Embed Size (px)
Citation preview
Hospice Care in Hospital: A Resource Dependence and Institutional Perspective
BIOS524Hsueh-Fen Chen
12/09/03

Introduction (I)
The Importance of this research The demand of hospice care
increased Not a high profit service for hospitals Hospices focus on caring; hospitals
focus on curing and discharging patients quickly.

Introduction (II)
Hospitals face technical environment and institutional environment.
Hospitals pursue autonomy and legitimacy.

Research Question
What economic and non-economic factors influence hospitals to engage in hospice care?

The Purpose of this Research
To understand the dynamics of the underlying organizational behavior.
To add the knowledge of macro-level organizational theories.

Literature Review (I) Resource dependence theory:
organizations survive dependent upon the extent to which they effectively manage their environmental demands, or acquire and maintain vital resources (Pfeffer and Salancik, 1978).
The types of resource are important resource, scarce resource, and resource capacity.

Literature Review (II) Institutional theory: organization’s behaviors
shaped by myth and irrationality (Scott, 2002). Organizations compete not just for resources,
but for political power and institutional legitimacy.
Through isomorphism mechanisms, coercive; mimetic, and normative isomorphism, organizations become legitimate and use their legitimacy to enhance their success and survival(Meyer, & Rowan, 1991; DiMaggio & Powell, 1991).
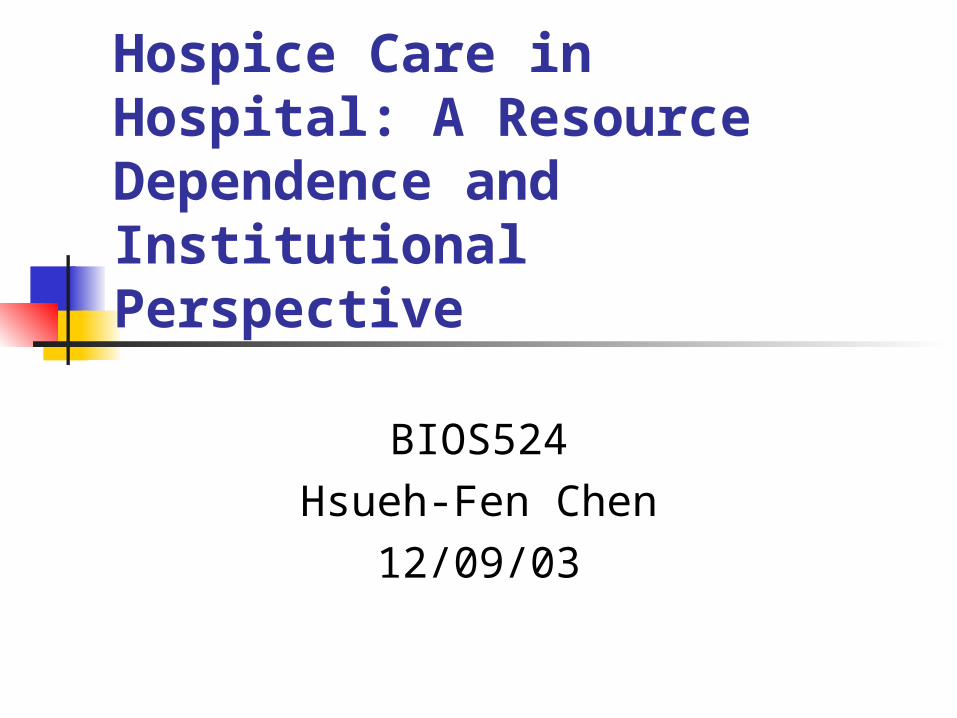
Theoretical Framework
Resource dependency theory Important resource Resource scarcity *Resource capacity -hospital size
Institutional theory Coercive pressure Professional pressure*Normative pressure -ownership
Hospice adoption

Hypotheses
H1: Hospitals with large size are more likely to employ vertical integration in providing hospice service than small hospitals. large hospitals have more
resource.
Hypotheses H2: Not-for-profit hospitals are
more likely to employ a higher degree of vertical integration in providing hospice service than profit hospitals. Not-for profit hospitals meet the
stakeholders’ expectation. For-profit hospital meet the
shareholders’ expectation.

