Embed Size (px)
Citation preview
How to prevent, diagnose and overcome resistance to nucleoside
analogs ?
Fabien Zoulim
Liver department, Hôtel Dieu Hospital
& Hepatitis research laboratory, INSERM U871
Lyon, France
Clinical definitions

Définition of resistance
• Virologic Breakthrough: Rebound in serum HBV DNA levels (e.g. 1 log10 above nadir)
• Genotypic Resistance: Detection of mutations known to confer resistance while on therapy
• Virologic Breakthrough with Genotypic Resistance: Viral rebound associated with a mutation(s) known to cause resistance.
• Primary non response: <1log10 decrease of viral load after 3 months
• Partial response: detectable HBV DNA levels during therapy
Zoulim & Perrillo, J Hepatol 2008; EASL CPG, J Hepatol 2009
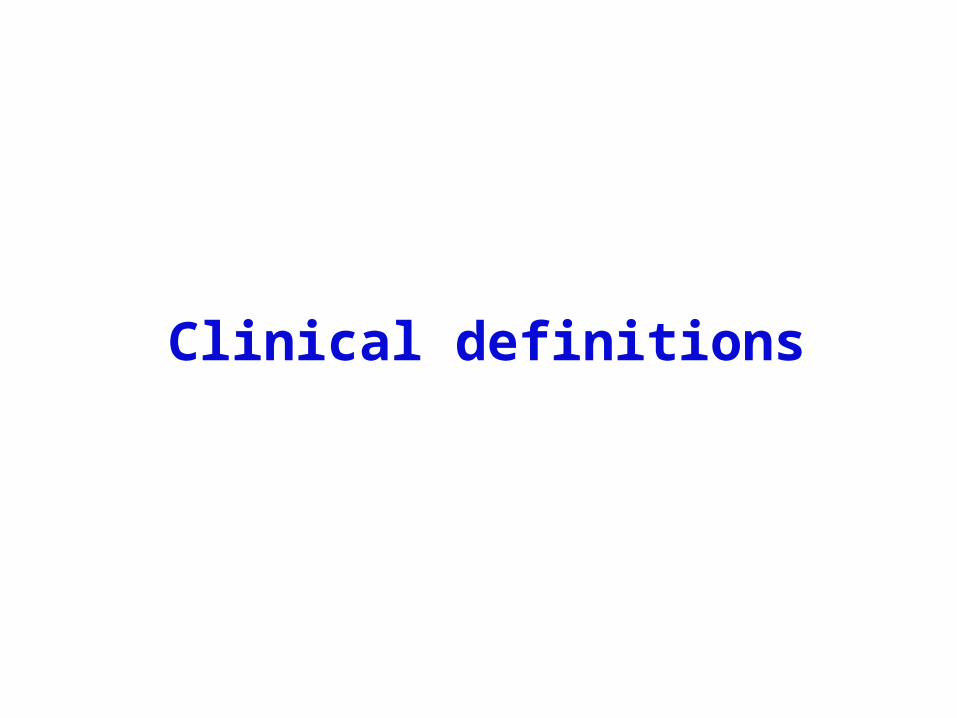
Treatment failure
Primary non responsePartial response
Secondary treatment failureAntiviral drug resistance
Host factorsDrug metabolismPatient’s compliance
Drug factorsAntiviral potency
Drug factorsBarrier to resistance
Viral factorsResistant mutants
Zoulim & Perrillo J Hepatol 2008; EASL CPG J Hepatol 2009
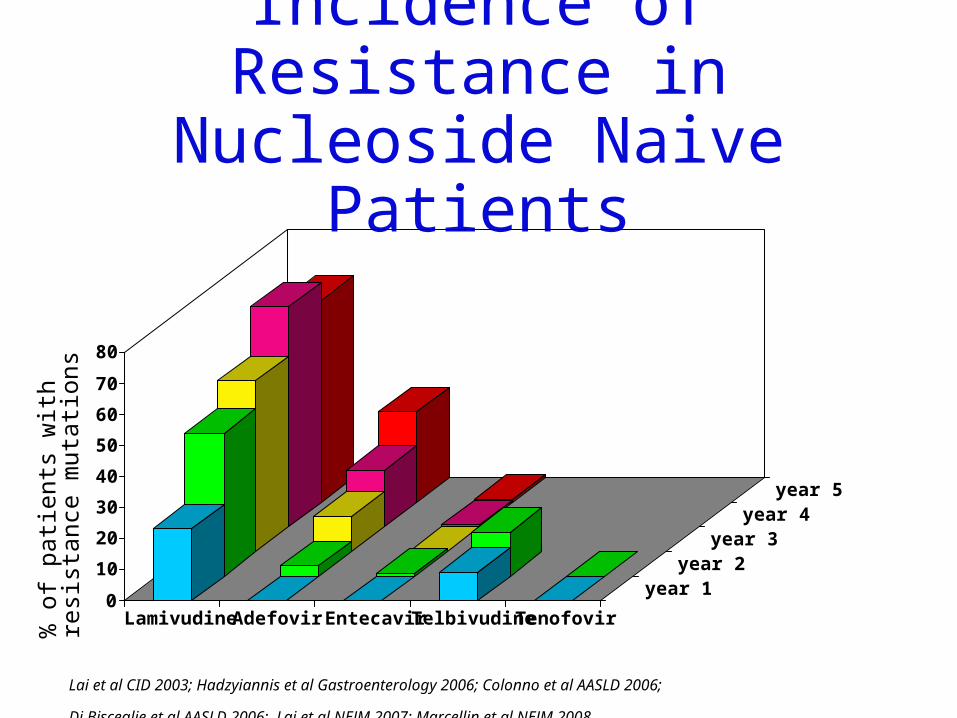
Incidence of Resistance in Nucleoside Naive Patients
% o
f pa
tien
ts w
ith
resi
stan
ce m
utat
ions
Lai et al CID 2003; Hadzyiannis et al Gastroenterology 2006; Colonno et al AASLD 2006;
Di Bisceglie et al AASLD 2006; Lai et al NEJM 2007; Marcellin et al NEJM 2008
0
10
20
30
40
50
60
70
80
Lamivudine Adefovir Entecavir Telbivudine Tenofovir
year 1year 2
year 3year 4
year 5

