Embed Size (px)
Citation preview

How to Look at Posture~::-':vc ::¡nts for EvaluationWe have a couple of options for looking at the body to 'read' the story behind the problem.
1. Place the body in an anatomically neutral or symmetrical stance. This reveáis coreimbalances responsible for postural misalignments.
2. Allow the body to unselfconsciously assume its habitual posture, and also observeits movement patterns. This reveáis patterns of compensation for core issues that areoften at the root of joint problems.
To observe the second case scenario, it can be helpful to have the student walk in place, or walk away fromyou and back again, so that when he comes to a stop, you can see him fall into his more habitual posture, >
íf only for a moment. In the process, you can often see the compensations that take place, such as throw- u
> more weight to the outer heel of the foot to avoid pronation. You can observe how the feet are placed
- whether one is turned out more than the other, or one is forward of the other — the orientation of the JJj
hips and so on.
This reveáis the kind of stress that is habitually placed on the body or joints. For instance, if the student has ce
chronic knee pain after walking, the outwardly turned foot (of the leg that is in pain) shows you the kind i-
of rotational stress being placed upon the knee.
This approach shows us the compensations — the rotations, distribution of weight and so on — but only t/i
suggests clues as to the core issues, and often masks them. Our habitual (usually asymmetrical) stance is the ^
product of the body's attempt to diffuse problems that lie at a deeper level. Misalignments at the core are
uncomfortable. We stand asymmetrically — whether consciously or unconsciously — as a way of decreas-
:he discomfort by adjusting at the periphery. When a student stands with a symmetrical foundation,
the true postural deviations of the spine show themselves, as well the imbalances in muscle tone in the legs,
s and so on.
Zich form of observation has its purpose. Our habitual stance reveáis the compensations that are mostlikely to be the immediate cause of pain or wear upon the body. A neutral stance — and the discomfort itbrings — reveáis the deeper causes behind the compensations.
We'll explore each of these forms of observation in turn, starting with the neutral stance.
Neutral Foundation for EvaluationA neutral or symmetrical stance will include the following:13
1. Feet hip distance (acetabular) apart — i.e. vertically in line with the center of theball-and-socket space of the hip joint.
2. Rotation of the feet: typically in yoga the placement of the feet in Tadasana is parallel,which is used as the stance in evaluation as well. But for the sake of providing a neutralbasis for evaluation (rather than an attempt at approximating an ideal of anatomi-cally neutral), it is more often recommended in the field of bodywork that there beapproximately 15 degrees of equal external rotation of both feet.14
3. Feet evenly positioned — one foot should not be in front of the other.
13 Integrative Manual Therapy volumc III, Thomas Giammatteo, p. 1114 Ibid.,p. 11
S
OOUG KELLER 2006 YOGA AS THERAPY

4. Knees equally flexed/extended — if one knee is hyperextended, it should be broughtto neutral (with a 'microbend') to match the posture of the other knee.
Sagíttal Plañe Evaluation — Tilting Forward and Back, as Seen from the SideThe 'Sagittal Plañe' provides a 'side view' of the body. Evaluation of the bodyfrom this 'side view' usually involves an imaginary or real 'plumb line' thattouches the curve of the upper back (thoracic kyphosis) and also in normalposture touches or is very cióse to the base of the head (occiput) and buttocks.The córner of a wall can be used for this, though the student has to resist the 5.5 cm
temptation to lean or press into it.
Healthy spinal curves typically give 5-6 cm of space between the plumb lineand the deepest part of the cervical curve and lumbar curve.
Typical Misalignments on the Sagittal Plañe15
The following are typical deviations of posture that we find in the sagittal plañe. 5-6 cm
These deviations can be either of a pair of opposites in each área of the spine:
Head and Neck:
— Forward Head and Neck — the head is forward of the center ofgravity through the spine. The vertebrae are 'stuck' forward of thisplumb line.
— Fíat Neck — loss of cervical curve in which the head and particularlythe jaw/chin is drawn back strongly, straightening the spine — likea ballerina.
Upper Back
— Fíat Upper Back — loss of thoracic curve by vertebrae that are 'stuck'forward. The reason for this can sometimes be traced to dysfunctionof the organs within the rib cage — lungs, heart, etc.
— Excessive Curve in Upper Back — excessive thoracic kyphosis becausethoracic vertebrae are stuck in a flexed or forward-bending position,which can involve osteoporosis. Often this is a protective mode of posture, especiallyprotecting the heart. In general, this is also a protective posture when the arteries areput under stress from standing up straight — particularly if there is a problem withthe femoral artery.
Lower Back
— We will be looking at basic postural types, all of which are categorized basically accord-ing to the alignment of the pelvis. The distinctions as seen in the sagittal plañe have todo with whether the pelvis is tilted too far forward, has a deficient tilt or is forward ofthe line of gravity causing a flattened lumbar spine, or is 'tucked' causing a roundedlumbar spine. The remaining types have to do with rotations or torsions of the pelvisobserved in the coronal and transverse planes.
15 The points and informational points here are paraphrased from Integrative Manual Therapy volume III, Giammatteo, p.11
YOGA AS THERAPY DOUG K E L L E R 2006

