Embed Size (px)
Citation preview

© 2005 Nature Publishing Group
PERSPECTIVES
only 1–4% of transplanted murine lym-phoma cells formed colonies in spleens ofrecipient animals8,9. This low clonogenicpotential was also observed in humanleukaemia cells by Jim Griffin and colleaguesin 1985, who reported that acute myeloge-nous leukaemia (AML) blasts (a blast is ahaematopoietic tumour cell with very primi-tive morphology, indicative of an acuteleukaemia or lymphoma) formed colonies atlow frequency in methylcellulose10,11.
Also at this time, it was found that solid-organ cancer cells vary in their ability to prolif-erate in similar assays. In standard soft-agarassays, where colony formation provides a sur-rogate for transformation, Anne Hamburgerand Sydney Salmon found that only 1 in 1,000to 1 in 5,000 cells isolated from solid tumours(such as lung, ovarian and brain tumours)were capable of forming colonies12. In addi-tion, in 1961, experiments (which now couldnot be justified ethically) carried out byChester Southam and Alexander Brunschwigshowed that tumour cells that had been har-vested from patients with disseminated malig-nancy and then injected subcutaneously intothe same patients led to a low frequency oftumour formation, and that tumours wereonly initiated when over 1,000,000 cells wereinjected13. These observations led the investiga-tors to speculate that the entire population of atumour’s cells might arise from a few so-called‘cancer stem cells’12.
A normal stem cell is defined by its dualproperties of self-renewal and multilineagedifferentiation potential, and continuouslyrepopulates the mature cells of the organ
system that it serves. Although homeostaticpressures can dictate that a stem cell under-goes symmetric division to produce twodaughter cells that are either both stem cellsor both progenitor cells (this outcomedepends on need) stem cells are defined bytheir ability to divide asymmetrically.Through this process, the division of a stemcell results in the formation of two daughtercells — one of which is another stem cell,and the other of which is a committed prog-enitor that is capable of further differentia-tion and proliferation but lacks the ability toself-renew. A cancer stem cell would functionin a similar way to sustain the growth andspread of tumours while repopulating thedistinct cell types represented within thetumour. However, a cancer stem cell wouldnot be subject to the same intrinsic andextrinsic controls as normal stem cells.
This ‘cancer-stem-cell hypothesis’ repre-sents a modern-day interpretation of the pro-posal made by pathologists such as RudolphVirchow and Julius Cohnheim ~150 yearsago (TIMELINE) that cancer results from theactivation of dormant embryonic-tissue rem-nants14,15. This ‘embryonal-rest hypothesis’ ofcancer was based on the histological similari-ties between the developing fetus and certaintypes of cancer, such as teratocarcinomas14,and the observation that both tissues have anenormous capacity for both proliferation anddifferentiation, albeit aberrant differentiationin the case of tumours. There is substantialevidence in the literature to support thismechanism in paediatric cancers; nephro-genic rests (abnormally retained embryonickidney precursor cells arranged in clusters)that antedate the development of Wilm’stumour can be detected by ultrasound duringgestation16, and certain mutations can bedetected at birth that are associated with apredisposition to paediatric leukaemias.These mutations include the somaticTEL–AML1 (REF. 17), MLL–AF4 (REF. 18),AML–ETO (REF. 19) and OTT–MAL translo-cations, as well as constitutional trisomy 21(REF. 20). Van R. Potter and Barry Pierce
Abstract | Many cancers seem to dependon a small population of ‘cancer stem cells’for their continued growth and propagation.The leukaemia stem cell (LSC) was the firstsuch cell to be described. The origins ofthese cells are controversial, and theirbiology — like that of their normal-tissuecounterpart, the haematopoietic stem cell(HSC) — is still not fully elucidated.However, the LSC is likely to be the mostcrucial target in the treatment of leukaemias,and a thorough understanding of its biology— particularly of how the LSC differs fromthe HSC — might allow it to be selectivelytargeted, improving therapeutic outcome.
It is now half a century since bone-marrowreconstitution experiments, following lethalirradiation in mice, first indicated the exis-tence of the haematopoietic stem cell(HSC)1,2 — a cell first postulated to exist byArtur Pappenheim as early as 1917 (REF. 3).Although this cell population is still not fullycharacterized, its discovery awakened thefield of stem-cell biology. The recent discov-ery of many more tissue-specific stem cells4–7
has kept this field of study at the forefront ofbiological research.
At around the same time that the existenceof the HSC was postulated, observations werereported of the heterogeneous potential oftumour cells to self-renew both in vitro and invivo. For example, in 1973, Ernest McCullochand colleagues observed that only 1 in 100 to1 in 10,000 murine myeloma cells had theability to form colonies in vitro. In 1963,Robert Bruce and colleagues showed that
NATURE REVIEWS | CANCER VOLUME 5 | APRIL 2005 | 311
Leukaemia stem cells and theevolution of cancer-stem-cell research
Brian J. P. Huntly and D. Gary Gilliland
T I M E L I N E

© 2005 Nature Publishing Group
312 | APRIL 2005 | VOLUME 5 www.nature.com/reviews/cancer
P E R S P E C T I V E S
Based on functional and immunopheno-typic analysis of subpopulations of cells withmodern technologies, cancer has becomeviewed increasingly as a stem-cell disorder,in which the continued growth and propaga-tion of the whole tumour depends on asmall subpopulation of self-renewing cancerstem cells. The HSC was the first adultsomatic stem cell to be described. The exis-tence of cancer stem cells was also firstdescribed in the haematopoietic system. Thedemonstration of a leukaemia-initiating cell,now commonly referred to as the leukaemiastem cell (LSC), in AML and otherleukaemias, along with the subsequent iden-tification of cancer stem cells in breast andcentral-nervous-system (CNS) tumours,provides evidence for the broad applicabilityof the cancer-stem-cell model.
It is plausible that malignant stem cellsshare a number of biological features that are different from their normal-tissuecounterparts and that these might beexploited for therapeutic benefits. As malig-nant haematopoieisis is well characterizedand amenable to laboratory and clinicalinvestigation, further investigation of thebiology of the LSC could provide a para-digm for all cancer stem cells and couldimprove the therapy of both leukaemiasand other solid-organ cancers. In addition,
The haematopoietic system is amenable toex vivo analysis, and, in the late 1980s and1990s, developments in antibody technologyallowed investigators — such as IrvingWeissman and colleagues — to define theontogeny of this system, based on surfaceimmunophenotype in humans and mice (fora comprehensive review see REF. 25). Thesestudies identified a large number of pheno-typic markers that are associated with definedlineages and developmental stages ofhaematopoietic cells, and concomitantlyallowed the annotation of malignanthaematopoietic ontogeny. Another technicaladvance that greatly facilitated the characteri-zation of leukaemia and other cancer stem cellswas the development of high-speed multi-parameter flow cytometry. This is an auto-mated technique that is used to identifyand/or purify distinct cell populations, basedon the ability of fluorescently labelled antibod-ies to bind cell-surface antigens. Followingexcitation with a laser, the fluorochrome-bound antibody emits light of a specific wavelength, allowing the detection and enu-meration of cell populations that express theantigen. Furthermore, by applying an electriccharge to deflect populations that are positivefor a predefined fluorochrome, and thereforeantigen, these populations can be collected forfunctional analysis26,27.
updated these ideas in the 1970s and 1980s,describing cancer as the maturation arrest oftissue-determined stem cells21–23. However,formal proof of these hypotheses would haveto await further technological advances.
So, it seems that tumours are composedof a heterogeneous population of cells,within which resides a small population ofcancer stem cells that are exclusively respon-sible for the growth and propagation poten-tial of the whole tumour. However, an alternative hypothesis, the stochastic model,could also explain the heterogeneous poten-tial of tumour cells to self-renew. This modelpredicts that all tumour cells have the poten-tial to self-renew and recapitulate thetumour, but that the probability that anyparticular tumour cell enters the cell cycleand finds an environment permissive forgrowth in an assay of tumorigenesis is low24.To differentiate between these two models itis necessary to define distinct populations ofcells within tumours, based on surfaceimmunophenotypic or functional character-istics, to purify these populations to homo-geneity and to develop long-term assays oftheir functional ability. The functionalassessment of a cancer stem cell requires notonly the ability to form a new tumour, but torecapitulate precisely the phenotype of theinitial disease (BOX 1).
Rudolph Virchow proposes the‘embryonal-rest hypothesis’ oftumour formation, based onhistological similarities betweentumours and embryonictissues14. This theory, laterexpanded by other pathologistssuch as Julius Cohnheim,suggested that tumoursdevelop from residualembryonic tissues15.
Low in vivo clonogenicefficiency of mouselymphoma cellsdemonstrated byRobert Bruce andHugo Van der Gaag9.
1967–1981: Philip Fialkow and co-workers use patterns of X-linked geneinactivation in patient samples todemonstrate that leukaemias andmyeloproliferative disorders are clonalin origin. These studies also indicatethe involvement of an early stem orprogenitor cell in chronic myelogenousleukaemia and acute myelogenousleukaemia (AML)28–31.
1968–1973:development offluorescence-activated cell sortingby LeonardHerzenberg and co-workers121 and theproduction of the firstcommerciallyavailable machines27.
1989–1994: refinement of theSCID and non-obese diabetic(NOD)/SCID mouse assays forassessment of normal andleukaemic stem-cell functionby John Dick and colleagues,as well as other investigators.
Van R. Potter, BarryPierce and otherinvestigators extend theembryonal-resthypothesis to suggestthat tumours arise frommaturation arrest intissue-specific stem cells.
