Embed Size (px)
DESCRIPTION
How to make sense of genetic studies in AML and MDS. Elie Traer September 13, 2012. Outline. Genetic tests and methodology Cytogenetics , i.e. large chromosomal abnormalities FISH, smaller chromosomal changes Genetic mutations AML Evolution of genetic tests in diagnosis and prognosis - PowerPoint PPT Presentation
Citation preview

How to make sense of genetic studies in AML and MDS
Elie TraerSeptember 13, 2012

Outline• Genetic tests and methodology
– Cytogenetics, i.e. large chromosomal abnormalities– FISH, smaller chromosomal changes– Genetic mutations
• AML– Evolution of genetic tests in diagnosis and prognosis– Risk groups and treatment– Future
• MDS– Current prognostication in acute leukemias
• What to order• How it affects treatment

Cytogenetics - Methodology• Cytogenetics (karyotype)
– Cells arrested in metaphase with mitotic inhibitors
– Depends upon chromatin condensation during metaphase (metaphase spread)
• Most cells are in interphase– Staining with Geimsa stain produces
distinctive G-banding patterns
Metaphase Of course, not everything is neatly arranged in real life…
Interphase

Normal cytogenetics – cleaned up
22 paired chromosomes + XY = 46 total(image from NHGRI)

Classic cytogenetics
• Advantages:– Whole chromosome analysis of individual cells– Bone marrow aspirate relatively easier
• Compared to solid tumors
• Disadvantages:– Time consuming– Need metaphase spreads– Not sensitive for small genetic deletions or
changes

FISH – a “new” technique for cytogenetics
• FISH = fluorescence in situ hybridization• Technique developed in part by Joe Gray
• Proc Natl Acad Sci U S A. 1986 May;83(9):2934-8
• Fluorescently labeled probes targeted to known areas of chromosomes
• Advantages compared to cytogenetics– Don’t need metaphase– Sensitive to small changes– Can target any part of chromosome
• BUT, you have to know what you are looking for

FISH – CML
• Red probe to chromosome 22
• Green probe to chromosome 9
• Fusion creates red-green or yellow color
Interphase Metaphase
Probes come together

Cytogenetics in leukemia• Oldest method for looking at chromosomes
– >300 cytogenetic abnormalities in acute leukemia• Most famous translocation is t(9;22), or
Philadelphia chromosome– fusion of BCR and ABL genes– led to development of imatinib
• Technique demonstrate clonality of leukemia– CML with specific secondary cytogenetic abnormalities
• Cytogenetic abnormalities associated with disease subtypes and prognosis

How important are genetics?
FAB CLASSIFICATIONo M1 myeloblastic
undifferentiatedo M2 myeloblastic with
differentiaiono M3 promyelocytico M4 myelomonocytico M5 monoblastico M6 erythroleukaemiao M7 megakaryoblastic
WHO CLASSIFICATION 2008o AML with recurrent genetic
abnormalitieso AML with multilineage
dysplasiao AML therapy relatedo AML not otherwise categorisedo AML of ambiguous lineage

WHO 2008 recurrent cytogenetics
• t(8;21)(q22;q22)• Inv(16)(p13.1q22) or t(16;16)(p13.1;q22)• t(15;17)(q22;q12)• t(9;11)(p22;q23):MLLT3-MLL• t(6;9)(p23;q34)• t(1;22)(p13q13)
*Considered acute leukemias regardless of blast count

Cytogenetic risk groups• Favorable (~20%)
– CBF: t(8;21)(q22;q22), Inv(16)(p13.1q22) or t(16;16)(p13.1;q22)– APL: t(15;17)
• Intermediate (~60%)– Normal cytogenetics (~50% of all AML cases)– t(9;11)(p22;q23):MLLT3-MLL– Any cytogenetic abnormality not classified as favorable or adverse
(trisomy 8)• Adverse (~20%)
– Inv(3)(q21q26.2) or t(3;3)(q21;q26.2)– t(6;9)(p23;q34)– t(v;11)(v;q23): MLL rearranged– - 5 or del(5q)– -7– Abnl 17p– Complex karyotype

Core Binding Factor Leukemias
• t(8;21) and inv16/t(16;16)
atlasgeneticsoncology.org

t(8;21)(q22;q22) RUNX1-RUNX1T1
• RUNX1 = AML1 = CBFa = 21• RUNX1T1 = ETO = 8• Approximately 8% of AMLs - predominately in younger patients• Blasts have cytoplasmic hoffs, occasional Auer rods, occasional salmon-
colored granules• Dysplastic features in maturing neutrophils• Favorable prognosis when presenting with white blood cell count less than
20 x 109/L and NO KIT mutationJaffe Hematopathology

Inv(16)(p13.1q22) or t(16;16)(p13.1;q22)
• CBFB = 16q22• MYH11 (smooth muscle myosin heavy chain) = 16p13• 5-8% of AML• All age groups, predominately in younger patients• Blasts have myelomonocytic features• Abnormal eosinophils with large granules in bone marrow
(M4Eo)– no peripheral eosinophilia
• Good prognosis when NO KIT mutation is present• May be missed on routine karyotyping, need FISH

