Embed Size (px)
Citation preview
Hybrid Imaging of Infection 9th Annual AFIM Meeting, Haifa May 2011
Ora Israel, MDDepartment of Nuclear Medicine
Rambam Health Care Campus
Technion, Israel Institute of Technology
Haifa, Israel
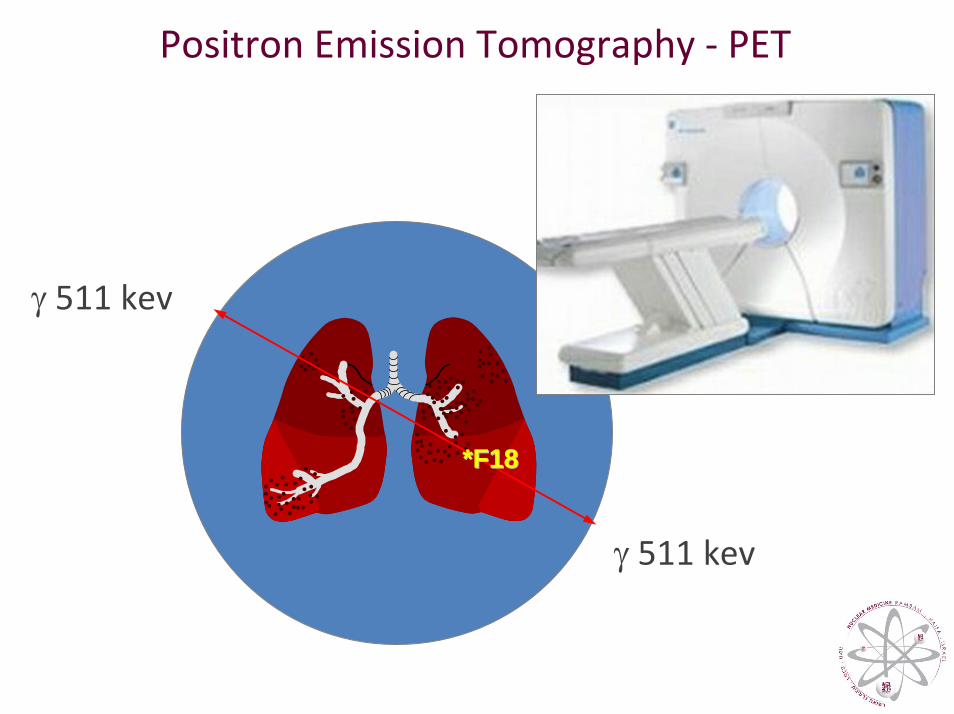
Positron Emission Tomography ‐ PET
γ 511 kev
γ 511 kev
**F18F18
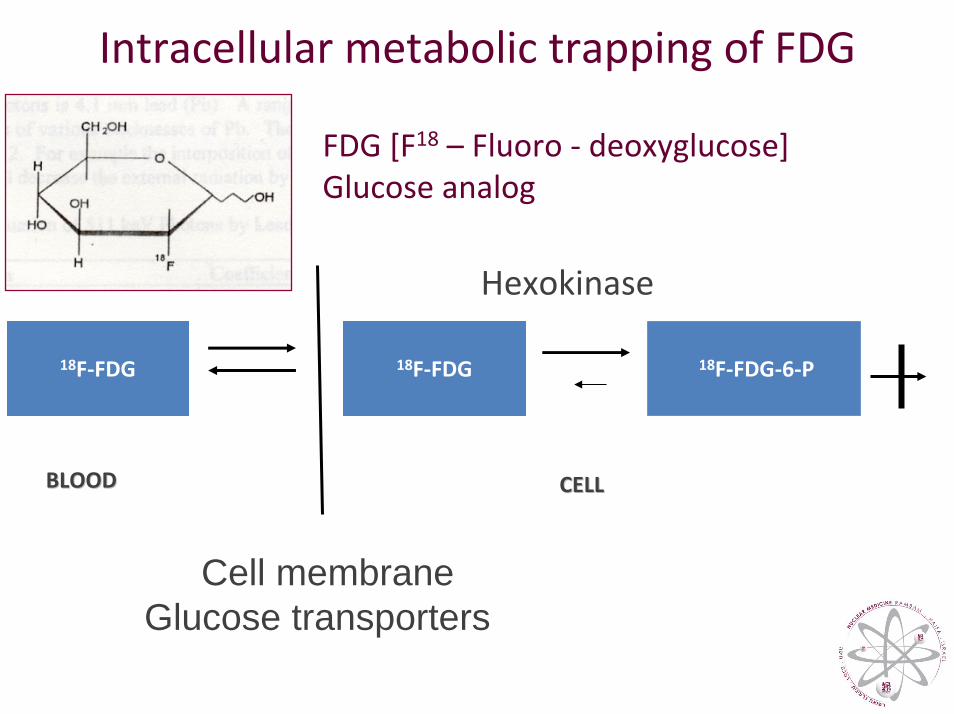
18F‐FDG 18F‐FDG 18F‐FDG‐6‐P
CELL CELL BLOODBLOOD
Hexokinase
Cell membraneGlucose transporters
Intracellular metabolic trapping of FDG
FDG [F18 – Fluoro ‐ deoxyglucose]Glucose analog
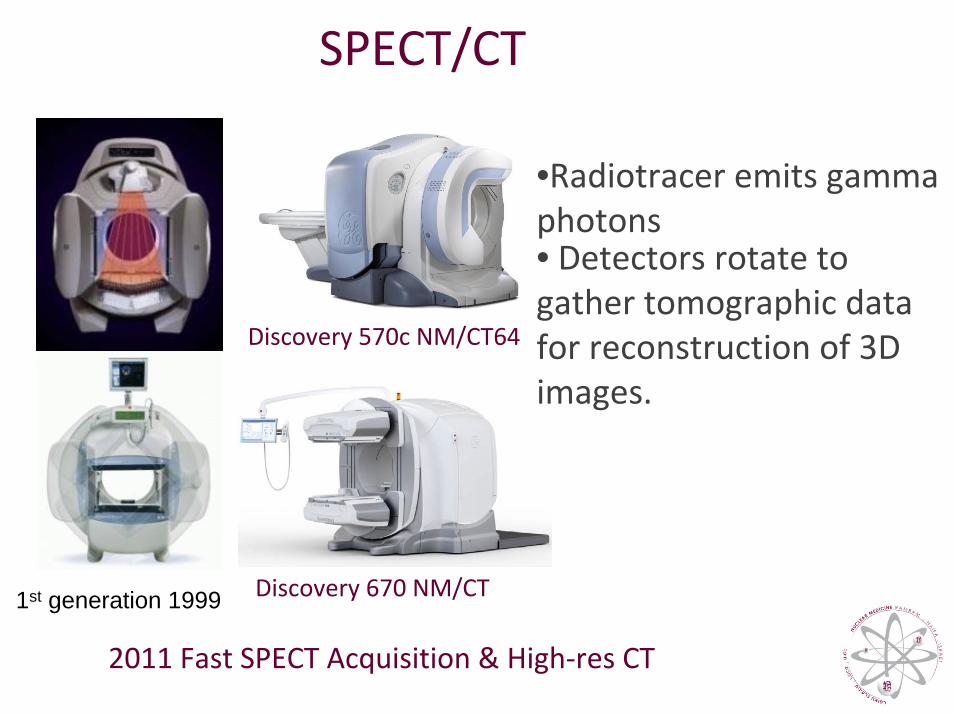
SPECT/CT
Discovery 670 NM/CT
Discovery 570c NM/CT64
•Radiotracer emits gamma photons • Detectors rotate to gather tomographic data for reconstruction of 3D images.