Advances in cell sorting withthe commercial manufactureof multiparameter high-speedmachines.
1980–1990s: creation ofmonoclonal antibodiesagainst numeroushaematopoietic cell-surface antigens.
Timeline | The evolution of cancer-stem-cell research
Characterizationof the NOD/SCIDimmunocompro-mised mouse123.
Irving Weissman andcolleagues are the first touse SCID mice as anassay system for humanhaematopoietic cells33.
1855 1961 1963 1967 1968 1970s 1985 1988 1989 1980 1990s 1992
Autotransplantation assays inhumans demonstrate a lowfrequency of tumour-initiating cells invarious solid-organ malignancies13.
James Till and Ernest McCullochsuggest the existence of thehaematopoietic stem cells, basedon experiments demonstrating theability of bone marrow to provideprotection to lethally irradiatedmice2.
Characterization of thesevere combinedimmunodeficiency (SCID)mutation in mice122.
Low clonogenic efficiencyof AML blasts in vitrodemonstrated by JimGriffin, Bob Lowenbergand co-workers10,11.

© 2005 Nature Publishing Group
P E R S P E C T I V E S
a better understanding of the relationshipbetween normal and cancer stem cellsmight provide insights that allow us to har-ness self-renewal programmes for regenera-tion of selected tissues without the need forembryonic tissue.
Demonstration of the LSCElegant experiments by Philip Fialkow andcolleagues, in which they used patterns ofinactivation in X-linked genes, had previ-ously shown that leukaemias such aschronic myelogenous leukaemia (CML)28
and AML29, together with preleukaemic diseases such as the myeloproliferative disorders30, are clonal in origin. Analyses of X-inactivation patterns in varioushaematopoietic lineages also indicated thatearly stem and progenitor cells are involvedin the development of CML and AML31.However, it was not until advances in theidentification and separation of discretetumour-cell populations, and the availabil-ity of appropriate assays (BOX 1), that theexistence of an LSC was first demonstrated.In a series of seminal experiments in 1997by investigators based at the University ofToronto — where James Till and ErnestMcCulloch had first shown the radiopro-tective effects of mouse bone marrow2 —the LSC for AML32 was first identified.
NATURE REVIEWS | CANCER VOLUME 5 | APRIL 2005 | 313
Box 1 | Functional assays for normal and malignant stem cells
For a malignant or normal cell to be considered a stem cell, it must be able to self-renew andentirely reconstitute its particular organ system over an extended period of time. The stemcell achieves this through a process of asymmetric division to generate one new stem celland one daughter cell, which undergoes differentiation. Stem cells are also capable ofsymmetrical division to form two daughter cells or two stem cells — the outcome dependson extracellular factors. To test the self-renewal potential of a cell population, it is necessaryto purify this cell population to functional homogeneity. For example, for a normalhaematopoietic stem cell, this would involve reconstitution of all hematopoietic lineages,whereas a leukaemic stem cell must accurately recapitulate the leukaemia phenotype.Although the differentiation potential of a cell can often be assayed in vitro, self-renewal canonly be measured in vivo (shown in diagram). This requires the transfer of the potentialstem-cell population to an immunologically permissive recipient, where the cells couldundergo self-renewal and differentiation. In vivo assessment of the self-renewal potential ofhuman stem cells has relied on xenotransplantation models, in which human normal ormalignant stem cells are grafted into immunocompromised mice124. Severe combinedimmunodeficient (SCID) mice, which lack both B and T cells, engraft both normalhaematopoietic stem cells (HSCs; left side of diagram), as well as leukaemia stem cells(LSCs; right side of diagram) isolated from patients with acute myelogenous leukaemia(AML) and chronic myelogenous leukaemia (CML)35,36. SCID mice can also be crossed withnon-obese diabetic (NOD) mice, which lack natural-killer cell activity and have otherimmune deficiencies, such as defects in macrophage activity and complement activation.These NOD/SCID progeny can engraft both normal and malignant human haematopoieticcell types and sustain serial transplantation125,126 — a necessary requirement for theassessment of long-term self-renewal potential. Transplantation experiments in NOD/SCIDmice have therefore become standard assays for the assessment of the self-renewal andreconstitution potential of normal and malignant HSCs.
Haematopoietic system
Purification of stem cellto functional homogeneity
In vivo transfer to an immunologically
permissive mouse(NOD/SCID mouse)
Leukaemia
Recapitulation of the organsystem/tumour in the
recipient organism
Peter Dirks andcolleagues definea cancer stem cellin tumours of thecentral nervoussystem50.
Michael Clarke and colleaguesdescribe the identification ofthe breast cancer stem cell —the first stem cell to beidentified from a solid tumour46.
John Dick and co-workers identify the firstcancer stem cell, theleukaemia stem cell, insamples from patientswith AML32.
1997 2003 2004

© 2005 Nature Publishing Group
314 | APRIL 2005 | VOLUME 5 www.nature.com/reviews/cancer
P E R S P E C T I V E S
transfer human AML to recipient mice residedexclusively within the CD34+CD38– fraction.Furthermore, these cells had the same capacityto induce all subtypes of AML, except for M3(the most differentiated subtype of AML, acutepromyelocytic leukaemia). The leukaemiasthat developed in the secondary recipientsclosely resembled the human cancer, demon-strating that LSCs have long-term self-renewalcapabilities and also determine the stage of thedifferentiation block during leukaemogenesis.
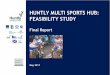
Based on these findings, the authors proposed a hierarchical organization for AML that is similar to normal haematopoiesis(FIG. 1). In this model, the LSC (or SL-IC, asthe authors named it) is responsible for bothself-renewal and the production of clono-genic leukaemic progenitors that have prolif-erative capacity, but not the capacity ofself-renewal. Based on similarities in the organization of the respective systems andphenotypic similarities, they also proposedthat the HSC was the most likely target fortransformation into an LSC. Further experi-ments from the laboratories of Craig Jordanand Donna Hogge have refined theimmunophenotype of the LSC in AML to beCD34+CD38–CD90– interleukin 3 receptor(IL-3R)+CD71– human leukocyte antigen(HLA)-DR–CD117– (REFS 37–40) (TABLE 1).
However, limitations of the SCID mouseassay system did not allow confirmation ofthe SL-IC phenotype from other AML sub-types or allow the authors to test long-termself-renewal of this population. In the SCIDsystem, large cell inoculums are required toensure engraftment, and serial transplanta-tion to subsequent generations of recipientmice to test for long-term self-renewal isnot possible.
The development of the NOD/SCID-leukaemia model obviated these drawbacks,and allowed the separation of leukaemia cellsinto subpopulations that could be evaluatedfor engraftment and serial-transplantationpotential. Cells derived from seven patientsrepresenting each subtype of AML (accordingto French-American-British classification stan-dards), were separated into CD34+CD38+ andCD34+CD38– fractions. These subpopulationswere injected intravenously into sublethallyirradiated NOD/SCID mice that received regu-lar injections of human cytokines. The micewere assessed at 4–8 weeks for engraftment,based on human-specific DNA sequences.Human cells from the bone marrow of trans-plant recipients were then isolated,based on theexpression of human form of CD45 (TABLE 1),
and transplanted into secondary recipients.These experiments showed that the capacity to
John Dick and colleagues were pioneersin developing and refining the severe com-bined immunodeficient (SCID) mouse andthe non-obese diabetic (NOD)/SCID mousexenotransplantation stem-cell assay systems,which were first described by Weissman andcolleagues33 (BOX 1). Dick showed that nor-mal human stem cells, as well as unfraction-ated AML, acute lymphoblastic leukaemia(ALL) and CML cells isolated from patients,could engraft and proliferate in SCID mice,and that the progeny of these cells could be detected by flow cytometry34–36. Moreover,all mature lineages, with the exception ofT cells, were detected in mice that were recip-ients of normal stem cells, whereas leukaemiccells recapitulated human leukaemias inrecipient mice. These findings indicated thattumour cells exist that fulfilled the criteria tobe called ‘stem cells’.
These investigators named the primitivecell responsible for the induction of normalhaematopoiesis in the recipient mice the‘SCID repopulating cell’ (SRC), and the cellresponsible for induction of leukaemia inmice the ‘SCID leukaemia-initiating cell’(SL-IC)36. Furthermore, a surface pheno-type similar to the SRC–CD34+CD38–
(TABLE 1) was demonstrated for the SL-IC inone patient with the M1 subtype of AML.
Table 1 | Markers of malignant and normal haematopoietic ontogeny
Marker Normal cell expression pattern Malignant cell expression pattern Description/function
CD10 Precursor B cells; some Common ALL cells; follicular lymphoma Neutral endopeptidase;mature B-cell subsets; neutrophils; cells; Burkitt’s lymphoma cells metalloendopeptidasesome non-haematopoietic stromal cells
CD19 Precursor and mature B cells B-cell leukaemia and lymphoma cells Signal-transduction molecule that regulatesB-lymphocyte development activation and differentiation
CD20 B cells; dendritic cells B-cell lymphoma cells Regulator of cell-cycle progression
CD34 Haematopoietic stem/progenitor cells; AML and ALL cells; bulk and leukaemia Sialomucin-like adhesion molecule;endothelial cells stem cells involved in cell adhesion
CD38 Myeloid, B- and T-cell progenitors; Non-clonogenic AML cells; ADP-ribosyl cyclase; regulator of cell monocytes; activated B and T cells; multiple myeloma cells activation and proliferationplasma cells
CD45RA B cells; monocytes; macrophages; B-cell lymphoma cells Restricted leukocyte common antigen;activated T cells regulator of leukocyte activation
CD71 All proliferating cells — particularly All proliferating cells Transferrin receptor — mediates iron erythroid progenitors entry into the cell
CD90 Haematopoietic stem cells; T cells; Some AML cells and occasional cells from Potentially contributes to haematopoietic(THY1) fibroblasts; stromal cells patients with ALL; fibroblast tumours and neural stem-cell differentiation
CD123 Myeloid progenitors AML cells, both bulk and leukaemia stem cells IL-3Rα — the low affinity binding (IL-3Rα) subunit of the IL-3 receptor, which binds to
IL-3 in association with α-subunit
CD138 B cells; plasma cells Multiple myeloma cells Syndecan-1 — an extracellular matrix receptor
HLA-DR B cells; antigen-presenting cells; Expressed on most cells from Human leukocyte antigen class II genemyeloid progenitor cells patients with AML (except patients with acute cluster — processes and presents antigen,
promyelocytic leukaemia); most B-cell and also interacts with CD4+ T cellsneoplasms; occasionally by T-ALL cellsand melanoma cells
ALL, acute lymphoblastic leukaemia; AML, acute myelogenous leukaemia.