Acute promyelocytic anemia (APL) with t(15;17)(q22;q12) PML-RARA
• Proliferation of leukemic blasts blocked at the promyelocyte stage of differentiatoin – 5-8% of AML– Abundant cytoplasmic granules and Auer Rods– Weak or absent HLA-DR and absent CD34 expression– Low white count– Disseminated intravascular coagulation (DIC) – Medical
Emergency!– Treat with all-trans-retinoic acid (ATRA)

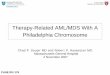
Survival associated with cytogenetics
Slovak et al. Blood, 2000Years After Entering Study
0
20
40
60
80
100
0 2
Cum
ulat
ive
Perc
ent
84 6
Favorable 121 53 55% (45-64%)Intermediate 278 168 38% (32-44%)Unfavorable 184 162 11% ( 7-16%)
Estimate (CI) At Risk Deaths at 5 Years
Heterogeneity of 3 Groups: p<.0001

Is cytogenetic analysis old news?
• Presence of a monosomy (ie chromosome 7 deletion) with 2 additional chromosomal deletions or with complex cytogenetics
• Associated with a poor CR rate and OS (4%)• Many recent studies have confirmed
– phrases such as dismal outcome and very unfavorable
Breems J Clin Oncol 2008

Effect on overall survival
Breems J Clin Oncol 2008

Cytogenetics summary
• Cytogenetics remains an important risk classification for acute leukemia, particularly AML
• Cytogenetics/FISH can only detect large genetic changes
• However, 50-60% of AML with “normal” cytogenetics– Really normal?

Mutations in leukemia (molecular markers)
• Smaller changes to DNA are not detected with cytogenetics/FISH– Mutations– Smaller duplications– Deletions

Quick genetic review
• DNA holds all instructions– 3 trillion base pairs
• mRNA translated from DNA– introns spliced out– hundreds to thousands
of base pairs• mRNA translated into
protein

Mutations – methodology• PCR
– Method for amplifying known sections of DNA or mRNA– Can be quantitative (QPCR)
• BCR-ABL, PML-RARA– Can detect small variations in size (deletions or amplifications)
• e.g. FLT3 ITD
• Sanger sequencing– Direct sequencing of DNA
• Sequenom– Multiplexed PCR and MALDI-TOF
• Next generation sequencing– Whole exome/genome– Deep sequencing

PCR
• Primers surrounding area of interest
• Selective area amplified• Can be sequenced or
analyzed by gel electrophoresis

FLT3 internal tandem duplication
ASH Education Book January 1, 2001 vol. 2001 no. 1 541-552
• FLT3 is receptor tyrosine kinase
• Japanese groups originally found internal tandem duplication
• Nakao et al. Leukemia 1996
• ITD leads to activation of kinase
• Can be detected by PCRITDnormal

FLT3 ITD is unfavorable risk marker• FLT3 ITD detected in
~30% of normal cytogenetics AML
• Point mutations, i.e. D835 mutations found in ~10%• Not prognostic
• Associated with higher relapse and worse overall survivalKottaridis et al. Blood 2001

Point mutations:CEBPa
• Transcription factor involved in neutrophil differentiation
• Mutations in multiple sites but most lead to early truncation of protein
• 10% mutations in normal cytogenetics AML
Preudhomme et al. Blood 2002

NPM1 mutations
• Most frequent molecular abnormality in normal cytogenetics AML: 50-60%
• Usually 4 nucleotide insertion
• Can be detected with Sanger sequencing
Chen et al. Arch Pathol Lab Med. 2006

NPM1 mutation• Nuclear transport protein• Mutation associated with abnormal
localization of protein in cytoplasm• C-terminal mutations detected in 85%
– NLS domain• Frequently occurs with FLT3 ITD Fallini N Engl J Med 2005; Döhner Blood 2005; Schnittger Blood 2005; Verhaak Blood 2005

NPM1 and CEBPa are favorable prognostic markers (without FLT3 ITD)
Schlenk N Engl J Med 2008

c-Kit• Receptor tyrosine kinase• Activating mutations in c-Kit have been described
in AML• Most common mutation in exon 17 (D816V)• Only has prognosis in core binding factor (CBF)
AML, inv(16) and t(8;21)• Paschka et al. J Clin Oncol, 24 2006
• However, recent report suggests that this may be limited to t(8;21)
• Park et al. Leuk Res, 2011

Genetic (cytogenetic and molecular) abnormalities and prognosis in AML

Sequencing more genes and more samples is increasing known mutations
• Largely driven by technology– Dramatic cost reductions– ~$100,000 to sequence genome in 2008
• Ley et al. Nature 2008– Now about $2000
• Prognosis still not clear for many of these genes