1st generation 1999
2011 Fast SPECT Acquisition & High‐res CT
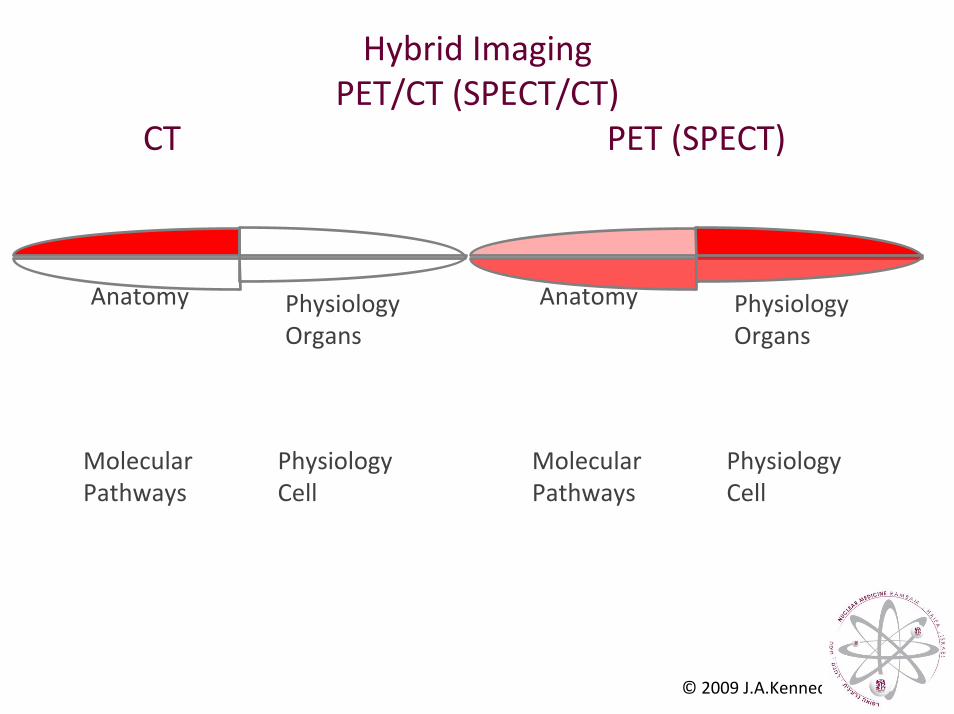
Hybrid ImagingPET/CT (SPECT/CT)
CT PET (SPECT)
Anatomy
PhysiologyCell
Molecular Pathways
PhysiologyOrgans
Anatomy
PhysiologyCell
Molecular Pathways
PhysiologyOrgans
© 2009 J.A.Kennedy
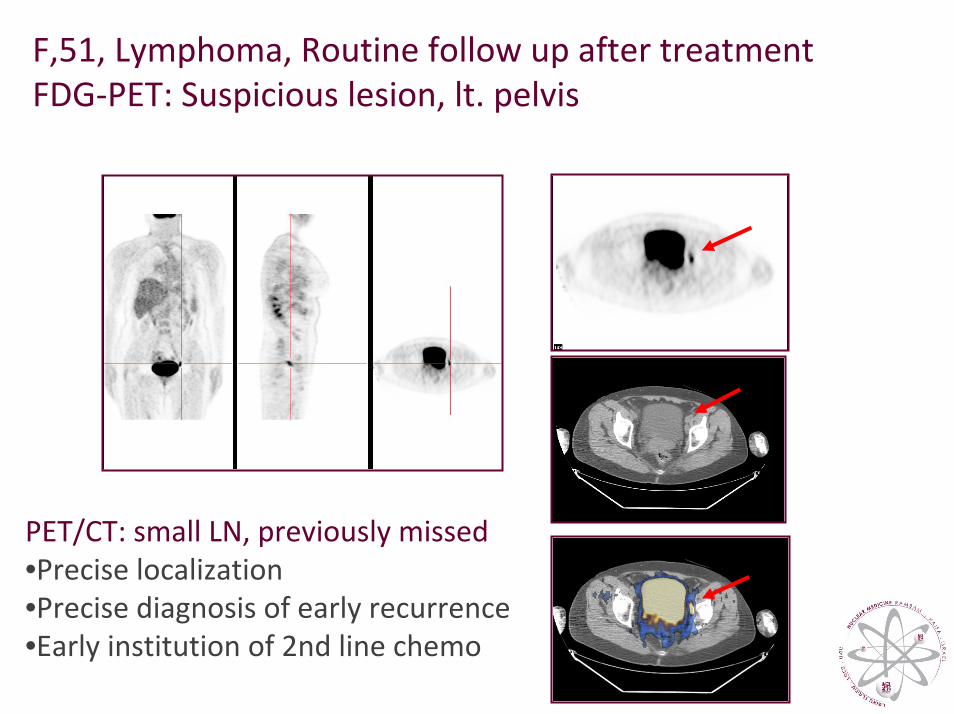
F,51, Lymphoma, Routine follow up after treatment FDG‐PET: Suspicious lesion, lt. pelvis
PET/CT: small LN, previously missed •Precise localization•Precise diagnosis of early recurrence•Early institution of 2nd line chemo
Almost three decades ago, the Surgeon General of the United States testified to Congress that it was time to "close the book on infectious diseases".…
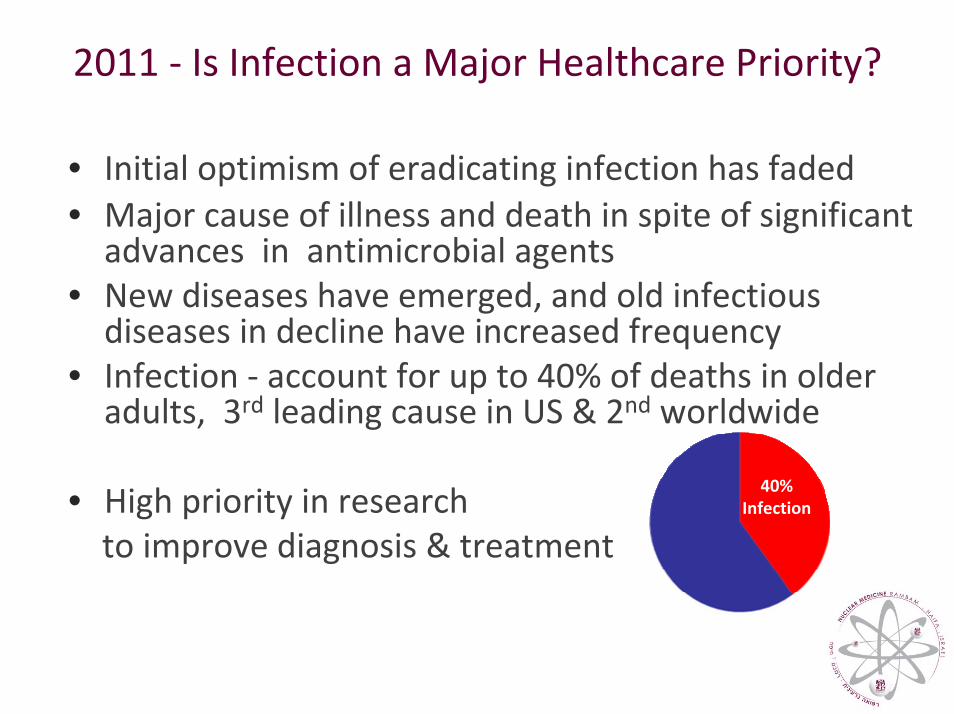
2011 ‐ Is Infection a Major Healthcare Priority?