© 2005 Nature Publishing Group
P E R S P E C T I V E S
tumours could be serially transplanted50. It islikely that, as suitable markers and assay sys-tems become available, more solid-tumourcancer stem cells will be described.
Characterization of the LSCAlthough the existence of a malignant stem-cell population has been demonstrated for anumber of cancer types, the nature and originsof this cell remain to be fully elucidated. It hasbeen proposed that the target cells for malig-nant transformation are adult somatic stemcells24, and that oncogenic mutations appropri-ate the capacity for self-renewal inherent inthese cells. Stem cells persist throughout adultlife and undergo an increased number of celldivisions, and therefore have a greater oppor-tunity than short-lived cells to acquire the min-imum number of mutations required formalignant transformation51–53.
Phenotypic evidence indicates thatsomatic stem cells are target cells for malig-nant transformation. Stem cells and tumourcells express similar levels of telomerase54,which is required to maintain telomere lengthand prevent replicative senescence. Thehuman LSC population that generates AML
Similar functional studies have been per-formed using primary ALL cells. In ALL cellsthat carry the BCR–ABL fusion gene, the SL-IC is also defined by the CD34+CD38–
immunophenotype41. In B-cell precursorALL, the SL-IC is CD34+ but lacks expressionof the more mature B-lymphoid markersCD10 and CD19 (REF. 42).
Another cancer type that is associated withthe BCR–ABL fusion is CML, which is alsoconsidered to be a stem-cell disorder.Expression of the BCR–ABL fusion transcripthas been observed in many maturehaematopoietic lineages as well as the CD34+
stem-cell compartment43,44. In addition, theobservation that CML cells have the potentialto generate acute leukaemias of various lin-eages during disease progression to blast crisis(the last of the three phases of CML)43 alsoindicates the transformation of a pluripotentcell, that is, an HSC. However, recent evidencefrom Irving Weissman’s laboratory indicatesthat the CML stem-cell compartment mightbe dynamic when it progresses to blast crisis45.In patients with myeloid CML blast crisis, self-renewal properties were observed in vitrowithin the granulocyte monocyte progenitor(GMP) population, a compartment that nor-mally lacks the potential for self-renewal, indi-cating that this progenitor compartmentmight contain the stem cells responsible forthe expansion of acute leukaemic blasts ontransformation. These data demonstrate thatthe LSC hierarchy might change or operate ondifferent levels during the progression ofleukaemia, with the accompanying acquisitionof further mutations.
Application of the principles of stem-cellbiology by John Dick and others recently ledinvestigators such as Michael Clarke and PeterDirks to propose a similar paradigm for solid-tumour development. However, stem cellshave been much more difficult to identify innon-haematopoietic cancers, because fewerwell-developed phenotypic markers anddefinitive assay systems are available.Nonetheless, significant progress has beenmade in the identification of cancer stem cellsin both breast and CNS tumours46–50. Breastcancer stem cells were first identified by Clarkeand colleagues in 2003, based on the expres-sion of surface markers and their potential toform tumours after injection into the mam-mary fat pad of NOD/SCID mice. Cells withthe phenotype of epithelial-specific antigen(ESA)+ Lineage marker (Lin)–CD24–/lowCD44+
(TABLE 1) were found to generate tumours thatwere histologically similar to those of primarybreast tumours in mice when as few as 100cells were transplanted46. Cells from theseNOD/SCID recipients were re-purified, and
cells with the same phenotype were found toreform tumours when transplanted into secondary and tertiary recipients. Theseexperiments demonstrated the long-term self-renewal capacity of these cells, therebyfulfilling the definition of a cancer stem cellfrom breast tumours.
In 2003, there were three separate reportsof the characterization of CNS tumour stemcells, from the laboratories of Peter Dirks,Harley Kornblum and Dennis Steindler.Previous studies had shown that neural stemcells (NSCs) form neurospheres in culture4,and that this function makes it possible toisolate these cell populations from braintumours for further analysis. The tumourNSCs can differentiate into cells that havecharacteristics of both neurons and glial cells,self-renew in vitro at higher levels than nor-mal NSCs, and grow and differentiate inneonatal rat brains47–49. Cells with these prop-erties all express CD133+ (REF. 47), a marker ofNSCs, and a recent report from Peter Dirks’laboratory in Toronto demonstrated thatonly this CD133+ subpopulation has the abil-ity to regenerate identical brain tumours inNOD/SCID mice. Furthermore, these
NATURE REVIEWS | CANCER VOLUME 5 | APRIL 2005 | 315
Self-renewal
Leukaemic Normal
SL-IC SRCHSCCD34+, CD38–
Leukaemogenic event
Leukaemia Lymphocytes Granulocytes Red blood cells
Platelets
Multipotentialprogenitors
Committed progenitors
Clonogenic leukaemicprogenitors
Figure 1 | Acute myelogenous leukaemia forms a stem-cell hierarchy. There are functional andphenotypic similarities between the normal haematopoietic stem cell (HSC) and the leukaemia stem cell(LSC) that initiates AML. Like the normal haematopoietic system, leukaemia cells are believed to be derivedfrom HSCs, which are CD34+CD38–. During normal cell haematopoiesis (right), the HSC gives rise to thesevere combined immunodeficiency (SCID) repopulating cell (SRC), which is capable of self-renewal andproduction of all mature lineages through a succession of multipotent and committed progenitors. Duringleukaemogenesis (left), the LSC (or SCID leukaemia-initiating cell, SL-IC) expresses some shared surfacephenotypic markers with the HSC. It also has the capacity for producing both the clonogenic leukaemicprogenitors and the non-clonogenic blast cells, which make up the bulk of the leukaemia. Figure adaptedfrom REF. 32 © (1997) Macmillan Magazines Ltd.

© 2005 Nature Publishing Group
316 | APRIL 2005 | VOLUME 5 www.nature.com/reviews/cancer
P E R S P E C T I V E S
However, committed progenitor cells thatdo not have the capacity to self-renew mightalso be transformed through the activationof oncogenic pathways that re-establishproperties of self-renewal (FIG. 2). Proof ofprinciple for this concept has recently been established in mouse models ofleukaemia61,62. In these experiments, popula-tions of progenitor cells that lack self-renewal properties were purified by flowcytometry and transduced with either theMLL–ENL or MOZ–TIF2 oncogenes, both ofwhich were originally cloned from humanleukaemias and generate leukaemia on retro-viral expression in mouse models. Both ofthese fusion genes also involve transcrip-tional regulators — MLL is a histonemethyltransferase involved in chromatinremodelling63, and both MOZ and TIF2 aretranscriptional co-activators64. Transductionwith either oncogene leads to the restorationof self-renewal properties in these progeni-tors in in vitro assays — such as the ability toform colonies in serial methylcellulose platesin the absence of stromal support, and togrow in liquid culture — properties that arenot even demonstrated by normal HSCs.These transduced progenitors were also ableto generate AML when transplanted intomice, and the resulting leukaemias could betransplanted to secondary recipients. Theseproperties could not be attributed solely toinsertional mutagenesis by the retroviralvector, because transduction with transfor-mation-defective mutants of MOZ–TIF2and MLL–ENL did not confer this pheno-type61,62. Furthermore, self-renewal is notconferred by all leukaemia-associated onco-genes — transduction with BCR–ABL doesnot change the self-renewal properties ofcommitted progenitor populations62.