Methods Research Design: cross-sectional
research. Population: non-government, and non-
federal hospitals. Research time frame: 1996-1998. Unit of analysis: hospital. Statistical analysis: descriptive and
logistic regression. Statistical software: SAS window 8.2.

Data source & measurement
Data source ARF: population & market characteristics
AHA: hospital characteristics link: link between AHA & PPS PPS: hospital financial report
Measurement: see handout
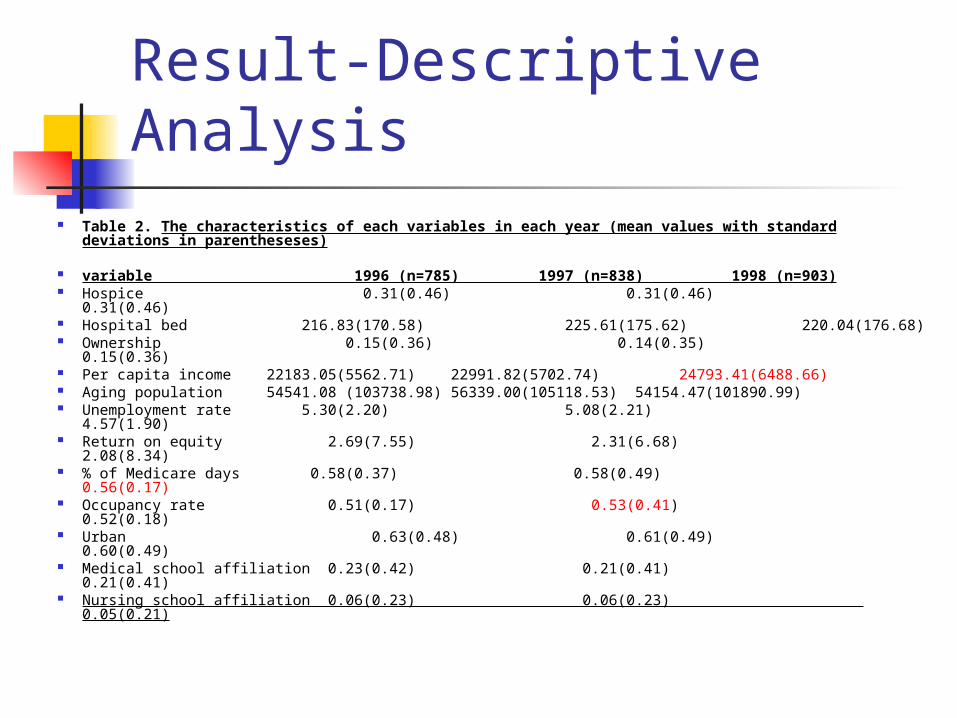
Result-Descriptive Analysis Table 2. The characteristics of each variables in each year (mean values
with standard deviations in parentheseses)
variable 1996 (n=785) 1997 (n=838) 1998 (n=903) Hospice 0.31(0.46) 0.31(0.46) 0.31(0.46) Hospital bed 216.83(170.58) 225.61(175.62)
220.04(176.68) Ownership 0.15(0.36) 0.14(0.35) 0.15(0.36) Per capita income 22183.05(5562.71) 22991.82(5702.74)
24793.41(6488.66) Aging population 54541.08 (103738.98) 56339.00(105118.53)
54154.47(101890.99) Unemployment rate 5.30(2.20) 5.08(2.21) 4.57(1.90) Return on equity 2.69(7.55) 2.31(6.68) 2.08(8.34) % of Medicare days 0.58(0.37) 0.58(0.49) 0.56(0.17) Occupancy rate 0.51(0.17) 