Embed Size (px)
Citation preview

Human Error and SafetyLecture 15
University of Michigan Human Factors Engineering Short Course
2016
Douglas A. Wiegmann, Ph.D.Department of Industrial and Systems Engineering
University of [email protected]
Overview and Objectives
Part 1: Background
• System Safety
• Human Error and Safety
• Models and Methods for Error Analysis
Part 2: Application (Healthcare)
• Identifying Factors that Cause Errors in the Operating Room
• Developing Interventions
Types of Safety
• System Safety (“three legged stool”)• Individual (employee Safety)
• Occupational Health and Safety• OSHA – Occupational Safety and Health
Administration (OHSA)• Environmental
• Environmental Protection Agency (EPA)• Process Safety (reliability)
• e.g., Nuclear Regulatory Agency, The Department of Transportation, Department of Energy
Approaches to Safety
• Proactive Approaches• Proactive Risk Assessment• Safety Audits• Near miss reporting Systems
• Reactive Approaches• Accident and Incident Investigation

Health Care – Root Cause Analysis (RCA) of significant patient-safety events is required for accreditation.
• For more information see the Joint Commission on Accreditation of Healthcare Organizations [JCAHO] at www.jointcommission.org or the National Quality Forum [NQF] at www.qualityforum.org
Standards and Regulations
Military – Mishap investigation rules and procedures are outlined in directives for each branch.
•For the Navy see OPNAV3750 at http://doni.daps.dla.mil/Directives/03000%20Naval%20Operations%20and%20Readiness/03-700%20Flight%20and%20Air%20Space%20Support%20Services/3750.6R.pdf or visit the Naval Safety Center at safetycenter.navy.mil
Standards and RegulationsTransportation: Rules for conducting investigations concerning transportation accidents (aviation, railway, maritime, and pipeline are contained in the code of federal regulations.
• For information regarding investigations of civil aviation accidents, see CFR Title 49 at http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c=ecfr&tpl=/ecfrbrowse/Title49/49cfr830_main_02.tpl or visit the National Transportation Safety Board (NTSB) at www.ntsb.gov
Human Error and Safety
Error – “…occasions in which a planned sequence of mental or physical activities fails to achieve its intended outcome and when these failures cannot be attributed to the intervention of some chance agency.” (Reason, 1990).
Human Error and SafetyReason’s General Error-modeling System (GEMS)

(Swain and Guttman, (1983)
Human error probabilities for specific tasks
Human Error and Safety
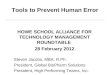
However, the rate of human error accidents has remained relatively stable over the past 20 years, whereas accidents associated with mechanical failures have been virtually eliminated.
Human error is associated with 60-80% of accidents in complex systems, including aviation, nuclear power, mining and health care.
All NAVY/MARINE Class A, B, & C Mishaps
Shappell, S. and Wiegmann, D. (1996). U.S. Naval aviation mishaps 1977-1992: Differences between single and dual-piloted aircraft. Aviation, Space, and Environmental Medicine, 67, 65-69.
Acci
dent
s/10
0,00
0 fli
ght h
ours
Cla
ss A
, B,&
C M
isha
ps/1
00,0
00 F
light
Hou
rs
0
2
4
6
8
10
12
14
16
1977
1979
1981
1983
1985
1987
1989
1991
Year
Mechanical
Human
Human Error Interventions
Development of interventions that effectively reduce the occurrence and/or consequences of errors is onerous. Brennan et al, 2005
• Factors that actually contribute to errors in many domains remain poorly understood. underdeveloped/under-specified concepts and models of human error
varying philosophical perspectives concerning the underlying causal mechanisms of errors
unsystematic and fragmented efforts

Initiation of Action/Procedure
Appropriate Action
Error Cause-Factor Present?
Desired Outcome
No
Causes and Consequences of Errors
Initiation of Action/Procedure
Appropriate Action
Error Cause-Factor Present?
Error or Unsafe Act
Desired Outcome
Yes
Error Detected/ Captured?
YesNo
Causes and Consequences of Errors
Initiation of Action/Procedure
Appropriate Action
Error Cause-Factor Present?
Error or Unsafe Act
Desired Outcome
Yes
No
No
Causes and Consequences of Errors
Undesired Outcome
Error Detected/ Captured?
Yes
Initiation of Action/Procedure
Appropriate Action
Error Cause-Factor Present?
Error Detected/ Captured?
Desired Outcome
Yes
YesNo
No
Error or Unsafe Act
Reputation & Accusation
Undesired Outcome
Causes and Consequences of Errors: Human Focus