Corroborating evidence for progenitorcells as targets for transformation has alsobeen observed in human leukaemia cells. Arecent report of the organization of the LSCcompartment following the progression ofCML to its acute, blast-crisis phase indicatesthat a committed progenitor populationmight be the target for further oncogenicmutations that re-confer properties of self-renewal. For example, GMPs purified frompatients with blast crisis CML have self-renewal properties in vitro45. These data alsoraise the possibility that ongoing acquisitionof second mutations that confer properties ofself-renewal to progenitor cells could alsocontribute to a hierarchy of LSCs that havedifferent long-term self-renewal properties65.This has been shown for AML cells60.Although in vivo confirmation of self-renewalin the GMP population of patients in the
multi-lineage differentiation potential, suchas an HSC43,44. Moreover, a recent mousemodel has shown that genetic inactivationof the AP-1 transcription factor JUNB cancause a myeloproliferative, CML-like diseasein mice only when JUNB is inactivated inthe HSC compartment59. Another recentstudy demonstrated that LSCs that have dif-ferent capacities for long-term self-renewal60
could be identified following serial trans-plantation of lentivirally labelled humanAML cells into NOD/SCID mice. These dataare consistent with the maintenance ofa normal HSC hierarchy in the LSC com-partment, and further implicate the HSC as a candidate cell for transformation byleukaemia-inducing oncogenes.
in the NOD/SCID mouse model has a similarphenotype (CD34+CD38–) to that of normalhuman HSCs, which induce multilineagehuman haematopoiesis when engrafted intoNOD/SCID mice36, and also to the cell com-partment that is enriched for human HSC55.Furthermore, cytogenetic abnormalities thatare consistently associated with certainleukaemias have been detected in this cell compartment in patients with AML, CML and ALL43,56–58. In addition, the t(9;22)(Philadelphia chromosome), which resultsin the BCR–ABL gene rearrangement asso-ciated with CML, can be detected in cells ofthe myeloid, erythroid, megakaryocytic andB-lymphoid lineages. This indicates that theinitial transformation occurred in a cell with
HSC
CLP CMP
Peripheral blood
Bone marrow
GMPPro-B cell Pro-T cell MEP
Lymphoid organs
Stimulated B cell Stimulated T cell
Naive B lymphocyte Naive T lymphocyte Erythrocyte Platelet Monocyte Granulocyte
Figure 2 | Ontogeny of haematopoietic cells and candidate leukaemia stem cells. Within thehaematopoietic system, the haematopoietic stem cell (HSC) has self-renewal potential and multipotentdifferentiation potential. Its progeny include multipotent common lymphoid progenitors (CLPs) and commonmyeloid progenitors (CMPs). In turn, these progenitors give rise to progenitors that have more limiteddifferentiation potential, Pro-B and Pro-T cells, megakaryocyte erythroid progenitors (MEPs) and granulocytemonocyte progenitors (GMPs). In the myeloid lineage, MEPs give rise to mature erythrocytes and platelets inthe peripheral blood. GMPs give rise to monocytes and the various granulocyte lineages. In the lymphoidlineages Pro-B and Pro-T cells give rise to mature (naive) B and T lymphocytes and then stimulated B and Tcells, respectively, following exposure to antigen. Cellular compartments that are known to be, or might be,potential targets for the generation of leukaemia stem cells (LSCs) are indicated by solid or dashed boxes,respectively. Not all of these cell types have self-renewal properties (which is indicated with a curved arrow).Mutations are therefore required to confer properties of self-renewal to these cell types, and to lead to LSCformation and leukaemogenesis.

© 2005 Nature Publishing Group
P E R S P E C T I V E S
resulting in T-ALL. A similar heterodimeriza-tion mutation in the Caenorhabditis elegansNotch homologue glp-1 has been describedand leads to a massive proliferation of germcells92. Interestingly, inhibitors of the prote-olytic enzyme γ-secretase have already beendeveloped, because of the involvement ofthis enzyme in the production of amyloido-genic peptides in patients with Alzheimer’sdisease. These γ-secretase inhibitors mighttherefore be of therapeutic value in patientsthat have T-ALL associated with NOTCH1-activating mutations, and also as probes for self-renewal potential conferred byNOTCH1. Therapeutic trials of γ-secretaseinhibitors in patients with T-ALL are nowunder development, and represent an initialstep in molecularly targeting the self-renewalpotential of leukaemia stem cells.
HOX family. The homeodomain-containingtranscription factors of the HOX family have also been found to be important inhaematopoietic development, leukaemogen-esis and self-renewal. They were initiallywidely studied as regulators of pattern for-mation and tissue identity during embryo-genesis in both Drosophila melanogaster andmammalian systems by investigators such asRobert Krumlauf 93. In 2002, HOX geneswere shown to be expressed in haematopoi-etic precursors, with preferential expressionin self-renewing HSCs, and are downregu-lated following differentiation94. Theirimportance in normal blood formation andmaintenance has been demonstrated ingene-targeting studies — abnormalities inmultiple haematopoietic lineages wereobserved in mice with disruptions in indi-vidual HOX genes95,96. Moreover, the overex-pression of specific HOX genes, such asHOXB4, is associated with the expansion ofthe HSC compartment ex vivo78 and with anincrease in competitive self-renewal follow-ing transplantation experiments in mice.Similar findings were reported for bothHOXB4 and HOXA9 (REFS 77, 97, 98).
The relationship between only certainHOX genes and leukaemogenesis is also amystery — transplantation of mice withbone marrow that overexpresses Hoxa9 willeventually lead to leukaemia, whereas recipi-ents of bone-marrow cells that overexpressHoxb4 do not develop leukaemia. However,in the 1990s, many HOX genes were directlylinked to the pathogenesis of acuteleukaemia99. Chromosome translocationsthat fuse HOXA9 or HOXD13 to NUP98,which encodes a component of the nuclearpore, were observed in AML cells100,101.HOX11 overexpression, resulting from its
blast-crisis stage of CML is required, thisreport further implicates transcriptional targets of β-catenin as the mediators of self-renewal in this system. Transduction of nor-mal GMPs with β-catenin restores in vitroself-renewal to this population, and the inhi-bition of nuclear β-catenin localization inblast-crisis GMPs, through lentiviral expres-sion of the specific inhibitor axin, inhibitsself-renewal.
Therefore, considerable evidence existsthat committed progenitors might be trans-formed to generate LSCs. Although the HSCis an attractive candidate for the cell of originof the LSC, it is also the most dangerous celltype for transformation. In metazoan biol-ogy, stem cells are the sole guardians of self-renewal in adult tissues, and would thereforebe expected to have evolved sophisticatedinhibitory machinery to prevent uncon-trolled self-renewal. However, these mecha-nisms would not be expected to function indaughter cells, which lack self-renewal prop-erties. It seems that there are oncogenicmutations that are tolerated by the HSC,such as BCR–ABL, and that are passed on tothe progeny of the mutated stem cell. Thesemutations might be tolerated because theyhave little or no effect on the stem cell itself,and confer their main biological impact ondownstream progeny. However, mutationsthat increase self-renewal and or impair dif-ferentiation (alone or in cooperation withother mutations) might be toxic or not toler-ated by the HSC. Alternatively these muta-tions could simply be constrained, such thatthe aberrant self-renewal that they confer canonly alter the capabilities of downstreamprogeny. Mutations that affect self-renewaland proliferation appear to be associated pri-marily with acute haematological malignan-cies. So, it might be (for the above reasons)that the stem cell is actually less likely toacquire these mutations, or to manifest bio-logical alterations that are secondary to thesemutations. In either situation, the net resultwill be the same, in that the LSC in acute dis-orders frequently lies downstream of thestem-cell compartment.
Regulating stem-cell self-renewalRelatively little is known about the molecularmechanisms of self-renewal in normal ormalignant stem-cell populations24. However, itseems likely that there will be at least somedegree of overlap in the regulation of self-renewal in normal and malignant stem cells.Genes and pathways implicated in the molec-ular control of self-renewal include productsof the Bmi1 (also known as PCGF4) and otherpolycomb genes66–68, the WNT–β-catenin
pathway45,69–71, the Notch72,73 and SHH74,75 sig-nalling pathways, as well as the HOX family oftranscription factors76–78. The WNT–β-catenin,BMI1/polycomb and SHH signalling pathwayshave been expertly reviewed elsewhere79–81.
Notch family. Notch family members aredevelopmental morphogens82. In the year2000, the Notch family members were shownto be expressed in self-renewing tissue, andactivation of Notch signalling was subse-quently shown to potentiate self-renewal ofboth HSCs72,73 and NSCs83,84. Notch signallingis also required for T-cell commitment85.There are four mammalian Notch genes, eachof which encodes a single-pass transmem-brane receptor. Notch signalling is initiated bythe binding of the cognate Jagged or Delta-like ligands, resulting in metalloproteinase (γ-secretase) cleavage in the extracellular portionof the receptor with release of intracellularNotch (for an extensive review of Notch func-tion see REF. 86) (FIG. 3). Intracellular Notchtranslocates to the nucleus, forms a multi-meric transcriptional complex with the tran-scription factor CSL and co-activators of themastermind-like (MAML) family, and acti-vates the transcription of Notch target genesinvolved in context-dependent processes suchas T-cell differentiation and self-renewal.
Notch family members were then shownto have activity as oncogenes or tumour suppressors, depending on the cellular con-text86,87. The role of Notch as an oncogene wasbest characterized in T-cell ALL (T-ALL). In1991, a small fraction of patients with T-ALLwere found to express a constitutively acti-vated form of NOTCH1, as a consequence ofchromosomal translocation involving the T-cell receptor β-subunit88. Subsequent stud-ies showed that NOTCH1 signalling causedT-ALL in mouse models89,90.
A recent study from the laboratories of JonAster and Tom Look reported that more than50% of patients with T-ALL carried somaticactivating point mutations of NOTCH1 (REF. 91). These mutations affected either theheterodimerization domain, leading to cleav-age and liberation of intracellular NOTCH1(ICN), or resulted in loss of function of thePEST domain, which targets ICN for degra-dation by the proteasome (FIG. 3). Both muta-tions, which often occurred on the sameallele, independently led to the increased acti-vation of the Notch-signalling pathway, sup-porting a cooperative effect between themutations in NOTCH1 activation.