Incidence of Resistance in Lamivudine Refractory Patients
% o
f pa
tien
ts w
ith
resi
stan
ce m
utat
ions
0
10
20
30
40
Adefovirswitch
Adefoviradd-on
Entecavirswitch
Tenofovir +FTC/3TC
baseline
Year 1
Year 2
Year 3
Year 4
Lampertico et al Hepatology 2005 & Gastroenterology 2007; Colonno et al AASLD 2007; Lacombe et al AIDS 2006
Time
Antiviral drug
HB
V D
NA
(lo
g1
0 I
U/m
L)
AL
T (IU
/L)
4
6
5
3
2 ULN
1
0
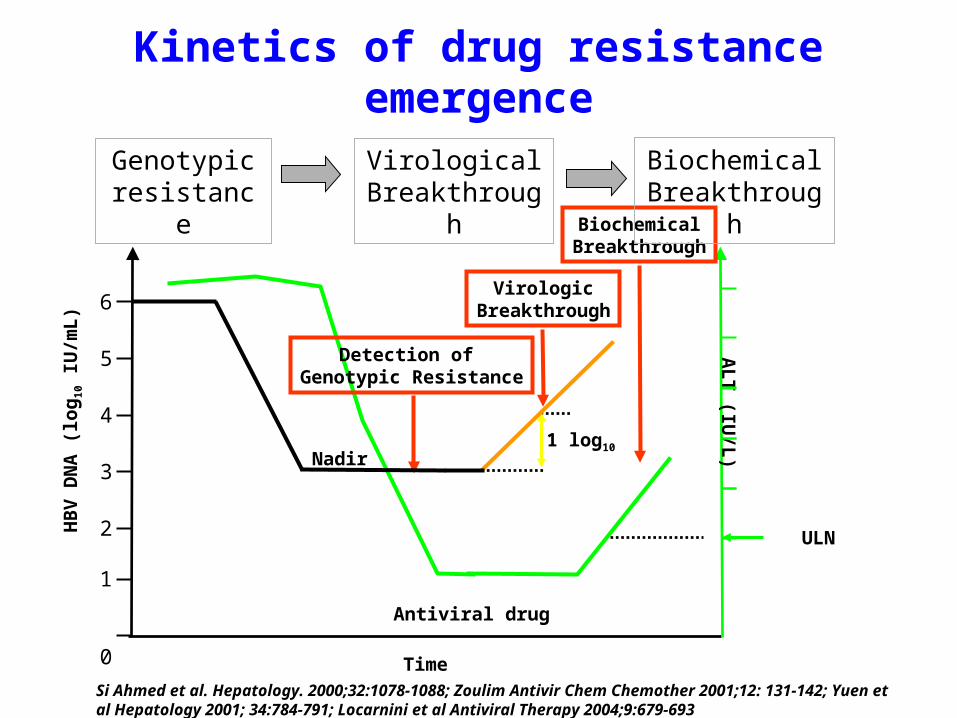
Detection of Genotypic Resistance
Nadir1 log10
VirologicBreakthrough
BiochemicalBreakthrough
Genotypic resistance
VirologicalBreakthrough
BiochemicalBreakthrough
Kinetics of drug resistance emergence
Si Ahmed et al. Hepatology. 2000;32:1078-1088; Zoulim Antivir Chem Chemother 2001;12: 131-142; Yuen et al Hepatology 2001; 34:784-791; Locarnini et al Antiviral Therapy 2004;9:679-693
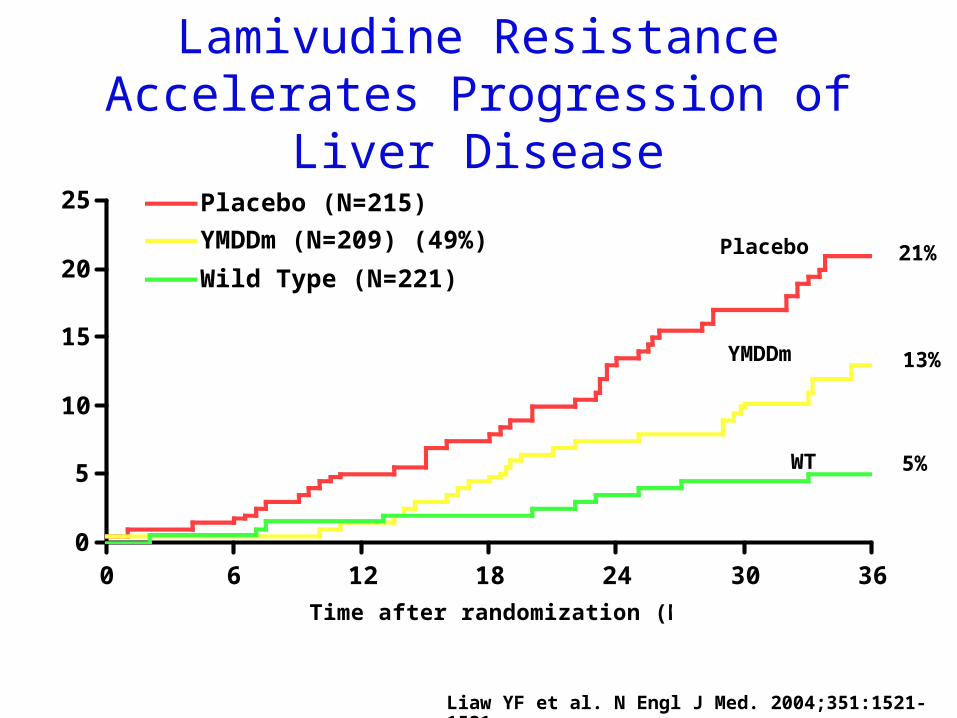
Lamivudine Resistance Accelerates Progression of Liver Disease
0
5
10
15
20
25