• Initial optimism of eradicating infection has faded • Major cause of illness and death in spite of significant advances in antimicrobial agents
• New diseases have emerged, and old infectious diseases in decline have increased frequency
• Infection ‐ account for up to 40% of deaths in older adults, 3rd leading cause in US & 2nd worldwide
• High priority in researchto improve diagnosis & treatment
40%Infection
Nuclear Medicine Assessing Infection and Inflammation
• Fever of unknown origin
• Osteomyelitis
• Lung infection
• Endocarditis
• Vascular prosthetic infection
• Abdominal infection
• Assessment of disease activity in IBD
• Kidney/transplant infection
Radiotracers for Infection Imaging
SPECT Tracers • Gallium‐67• In‐111 & Tc‐99m Leucocytes• Labeled Human Immunoglobulin• Labeled Antigranulocyte Antibodies• Labeled Peptides
PET Tracers• F18‐FDG (Fluorodeoxy‐Glucose) (PET)• FDG‐labeled Leucocytes
FDG‐PET in Infection & Inflammation
Inflammatory cells & granulation tissue (activated lymphocytes, neutrophils, macrophages) as well as malignant cells, exhibit high intracellular levels of hexokinase & increased expression of surface glucose transporter proteins with high affinity to FDG
“the blessing of the curse…”
FDG‐imaging – a good alternative for assessment of infection and inflammation
Nuclear Medicine ProceduresPros:
• Highly sensitive
• Whole body imaging
• Detection & characterization of functional alterations
Infectious processes may be visualized in their early phases when anatomic lesions are not yet detectable.
Cons:• Poor physical characteristics & image quality degradation • Lack of anatomical landmarks • Non‐specificity of tracers