Other Deviatíons
— Protruding Chin from hyperextension of the neck (between occiput and atlas). Head-aches can result from the compression of the back of the neck at the space beneaththe head.
— Dowager's hump — a dysfunction at the junction between the cervical and thoracicvertebrae.
»Misalignments at the ExtremitiesMisalignments in the Sagittal Plañe can also show up in the limbs:
1. Forward (anterior) Shoulders — most often from shortness of pectoralis minor andsubscapularis. >
2. Hyperextension of the Knees LL¡OL
3. Posterior Glide of the base of the tibia — limitation of the ability to 'flex' the foot ce
(dorsiflexion) because the tibia is stuck 'back' (posterior) on the talus bone. This is a
very common problem, a limitation of movement quite often associated with hyper- <
extensión of the knees.U15ceI-uiLU
I
H
DOUG KELLER 2006 YOGA AS THERAPY

Coronal Plañe Evaluation — Highs and Lows, as Seen from Front and BackEvaluation in the Coronal plañe looks at the body from trie front and back, taking note of differences inelevation between right and left sides of the body — highs and lows — that indícate either 'bends' (inthe spine — side to side) or 'shifts' (such as a shift of the head or chest to one side, or a sideward shift ofthe pelvis).
A useful grid is suggested by Pete Egoscue in which we Une up the key joints: ankles, knees, hips andshoulders. The point here is largely to determine whether the joints on the two sides of the body are levelwith each other, or whether one side is higher or lower. Vertical alignrnent of the joints is an added anddesirable bonus.
The shoulders, of course, vary a great deal in width among various body types (measured at the axis of thejoint, or head of the armbone). Thus we look more to the chest at the hollow space just beneath the col-larbone, to the outside of the rib cage. The point is that the shoulders be 'level' across the collarbones, andparallel to the horizontal lines of the rest of the joints — notably the hips.
Because of the variety of shoulderwidths, the shoulder joints them-selves may not une up verticallywith the hips, knees and ankles.Nevertheless, the joint levéis(horizontal lines) should ideallybe parallel with each other.
The level of the hips is ideallymeasured at the joint itself. This ¡susually rather hard for most of usto determine, so a sood indicatoris to find your 'hip points' withyour thumbs, and check whetherthey are level' in a mirror.
The knee joints are meant to bend atright ansies, and so ideal placementis vertically below the hip joints.Wide hip joints that créate a greater'Q' angle from hip bone to knee willplace uneven pressure on the kneeas well as affect the tone of the fourmuscles of the quadriceps, withgreater chance of knee problems
The quality of the arches — whetherthe feet pronate (fallen arches, archesturning in) or supínate (high arches,ankles turning out) will affect howwell the ankles bend in une with theknee and hip.
Redrawn from The Egoscue Method of Heaüng Through Motion, p. 12
YOGAASTHERAPY DOUG K E L L E R 2006