The increase in Notch-pathway signallingactivity appears to both induce T-cell differ-entiation and increase self-renewal propertiesin primitive haematopoietic progenitors,
NATURE REVIEWS | CANCER VOLUME 5 | APRIL 2005 | 317

© 2005 Nature Publishing Group
318 | APRIL 2005 | VOLUME 5 www.nature.com/reviews/cancer
P E R S P E C T I V E S
Taken together, these reports indicate thatthe self-renewal properties that are requiredfor leukaemia induction and maintenanceare restored (or augmented) by transcrip-tional programmes induced by certain onco-genes. However, as leukaemogenesis is amultistep process 117, the transcriptome ofleukaemia stem cells will demonstratechanges that reflect a number of oncogenicmutations. In future experiments, mousemodels may simplify matters and revealmany of the changes that result from theoverexpression of a single oncogene in ahomogeneous cellular context, and mightprovide a powerful prospective platform toelucidate the transcriptional programmesinvolved in self-renewal. Candidate self-renewal genes could be identified throughmicroarray analysis, and could be validatedusing functional assays of mouse and humanLSCs and HSCs. Comparisons of LSC andHSC gene-expression patterns might iden-tify similarities and differences in molecularself-renewal mechanisms used by normaland malignant stem cells. It is also likely thatthe WNT, polycomb, HOX, SHH and Notchpathways form important hubs in the net-work of self-renewal transcriptional pro-grammes. Further study of the downstreamtargets of these self-renewal pathways, and ofany potential interactions between thesepathways80 might be used to identify crucialeffectors of self-renewal.
The identification of additional genesthat regulate self-renewal might also providerational targets for therapeutic intervention— particularly if their requirement is morecritical for self-renewal in LSCs than HSCs.Understanding the pathogenic mechanismsof leukaemia stem cells might also provideinsight into the reasons that chemothera-peutic regimens can markedly reducetumour burden, but result in relapse at alater stage. It is likely that chemotherapeu-tics only target the bulk, non-clonogenictumour cells and spare the leukaemia stemcells, allowing for recrudescence of tumourfollowing cessation of therapy79. Becauseunlimited self-renewal is an absolute prereq-uisite for tumour growth118, inhibition ofthis property should have a marked effecton cancer progression and recurrence fol-lowing, or in conjunction with, standardtherapies. This would be a paradigm shift inthe treatment of leukaemia, away from tar-geting the blast cells and towards the target-ing of the LSC. This approach couldincrease the incidence of remission anddecrease the incidence of relapse. A chal-lenge to this approach is to find a way tospecifically target cancer-cell self-renewal
HOXA9 overexpression is now the singlemost highly correlated factor with poor prog-nosis in patients with AML104. Several othermembers of the HOX gene family, such asHoxb3 (REF. 105), Hoxb8 (REF. 106) and Hoxa10(REF. 107), have also been associated withleukaemogenesis in mouse models. Thesefindings indicate a role for HOX genes inleukaemia induction, and their role in HSCself-renewal indicate that they might alsomediate LSC self-renewal.
The central role of HOX deregulation inleukaemia is further emphasized by the roleof upstream regulators such as MLL and theCDX proteins in leukaemia. Targeted-dis-ruption experiments have demonstrated thatthe Mll gene in mice is required for themaintenance of HOX gene-expression pat-terns during development108. Rearrangementof MLL with more than 40 partner genes hasbeen reported in acute leukaemia (reviewedin REFS 109,110) and transformation by MLLfusion proteins is thought to be mediated bytheir altered transcriptional properties63,with dysregulation of HOX gene expressionas a crucial event111. Another recentlydescribed gene family, CDX, also regulatesexpression of HOX genes112. The CDX genesare mammalian homologues of theDrosophila melanogaster caudal gene, amaster regulator of embryonic body seg-mentation113. CDX genes are also impli-cated in human leukaemogenesis, with thedescription of a t(12;13) in human AML114.This chromosomal rearrangement juxta-poses the TEL and CDX2 loci and isthought to result in the overexpression ofCDX2 from the TEL locus, and expressionof CDX2 induces leukaemia in murineretroviral transduction models115.
Future directionsDecades of research into the pathways thatcontrol cellular self-renewal indicate alter-ations in gene transcription as a common endpoint. However, the specific transcriptionalprogrammes that are activated by these path-ways are not well understood. The leukaemia-associated fusion genes MOZ–TIF2 andMLL–ENL confer properties of self-renewalto committed myeloid progenitors61,62. Theyare able to transform cells by altering theirtranscriptional programme64,116; and presum-ably restore self-renewal properties to progen-itor cells through similar mechanisms.Moreover, the restoration of in vitro self-renewal properties in GMPs isolated frompatients with blast-crisis CML appears to beassociated with increased transcriptionalactivity of β-catenin45, albeit with unknowngene targets.
translocation to promoter regions of the T-cell receptor locus, was also described in T-ALL cells102. Moreover, HOX11 andHOX11L2 were found to be frequentlyupregulated in T-ALL cells and to conferfavourable or poor prognosis, respectively103.
γ-Secretase
Inhibitors
Jagged/Delta ligand
Ubiquitylation
ECN
ICN
CSL
CoA
MAML
HESPre-TCDKN1A
Mutations in T-ALL
PEST domain
HD
α
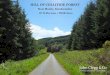
Figure 3 | The Notch signalling pathway.Notch family members are transmembranereceptors and developmental morphogens. Inadult tissue, activation of the NOTCH1 pathwaymediates context-specific functions, such as self-renewal and T-cell differentiation. NOTCH1signalling is initiated by the engagement ofextracellular portions (ECN) of NOTCH1 with itsligands, which are members of the Jagged/Deltafamily. This binding induces metalloprotease-dependent cleavage of the NOTCH1heterodimerization domain (HD) with terminalcleavage that is dependent on γ-secretaseactivity. This process releases intracellularNOTCH1 (ICN), which translocates to the nucleusto form a multimeric transcriptional factorcomplex with the transcription factor CSL andco-activators of the mastermind-like (MAML)family. These recruit additional co-activators,such as p300 and PCAF (CoA), to activate thetranscription of target genes such as HES, pre-Tαand CDKN1A. The transcriptional programmesthat are initiated are thought to mediate T-celldifferentiation and increase the self-renewal that isassociated with NOTCH1 signalling activity. ICN istargeted for degradation by the polyubiquitylationof sequences in its PEST domain. Mutations (redarrows) in the HD and PEST domain of NOTCH1have recently been associated with T-cell acutelymphoblastic leukaemia (T-ALL). Thesemutations are believed to activate NOTCH1signalling by increasing NOTCH1 cleavage andliberation of ICN, as well as by increasingNOTCH1 protein stability by decreasingproteosomal degradation.

© 2005 Nature Publishing Group
P E R S P E C T I V E S
11. Griffin, J. & Lowenberg, B. Clonogenic cells in acutemyeloblastic leukemia. Blood 68, 1185–1195 (1986).
12. Hamburger, A. W. & Salmon, S. E. Primary bioassay ofhuman tumor stem cells. Science 197, 461–463(1977).
13. Southam, C. & Brunschwig, A. Quantitative studies ofautotransplantation of human cancer. Cancer 14,461–463 (1961).
14. Virchow, R. Editorial. Virchows Arch. Pathol. Anat.Physiol. Klin. Med. 3, 23 (1855).
15. Cohnheim, J. Ueber entzundung und eiterung. Path.Anat. Physiol. Klin. Med. 40, 1–79 (1867).
16. Beckwith, J. B., Kiviat, N. B. & Bonadio, J. F.Nephrogenic rests, nephroblastomatosis, and thepathogenesis of Wilms’ tumor. Pediatr. Pathol. 10, 1–36(1990).
17. Wiemels, J. L. et al. Prenatal origin of acute lymphoblasticleukaemia in children. Lancet 354, 1499–1503 (1999).
18. Gale, K. B. et al. Backtracking leukemia to birth:identification of clonotypic gene fusion sequences inneonatal blood spots. Proc. Natl Acad. Sci. USA 94,13950–13954 (1997).
19. Wiemels, J. L. et al. In utero origin of t(8;21) AML1–ETOtranslocations in childhood acute myeloid leukemia.Blood 99, 3801–3805 (2002).
20. Greaves, M. F. & Wiemels, J. Origins of chromosometranslocations in childhood leukaemia. Nature Rev.Cancer 3, 639–649 (2003).
21. Pierce, G. B. & Johnson, L. D. Differentiation and cancer.In Vitro 7, 140–145 (1971).
22. Potter, V. R. Phenotypic diversity in experimentalhepatomas: the concept of partially blocked ontogeny.The 10th Walter Hubert Lecture. Br. J. Cancer 38, 1–23(1978).
23. Sell, S. & Pierce, G. B. Maturation arrest of stem celldifferentiation is a common pathway for the cellular originof teratocarcinomas and epithelial cancers. Lab. Invest.70, 6–22 (1994).
24. Reya, T., Morrison, S., Clarke, M. & Weissman, I. Stemcells, cancer, and cancer stem cells. Nature 414,105–111 (2001).
25. Kondo, M. et al. Biology of hematopoietic stem cells andprogenitors: implications for clinical application. Annu.Rev. Immunol. 21, 759–806 (2003).
26. Ibrahim, S. F. & van den Engh, G. High-speed cell sorting:fundamentals and recent advances. Curr. Opin.Biotechnol. 14, 5–12 (2003).
27. Herzenberg, L. A., Parks, D., Sahaf, B., Perez, O. &Roederer, M. The history and future of the fluorescenceactivated cell sorter and flow cytometry: a view fromStanford. Clin. Chem. 48, 1819–1827 (2002).
28. Fialkow, P., Gartler, S. M. & Yoshida, A. Clonal origin ofchronic myelocytic leukemia in man. Proc. Natl Acad. Sci.USA 58, 1468–1471 (1967).