• Focuses on errors and procedural violations of individuals
• Unsafe acts arise from aberrant mental processes such as inattentiveness, lack of good judgment, forgetfulness, recklessness, or even negligence.
• Interventions are directly aimed at reducing the “unwanted variability” in human behavior.
• Common methods include retraining, recurrent proficiency tests, disciplinary measures, or even termination and litigation.
• When taken to the extreme, errors are viewed as a moral issue, with the notion that bad things (i.e., errors) happen to bad people.
Traditonal Perspective
• Focuses on errors and procedural violations of individuals
• Unsafe acts arise from aberrant mental processes such as inattentiveness, lack of good judgment, forgetfulness, recklessness, or even negligence.
• Interventions are directly aimed at reducing the “unwanted variability” in human behavior.
• Common methods include retraining, recurrent proficiency tests, disciplinary measures, or even termination and litigation.
• When taken to the extreme, errors are viewed as a moral issue, with the notion that bad things (i.e., errors) happen to bad people.
Traditional Perspective
• Humans are fallible and errors are to be expected, even in the best organizations.
• Errors are consequences of deficient processes and/or system failures rather than simply causes of bad outcomes.
• Consistency in performance is important but flexibility is also invaluable during dynamic operations.
• Countermeasures are based on the assumption that “though we cannot change the human condition, we can change the conditions under which humans work.”
• The best people can make the worst mistakes. The important issue is not who blundered but how and why the defenses failed.
Systems Perspective
Initiation of Action/Procedure
Appropriate Action
Error Cause-Factor Present?
Error Detected/ Captured?
Desired Outcome
Yes
YesNo
No
Error or Unsafe Act
Reputation & Accusation
Undesired Outcome
Causes and Consequences of Errors: Traditional Focus
Appropriate Action
Error Cause-Factor Present?
Error or Unsafe Act
Error Detected/ Captured?
Undesired Outcome
Desired Outcome
Yes
YesNo
No
Initiation of Action/Procedure
Causes and Consequences of Errors: Systems Perspective
What are the mechanisms of error detection
and why do these mechanisms
sometimes fail?
What are the underlying factors that commonly
cause errors?

Error Prevention
Appropriate Action
Error Cause-Factor Present?
Error or Unsafe Act
Error Detected/ Captured?
Desired Outcome
Yes
YesNo
No
Error Management
Undesired Outcome
Initiation of Action/Procedure
Causes and Consequences of Errors: Systems PerspectiveModels and Methods
• Variety of Approaches– Theoretical vs. Applied– Focused vs. Broad– Analysis vs. Prediction– Hybrid
• Multiple Names– Probability risk assessment (PRA)– Human reliability assessment (HRA)
Inputs
Adapted from Reason (1990)
Accident & Injury
“Swiss-cheese” Model of Accidents
OrganizationalFactors
UnsafeSupervision
Preconditionsfor
Unsafe Acts
UnsafeActs
Failed orAbsent Defenses
UnsafeActs
Routine Exceptional
ViolationsErrors
DecisionErrors
Skill-basedErrors
PerceptualErrors
Preconditionsfor Unsafe Acts
Crew ResourceManagement
PersonalReadiness
PersonnelFactors
Condition ofOperators
AdverseMental States
AdversePhysiological
States
Physical/Mental
Limitations
PhysicalEnvironment
TechnologicalEnvironment
EnvironmentalFactors
UnsafeSupervision
SupervisoryViolations
InadequateSupervision
PlannedInappropriate
Operations
Failed toCorrectProblem
OrganizationalInfluences
ResourceManagement
OrganizationalClimate
OperationalProcess
Human Factors Analysis and Classification System
®