0.53(0.41) 0.52(0.18) Urban 0.63(0.48) 0.61(0.49) 0.60(0.49) Medical school affiliation 0.23(0.42) 0.21(0.41) 0.21(0.41) Nursing school affiliation 0.06(0.23) 0.06(0.23) 0.05(0.21)
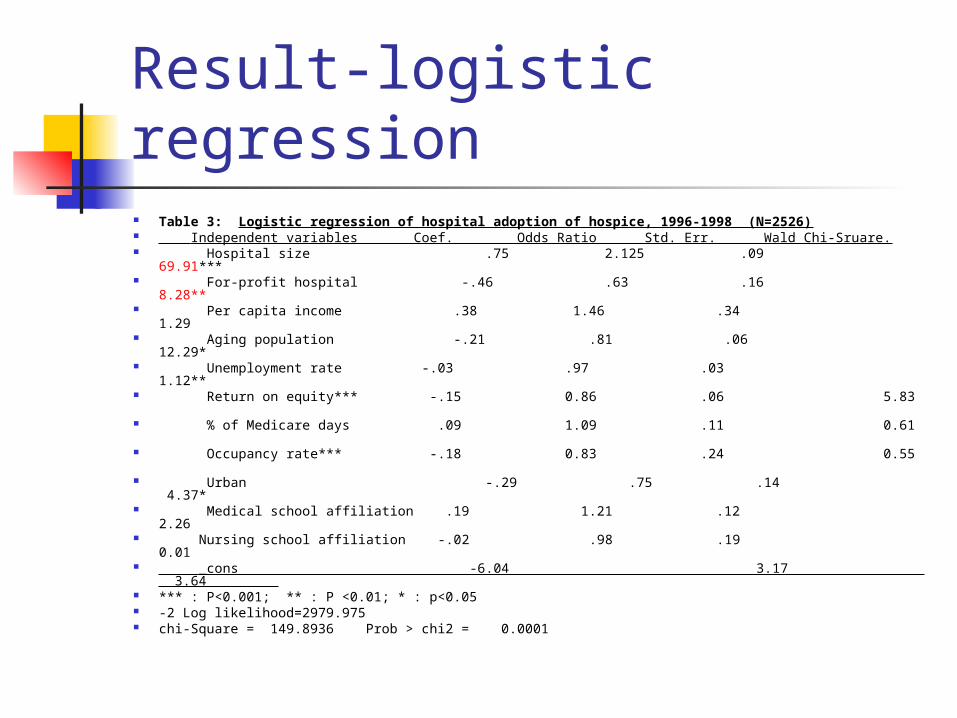
Result-logistic regression Table 3: Logistic regression of hospital adoption of hospice, 1996-1998
(N=2526) Independent variables Coef. Odds Ratio Std. Err. Wald Chi-
Sruare. Hospital size .75 2.125 .09 69.91***
For-profit hospital -.46 .63 .16 8.28** Per capita income .38 1.46 .34 1.29 Aging population -.21 .81 .06 12.29* Unemployment rate -.03 .97 .03 1.12** Return on equity*** -.15 0.86 .06 5.83 % of Medicare days .09 1.09 .11 0.61 Occupancy rate*** -.18 0.83 .24 0.55 Urban -.29 .75 .14 4.37* Medical school affiliation .19 1.21 .12 2.26 Nursing school affiliation -.02 .98 .19 0.01 _cons -6.04 3.17 3.64 *** : P<0.001; ** : P <0.01; * : p<0.05 -2 Log likelihood=2979.975 chi-Square = 149.8936 Prob > chi2 = 0.0001
Discussion and Implication.
The results in this study strongly support these two hypotheses. Size and hospice adoption
More resource Not-for proit vs. for profit
The expectation of stakeholders vs. of shareholders