[Conventional] Imaging of Infection
Timely diagnosis: critical for appropriate management
Pros ‐ High resolution imaging• CT: bone destruction, soft tissue changes • MRI: sensitive for osteomyelitis• US: fluid collections
Cons• limited value in early stages (insignificant/no infection‐related tissue
changes) • After treatment: difficult differential diagnosis between active and
indolent morphologic changes • challenging in the presence of:
• coexisting pathology (eg: fractures, osteo‐arthropathy)• coexisting structural changes related to treatment and/or healing (eg: bone remodeling, post‐operative edema, scar, fibrosis)
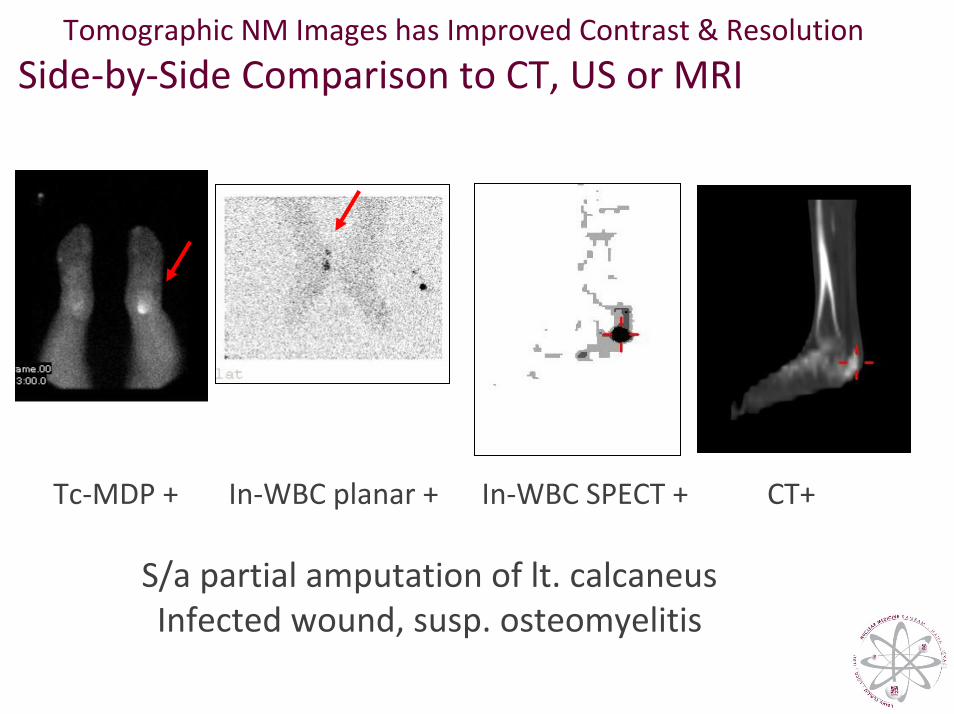
Tomographic NM Images has Improved Contrast & Resolution
Side‐by‐Side Comparison to CT, US or MRI
Tc‐MDP + In‐WBC planar + In‐WBC SPECT + CT+
S/a partial amputation of lt. calcaneusInfected wound, susp. osteomyelitis
NM (SPECT/PET) & CT Complementary Role in
Patients with Suspected Infection
SPECT – detection of a suspicious focus CT – precise localization to tissue/organ
CT – detection of an anatomic lesionSPECT ‐ confirmed as active infectious process
Correlation of anatomical & functional data obtained from tests performed on different devices, on
different days, is difficult
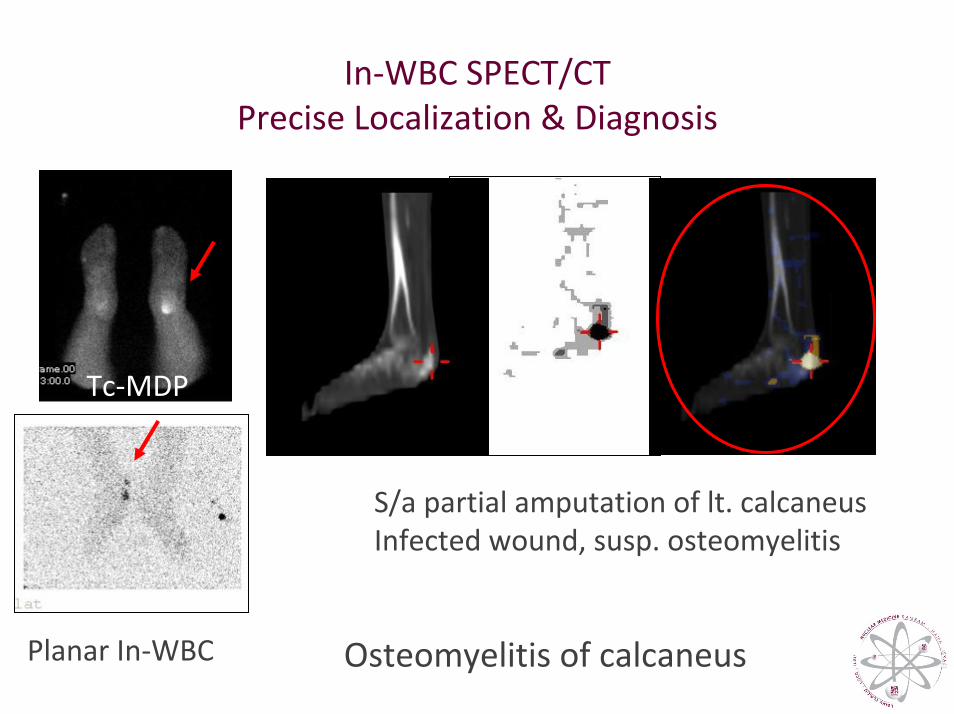
In‐WBC SPECT/CTPrecise Localization & Diagnosis
Tc‐MDP
S/a partial amputation of lt. calcaneusInfected wound, susp. osteomyelitis
Planar In‐WBC Osteomyelitis of calcaneus
Hybrid Imaging (SPECT/CT & PET/CT) Assessment of Infection The Experience
SPECT/CT• Ga‐67: FUO, susp. abscess, osteomyelitis• In‐111/Tc‐99m WBC: vascular graft &
complicated bone infection
FDG‐PET/CT• Vascular graft infection• Diabetic foot• FUO