Root Causes Analysis
Source: http://withfriendship.com/user/mithunss/root-cause-analysis.php
Root Causes Analysis
Subsystem/Name: DC motor P = Probabilities (chance) of OccurrencesModel Year/Vehicle(s): 2000/DC motor S = Seriousness of Failure to the Vehicle
D = Likelihood that the Defect will Reach the customer R = Risk Priority Measure (P x S x D)
1 = very low or none 2 = low or minor 3 = moderate or significan 4 = high 5 = very high or catastrophic
No. Part NamePart No.
Function FailureMode
Mechanism(s) & Causes(s) of
Failure
Effect(s)Of Failure
CurrentControl
P.R.A. RecommendedCorrective Action(s)
Action(s)Taken
P S D R
1 PositionController
Receive a demand position
Loose cable connection
Incorrect demand signal
Wear and tear
Operator error
Motor fails to move
Position controller breakdown in a long-run
2
4
4
4
1
3
8
48
Replace faulty wire. Q.C checked.
Intensive training for operators.
FMEA is intended to document:a Failure its Mode its Effect
by Analysis
FAILURE MODE AND EFFECTS ANALYSIS (FMEA)
Move to next Failure Possibility

Other Approaches
• Technique for Human Error Rate Prediction (THERP)
• Maintenance Error Detection Aid (MEDA)• Operator Action Trees (OATS)
Part 2: Application
• Identifying Factors that Cause Errors in the Operating Room
• Developing Error Management / Patient Safety Programs
Human Error in Healthcare
Within the U.S. health care system, “more than 1 million patients are injured and approximately 180,000 die each year” due to medical error – roughly equivalent to the number of deaths that would occur if three commercial airliners crashed every two days. (Andrews LB, Stocking C, Krizek T, et al. 1997)
As a result, deaths due to medical error the 8th leading cause of death in the United States (U.S.), ahead of motor vehicle accidents, breast cancer and AIDS. (Leape 1994)
Not surprising, errors during surgical operations are among the most common in the healthcare industry.
Patient Safety in the ORA marker of surgical excellence is the ability to successfully manage distractions and errors during surgery (de Leval et al., 2000).
•However, even experienced surgical teams can become mired by minor problems that disrupt surgical flow.
•As the number of minor events increase, the likelihood that the surgical team is able to cope with a major event decreases.
•Minor events appear to exert an additive effect by cumulatively eroding the limited compensatory resources of the surgical team (Reason, 2001).
What are the factors that determine a surgeon’s ability to perform well and produce good outcomes?
There are two perspectives….
Human Factors and Cardiac Surgery: A Multicenter Study (de Leval, et al. 2000)

OutcomePatient Risk Factors
Surgeon Factors
“Once outcomes (usually mortality) have been correctly adjusted for patient risk factors, the remaining variance is assumed to be explained by individual surgical skill.” Vincent et al. (2004). Annals of Surgery 239(4): 475-82.
Traditional (Person-Centered) Perspective“Refinements in skill may be a relatively small element in the drive to reduce mortality from 10% to 1%. Optimizing the surgical environment, attention to ergonomics and equipment design, understanding the subtleties of decision making in a dynamic environment, enhancing communication and team performance may be more important than skill when reaching for truly high performance.” Vincent et al. (2004). Annals of Surgery 239(4): 475-82.
Systems Perspective: The “Operational Profile”
OutcomePatient Risk Factors
Surgeon Factors
OutcomePatient Risk Factors
Surgeon Factors
“Refinements in skill may be a relatively small element in the drive to reduce mortality from 10% to 1%. Optimizing the surgical environment, attention to ergonomics and equipment design, understanding the subtleties of decision making in a dynamic environment, enhancing communication and team performance may be more important than skill when reaching for truly high performance.” Vincent et al. (2004). Annals of Surgery 239(4): 475-82.
Systems Perspective: The “Operational Profile”
HFACS (flow disruptions)
Environmental Factors• Equipment Design• Extraneous distractions
Social Factors (CRM)• Teamwork• Communication• Familiarity
Supervisory Factors• Training• Staffing• Scheduling
Organizational Factors• Resources• Climate• Process
Purpose of the Study
Specific Aim 1 —Describe frequency andnature of surgical flowdisruptions
Specific Aim 2 —Test hypothesis that surgicalflow disruptions are associatedwith surgical errors
• Develop– Evidence-based interventions– Methodology/measurement
tools for validating patient safety initiatives
Wiegmann et al., 2006