29. Fialkow, P. et al. Acute nonlymphocytic leukemia:heterogeneity of stem cell origin. Blood 57, 1068–1073(1981).
30. Fialkow, J. P., Faguet, G. B., Jacobson, R. J., Vaidya, K.& Murphy, S. Evidence that essential thrombocythemia isa clonal disorder with origin in a multipotent stem cell.Blood 58, 916–919 (1981).
31. Fialkow, P. J., Jacobson, R. J. & Papayannopoulou, T.Chronic myelocytic leukemia: clonal origin in a stem cellcommon to the granulocyte, erythrocyte, platelet andmonocyte/macrophage. Am. J. Med. 63, 125–130(1977).
32. Bonnet, D. & Dick, J. E. Human acute myeloid leukemiais organized as a hierarchy that originates from a primitivehematopoietic cell. Nature Med. 3, 730–737 (1997).
33. McCune, J. M. et al. The SCID-hu mouse: murine modelfor the analysis of human hematolymphoid differentiationand function. Science 241, 1632–1639 (1988).
34. Kamel-Reid, S. et al. A model of human acutelymphoblastic leukemia in immune-deficient SCID mice.Science 246, 1597–1600 (1989).
35. Sirard, C. et al. Normal and leukemic SCID-repopulatingcells (SRC) coexist in the bone marrow and peripheralblood from CML patients in chronic phase, whereasleukemic SRC are detected in blast crisis. Blood 87,1539–1548 (1996).
36. Lapidot, T. et al. A cell initiating human acute myeloidleukaemia after transplantation into SCID mice. Nature367, 645–648 (1994).
37. Jordan, C. T. et al. The interleukin-3 receptor α chain is aunique marker for human acute myelogenous leukemiastem cells. Leukemia 14, 1777–1784 (2000).
38. Blair, A., Hogge, D. E., Ailles, L. E., Lansdorp, P. M. &Sutherland, H. J. Lack of expression of Thy-1 (CD90) onacute myeloid leukemia cells with long-term proliferativeability in vitro and in vivo. Blood 89, 3104–3112 (1997).
pathways without toxicity to normalcells119,120 (FIG. 4). Trials with γ-secretaseinhibitors, which target the Notch signallingpathway in T-ALL cells, might provide someinsight into the therapeutic window in targeting self-renewal.
As there are many functional similaritiesbetween the LSC and solid tumour stemcells, it is likely that malignant stem cells willshare a number of molecular mechanisms bywhich they control fundamental cellularprocesses such as self-renewal, cell-fate deter-mination and apoptosis. The further charac-terization of the LSC will therefore provideparadigms of the biology of malignant stemcells that can be applied to solid-organtumours and might also lead to improvedtherapeutics for these malignancies.
Building on the seminal observations ofJohn Dick and others, a picture is emerging inwhich tumours have a similar hierarchicaldevelopment and architecture as the normal-tissue counterpart, including the existence ofa multipotent stem cell and an aberrant dif-ferentiation programme. Not only is this rele-vant in the haematopoietic system in which itwas first defined, but also in several solidtumours. Indeed, it is plausible that such ahierarchy is present in all tumours. Becausethere is an enticing congruence between nor-mal and malignant stem-cell function, it isprobable that if we understand one, we willhave major insights into the other.
Brian J. P. Huntly is at the Division of Hematology, Department of Medicine,
Brigham and Women’s Hospital, Boston,MA 02115, USA.
D. Gary Gilliland is at theHoward Hughes Medical Institute, Harvard
Medical School, Boston, MA 02115, USA.
e-mails: [email protected];[email protected]
doi: 10.1038/nrc1592
1. Main, J. M. & Prehn, R. T. Successful skin homograftsafter the administration of high dosage X radiation andhomologous bone marrow. J. Natl Cancer Inst. 15,1023–1029 (1955).
2. Till, J. E. & McCulloch, E. A. A direct measurement of theradiation sensitivity of normal mouse bone marrow cells.Radiat. Res. 14, 213–222 (1961).
3. Pappenheim, A. Prinzipen der neuren morphologischenhaematozytologie nach zytogenetischer grundlage. FoliaHaematol. 21, 91–101 (1917).
4. Reynolds, B. A. & Weiss, S. Generation of neurons andastrocytes from isolated cells of the adult mammaliancentral nervous system. Science 255, 1707–1710(1992).
5. Blanpain, C., Lowry, W. E., Geoghegan, A., Polak, L. &Fuchs, E. Self-renewal, multipotency, and the existenceof two cell populations within an epithelial stem cell niche.Cell 118, 635–648 (2004).
6. Smith, G. H. & Medina, D. A morphologically distinctcandidate for an epithelial stem cell in mousemammary gland. J. Cell Sci. 90 (Part 1), 173–183(1988).
7. Kordon, E. C. & Smith, G. H. An entire functionalmammary gland may comprise the progeny from a singlecell. Development 125, 1921–1930 (1998).
8. Park, C. H., Bergsagel, D. E. & McCulloch, E. A. Mousemyeloma tumor stem cells: a primary cell culture assay. J. Natl Cancer Inst. 46, 411–422 (1971).
9. Bruce, W. R. & Van Der Gaag, H. A quantitative assay forthe number of murine lymphoma cells capable ofproliferation in vivo. Nature 199, 79–80 (1963).
10. Sabbath, K. D., Ball, E. D., Larcom, P., Davis, R. B. &Griffin, J. D. Heterogeneity of clonogenic cells in acutemyeloblastic leukemia. J. Clin. Invest. 75, 746–753(1985).
NATURE REVIEWS | CANCER VOLUME 5 | APRIL 2005 | 319
Recurrence of disease
Conventional
chemotherapy
Tumour involution
Disease remission
a
b Targeted LSC therapy alone
Targeted LSC plusconventional therapy
Tumour debulking
Figure 4 | Targeting leukaemia stem cells. a | At present, treatment for leukaemia useschemotherapeutic agents that target all leukaemia cells (grey), based on properties such as their increasedproliferation and entry into the cell cycle. However, it is likely that this approach spares the population ofleukaemia stem cell (LSCs; green), which are responsible for the continued growth and propagation of thetumour. In many instances, this leads to recurrence of the disease. b | A greater understanding of LSCbiology will allow us to design therapeutic agents that specifically target the LSC populations. Suchtherapies used alone, or in combination with conventional chemotherapteutic agents that reduce tumourburden, should lead to tumour involution or disease remission, respectively. Both of these approachescould improve both initial response rates and overall survival, through a decrease in the relapse of disease.

© 2005 Nature Publishing Group
320 | APRIL 2005 | VOLUME 5 www.nature.com/reviews/cancer
P E R S P E C T I V E S
94. Pineault, N., Helgason, C. D., Lawrence, H. J. &Humphries, R. K. Differential expression of Hox, Meis1,and Pbx1 genes in primitive cells throughout murinehematopoietic ontogeny. Exp. Hematol. 30, 49–57(2002).
95. Lawrence, H. J. et al. Mice bearing a targeted interruptionof the homeobox gene HOXA9 have defects in myeloid,erythroid, and lymphoid hematopoiesis. Blood 89,1922–1930 (1997).
96. Kappen, C. Disruption of the homeobox gene Hoxb-6in mice results in increased numbers of earlyerythrocyte progenitors. Am. J. Hematol. 65, 111–118(2000).
97. Thorsteinsdottir, U. et al. Overexpression of the myeloidleukemia-associated Hoxa9 gene in bone marrow cellsinduces stem cell expansion. Blood 99, 121–129(2002).
98. Krosl, J., Beslu, N., Mayotte, N., Humphries, R. K. &Sauvageau, G. The competitive nature of HOXB4-transduced HSC is limited by PBX1: the generation ofultra-competitive stem cells retaining full differentiationpotential. Immunity 18, 561–571 (2003).
99. Look, A. Oncogenic transcription factors in the humanacute leukaemias. Science 278, 1059–1064 (1997).
100. Borrow, J. et al. The t(7;11)(p15;p15) translocation inacute myeloid leukaemia fuses the genes for nucleoporinNUP98 and class I homeoprotein HOXA9. Nature Genet.12, 159–167 (1996).
101. Raza-Egilmez, S. Z. et al. NUP98–HOXD13 gene fusionin therapy-related acute myelogenous leukemia. CancerRes. 58, 4269–4273 (1998).
102. Hatano, M., Roberts, C. W., Minden, M., Christ, W. M. &Korsmeyer, S. J. Deregulation of a homeobox gene,HOX11, by the t(10;14) in T cell leukemia. Science 253,79–82 (1991).
103. Ferrando, A. A. et al. Gene expression signatures definenovel oncogenic pathways in T cell acute lymphoblasticleukemia. Cancer Cell 1, 75–87 (2002).
104. Golub, T. R. et al. Molecular classification of cancer: classdiscovery and class prediction by gene expressionmonitoring. Science 286, 531–537 (1999).
105. Sauvageau, G. et al. Overexpression of HOXB3 inhematopoietic cells causes defective lymphoid developmentand progressive myeloproliferation. Immunity 6, 13–22(1997).
106. Perkins, A., Kongsuwan, K., Visvader, J., Adams, J. M. &Cory, S. Homeobox gene expression plus autocrinegrowth factor production elicits myeloid leukemia. Proc.Natl Acad. Sci. USA 87, 8398–8402 (1990).
107. Thorsteinsdottir, U. et al. Overexpression of HOXA10 inmurine hematopoietic cells perturbs both myeloid andlymphoid differentiation and leads to acute myeloidleukemia. Mol. Cell. Biol. 17, 495–505 (1997).
