55-77;
have a 30 pack-year of smoking; or have quit within the last 15 years.
In the year 2016 we completed Low-Dose CTs on 116 patients with a percentage
rate of 30% of these patients having an abnormal outcome. The goal of
screening is to find cancer early when it is more treatable and even curable.
The screening itself is quick and painless; the scan is done while the patient
holds his breath for 5 to 10 seconds and its noninvasive, no contrast dye is
administered and no IV is required. The radiation dose is extremely low, less
than one-fifth of a routine chest CT Scan. The cost of the screening is $100. We
currently have funding provided by a Grant from Whedon Cancer Institute to
off-set this cost if the patient qualifies. We provide this service at our Gallipolis
and Athens locations.
We had a community awareness event called Shine A Light on Tuesday,
November 1, 2016 at the Holzer Center for Cancer Care. The goal of the Shine A
Light Event was to create more awareness and education on lung cancer in our
community. Our featured speaker, David Clagg, is walking proof that the Holzer
Low-Dose CT Program works.
34 35

PATIENT STORY
Holzer Staff, Community Shine Awareness on Lung Cancer
Holzer offered the Shine a Light
on Lung Cancer event on Tuesday,
November 1, at the Holzer Center for
Cancer Care. Shine a Light is the largest
coordinated awareness event for lung
cancer in the United States.
“Cancer changes how you spend
your time. It changes what tomorrow
means. But there is hope,” stated Sandy
Thomas, Program Coordinator, Low-Dose
CT Scan, Holzer Health System. “We are
not promised tomorrow, but with the
technology and advances of healthcare
through the utilization of our program,
we are able to offer hope to individuals
when it is needed most. The goal of the
Shine A Light event is to create even
more awareness and education on lung
cancer in our communities.”
The event featured guest speaker
Ghada Kunter, MD, Radiation Oncology,
Holzer Center for Cancer Care, and Candy
Bowers, who shared the story of her
father, David Clagg, a former patient of
the Holzer Low-Dose CT Scan Program.
“As a physician, I hope to cure every
patient,” stated Dr. Kunter. “It is crucial
to increase awareness in our area. I see
many patients who have smoked from a
very young age. Through events like this,
we are able to shine a light for those who
have passed and those who are currently
fighting cancer.”
“My dad was a smoker from his teens,
and actually quit 10 years ago,” shared
Bowers. “He was the walking definition
of high-risk for lung cancer, but has
always been relatively healthy. He had
no symptoms and through the years, his
numbers always came back in the good
category. We spoke to his Family Practice
Physician about the screening, and since he
fit the qualifications, he agreed to have it.”
In October 2015, Clagg had a Low-Dose
CT Scan at Holzer in Gallipolis. The scan
results warranted a referral to The James
Cancer Center in Columbus, Ohio. “I had
the scan just to appease everyone,” said
Clagg. “I didn’t feel bad, my appetite was
good, I had no symptoms of lung cancer
yet. However, early detection is the key.”
“They removed a tumor from Dad’s
lung. It took three months to reach full
recovery. In October of 2016, he received
an all clear for the year,” commented
Bowers. “Dad is still here because of this
screening tool. Lung cancer does not
have to be a death sentence. My family
and I firmly believe that God had his
hands in this from the beginning. We
are here to share his story to make a
difference in someone’s life.”
According to the Lung Cancer Alliance,
lung cancer causes more deaths each
year than breast, prostate, colon and
pancreatic cancers combined. Nearly 80
percent of those diagnosed are former or
non-smokers. Unfortunately, lung cancer
receives the least amount of research
dollars of all major cancers.
For more information, call 740-441-
3905 or visit www.holzer.org.
Sandy Thomas, Program Coordinator, Low-Dose CT Scan, Holzer Health System
“CANCER CHANGES HOW YOU
SPEND YOUR TIME. IT CHANGES
WHAT TOMORROW MEANS. BUT
THERE IS HOPE. WE ARE NOT
PROMISED TOMORROW, BUT WITH
THE TECHNOLOGY AND ADVANCES
OF HEALTH CARE THROUGH THE
UTILIZATION OF OUR PROGRAM,
WE ARE ABLE TO OFFER HOPE TO
INDIVIDUALS WHEN IT IS NEEDED
MOST. THE GOAL OF THE SHINE
A LIGHT EVENT IS TO CREATE
EVEN MORE AWARENESS AND
EDUCATION ON LUNG CANCER IN
OUR COMMUNITIES.”
Shown pictured is David Clagg, center, Holzer Low-Dose CT Scan former patient, and his family during the recent Shine A Light on Lung Cancer Awareness Event. Clagg and his daughter, Candy Bowers, second from right, who is also a Holzer employee, shared their story as part of the evening’s program.
INSET Photo: Ghada Kunter, MD, Hematology, Oncology, Holzer Center for Cancer Care, speaks during the Shine a Light on Lung Cancer event.
36 37

