Embed Size (px)
Citation preview
PEPTIC ULCER DISEASE
Dr. Saelinger Microbiology
Dr. Noffsinger Pathophysiology
Dr. Long Clinical presentation
Dr. Goldberg Treatment
HELICOBACTER PYLORI
Background
Human stomach long considered inhospitable forbacteria
Spiral shaped organisms occasionally visualized ingastric mucous layer, but no evidence of diseaseassociation
Organism classified first as Campylobacter pylori
Now Helicobacter pylori
Other species of Helicobacter isolated fromstomach, intestine of other animals
Marshall and Warren culture organism from humangastric mucosa and show association with gastricinflammation
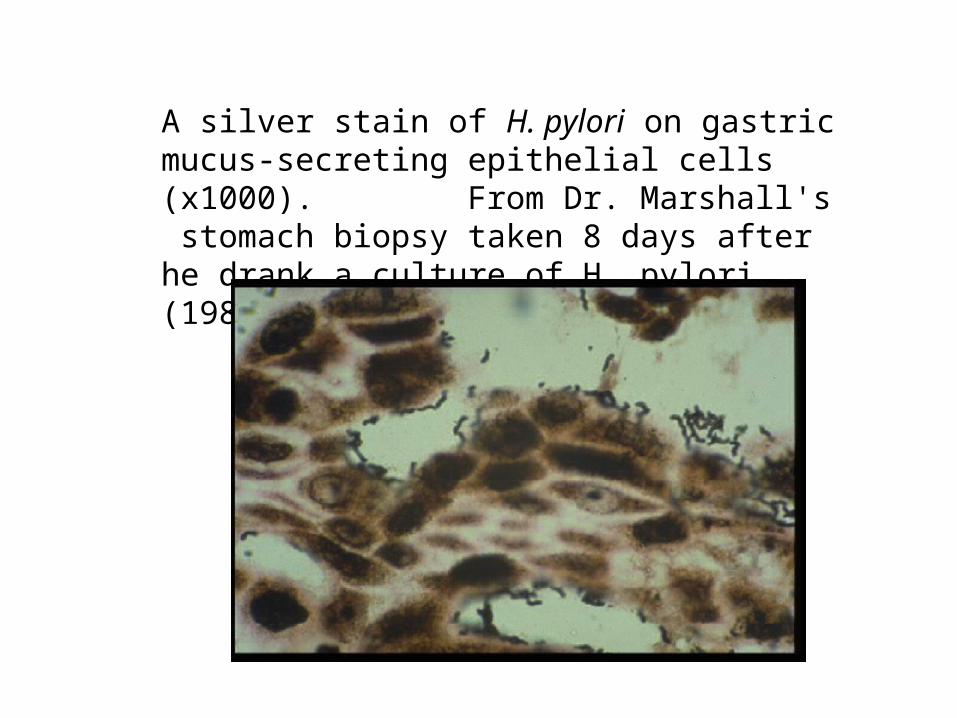
A silver stain of H. pylori on gastric mucus-secreting epithelial cells (x1000). From Dr. Marshall's stomach biopsy taken 8 days after he drank a culture of H. pylori (1985).

MICROBIOLOGY
1. Gram negative, spiral, flagellated(motile) bacilli
2. Slow growing, requires complexmedia, microaerophilic
3. Oxidase and catalase positive
4. Produces urease
5. Noninvasive; proliferates inmucus overlying gastric typemucosa
6. Not cleared by host immuneresponse
TRANSMISSION
1. Humans are major - if not only - reservoir
2. Transmission believed to be by fecal-oralroute
organism can be cultured from feces family members often carry same strain prevalence of infection likely related to
inferior hygienic conditions and poorsanitation
infection from environment or from animalscannot be totally excluded
EPIDEMIOLOGY
1. Gastric colonization rate in developing countries isabout 80%
Very high from early childhood
2. Gastric colonization rate in US and otherdeveloped countries is about 30%
3. Prevalence of infection increases with age
Age 10 = ~5%Age 30 = ~ 25%Age 60 = ~ 50%
4. In US, prevalence rates are higher in African-Americans and Hispanics
5. Age and low income = main risk factors for H.pylori infection
Nearly all H. pylori colonized persons have gastric inflammation - but this - by itself is asymptomatic.