Vascular Graft Infection
• Uncommon (0.5‐5%) but severe complication• Eradication: rarely possible • Prognosis: poor, with life or limb loss (>50% pts)• Diagnosis: early & accurate is challenging • CT: diagnostic procedure of choice; high resolution
FP: after recent Sx, FN: low‐grade, early‐stage infection • Delay in treatment: severe complications• Main successful treatment: Sx removing the infected graft
high morbidity procedure
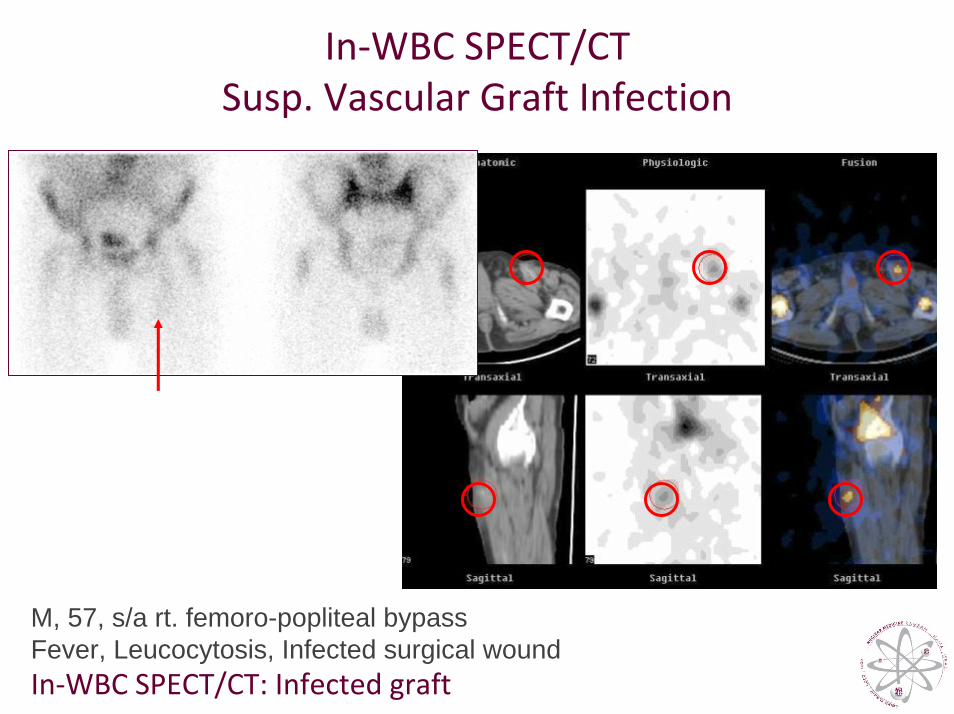
In‐WBC SPECT/CTSusp. Vascular Graft Infection
M, 57, s/a rt. femoro-popliteal bypassFever, Leucocytosis, Infected surgical wound In‐WBC SPECT/CT: Infected graft
Ga‐67 & WBC SPECT/CT for Diagnosis and Localization of Infection
Bar‐Shalom et al, J Nucl Med 2006
82 patientsSPECT/CT– better diagnosis & localization in ~50% ptsGa‐67 SPECT/CT contributory in 36% of 47 pts
48% with susp. osteomyelitis23% with susp. soft‐tissue infection
31% with FUOWBC ‐ SPECT/CT was contributory in 63% of 35 pts:
67% ‐ with susp. vascular graft infection 55% ‐ with susp. osteomyelitis
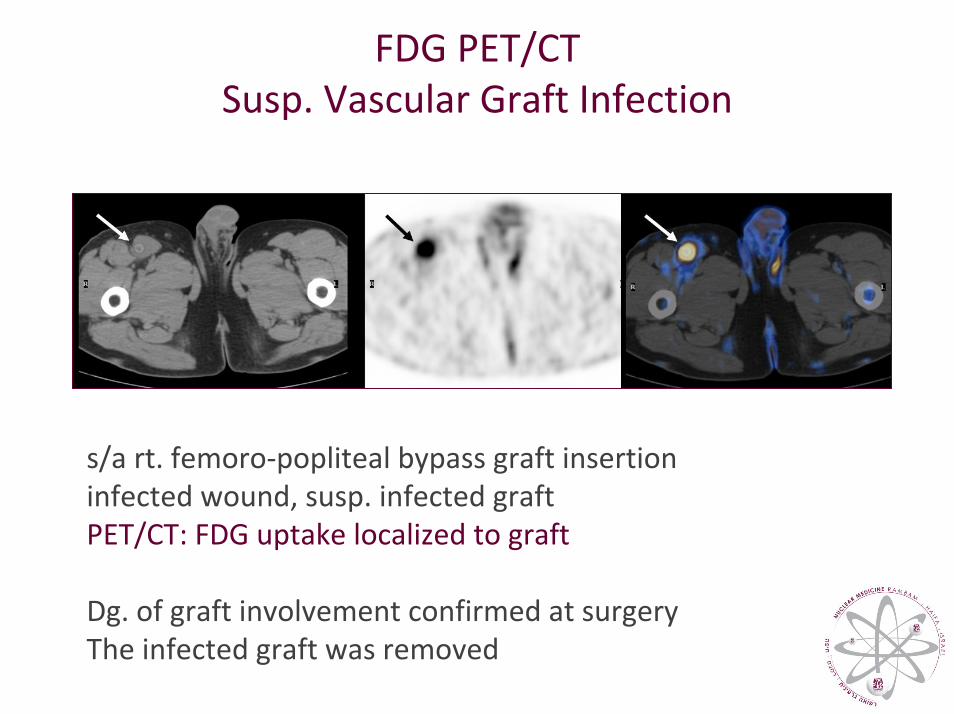
FDG PET/CTSusp. Vascular Graft Infection
s/a rt. femoro‐popliteal bypass graft insertion infected wound, susp. infected graft PET/CT: FDG uptake localized to graft
Dg. of graft involvement confirmed at surgery The infected graft was removed
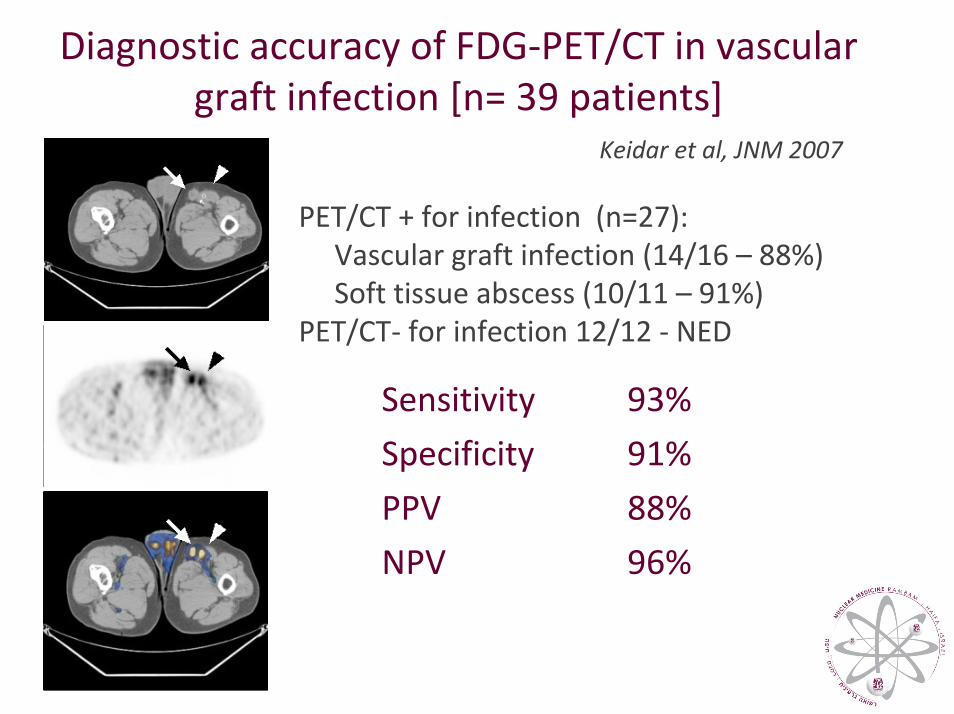
Diagnostic accuracy of FDG‐PET/CT in vascular graft infection [n= 39 patients]
Keidar et al, JNM 2007
PET/CT + for infection (n=27): Vascular graft infection (14/16 – 88%)Soft tissue abscess (10/11 – 91%)
PET/CT‐ for infection 12/12 ‐ NED
93%Sensitivity
91%Specificity
88%PPV
96%NPV
Diabetic FootCommon complication in DM