0 6 12 18 24 30 36
Time after randomization (Months)
% W
ith
dis
ea
se
pro
gre
ss
ion
Placebo (N=215)
YMDDm (N=209) (49%)
Wild Type (N=221)
YMDDm
WT
Placebo
5%
13%
21%
Liaw YF et al. N Engl J Med. 2004;351:1521-1531
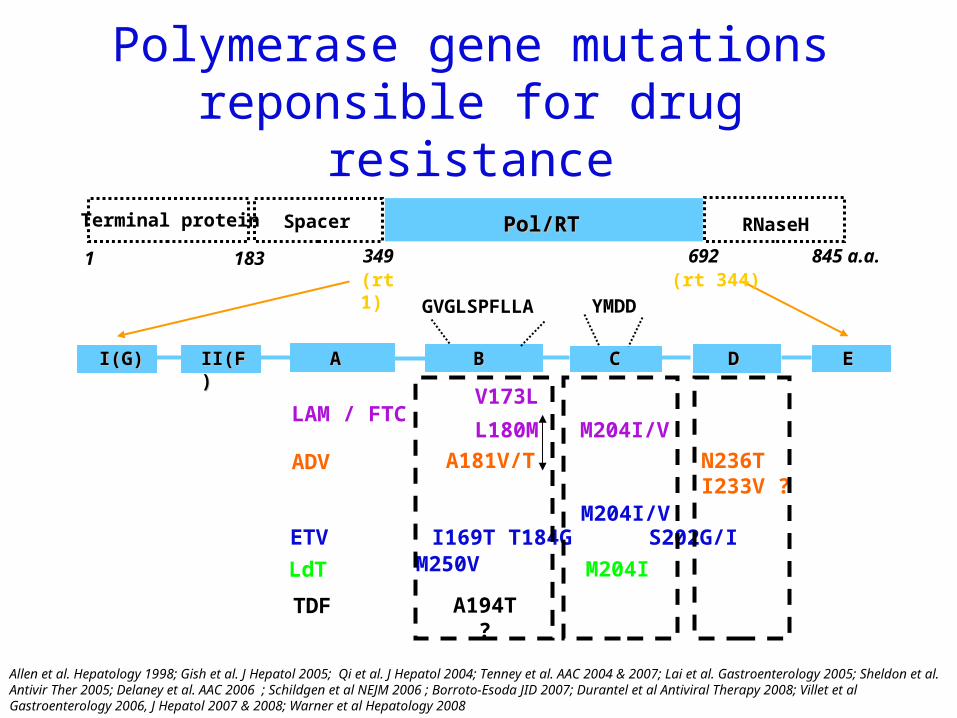
Polymerase gene mutations reponsible for drug resistance
Allen et al. Hepatology 1998; Gish et al. J Hepatol 2005; Qi et al. J Hepatol 2004; Tenney et al. AAC 2004 & 2007; Lai et al. Gastroenterology 2005; Sheldon et al. Antivir Ther 2005; Delaney et al. AAC 2006 ; Schildgen et al NEJM 2006 ; Borroto-Esoda JID 2007; Durantel et al Antiviral Therapy 2008; Villet et al Gastroenterology 2006, J Hepatol 2007 & 2008; Warner et al Hepatology 2008
RNaseH
845 a.a.
Terminal protein Spacer Pol/RTPol/RT
AA BB CC EED D
1 183 349 692
YMDD
V173L
L180M M204I/V
GVGLSPFLLA
I(G)I(G) II(F) II(F)
(rt1) (rt 344)
LAM / FTC
ETV I169T T184G S202G/I M250V
ADV A181V/T N236TI233V ?
LdT M204I
TDF A194T ?
M204I/V