• When the number, location, and extent of coronary artery stenosis injuries (occlusions) present a significant risk of heart attack for the patient, surgery is the preferred method of treatment.
• The principal methods of surgery for treatment of CAD involve bypassing blockages in coronary arteries with a blood vessel taken from another part of the patient's body.
• The standard procedure is called Coronary Artery Bypass Grafting (CABG) surgery, or simply coronary artery bypass surgery. Today CABG surgery is one of the most common surgical procedures.
• Other types of procedures include valve replacement/replacement, aortic root repair, heart transplant, etc.
Task: Open-heart Surgery•The surgery is done by opening the patient's chest with an incision over the sternum (breast bone) and dividing it to expose the heart.
•Simultaneously, the greater saphenous vein from one of the patient's legs is "harvested" to be used for the bypass procedure.
•During the operation the patient's heart is connected to a heart-lung machine which is used to circulate and oxygenate the blood while the heart is stopped.
•Depending on the number and location blockages, the surgeon might perform between one and seven bypasses. When the bypasses are completed, the heart is restarted.
•Once the heart beats normally the patient is removed from the heart-lung machine and the chest is closed up, the sternum is stabilized with stainless steel wire suture, and the chest and leg wounds are closed with sutures or clips.
•Recovery is required in and ICU for approximately two days. Barring any complications, a total hospital stay of 7 to 10 can be expected.
Task: Open-heart Surgery
• Surgeons • Residents/Fellows• Anesthesiologists• Nurse Anesthetists• Circulating Nurse• Surgical Technicians• Surgical Assistants• Perfusionists• Monitor Technicians
Members of the Surgical Team Method and ProceduresSample of Surgical Cases• 31 cardiac surgical cases observed across three-week
study period and five surgeons performing multiple procedures
– Coronary Artery Bypass Graft (CABG) n = 13– Valve repair/replacement 6– CABG and valve repair 4– Aortic root replacement 3– Other 5
• Observations occurred during high-risk portion of procedure– Time in which cardiopulmonary bypass was initiated
and time in which patient was successfully weanedfrom bypass pump
• Data reflect ~42 hrs of observation

Teamwork/Communication
Results: Surgical Flow Disruptions
“Surgeon was under the impression that the patient had been given inotropes as he had previously asked, but none had been given. After surgeon again asked the CRNA if inotropes had been given,she stated they had not and then turned the inotropes on”
52%
0 10 20 30 40 50 60%
Teamwork
n=341, 8.10/hr,11+5.56/case
“Surgeon’s pager went off in the room, circulating RN answered call”
Teamwork/CommunicationExternal/extraneous interruptions
52%
17%
0 10 20 30 40 50 60%
Teamwork
Externalinterruptions
Results: Surgical Flow Disruptions
n=341, 8.10/hr,11+5.56/case
“Surgical assistant trainee unfamiliar with technique of clamping down purse string stitches on aorticcannula and needed to be taught”
Teamwork/CommunicationExternal/extraneous interruptionsSupervisory/training distractions 52%
17%
12%
0 10 20 30 40 50 60%
Teamwork
Externalinterruptions
Training
Results: Surgical Flow Disruptions
n=341, 8.10/hr,11+5.56/case
“Cryocath machine should go for 60 seconds but stopped freezing at 19 seconds…no one knew why the machine had stopped; freezing was reattempted and machine worked the second time”
Teamwork/CommunicationExternal/extraneous interruptionsSupervisory/training distractionsEquipment/technology problems
52%
17%
12%
11%
0 10 20 30 40 50
60%
Teamwork
Externalinterruptions
Training
Equipment
Results: Surgical Flow Disruptions
n=341, 8.10/hr,11+5.56/case