Discussion and implication Expected outcome of variables
The coefficient of unemployment (-) The coefficient of per capita income (+) The coefficient of Medicare inpatient days
(+). The coefficient of occupancy rate (-). The coefficient of urban (-) The coefficient of Medical school affiliation
(+)
Discussion and implication
Unexpected outcome of variable Aging population (-): People over 65
years might not a good indicator. Return on equity (-): Nursing school affiliation (-)

Limitations and further research
Younger aging people and older aging people.
The quality of data Extended the research time frame:
most hospice adoption before 1996.
Reference Aldrich, H. (1979). Chapter 12: Managing interdependence through interorganizational
relations, Organizations and Environments (pp.292-322): Prentice Hall. Banaszak-Holl, J., Zinn, J., Mor, J. S. (1996). The impact of market and organizational
characteristics on nursing care facility service innovation: A Resource Dependence Perspective. Health Services Research, 31(1), 97-117.
Chiu, H. C. (1995). The linkage between hospitals and nursing homes: alternative pproaches to minimizing transaction costs. Dissertation in Department of Health Administration in VCU.
DiMaggio, P. J. & Powell, W. W. (1991). Chapter 3: the iron cage revisited: institutional isomorphiam and collective rationality in organization fields. In Powell, W. W. & DiMaggio, P. J (Eds.), The New Institutionalism in organizational Analysis (pp.63-82). Chicago: the University of Chicago.
Freund, R. J. & Littell, R. C. (2000, 3ed.). SAS System for Regression. NC:” Cary. Luke, R. D. & Walston, S. L. (2003). Strategy in an Institutional Environment: Lessons learned
from the 1990s “revolution” in health care. In Mick, S. S. & Wyttenbach, M. E. (Eds.), Advances in Health Care Organization Theory (pp289-323). CA, San Fransico: Jossey-Bass.
Meyer, J. W. and Rowan, B. (1991). Chapter 2: Institutionalized organizations: formal structure
as myth and ceremony. In Powell, W. W., and DiMaggio, P. J.(Eds.), The New Institutionalism in Organizational Analysis (pp 41-62). Chicago: the University of Chicago.
National Hospice and Palliative Care Organization (2002). National Trend Summary, 1-13. Proenca, E. J., Rosko, M. D. & Zinn, J. S. (2000). Community orientation in hospitals: as
institutional and resource dependence perspective. Health services research, 35(5), 1011-1035.

Reference Shah, A., Fennell, M., and Mor, V. (2001). Hospital diversification into long-term
care. Health Care Management Review/summer, 86-100. Snail, T. S. & Robinson, J. C. (1998). Organizational diversification in the
American hospital. Annual Review of Public Health, 19, 417-53. Scott, W. R. (2002). Organiations: rational, natural, and open system. Englewood
Cliffs, New Jersey: Prentice Hall. Tabachnick, B. G. & Fidnell, L. S. (2001, 4ed.). Using multivariate statistics. MA :
Allyn & Bacon. Westphal, J. D., Gulati, R., & Shortell, S. M. (1997). Customization or conformity?
An institutional and network perspective on the content and consequences of TQM adoption. Administrative Science Quartely, 42, 366-394
Wheeler, J. R. C., Burkhardt, J., Alexander, J. A., & Magnus, S. A. (1999). Financila and organizational determinants of hospital diversification into subacute care. Health Services Research, 34(1), 61-81.
White, K. R., Cochran, C. E., & Patel, U. B. (2002). Hospital provision of end of life services who, what, and where? Medical Care 40(1), 17-25.
Wooldrige, J. M. (2003). Introductory Econometrics: A modern approach. Michigan: South-Western.
Zinn, J. S., Weech, R., & Brannon, D. (1998). Resource dependence andhinstitutional elements in nursing home TQM adoption. Health Services Research, 33(2), 261-74.

SAS
Make a planSAS program

Thank youHave a wonderful winter break