Tools for the diagnosis of resistance

Dynamic ranges of quantificationof HBV DNA assays
Amplicor HBV Monitor v2.0 (Roche)
HBV Hybrid-Capture II (Digene)
Ultra-sensitive HBVHybrid-Capture II
Versant HBV DNA3.0 (bDNA, Siemens)
Cobas Taqman HBV(Roche)
Abbot Real-time HBV(Abbott)
Versant HBV DNA 1.0(kPCR, Siemens)*
*in development
1010 101022 101033 101044 101055 101066 101077 101088 101099
RealArt HBV LC PCR(Artus Biotech)

Methods to detect genotypic resistance
• Direct PCR sequence analysis
• Reverse hybridization assay (INNO-LiPA DR)
• Others• Restriction fragment length polymorphism (RFLP) analyses• Matrix-assisted laser desorption/ionization-Time of light Mass
Spectrometry (MALDI-TOF MS)
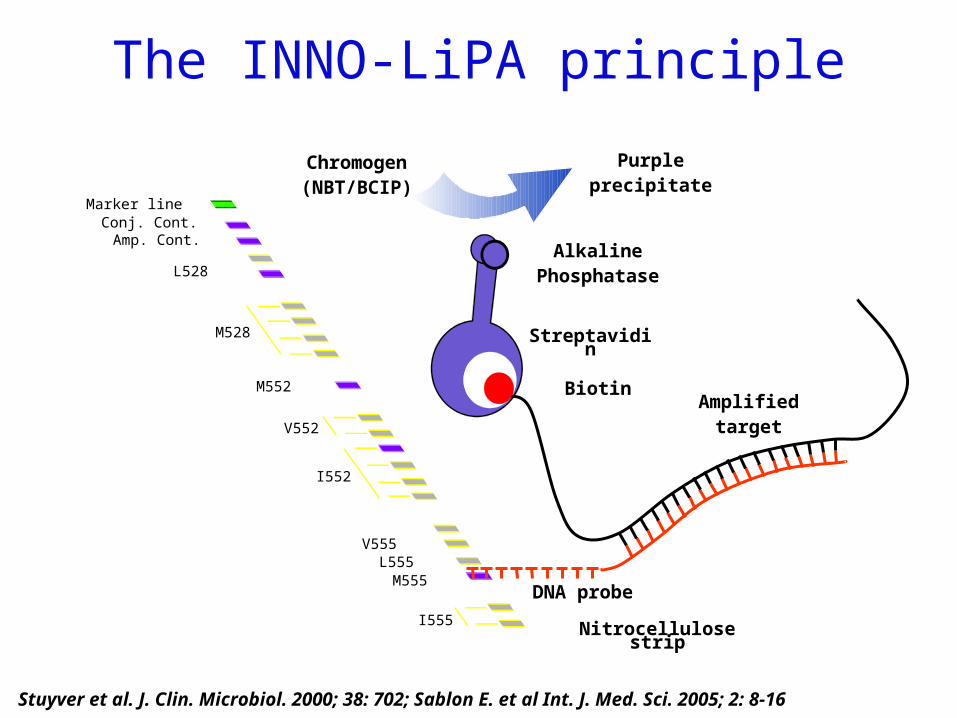
The INNO-LiPA principle
DNA probe
Nitrocellulose stripI555
M555L555
V555
I552
V552
M528
M552
L528
Amp. Cont.Conj. Cont.
Marker line
AlkalinePhosphatase
Streptavidin
Chromogen(NBT/BCIP)
Purpleprecipitate
BiotinAmplified
target
Stuyver et al. J. Clin. Microbiol. 2000; 38: 702; Sablon E. et al Int. J. Med. Sci. 2005; 2: 8-16

Phenotypic resistance testing
• Determines in vitro inhibitory concentrations (IC)/effective concentration (EC) of specific HBV inhibitors relative to a wild type or reference strain
• Allows the quantification of the magnitude of resistance to a drug without the need to know the responsible mutation(s)
• Confirms the drug susceptibility associated with a given amino-acid change in HBV polymerase (eg. M204V/I) and determines its cross-resistance profile

Results of phenotypic assaysIn
hib
itio
n o
f vi
ral
rep
lica
tio
n
100%
0%
50%
Concentration of drug
Wild-type virus
Patient’s virus
IC50IC50
IC50 wild type
IC50 patient= Fold change
IC50 = Drug susceptibility

Choice of drug for treatment adaptation

Lamivudine Telbivudine Entecavir Adefovir Tenofovir
Wild-type S S S S S
M204l R R I S S
L180M + M204V
R R I S S
A181 T/V I S S R S
N236T S S S R I
I169T + V173L + M250V*
R R R S S
T184G + S202lI/G * R R R S S
*: (+ L180M + M204I/V).
Cross-resistance data for the most frequent resistant mutants
Durantel et al Hepatology 2004; Brunelle et al Hepatology 2005; Yang et al Antiviral Therapy 2005; Villet et al Gastroenterology 2006 & 2008; Delaney et al AAC 2006; Villet et al J Hepatol 2007 & 2008; Brunelle et al AAC 2007;
Qi et al Antiviral therapy 2007; Tenney et al AAC 2004 & 2007
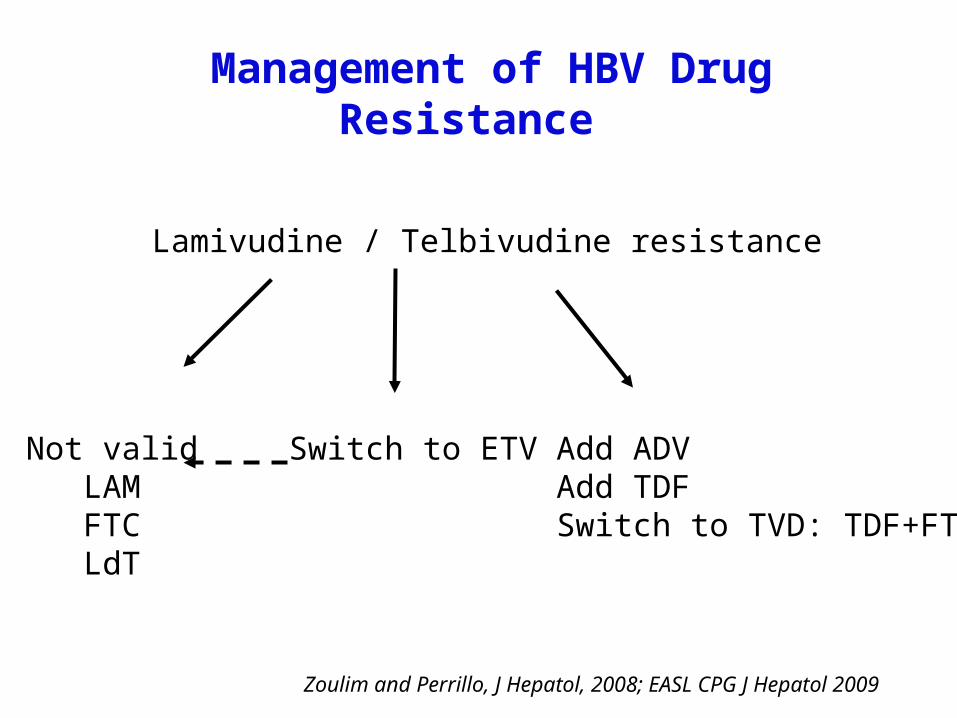
Lamivudine / Telbivudine resistance
Add ADV Add TDFSwitch to TVD: TDF+FTC
Switch to ETVNot validLAMFTCLdT
Management of HBV Drug Resistance
Zoulim and Perrillo, J Hepatol, 2008; EASL CPG J Hepatol 2009