“Surgeon requested a 7.0 prolene stitch which was not at the table… circulating nurse went to retrieve from the core, returned several minutes later”
Teamwork/Communication
n=341, 8.10/hr,11+5.56/case
52%
17%
12%
11%
7%
0 10 20 30 40 50 60%
Teamwork
Externalinterruptions
Training
Equipment
Resources
External/extraneous interruptionsSupervisory/training distractionsEquipment/technology problemsResource accessibility
Results: Surgical Flow Disruptions Results: Surgical Errors
The vast majority of errors were relatively minor
“While reducing stenosis, surgeon perforated the vein graft and a new stitch was placed to reseal graft.”
“A hole was created in artery while dissecting and a stitch was used to seal the punctured area.”
“After the cross clamp was removed, surgeon became aware of a leaking anastomosis.”
“Upon double checking the integrity of an aortic value replacement, the surgeon noticed that the wrong stitch had been used. The correct stitches were identified and the procedure was redone.”
n=148, 3.5/hr, 5.0/case
All events were managed without intraoperative mortality
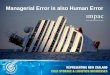
Flow Disruptions and Error Occurrence
Flow Disruption (rate/hr)
(Unstandardized Predicted Value)
Erro
r (ra
te/h
r)
r2= 0.627, p < .01
Flow Disruptions and Error Occurrence
Flow Disruption (rate/hr)
(Unstandardized Predicted Value)
Erro
r (ra
te/h
r)
r2= 0.49, p < .01

Timing of Detection
• Immediate Detection ~ 60%.• Delayed Detection ~ 40%
• Immediate - had direct impact on progress of operation; had clear visual effects on the operative site and/or required immediate correction.
• Delayed - detected through use of standard/conventional protocols for verifying procedures; problem did not require immediate correction.
Error ManagementAgent of Detection
• Person who committed error ~ 53%• Person who did not commit error ~ 47%
0
10
20
30
40
50
60
70
80
90
100
Immediate Delayed
Timing of Error Detection
Perc
ent (
%)
Person who committed error
Person who did not commit error
Error detected by:
OR = 2.74 (95% CI: 1.3928 - 5.3744).
• The largest percentage of surgical errors was detected by the surgeon.
• A larger percentage immediately captured errors (65.5%) were detected by the same individual who committed the error verses only 41% of delayed captured errors.
• Delayed captured errors were 2.74 times more likely to be caught by someone other than the person committing the error than were errors that were captured immediately.
Results: Errors Detection
Discussion
Surgical errors occur on a regularbasis, tend to be minor, are detectedby surgical team, and managedappropriately without incidentNonetheless…
– Minor technical errors can havemajor effects on patient safety if notdetected and corrected in a timely manner
– Minor errors can decrease ability of a surgicalteam to cope with major events decreases(de Leval et al., 2000)
Discussion
• Understanding why errors occur(even minor errors) is importantfor developing effective error-management programs
• Errors are significantly associatedwith surgical flow disruptions –including teamwork problems,equipment factors, extraneousdistractions, training-relatedissues, and resource accessibility

• Pre-operative briefings
Addressing Human Factors Issues
Addressing Human Factors Issues
The goal of this project was to “...develop, implement, and evaluate apreoperative briefing for cardiovascular surgery.”
“After implementation..., there was a reduction in total surgical flow disruptions per case including miscommunication events ...On average, briefed teams experienced fewer trips to the core and spent less time in the core ...and there was a trend toward decreased waste .”
• Pre-operative briefings
Addressing Human Factors Issues
Addressing Human Factors Issues
• Standardization of communication
“Intraoperative communication was assessed before (n =18) and after (n =16) introduction of a structured communication protocol... Frequency of communication breakdowns per case decreased significantly after implementation.”
• Pre-operative briefings
• Usability of Technology
• Standardization of communication
Addressing Human Factors Issues
Addressing Human Factors Issues
“This project is the first step in the process of developing a new perfusion pump system that is specifically designed to reduce operator errors and improve patient safety during cardiovascular surgery.”
Summary: Human Error InterventionsDevelopment of interventions that effectively reduce the occurrence and/or consequences of errors is onerous. Brennan et al, 2005
• Factors that actually contribute to errors in many domains are often poorly understood.
• However, a human factors approach can facilitate the identification of systems factors that impact errors and error management processes.
• As a result, targeted interventions can be developed and empirically validated!