108. Yu, B. D., Hess, J. L., Horning, S. E., Brown, G. A. &Korsmeyer, S. J. Altered Hox expression and segmentalidentity in Mll-mutant mice. Nature 378, 505–508(1995).
109. Ayton, P. M. & Cleary, M. L. Molecular mechanisms ofleukemogenesis mediated by MLL fusion proteins.Oncogene 20, 5695–5707 (2001).
110. Daser, A. & Rabbitts, T. H. Extending the repertoire of themixed-lineage leukemia gene MLL in leukemogenesis.Genes Dev. 18, 965–74 (2004).
111. Armstrong, S. A., Golub, T. R. & Korsmeyer, S. J. MLL-rearranged leukemias: insights from gene expressionprofiling. Semin. Hematol. 40, 268–273 (2003).
112. Davidson, A. J. et al. cdx4 mutants fail to specify bloodprogenitors and can be rescued by multiple hox genes.Nature 425, 300–306 (2003).
113. Mlodzik, M. & Gehring, W. J. Expression of the caudalgene in the germ line of Drosophila: formation of an RNAand protein gradient during early embryogenesis. Cell 48,465–478 (1987).
114. Chase, A. et al. Fusion of ETV6 to the caudal-related homeobox gene CDX2 in acute myeloidleukemia with the t(12;13)(p13;q12). Blood 93,1025–1031 (1999).
115. Rawat, V. P. et al. Ectopic expression of the homeoboxgene Cdx2 is the transforming event in a mouse model oft(12;13)(p13;q12) acute myeloid leukemia. Proc. NatlAcad. Sci. USA 101, 817–822 (2004).
116. Ayton, P. & Cleary, M. Molecular mechanisms ofleukemogenesis mediated by MLL fusion proteins.Oncogene 20, 5695–5707 (2001).
117. Kelly, L. & Gilliland, D. Genetics of myeloid leukemias.Annu. Rev. Genomics Hum. Genet. 3, 179–198 (2002).
118. Hanahan, D. & Weinberg, R. The hallmarks of cancer. Cell100, 57–70 (2000).
119. Guzman, M. L. et al. Preferential induction of apoptosisfor primary human leukemic stem cells. Proc. Natl Acad.Sci. USA 99, 16220–16225 (2002).
65. Huntly, B. J. & Gilliland, D. G. Blasts from the past: newlessons in stem cell biology from chronic myelogenousleukemia. Cancer Cell 6, 199–201 (2004).
66. Park, I. K. et al. Bmi-1 is required for maintenance of adultself-renewing haematopoietic stem cells. Nature 423,302–305 (2003).
67. Lessard, J. & Sauvageau, G. Bmi-1 determines theproliferative capacity of normal and leukaemic stem cells.Nature 423, 255–260 (2003).
68. Ohta, H. et al. Polycomb group gene rae28 is required forsustaining activity of hematopoietic stem cells. J. Exp.Med. 195, 759–770 (2002).
69. Reya, T. et al. A role for Wnt signalling in self-renewal ofhaematopoietic stem cells. Nature 423, 409–414 (2003).
70. Muller-Tidow, C. et al. Translocation products in acutemyeloid leukemia activate the Wnt signalling pathway inhematopoietic cells. Mol. Cell Biol. 24, 2890–2903 (2004).
71. Zheng, X. et al. γ-catenin contributes to leukemogenesisinduced by AML-associated translocation products byincreasing the self-renewal of very primitive progenitorcells. Blood 103, 3535–3543 (2004).
72. Varnum-Finney, B. et al. Pluripotent, cytokine-dependent,hematopoietic stem cells are immortalized by constitutiveNotch1 signaling. Nature Med 6, 1278–1281 (2000).
73. Karanu, F. N. et al. The notch ligand jagged-1 representsa novel growth factor of human hematopoietic stem cells.J. Exp. Med. 192, 1365–1372 (2000).
74. Zhang, Y. & Kalderon, D. Hedgehog acts as a somaticstem cell factor in the Drosophila ovary. Nature 410,599–604 (2001).
75. Wechsler-Reya, R. J. & Scott, M. P. Control of neuronalprecursor proliferation in the cerebellum by SonicHedgehog. Neuron 22, 103–114 (1999).
76. Sauvageau, G. et al. Overexpression of HOXB4 inhematopoietic cells causes the selective expansion ofmore primitive populations in vitro and in vivo. Genes Dev.9, 1753–1765 (1995).
77. Thorsteinsdottir, U., Sauvageau, G. & Humphries, R. K.Enhanced in vivo regenerative potential of HOXB4-transduced hematopoietic stem cells with regulation oftheir pool size. Blood 94, 2605–2612 (1999).
78. Antonchuk, J., Sauvageau, G. & Humphries, R. K.HOXB4-induced expansion of adult hematopoietic stemcells ex vivo. Cell 109, 39–45 (2002).
79. Pardal, R., Clarke, M. F. & Morrison, S. J. Applying theprinciples of stem-cell biology to cancer. Nature Rev.Cancer 3, 895–902 (2003).
80. Valk-Lingbeek, M. E., Bruggeman, S. W. & van Lohuizen, M.Stem cells and cancer; the polycomb connection. Cell118, 409–418 (2004).
81. Taipale, J. & Beachy, P. A. The Hedgehog and Wntsignalling pathways in cancer. Nature 411, 349–354(2001).
82. Schweisguth, F. Notch signaling activity. Curr. Biol. 14,R129–R138 (2004).
83. Shen, Q. et al. Endothelial cells stimulate self-renewal andexpand neurogenesis of neural stem cells. Science 304,1338–1340 (2004).
84. Hitoshi, S. et al. Notch pathway molecules are essentialfor the maintenance, but not the generation, ofmammalian neural stem cells. Genes Dev. 16, 846–858(2002).
85. Radtke, F., Wilson, A., Mancini, S. J. & MacDonald, H. R.Notch regulation of lymphocyte development andfunction. Nature Immunol. 5, 247–253 (2004).
86. Weng, A. P. & Aster, J. C. Multiple niches for Notch incancer: context is everything. Curr. Opin. Genet. Dev. 14,48–54 (2004).
87. Radtke, F. & Raj, K. The role of Notch in tumorigenesis:oncogene or tumour suppressor? Nature Rev. Cancer 3,756–767 (2003).
88. Ellisen, L. W. et al. TAN-1, the human homolog of theDrosophila Notch gene, is broken by chromosomaltranslocations in T lymphoblastic neoplasms. Cell 66,649–661 (1991).
89. Aster, J. C. et al. Essential roles for ankyrin repeat andtransactivation domains in induction of T-cell leukemia byNotch1. Mol. Cell. Biol. 20, 7505–7515 (2000).
90. Hoemann, C. D., Beaulieu, N., Girard, L., Rebai, N. &Jolicoeur, P. Two distinct Notch1 mutant alleles areinvolved in the induction of T-cell leukemia in c-myctransgenic mice. Mol. Cell. Biol. 20, 3831–3842 (2000).
91. Weng, A. P. et al. Activating mutations of NOTCH1 inhuman T cell acute lymphoblastic leukemia. Science 306,269–271 (2004).
92. Berry, L. W., Westlund, B. & Schedl, T. Germ-line tumorformation caused by activation of glp-1, a Caenorhabditiselegans member of the Notch family of receptors.Development 124, 925–936 (1997).
93. Krumlauf, R. Hox genes in vertebrate development. Cell78, 191–201 (1994).
39. Blair, A., Hogge, D. E. & Sutherland, H. J. Most acutemyeloid leukemia progenitor cells with long-termproliferative ability in vitro and in vivo have thephenotype CD34+/CD71–/HLA–DR–. Blood 92,4325–4335 (1998).
40. Blair, A. & Sutherland, H. J. Primitive acute myeloidleukemia cells with long-term proliferative ability in vitroand in vivo lack surface expression of c-kit (CD117). Exp.Hematol. 28, 660–671 (2000).
41. Cobaleda, C. et al. A primitive hematopoietic cell is thetarget for the leukemic transformation in humanphiladelphia-positive acute lymphoblastic leukemia.Blood 95, 1007–1013 (2000).
42. Cox, C. V. et al. Characterization of acute lymphoblasticleukemia progenitor cells. Blood 104, 2919–2925(2004).
43. Deininger, M., Goldman, J. & Melo, J. The molecularbiology of chronic myeloid leukemia. Blood 96,3343–3356 (2000).
44. Martin, P. J. et al. Involvement of the B-lymphoid systemin chronic myelogenous leukaemia. Nature 287, 49–50(1980).
45. Jamieson, C. H. et al. Granulocyte-macrophageprogenitors as candidate leukemic stem cells in blast-crisis CML. N. Engl J. Med. 351, 657–667 (2004).
46. Al-Hajj, M., Wicha, M., Benito-Hernandez, A., Morrison,S. & Clarke, M. Prospective identification of tumorigenicbreast cancer cells. Proc. Natl Acad. Sci. USA 100,3983–3988. (2003).
47. Singh, S. K. et al. Identification of a cancer stem cell inhuman brain tumors. Cancer Res. 63, 5821–5828(2003).
48. Hemmati, H. D. et al. Cancerous stem cells can arisefrom pediatric brain tumors. Proc. Natl Acad. Sci. USA100, 15178–15183 (2003).
49. Ignatova, T. N. et al. Human cortical glial tumors containneural stem-like cells expressing astroglial and neuronalmarkers in vitro. Glia 39, 193–206 (2002).