The hips are measured at the hip joint itself, where the head of the thighbone fits in the socket. This is ofcourse very hard to observe, so a helpful and more accessible indicator would be the 'hip points,' whichcan easily be found by touch. This gives a fair indication of whether one hip is higher than the other, andalso tells you of rotations in the pelvis: when one hip point is higher than the other, it is often rotated moreposteriorly ('back') than the other, indicating that the hip bone itself is rotated back. The other hip pointwhich is lower is often tipped anteriorly, indicating that the hip bone is rotated forward. This is one of themost accessible and important bits of information you can fmd for figuring out sacral and hip problems.
The Most Common Problem Observed at the Hip PointsThe most common problem you will observe in the Coronal plañe is a discrepancy in the level of the hippoints — one hip point (quite often the left) is observed to be higher (toward the head) than the other.This can be due to a real discrepancy in leg length — causing a sideward tilt to the hips — or much morecommonly an apparent discrepancy in leg length arising from the habit of putting more weight on one legthan the other, usually with pronation of the foot on the more weight-bearing side. This makes the otherleg seem to be shorter, since it struggles to reach the ground — usually supinating the foot. In this casethere is not so much a tilt to the side, but rather a torsión, in which the hip bones are rotated in oppositedirections — the 'low' hip point rotated forward and down on the more weight-bearing and collapsed side;the 'high' hip rotated up and back on the lighter side.
This discrepancy in hip height has consequences for the knees and shoulders.
Knees
There will be rotations in the bones of the legs that will cause wear and tear on the knees — largely becausethe hip joints and feet will be 'pointing' in different directions, causing twisting or uneven pressure in theknees.
The single most important principie at work for motion in the lower body is that the lower leg joints — kneeand ankle — are meant to move at right angles both in line with each other and in line with the hip. If weare walking forward, the hip joint 'points' us forward, and the knee and ankle should also 'point' straightforward as they bend and extend in the process of walking.
But all too often they don't. When there is a discrepancy in the hip joints because of rotations in the hipbones. the hips 'point' the legs in different directions: one thigh is rotated inwardly, pointing the thighbone/knee inward toward the midline as it bends; the other is rotated more externally, pointing the thighbone/knee outward. The inward rotation is on the side of the hip point that is 'down;' the external rotation ison the side of the 'high' hip point. On the high side, the hip is doing the walking rather than the core hipñexors (psoas), and the leg and hip get stifF.
Usually, as we'll see in cases of rotated and twisted postures, the foot will be turned out (externally rotated)on the leg in which the thigh is turned in (medially rotated) — meaning that the thighbone and shins areturned in opposite directions at the knee, twisting the knee. On the side of the 'high' hip, the stifíhess andexternal rotation of the hip will cause more jamming at the outer knee.
Many knee problems arise from the fact that the knee essentially tries to do whatever the hip and foot tellit to do. When it receives opposing messages, it suffers!
The first clue to the cause of problems in the knee, foot and hip thus can be found in the Coronal plañe- from observing the relative 'height' of the hip points and arches of the feet (pronation or supination),
and from observing the rotations of the thighbone and shin relative to each other at the knee.
IG KELLER 2006 YOGA AS THERAPY

Shoulders
The shoulder is often — though not always — elevated on the same side as the 'high' hip. The shouldergenerally acts as a counterweight to the hips, and can be involved in the effort of hoisting up the stiff legand swinging it around to bring it forward. This is dramatized by actors playing the role of a hunchback inhorror films. With most of the weight shifted to one side of the body, they throw the opposite hip and legforward with the help of the lifted or 'hunched' shoulder, as if that side of the body were half paralyzed. Insome cases that's not far from the mark, minus the hammy theatricality.16
Postural dysfunctions that show up in the Coronal plañe thus include shifts, bends and tilts to the side: ashift in weight (via a shift in the hips to one side, along with a tilt) can créate a side-bend in the spine, anda tilt (and even a shift) of the head to the opposite side as a counterbalance.
But at least in this case, the problem lies not in the architecture; it lies in the unbalanced use to which it isbeing put — in a word, ftmction. And form — our physical form — most often follows function.
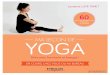
The'Shorter Leg Syndrome'which ¡s Observable ¡n the Coronal Plañe
Shoulders and HipsMove and Work as
aUnit
Elevated Hip
Lighter Load:
Muscles and Bonespulled up away
from floor
Right Leg Stiffens
Foot supinates (higharch) as it 'reaches'
for the floor— while bearing
less weight
Habitually shifting the weightto one side ¡s like carryinga heavy bucket; the heavyside is compressed down-ward, while the light side ispulled upward
Lower HipGreater weight-
bearing
Increased stress onhip joint, knee and
ankle
Foot Pronatesunder the weight:
pressure fromwalking rebounds¡nto the ankle and
knee
Redrawn from The Egoscue Method of Healing Through Motion, p. 32
As the pelvis shifts to the weight-bearing side, the¡lium of the weight-bearing side tips downward (ante-riorly) from pressure, especially as the weight-bearingmuscles of the hip tire. This can cause pinching orcompression in the groin at the hip joint.
To get a sense of this, imagine carrying a heavy bucket:the compressed leg is on the side of the bucket.
The other leg is lighter: the ilium pulís upward and usu-aily tips back (posteriorly) as the energy of the entireleg (and shoulder) pulís upward to maintain balance.Thus the 'hip points' are noticeably uneven.
Usually foot of the 'short' weight-bearing leg will bepronated (weight on the inner edge; fíat foot) whilethe foot of the long' leg will be supinated (weight onthe outer edge; high arch). Since the supinated footseems to struggle to reach the ground and has lessweight on it—because the hip is pulled up higher—the leg seems to be shorter — and will even appearto be so if you have the person lie down, and lookat the apparent leg length.
16 The Egoscue Method of Healing Through Motion, p. 36
YOGAASTHERAPY DOUG KELLER 2006