Questions?Bibliography
(*Main References)
[1] de Leval MR, Carthy, J, Wright, DJ, Farewell, VT, Reason, JT. Human factors and cardiac surgery: A multicenter study. J. Thorac Cardiovsac Surg, 2000; 119(4): 661-672.
[2] Carthy J, de Leval, MR, Reason, JT. The human factor in cardiac surgery: Errors and near misses in high technology medical domain. Ann Thorac Surg 2001;72:300-3005).
[3*] Carthy, J, de Leval MR, Wright, DJ, Farewell, VT, Reason, JT. Behavioural markers of surgical excellence. Safety Science 2003; 41:409-425.
[4*] National Patient Safety Foundation, RCA2: Improving root cause analysis and actions to prevent harm. 2016
[5] Kohn LT, Corrigan JM, Donaldson MS. To err is human. Washington, DC: National Academy Press; 1999.
[6*] Wiegmann DA, Shappell SA. Human error approach to aviation accident analysis: the human factors analysis and classification system, Ashgate Press; 2003.
[7] Vincent C, Morrthy K, Sarker SK, Chang A, Darzi AW. Systems approaches to surgical quality and safety from concept to measurement. Annals of Surgery 2004; 239(4): 475-482.
[8] Healy AN, Undre S, Vincent CA. Developing observational measures of performance in surgical teams. Qaul Safe Health Care 2004; 13 (Suppl 1):i33-i40.
[9] Reason J. Human error: Models and management. BMJ 2000; 320: 768-770.
[10] Brennan TA, Gwande A, Thomas E, Studdert D. Accidental deaths, saved lives, and improved quality. NEJM 2005; 13:1405-1409.
[11] Grogan EL, Stiles RA, France DJ, Speroff T, Morris JA, Nixon B, Gaffney FA, Seddon R, Pinsoin CW. The impact of aviation-based teamwork training on the attitudes of health-care professionals. J. Am Coll Surg2004; 8: 843-848.
[12*] Lingard L, Espin S, Whyte S, Regehr G, Baker GR, Reznick R, Bohenen J, Orser B, Doran D, Grober E. Communication failures in the operating room: An observational classification of recurrent types and effects. Qual Saf Health Care 2004; 13:330-334.
[13] Dhillon, BS. Human reliability and error in medical system. World Scientific; New Jersey. 2003
[14] Hollnagel, E. Cognitive reliability and error analysis method. Oxford; New York. 1998

[15*] Rosenthal, M. Sutcliffe K. Medical error: what do we know? What do we do? Jossey-Bass; San Francisco. 2002
[16] Diller et al.,The Human Factors and Analysis System (HFACS) applied to health Care. 2013; Am Jn of Med Qaul., 29(3), 181-90.
[17] Guerlain S, Adams RB, Turrentine FB, Shin T, Guo H, Collins SR, Calland JF. Assessing team performance in the operating room: development and use of a “black box” recorder and other tools for the intraoperative environment, J. Am Coll of Surg 2005; 2000:29-37.
[18] Swain, A.D., Guttman, H.E., 1983. Handbook of Human Reliability Analysis with Emphasis on Nuclear Power Plant Applications, NUREG/CR-1278, USREG, Washington, DC.
[19*] Gawande, A. The Checklist Manifesto: How to Get Things Right; New York: Metropolitan Books. 2010.
[20] Godon et al. Beyond the Checklist: What Else Health Care Can Learn from Aviation Teamwork and Safety. Cornell Univ. Press. 2013
[21*] Wiegmann, D.A., ElBardissi, A.W., Dearani, J.A., Daly, R.C., & Sundt, T.M. Disruptions in surgical flow and their relationships to surgical errors: An exploratory investigation. Surgery 2007; 142, 658-665.
[22] Henrickson, S., Wadhera, R., Elbardiss, A., Wiegmann, D. & Sundt, T. Development and pilot evaluation of a preoperative briefing protocol for cardiovascular surgery. Journal of the American College of Surgeons, 2009; 208:1115-1123.

Appendix A:HFACS causal factors
• From: Wiegmann DA, Shappell SA. Human error approach to aviation accident analysis: the human factors analysis and classification system, Ashgate Press; 2003.