Adefovir resistance
Add LamivudineAdd ETVAdd Telbivudine
Switch to TVD: TDF+FTC
Management of HBV Drug Resistance
Switch toTDFTVDETVLdT
Adefovir non response
Zoulim and Perrillo, J Hepatol, 2008; EASL CPG J Hepatol 2009
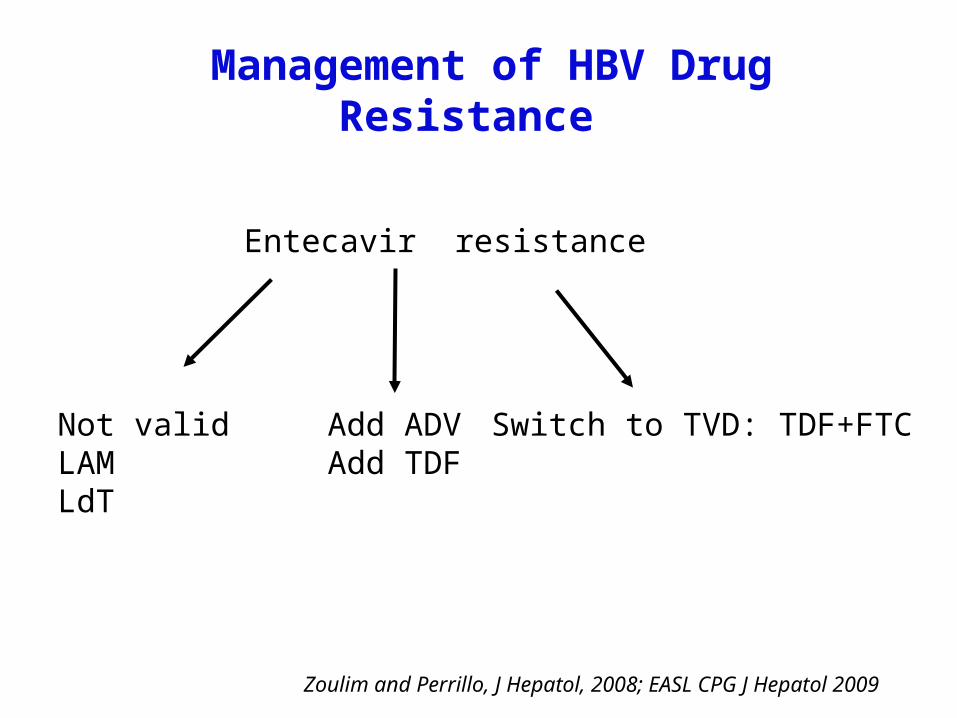
Entecavir resistance
Add ADVAdd TDF
Switch to TVD: TDF+FTCNot validLAMLdT
Management of HBV Drug Resistance
Zoulim and Perrillo, J Hepatol, 2008; EASL CPG J Hepatol 2009
Add-on or switch ?

Zoulim Antivir Res 2004;Villeneuve et al J Hepatol 2003; Lampertico et al Gastroenterology 2007
+
LAM
ADV
Add-on therapy with drugs having a complementary cross-resistance profile
Wild type
LAM-R
ADV-R
ADVLAM