Mutations in AMLNPM1 45-64% CN-AML Good without other mutations presentCEBPA 10-18% CN-AML Good with both alleles are mutatedFLT3 ITD 28-34% CN-AML WorseKIT 25-30% CBF AML Inferior* in CBF-AMLFLT3 TKD 5-10% all AML/11-14% CN-AML ?IDH1/2 10-15% CN-AML Inferior – controversialWT1 10-13% CN-AML ?RUNX1 5-13% all AML few studies – worseMLL-PTD 5-11% CN-AML Worse, but not an independent prognostic factorNRAS 9-14% CN-AML, 40% CBF AML,
25-30% AML with inv(3)None
KRAS 5-17% CBF-AMLTP53 Complex/monosomal karyotpype
and tx-related AMLInferior
TET2 23% of CN-AML ?ASXL1 ~15%, Exon 12 Few studies, worseDNMT3A 20% inferiorBCOR 6% ?Others: CBL, JAK2, EZH2
J Clin Oncol. 2011 Feb 10;29(5):475-86

AML and MDS panel at OHSU
Ion Torrent – next generation sequencing

A “torrent” of data
• ~25 base pairs of data
• Massive computing to align sequences
• Deep sequencing– average
coverage of one nucleotide

Ion Torrent panel - GeneTrailsR-tyrosine kinase FLT3 KIT CSF3R
C-tyrosine kinase JAK2 ABL1 Signaling molecule
CBL CBLB NRAS KRAS HRAS
Serine/threonine kinase
BRAF
Cytokine receptor MPL Phosphatase PTPN11 Epigenetic IDH1 IDH2 DNMT3A TET2 MLL EZH2 UTXSplicing machinery
SF3B1 PRPF40B SF1 SF3A1
ZRSR2 SRSF2 U2AF1/U2AF2
Transcriptional factor
NPM1 GATA1 CEBPA ETV6 RUNX1 WT-1
Other ASXL1 SH2B3(LNK)
TP53

Why do extra testing?
• Clinical– Help with prognosis and/or treatment
• e.g. AML with multiple MDS-type mutations
• Prepare for the future– Ion Torrent can sequence multiple genes at once
• Replace multiple genetic tests• More sensitive• Prepare for future prognostic studies• Cost is going down

Reality check – How does this influence therapy?

EORTC AML-10 trial
• After induction, all patients < 46y allocated to - alloSCT if they have a donor - ASCT otherwise• Intent-to-treat analysis• N= overall 1198 pts• After induction, n=293 with a donor, n=441
without a donor Suciu et al, Blood 2003

EORTC AML-10: results in cytogenetics groups
Intermediate CGFavorable CG
Poor CG
Favorable risk gets no improvement in OS with allo
Intermediate group as well but good portion were certainly favorable risk by molecular studies (just not known at time)

RFS in a donor vs no donor basis: NPM1+ FLT3-ITD-
Schlenk N Engl J Med 2008

And that’s why we do this
3+7 followed by HiDAC
3+7 followed by allo SCT if good match available, consider auto or just chemo
3+7 followed by allo SCT

Myelodysplastic syndrome• MDS – classically defined
– Cytopenias– Abnormal cell maturation (dysplasia)– Can transform to AML
• Arbitrary line = 20% blasts in marrow is AML• Shared genetic abnormalities
• Heterogeneous disease (like AML)– Transplant is only cure, but timing is important– Genetic studies becoming more important
• Diagnosis/prognosis• Defining treatment

Old classification - Morphology
Up To Date

WHO 2008 classification
• Genetic abnormalities becoming more important– Added MDS with isolated 5q-
• More importantly, risk assessment and genetics becoming more refined– Revised-IPSS

CytogeneticsR-IPSS
Blood. 2012;120(12):2454

Scoring system R-IPSSCytogenetics influences prognosis
Blood. 2012;120(12):2454

Like AML, mutations are
becoming more important in
MDS
N Engl J Med. 2011 364(26):2496-506

Many concurrent mutations
N Engl J Med. 2011 364(26):2496-506

Mutations can be used to assess risk
N Engl J Med. 2011 364(26):2496-506

Some mutations associate with low risk MDS
Blood 2011 118(24):6239-46
RARS – refractory anemia with ringed sideroblastsLower risk disease by morphology

SF3B1 mutations - OS
Blood 2011 118(24):6239-46
* Not independent of morphology

Ion Torrent panel - GeneTrailsR-tyrosine kinase FLT3 KIT CSF3R
C-tyrosine kinase JAK2 ABL1 Signaling molecule
CBL CBLB NRAS KRAS HRAS
Serine/threonine kinase
BRAF
Cytokine receptor MPL Phosphatase PTPN11 Epigenetic IDH1 IDH2 DNMT3A TET2 MLL EZH2 UTXSplicing machinery
SF3B1 PRPF40B SF1 SF3A1
ZRSR2 SRSF2 U2AF1/U2AF2
Transcriptional factor
NPM1 GATA1 CEBPA ETV6 RUNX1 WT-1
Other ASXL1 SH2B3(LNK)
TP53

Genetics and treatment
• Isolated 5q– Lenalidomide
• Epigenetic mutations (TET2, DNMT3A, ASXL1)– May predict better response to hypomethylating agents
• Leukemia 2011 25(7):1147-1153
• High risk– Allogeneic transplant

Summary• Cytogenetics and genetic tests are important for risk stratification
and treatment
• Important to collect information at diagnosis– Especially AML
• Cytogenetics and FISH still important
• Mutations also prognostic
• More mutations being discovered– GeneTrails/Ion Torrent