38 39
Treatment options are determined by the type (Small Cell & Non-Small Cell)
and stage of the cancer. Treatments include: surgery, radiation therapy,
chemotherapy, and targeted biologic therapies such as Avastin, Tarceva, and
Xalkori. For localized cancers, surgery is usually the treatment of choice and
is improved by chemotherapy following surgery for non-small cell tumors.
Because the disease has usually spread by the time it is discovered, radiation
therapy and chemotherapy are often used, sometimes in combination with
surgery. Advanced-stage non-small cell lung cancers are usually treated
with chemotherapy, targeted drugs, or some combination of the two.
Chemotherapy alone or combined with radiation is the usual treatment of
choice for Small Cell Lung Cancer; on this regimen, a large percentage of
patients experience remission, although, the cancer often returns.
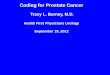
HISTOLOGY NBR_CASES
Small Cell Carcinoma
15
Non-Small Cell Carcinoma
47
TOTAL CASES 62
HISTOLOGY Distribution2016 Lung Cases by Histology
As previously stated, the two types of lung cancer are Small Cell (SCLC) and Non-Small Cell (NSCLC). Non-small
cell lung cancer usually grows and spreads to other parts of the body more slowly than small cell lung cancer.
There are three different types of Non-Small Cell Lung Cancer: Adenocarcinoma, Squamous Cell Carcinoma and
Large Cell Carcinoma. Each type is different, but they are grouped together because they are treated similarly.
Small cell lung cancer is almost always associated with cigarette smoking. It is important to know the type of lung
cancer you have because it helps determine what treatment options are available.
Rx TYPE # of CASES
No Treatment 23
Chemo/Rad 11
Chemo only 9
Radiation only 7
Surgery/Chemo 5
Surgery only 3
Surgery/Chemo/Rad 2
Surgery/Rad 2
TOTAL CASES 62
Treatment Combination2016 Lung Cases by Treatment
2016 LUNG
CASES
FOR
HOLZER
TREATMENT
No Treatment
Chemo/Rad
Chemo only
Radiation only

In Ohio, between 2006 and 2010, 95% of individuals who developed lung and bronchus cancer were age 50 and older. In 2016, HCCC
shows a rate of 99.9%.
There are more women diagnosed with stage 1 lung cancer. Lung and Bronchus cancer is more common in men than women. For
Holzer patients in 2016, 46% were women and 54% were men.
AGE RANGE MALE FEMALE
40-49 1 1
50-59 3 4
60-69 11 11
70-79 9 12
80-89 6 4
TOTALS 30 32
Lung Cases by Age & Sex
STAGE MALE FEMALE
I 3 6
II 5 0
III 8 11
IV 14 14
UNK 0 1
TOTALS 30 32
AJCC Stage by Sex2016 Lung Cases by Sex by Stage
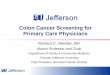
HCCC covers a broad geographical area. Counties represented
in 2016 were Gallia, Meigs, Jackson, Vinton, Ohio, and Mason
County, West Virginia.
Diagnosis County Distribution2016 Lung Cases by County
DIAGNOSIS COUNTY CASES
Gallia 28
Meigs 12
Jackson 9
Mason County, WV 9
Athens 2
Vinton 2
TOTALS 62
COUNTIES
Mason County
West Virginia
40 41
12
5
34
1. Gallia2. Jackson3. Meigs4. Athens5. Lawrence

170JacksonPike•Gallipolis,Ohio1.855.4HOLZER (1.855.446.5937)
www.holzer.org
On behalf of Holzer and its Cancer Committee, we want to thank our awesome community
members for your generous and steadfast support for the past 80 years. Together we will
continue to grow and develop expertise in broader and more sophisticated treatments and
support our patients and their families in the fight against cancer.
Dr. Alice Dachowski, Cancer Liaison Physician