HBV DNA ALT
The problem of sequential therapy and switching strategy
Villeneuve et al, J Hepatol 2003
N236T
Ser
um
HB
V D
NA
(L
og1
0 c
opi e
s/m
L)
ALT
(IU/L )
300
250
200
150
100
50
L180M+M204V
LAM
ADV
Reverted to wild type
2
3
4
5
6
7
8
9
10
janv-98 janv-99 janv-00 janv-01 janv-02 janv-03 janv-04 janv-05
LAM
Months
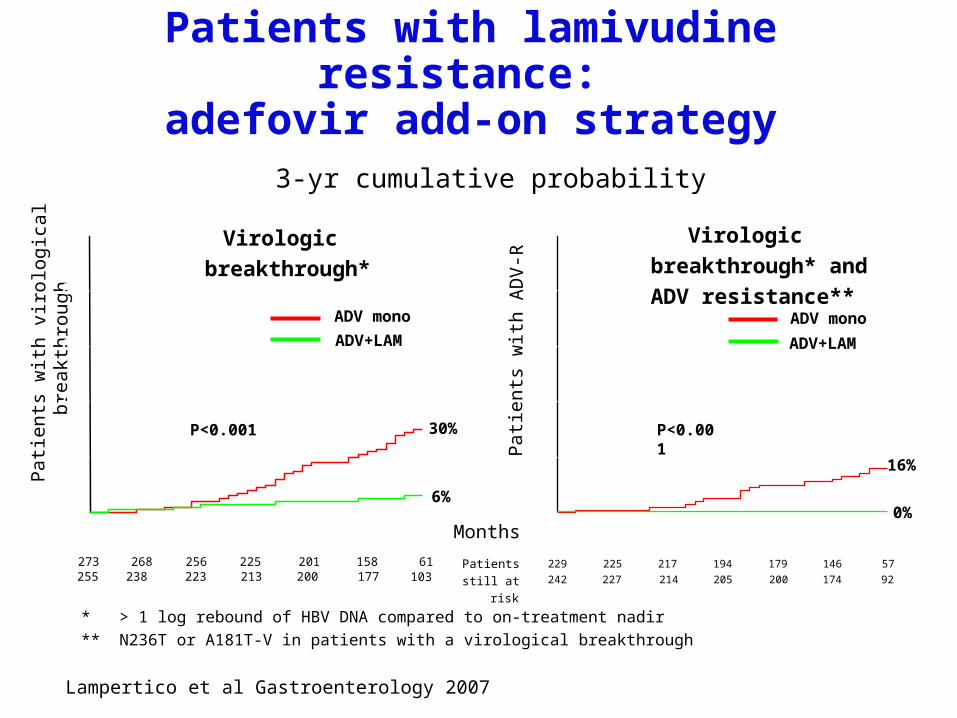
ADV mono
Pat
ient
s w
i th v
irolo
gica
l bre
a kth
roug
h
273 268 256 225 201 158 61
30%
6%
P<0.001
ADV+LAM
255 238 223 213 200 177 103
Pat
ient
s w
i th A
DV
-R
229 225 217 194 179 146 57
16%
0%
P<0.001
ADV mono
ADV+LAM
242 227 214 205 200 174 92
3-yr cumulative probability
* > 1 log rebound of HBV DNA compared to on-treatment nadir
** N236T or A181T-V in patients with a virological breakthrough
Patients
still at risk
Virologic breakthrough* Virologic breakthrough*
and ADV resistance**
Lampertico et al Gastroenterology 2007
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27 30 33 36
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27 30 33 36
Patients with lamivudine resistance: adefovir add-on strategy
When changing treatment ?
M0
M6
M1
2
M1
8
M2
4
M3
0
M3
6 ALT0
2
4
6
8
ALT HBV DNA
Month of therapy
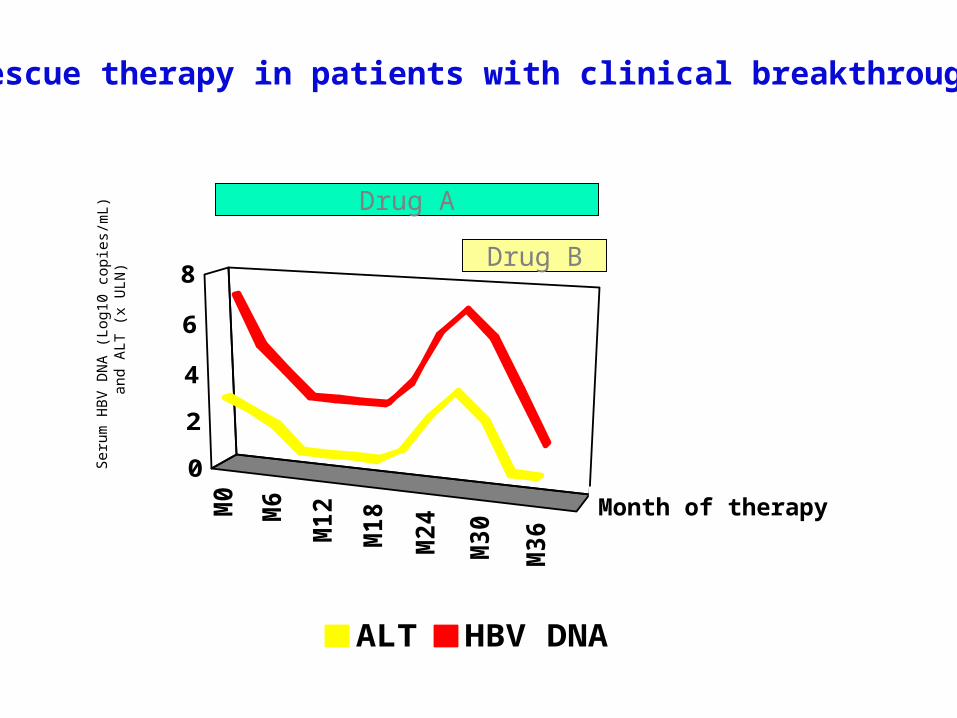
Rescue therapy in patients with clinical breakthrough
Drug A
Drug B
Seru
m H
BV
DN
A (
L og1
0 c
opi e
s /m
L )
an
d A
LT (
x U
LN)