Difficult differential diagnosis: rapidly progressive neuropathic joint vs. osteomyelitis
Osteomyelitis: ̃1/3 infections, mainly direct spread from contaminated soft tissue
Early diagnosis: clinical challenge & crucial Antibiotic therapy can be curative & prevent amputation
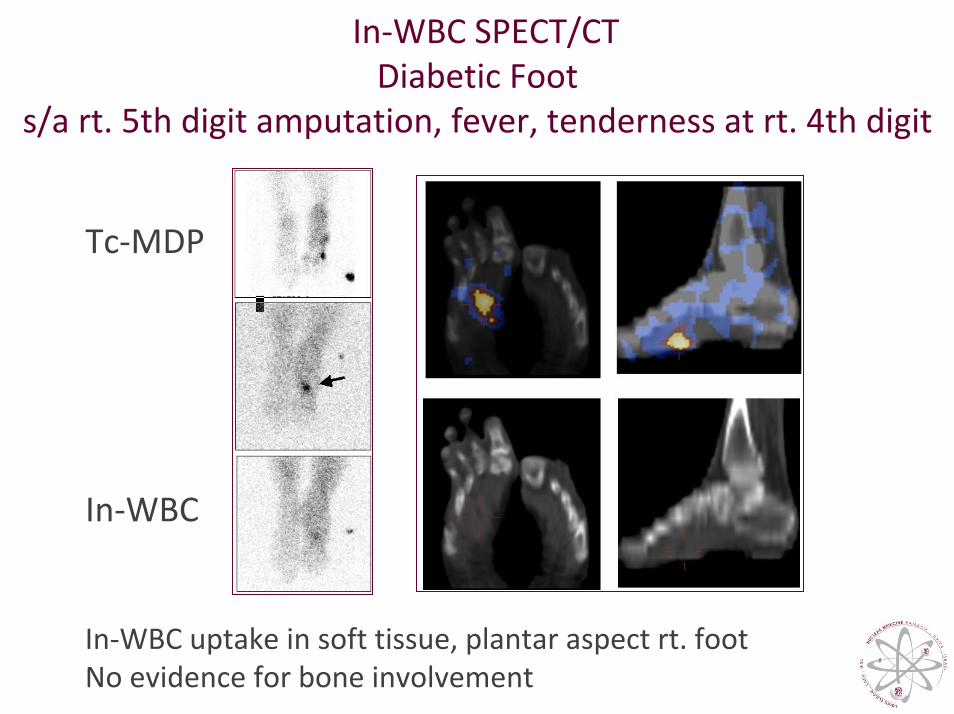
In‐WBC SPECT/CT Diabetic Foot
s/a rt. 5th digit amputation, fever, tenderness at rt. 4th digit
Tc‐MDP
In‐WBC
In‐WBC uptake in soft tissue, plantar aspect rt. footNo evidence for bone involvement
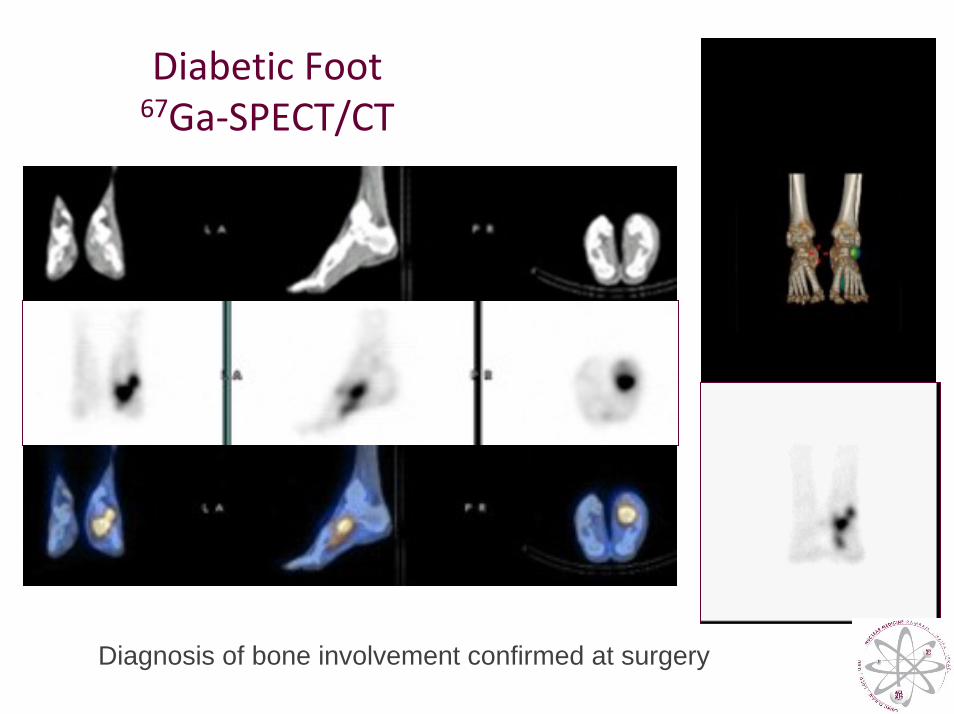
Diabetic Foot67Ga‐SPECT/CT
Diagnosis of bone involvement confirmed at surgery
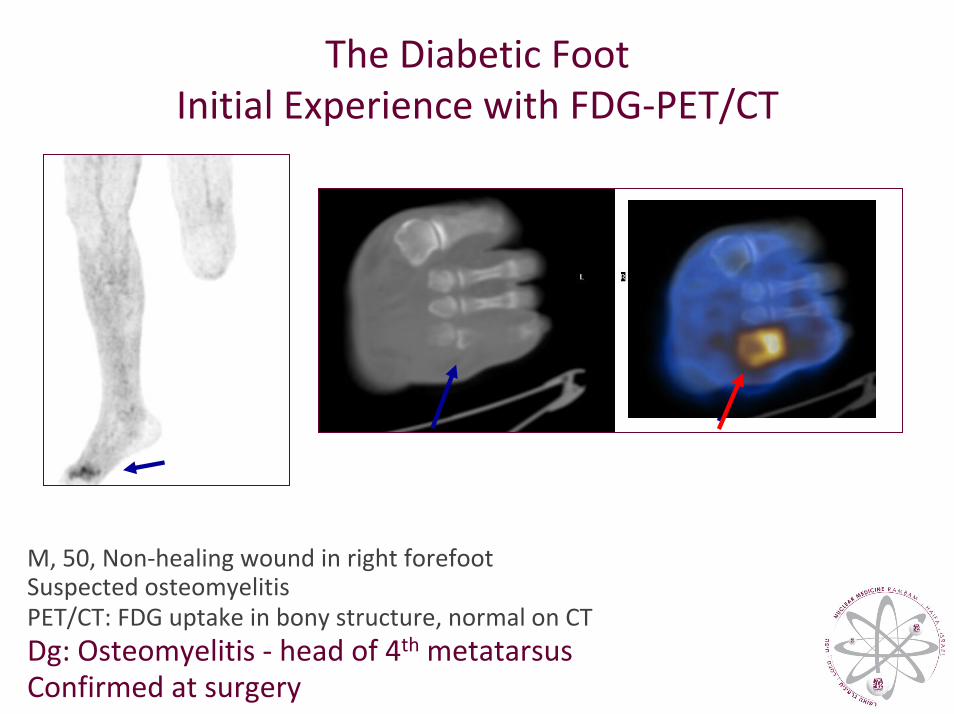
The Diabetic Foot Initial Experience with FDG‐PET/CT
M, 50, Non‐healing wound in right forefoot Suspected osteomyelitisPET/CT: FDG uptake in bony structure, normal on CTDg: Osteomyelitis ‐ head of 4th metatarsusConfirmed at surgery
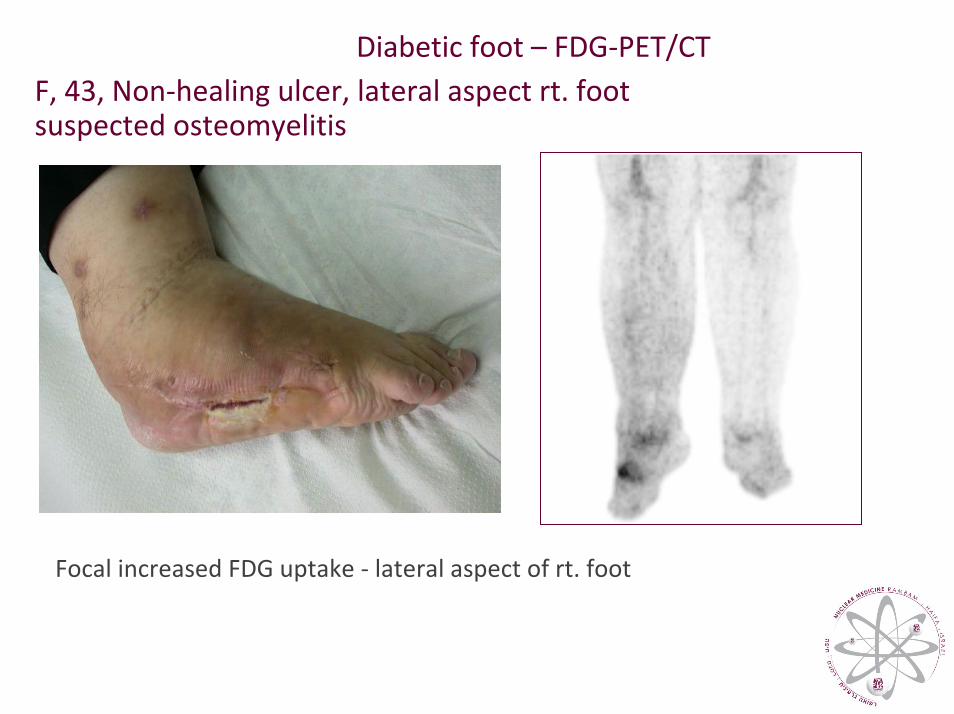
Diabetic foot – FDG‐PET/CTF, 43, Non‐healing ulcer, lateral aspect rt. foot suspected osteomyelitis
Focal increased FDG uptake ‐ lateral aspect of rt. foot
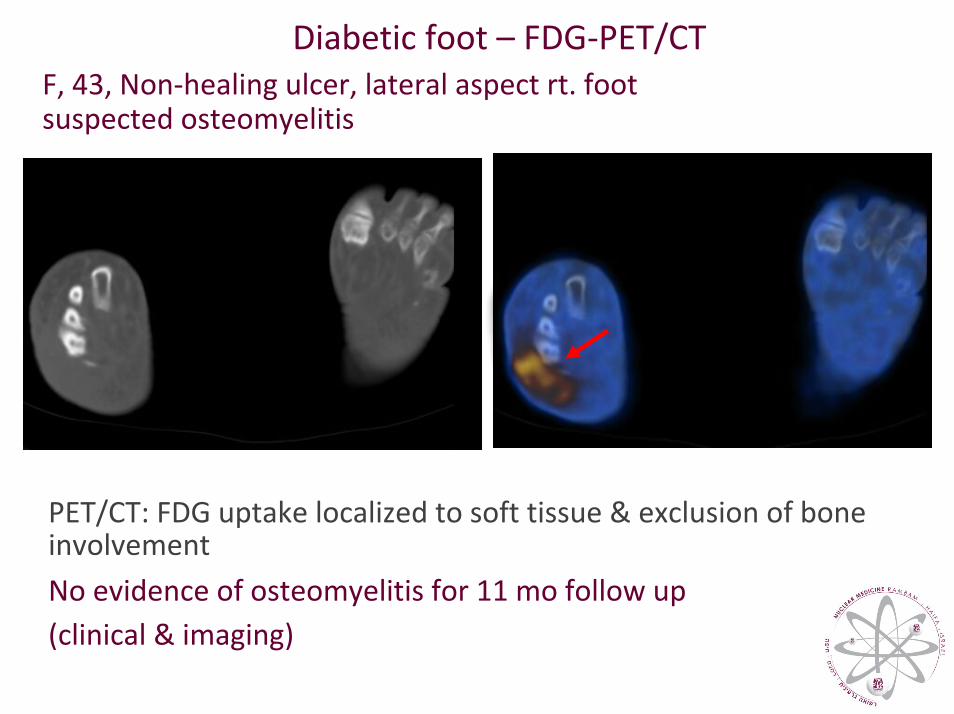
Diabetic foot – FDG‐PET/CT F, 43, Non‐healing ulcer, lateral aspect rt. foot suspected osteomyelitis
PET/CT: FDG uptake localized to soft tissue & exclusion of bone involvementNo evidence of osteomyelitis for 11 mo follow up (clinical & imaging)
PET/CT USING FDG FOR THE EVALUATION OF THE DIABETIC FOOT
Keidar et al, J Nucl Med, 2005
• PET/CT localized
75% (12/16) lesions to bone, further confirmed
19% (3/16) lesions to soft tissue, no further evidence of osteomyelitis
1 lesion, [mild FDG uptake] in neuropathicosteoarthropathy – false positive?