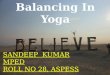
Space betweenlower ribs and ¡liui(top of hip bone)
PSIS
Gluteal Folds
Lateral Shift of Neck
Shoulder Girdle
Inferior angle of scapula
12th Ribs (lateral)
Elbow Level (flexed)
lliac Crest
Ears
Lateral Shift of Neck
Shoulder Girdle
Nipple Lin
Elbow Level(when flexed)
'Hip Points'.
There are of course more elabórate and precise points for checking difFerencesin elevation on either side of the body.17 These can include lateral shifts in thebones, such as in the head of the shin bone, or in the bones of the ankles.
In the legs and arms, coronal deviations show up as the following:
1. Lateral (sideways) shift or compression at the hips (greatertrochanters). Checking the level of the 'hip points' tipsus offon this.
2. Lateral glide of the head of the shin (tibial plateau) at theknee joint. Here we can check the 'bump of the tibiabelow the kneecap.
3. Pronation or Supination of the foot and anide. Here welook to the inner ankle (inferior medial malleolus)
4. The angle of the elbow (as well as the level), and theturn or 'ulnar deviation' of the wrist. Here we can tellespecially by noting how much of the back of the handis showing.
uLU0-l/lce
=31-
QCI-OO
Integrativc Manual Therapy volume III, Thomas Giammatteo, p. 21
DOJG K E L L E R 2006YOGA AS THERAPY

Transverse Plañe Posture Evaluatíon: Rotations around the CenterTransverse Plañe evaluation has to do with rotational dysfunctions of the spine, and the checking is donefor the most part from the back body by looking at the tone and prominence of the muscles at either sideof the spine, and at the transverse processes.18
These kinds of rotations are obviously related to'outer body' rotations seen in the Coronal Plañeevaluation, especially when there is scoliosis.Transverse Plañe evaluation looks closer to thespine in the back body, noticing prominencesaround the vertebrae, which are more 'in' or'out' rather than high or low.
At the front body, we can look at the shouldersfor transverse dysfunction. We look for whethera shoulder is 'forward.' This will bring limita-tions in movement: if the right shoulder isforward (protracted, with the shoulder blademoving away from the spine), then the armwill be limited in its ability to lift out to theside (horizontal abduction) as well as limita-tions in the ability to draw back (retract) theshoulder.
The most important landmarks at the frontbody are the 'hip points,' which can give a clueto rotations of the spine at the sacrum. Becauseof their connection to the Spiral Sutra, rota-tions of the pelvic bones that appear at the hippoints will be closely allied with misalignmentsand rotations that appear in the arches of thefeet, the knees, spine, shoulders and neck.
Transverse evaluation looks 'around' the centralaxis of the body to see rotations that appear ascombinations of 'tilts' (anterior or 'forward,'and posterior or 'back') that appear in the sag-ittal plañe, and highs and lows that appear inthe coronal plañe. The transverse plañe makesthese observations 'three-dimensional' by not-ing rotations in three-dimensional space.
18 Integrative Manual Therapy volume III, Thomas Giammatteo, p. 24
YOGAASTHERAPY DOUG KELLER 2006

Basic Types of PostureClassification of Types of Posture can be based essentially upon what the hips are doing, from a forwardtilt to the pelvis causing excessive lumbar curve, to a backward tilt — in the extreme, a 'tuck' — causing aflat or even rounded lumbar spine.
Each postural type will carry with it specific problems, particularly for the low back, which we'll explore.
Tilted'
Forward Pelvic Tilt
Forward Hips/ Swayback
Forward Pelvic Shift
'Fíat'
Backward Pelvic Tilt
Tucked'
Backward Pelvic Tilt and Shift
t—uLUIX
ocLUO.
u=3ce\-1/1
'Rotated'
Rotated around central axis,with some discrepancy in hip~eght from rotation of torso
Basic Postural Types can be distinguishedaccording to:
1. The 'tilt' of the pelvis, which is relative to
1. The 'shift' of the pelvis relative to thecenter of gravity.
It is far more common that the basic posturaltype is combined with some degree of rota-tion in the pelvis, whether it ¡s
1. A 'rotation' of the pelvis around thecentral axis of the body, with one side ofthe body — hip and shoulder — forwardof the other.
1. A 'twist' or torsión in the pelvis itself,most often from uneven weight bearing onthe feet or greater pronation and outwardrotation of one foot; also accompanied bythe opposite shoulder being pulled towardthe 'low' hip, causing twisting in the upperbody.
Twisted'
Pelvis Twisted from opposins pulíof shoulders and feet: greater
discrepancy in hip height
: :_G < E L L E R 2000 YOGAASTHERAPY