M0
M6
M1
2
M1
8
M2
4
M3
0
M3
6
ALT0
2
4
6
8
ALTHBV DNA
Month of therapy
Rescue therapy in patients at the time of virologic breakthrough
Drug A
Drug B
Seru
m H
BV
DN
A (
L og1
0
c op
i es/
mL )
an
d A
LT (
x U
LN)
Zoulim and Perrillo, J Hepatol, 2008; EASL CPG J Hepatol 2009
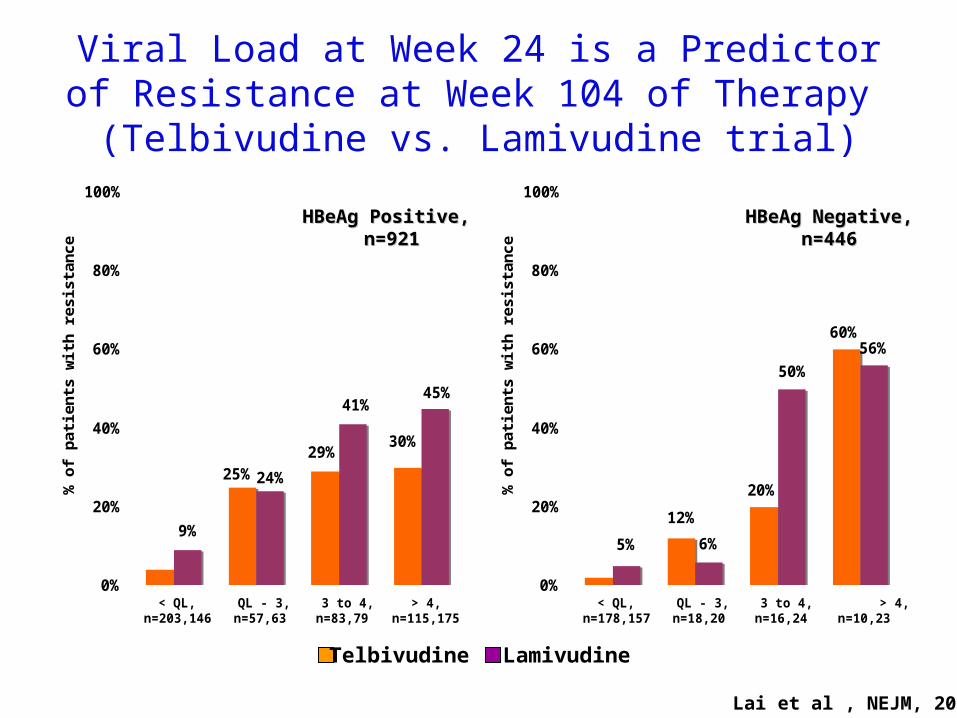
Viral Load at Week 24 is a Predictor of Resistance at Week 104 of Therapy
(Telbivudine vs. Lamivudine trial)
4%
25%29%
30%
9%
24%
41%45%
0%
20%
40%
60%
80%
100%
< QL,n=203,146
QL - 3,n=57,63
3 to 4,n=83,79
> 4,n=115,175
% o
f pat
ient
s w
ith
resi
stan
ce
2%
12%
20%
60%
5% 6%
50%
56%
0%
20%
40%
60%
80%
100%
< QL,n=178,157
QL - 3,n=18,20
3 to 4,n=16,24
> 4,n=10,23
% o
f pat
ient
s w
ith
resi
stan
ce
Telbivudine Lamivudine
HBeAg Positive, HBeAg Positive, n=921n=921
HBeAg Negative, HBeAg Negative, n=446n=446
Lai et al , NEJM, 2007
M0
M6
M1
2
M1
8
M2
4
M3
0
M3
6
ALT0
2
4
6
8
ALTHBV DNA
Month of therapyMonth of therapy
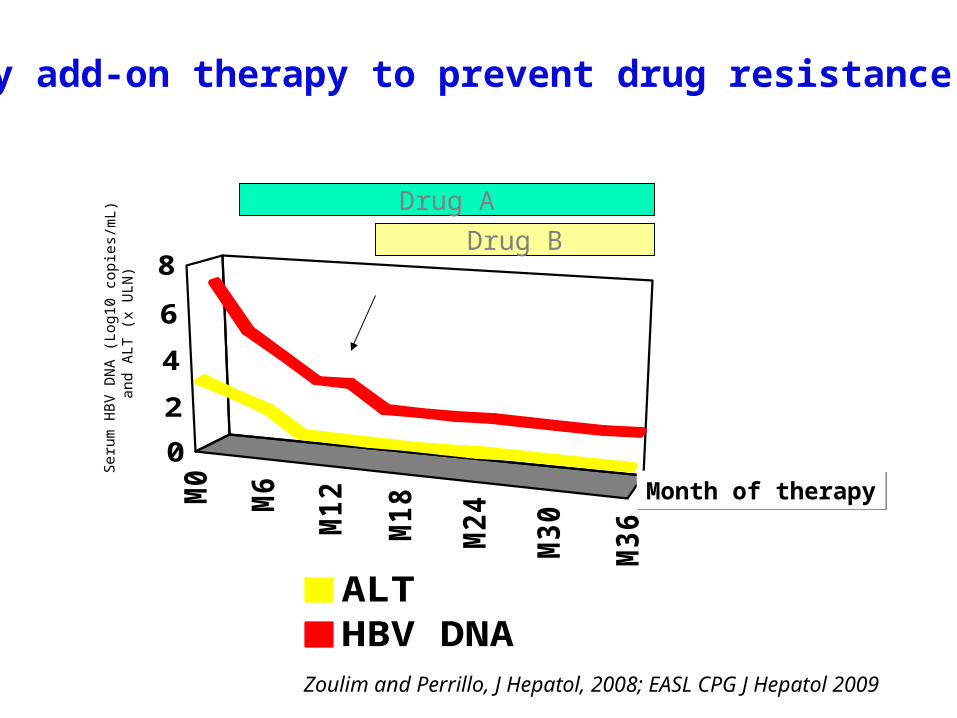
Early add-on therapy to prevent drug resistance
Drug A
Drug B
Seru
m H
BV
DN
A (
L og1
0 c
opi e
s /m
L )
and A
LT (
x U
LN)
Zoulim and Perrillo, J Hepatol, 2008; EASL CPG J Hepatol 2009