Symptoms are due to illness - such as peptic ulceration or gastric malignancy.
Develop in <10% individuals colonized with H. pylori.
Over 80% peptic ulcers related to H. pylori colonization.
Evidence supporting H. pylori as major causeof peptic ulcer disease
1. H. pylori is found in almost all cases of PUD, whenthe use of NSAIDs is definitely excluded
2. When H. pylori is treated and eradicated, the rateof ulcer recurrence is dramatically reduced
3. H. pylori induced changes in acid secretion andmucosal resistance provide a plausiblepathophysiologic explanation
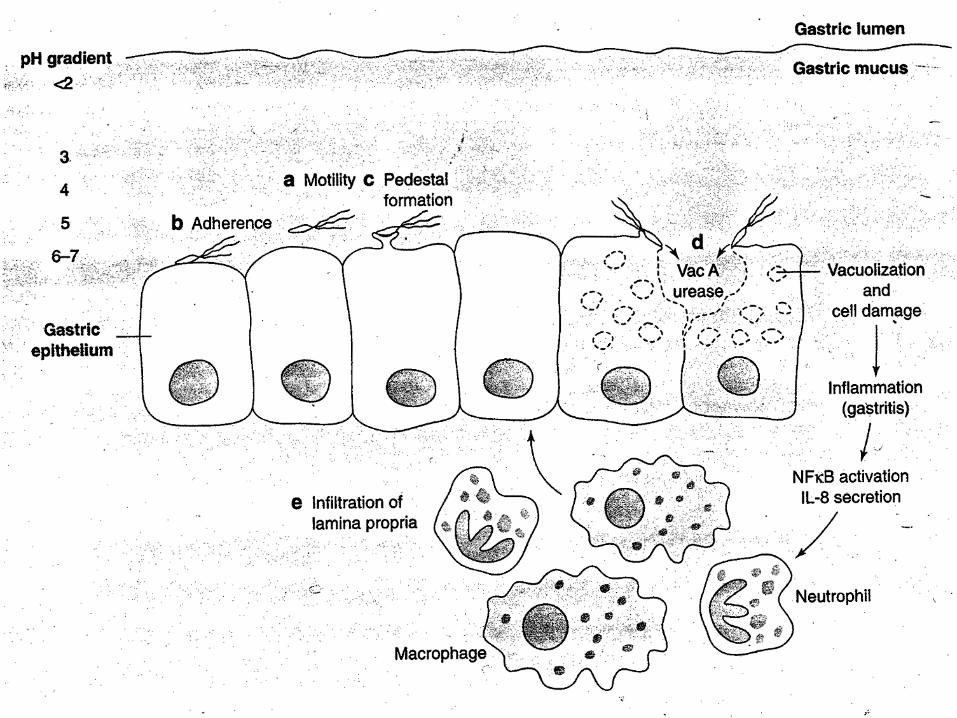
PATHOGENESIS
Colonization
1. Most bacteria killed in hostile environment of gastriclumen
2. H. pylori proliferates in mucus layer over epitheliumand is not cleared by host immune response
3. H. pylori survives and grows there because of avariety of virulence factors that contribute to gastricinflammation, alter gastric acid production, and causetissue destruction.
VIRULENCE FACTORS
Initial colonization facilitated by:
Acid inhibitory protein - blocks acid secretion from parietal cells during acute infection
Urease - neutralizes gastric acids due to ammonia production. [also stimulates monocytes and neutrophil chemotaxis; stimulates production of inflammatory cytokines]
Heat shock protein - enhances urease expression; co-expressed with urease on bacterial surface
Flagella - allows penetration into gastric mucous layer
Adhesins - mediate binding to host cells
Localized tissue damage mediated by:
Mucinases and phospholipases - disrupt gastric mucus
Vacuolating cytotoxin - induces vacuolation in epithelial cells that results in epithelial cell damage
All these factors plus LPS stimulate inflammatory response
SOD and catalase - prevent from phagocytosis and intracellular killing
Plus other poorly defined factors that stimulate IL-8 secretion by epithelial cells, that induce nitric oxide synthase which mediates tissue injury, and that induce programmed death of gastric epithelial cells.
Cag pathogenicity island - includes genes that confer enhanced pathogenicity, in part by inducing epithelial cells to produce proinflammatory cytokines