50. Singh, S. K. et al. Identification of human brain tumourinitiating cells. Nature 432, 396–401 (2004).
51. Chesier, S., Morrison, S., Liao, X. & Weissman, I. In vivoproliferation and cell cycle kinetics of long-term self-renewing hematopoietic stem cells. Proc. Natl Acad. Sci.USA 96, 3120–3125 (1999).
52. Bradford, G., Williams, B., Rossi, R. & Bertoncello, I.Quiescence, cycling, and turnover in the primitivehematopoietic stem cell compartment. Exp. Hematol. 25,445–453 (1997).
53. Lansdorp, P. Self-renewal of stem cells. Biol. BloodMarrow Transplant. 3, 171–178 (1997).
54. Morrison, S., Prowse, K., Ho, P. & Weissman, I.Telomerase activity in hematopoietic cells is associatedwith self-renewal potential. Immunity 5, 207–216(1996).
55. Manz, M. G., Miyamoto, T., Akashi, K. & Weissman, I. L.Prospective isolation of human clonogenic commonmyeloid progenitors. Proc. Natl Acad. Sci. USA 99,11872–11877 (2002).
56. Mehrotra, B. et al. Cytogenetically aberrant cells in thestem cell compartment (CD34+lin–) in acute myeloidleukemia. Blood 86, 1139–1117 (1995).
57. Haase, D. et al. Evidence for malignant transformation inacute myeloid leukemia at the level of early hematopoieticstem cells by cytogenetic analysis of CD34+
subpopulations. Blood 86, 2906–2912. (1995).58. Quijano, C. et al. Cytogenetically aberrant cells are
present in the CD34+CD33–38–19– marrow compartmentin children with acute lymphoblastic leukemia. Leukemia11, 1508–1515 (1997).
59. Passegue, E., Wagner, E. F. & Weissman, I. L. JunBdeficiency leads to a myeloproliferative disorder arisingfrom hematopoietic stem cells. Cell 119, 431–443(2004).
60. Hope, K. J., Jin, L. & Dick, J. E. Acute myeloid leukemiaoriginates from a hierarchy of leukemic stem cell classesthat differ in self-renewal capacity. Nature Immunol. 5,738–743 (2004).
61. Cozzio, A. et al. Similar MLL-associated leukemias arisingfrom self-renewing stem cells and short-lived myeloidprogenitors. Genes Dev. 17, 3029–3035 (2003).
62. Huntly, B. J. P. et al. MOZ–TIF2, but not BCR–ABL,confers properties of leukemic stem cells to committedmurine hematopoietic progenitors. Cancer Cell 6,587–596 (2004).
63. Ernst, P., Wang, J. & Korsmeyer, S. J. The role of MLL inhematopoiesis and leukemia. Curr. Opin. Hematol. 9,282–287 (2002).
64. Deguchi, K. et al. MOZ–TIF2-induced acute myeloidleukemia requires the MOZ nucleosome binding motifand TIF2-mediated recruitment of CBP. Cancer Cell 3,259–271 (2003).

© 2005 Nature Publishing Group
P E R S P E C T I V E S
puncture, which can occur during any of theminimally invasive procedures described inBOX 1. A high-energy focused ultrasoundbeam is directed harmlessly across the skinand intervening tissues towards the targettumour. Only at the focus of the beam is theenergy level great enough to cause a tempera-ture rise sufficient for instantaneous celldeath. The mechanism of action of HIFU isnot tumour-specific and so a wide range oftumour types can be targeted. In addition, incontrast to ionizing radiation, treatment canbe given more than once as there is no upperlimit of tissue tolerance to repeated ultra-sound exposure. There are very few sideeffects of treatment, and serious adverseevents are rare. As a result, HIFU treatmentwith palliative intent, aimed either towardssymptom or local tumour control can also beseriously contemplated for patients withpoor prognoses.
In several centres worldwide, HIFU isnow being used clinically to treat solidtumours (both malignant and benign),including those of the prostate4, liver5,6,breast7, kidney8, bone and pancreas, andsoft-tissue sarcoma6. This has only been thecase for the past 5 years, so, perhaps with theexception of prostate cancer, the evidencebase for long-term efficacy is far frommature. However current data are veryencouraging and the role of HIFU in oncol-ogy is likely to expand as devices becomemore widely available.
How does HIFU work?The term ‘ultrasound’ refers to mechanicalvibrations above the threshold of humanhearing (16 kHz). Medical ultrasound is gen-erated by applying an alternating voltageacross a piezoelectric material such as lead zir-conate titanate. Such materials oscillate inthickness at the same frequency as the drivingcurrent. The resulting ultrasound wave prop-agates through tissues, causing alternatingcycles of increased and reduced pressure(compression and rarefaction, respectively).Most of us are familiar with diagnostic ultra-sound, which usually uses frequencies in therange of 1–20 MHz. By contrast, frequenciesof 0.8–3.5 MHz are generally used during theclinical applications of HIFU, and the energylevels carried in the HIFU beam are severalorders of magnitude greater than those of astandard diagnostic ultrasound beam. In away analogous to the focusing of light, ultra-sound waves can be focused at a given point.The high energy levels carried in a HIFUbeam can therefore be magnified further anddelivered with precision to a small volume,while sparing surrounding tissues9.
120. Guzman, M. et al. The sesquiterpene lactoneparthenolide induces apoptosis of human acute leukemiastem and progenitor cells. Blood 1 Feb 2005 (doi:10.1182/blood-2004-10-4135).
121. Bonner, W. A., Hulett, H. R., Sweet, R. G. & Herzenberg, L.A. Fluorescence activated cell sorting. Rev. Sci. Instrum.43, 404–409 (1972).
122. Czitrom, A. A. et al. The function of antigen-presentingcells in mice with severe combined immunodeficiency. J.Immunol. 134, 2276–2280 (1985).
123. Prochazka, M., Gaskins, H. R., Shultz, L. D. & Leiter, E. H.The nonobese diabetic scid mouse: model forspontaneous thymomagenesis associated withimmunodeficiency. Proc. Natl Acad. Sci. USA 89,3290–3294 (1992).
124. Dick, J. E. Human stem cell assays in immune-deficientmice. Curr. Opin. Hematol. 3, 405–409 (1996).
125. Larochelle, A. et al. Identification of primitive humanhematopoietic cells capable of repopulatingNOD/SCID mouse bone marrow: implications for gene therapy. Nature Med. 2, 1329–1337 (1996).
126. Wang, J. C. et al. High level engraftment ofNOD/SCID mice by primitive normal and leukemichematopoietic cells from patients with chronicmyeloid leukemia in chronic phase. Blood 91,2406–2414 (1998).
AcknowledgementsWe acknowledge the members of the Gilliland lab for helpful dis-cussion. D.G.G. is an Investigator of the Howard Hughes MedicalInstitute and is a Doris Duke Distinguished Clinical Scientist.B.J.P.H is a Senior Clinical Fellow of the Leukaemia ResearchFund (UK).
Competing interests statementThe authors declare no competing financial interests.
Online links
DATABASESThe following terms in this article are linked online to:Cancer.gov: http://cancer.gov/acute lymphoblastic leukaemia | acute myelogenousleukaemia | chronic myelogenous leukaemia Entrez Gene:http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=geneABL | BCR | HOX11 | HOX11L2 | HOXA9 | HOXB4 | HOXD13 |NOTCH1 | NUP98
FURTHER INFORMATIONGilliland laboratory:http://www.hms.harvard.edu/dms/bbs/fac/gilliland.htmlAccess to this interactive links box is free online.
NATURE REVIEWS | CANCER VOLUME 5 | APRIL 2005 | 321
High-intensity focused ultrasound inthe treatment of solid tumours
James E. Kennedy
I N N O VAT I O N
Abstract | Traditionally, surgery has been theonly cure for many solid tumours.Technological advances have catalysed ashift from open surgery towards lessinvasive techniques. Laparoscopic surgeryand minimally invasive techniques continueto evolve, but for decades high-intensityfocused ultrasound has promised to deliverthe ultimate objective — truly non-invasivetumour ablation. Only now, however, withrecent improvements in imaging, has thisobjective finally emerged as a real clinicalpossibility.
The 1990s witnessed an explosion in mini-mally invasive alternatives to open surgeryfor localized malignancy. Quite apart fromthe inherent attractions of new technology,the incentives behind this movement areplain. Open surgery is associated with signif-icant morbidity and with mortality, andcauses suppression of a patient’s immunesystem, which in turn can lead to the risk ofperioperative metastatic tumour dissemina-tion. Patients themselves usually complain ofpostoperative pain and recovery can belengthy. Laparoscopic surgery might bemore acceptable to patients, and leads to aquicker return to work, but usually takes
longer, and both operative morbidity andmortality are broadly comparable with opensurgery.
Other minimally invasive techniques usea range of energy-based methods for in situtumour destruction. Apart from radiother-apy, these include radiofrequency ablation,laser ablation, cryoablation (BOX 1) and high-intensity focused ultrasound (HIFU). Inprinciple, where surgery usually aims toremove a tumour with an adequate normal-tissue margin, if a minimally invasive tech-nique can destroy the equivalent tissue volume, then outcome in terms of disease-free survival should be at least equal. Ifoperative mortality is avoided, then out-come could even be better. In fact, taking theexample of interstitial laser ablation for iso-lated colorectal liver metastases, data arenow emerging to support this assertion1.
Treatment with HIFU is the only one ofthese alternatives to surgery that is truly non-invasive. Theoretical advantages of this lackof invasiveness are that there is no risk oftumour seeding along a needle track, whichhas been reported after procedures such as percutaneous ethanol injection2 andradiofrequency ablation3, and there is no riskof haemorrhage from visceral or vascular