Secondary Treatment Preferences Based on Virologic Monitoring
Partial virologic response Virologic breakthrough
Nucleoside analog treatment
Add a more potent agent* or switch to a more potent combination
(emtricitabine/tenofovir*)
* Choice based on cross-resistance data
Monitorat 12-24 weeks
Early non reponse
Monitorevery 12 weeks
Switch to morepotent agent*
Zoulim and Perrillo, J Hepatol, 2008; EASL CPG J Hepatol 2009
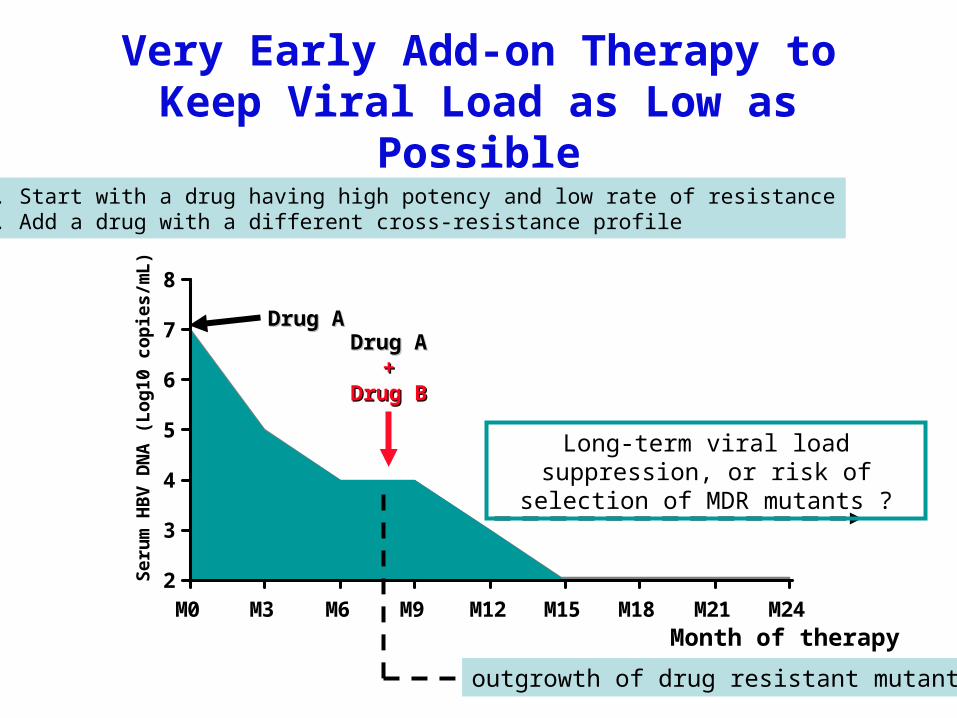
Very Early Add-on Therapy to Keep Viral Load as Low as Possible
2
3
4
5
6
7
8
M0 M3 M6 M9 M12 M15 M18 M21 M24
Se
rum
HB
V D
NA
(L
og
10
co
pie
s/m
L)
Drug ADrug ADrug ADrug A
++Drug BDrug B
Month of therapy
1. Start with a drug having high potency and low rate of resistance2. Add a drug with a different cross-resistance profile
outgrowth of drug resistant mutant?
Long-term viral load suppression, or risk of selection of MDR mutants ?
Prevention of drug resistance• First line therapy
– Use of antivirals with high antiviral potency and high barrier to resistance
– Combination therapy with complementary drugs
• Second line treatment– Add-on strategies with complementary drugs preferred to
sequential monotherapies
– Early treatment adaptation to prevent accumulation of mutations
– Choice always based on cross-resistance data
• It’s prime time for the next treatment objective– Clearance of HBsAg !
![A Direct Synthesis of Nucleoside Analogs Homologated at ...ffame.org/pubs/A direct synthesis of nucleoside analogs homologated at the 3 '- and 5... · crystal [14]. Longer sulfone-linked](https://img.pdfslide.net/doc/110x75/5d4d2a7c88c99309068b4874/a-direct-synthesis-of-nucleoside-analogs-homologated-at-ffameorgpubsa-direct.jpg)
![Non-radioactive Labeling - Jena BioscienceIn: Nucleoside Triphosphates and their Analogs (Vaghefi). CRC Press. [7] Anderson et al. (2005) Incorporation of reporter-labeled nucleotides](https://img.pdfslide.net/doc/110x75/5ed96491f59b0f56f45f6889/non-radioactive-labeling-jena-in-nucleoside-triphosphates-and-their-analogs-vaghefi.jpg)





![The efficacy and safety of methylprednisolone in hepatitis ...use of methylprednisolone (MP) in HBV-ACLF is still uncertain and controversial [13]. With the coming of nucleoside analogs](https://img.pdfslide.net/doc/110x75/60a58b90b7f2c771c8337391/the-efficacy-and-safety-of-methylprednisolone-in-hepatitis-use-of-methylprednisolone.jpg)