At present >50 patients
FDG uptake unrelated to glycaemic state
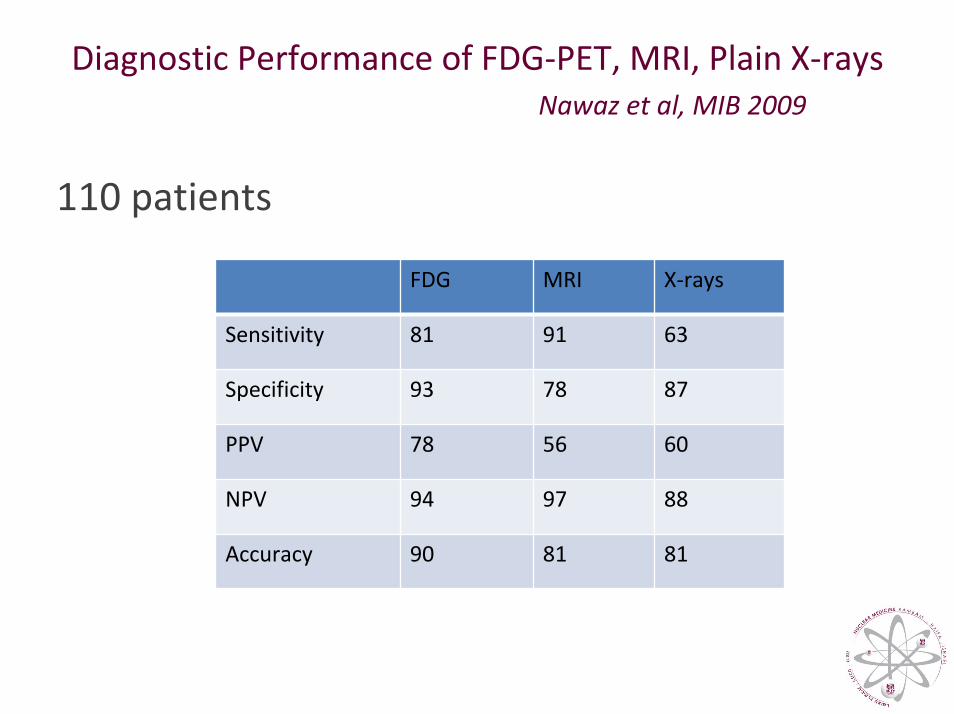
Diagnostic Performance of FDG‐PET, MRI, Plain X‐raysNawaz et al, MIB 2009
110 patients
FDG MRI X‐rays
Sensitivity 81 91 63
Specificity 93 78 87
PPV 78 56 60
NPV 94 97 88
Accuracy 90 81 81
Fever of Unknown Origin (FUO)
• Fever >38.3ºC, >3 weeks duration• Incidence: 7‐53% (geographic factors, definition) • Final Diagnosis:• Neoplasms ~1/3• Infection ~1/3• Collagen & granulomatous diseases ~1/3• Recent: decrease in patients with final etiology• Functional imaging approach: WBC, Ga‐67, FDG
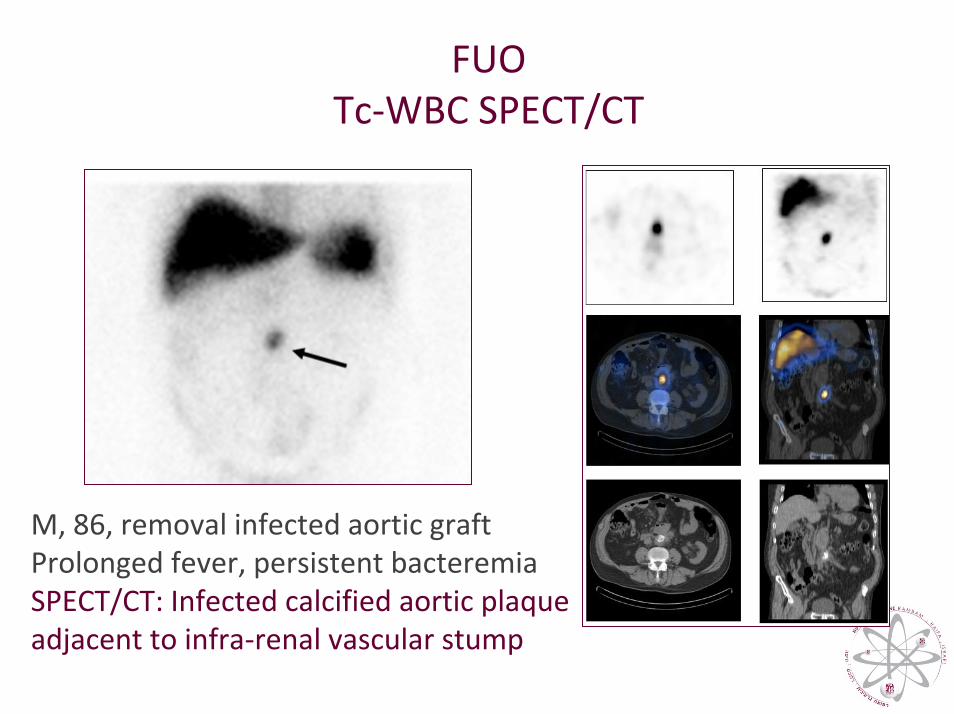
FUO Tc‐WBC SPECT/CT
M, 86, removal infected aortic graft Prolonged fever, persistent bacteremiaSPECT/CT: Infected calcified aortic plaque adjacent to infra‐renal vascular stump
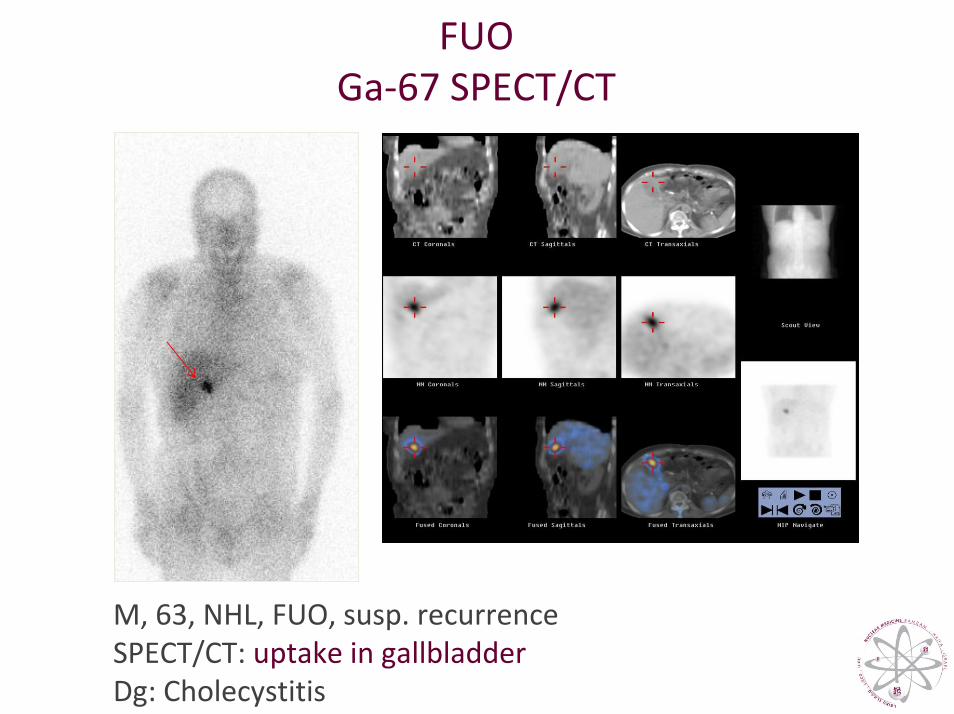
FUO Ga‐67 SPECT/CT
M, 63, NHL, FUO, susp. recurrence SPECT/CT: uptake in gallbladderDg: Cholecystitis
Ga‐67 & WBC SPECT/CT for Diagnosis & Localization of InfectionBar‐Shalom et al, J Nucl Med 2006
82 patients (88 susp. sites)SPECT/CT– better diagnosis & localization in ~50% ptsGa‐67 SPECT/CT contributory in 36% of 47 pts
48% with susp. osteomyelitis23% with susp. soft‐tissue infection
31% with FUOWBC ‐ SPECT/CT was contributory in 63% of 35 pts:
67% ‐ with susp. vascular graft infection 55% ‐ with susp. osteomyelitis
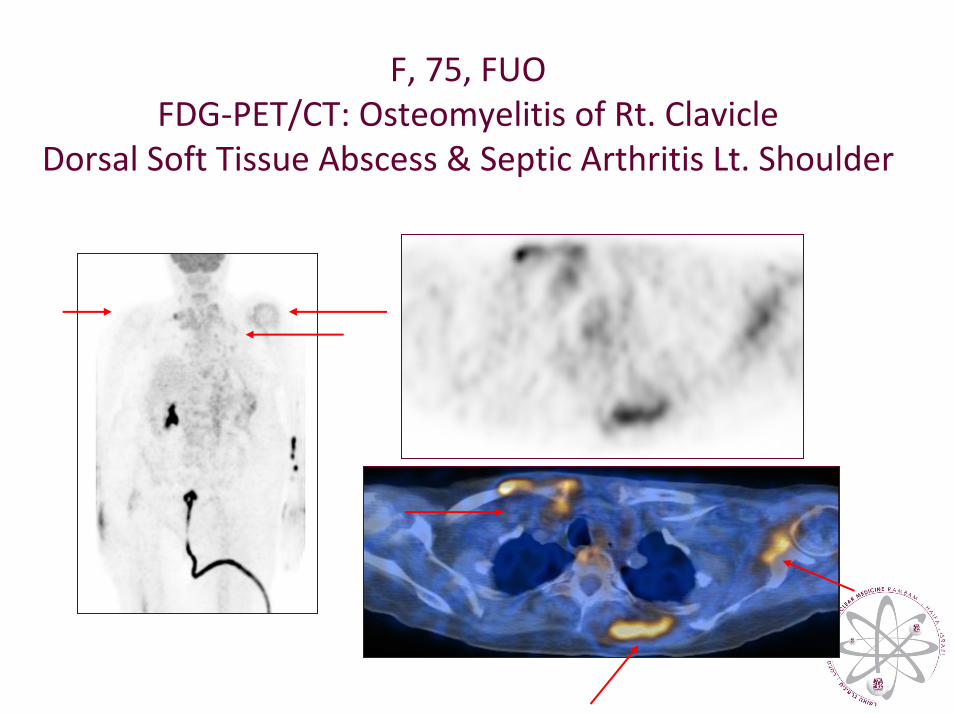
F, 75, FUOFDG‐PET/CT: Osteomyelitis of Rt. Clavicle
Dorsal Soft Tissue Abscess & Septic Arthritis Lt. Shoulder
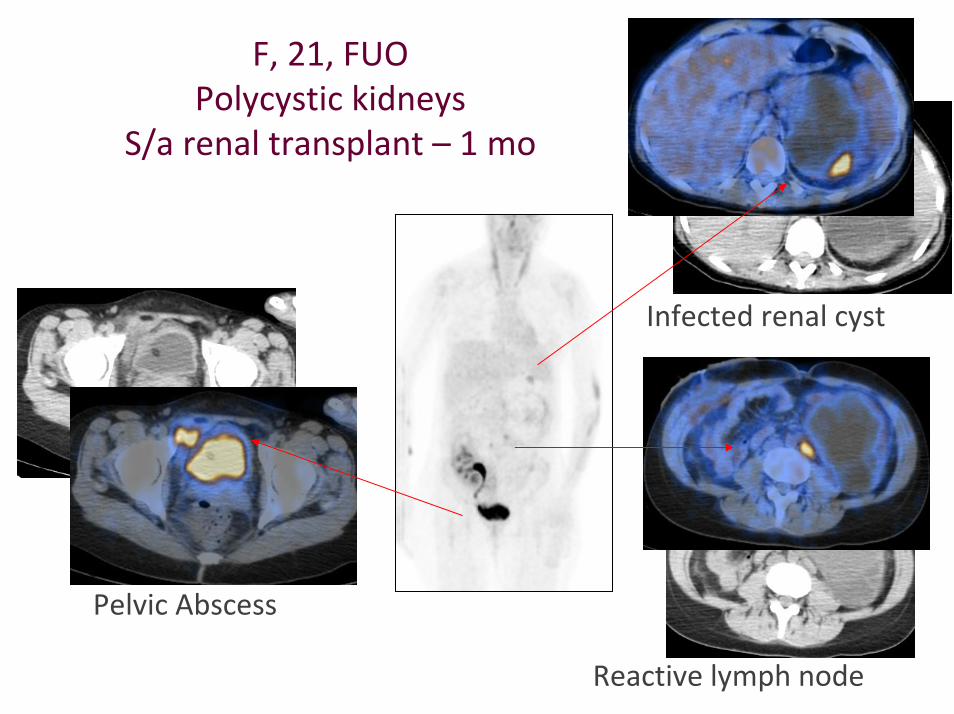
F, 21, FUOPolycystic kidneys
S/a renal transplant – 1 mo
Infected renal cyst
Reactive lymph node
Pelvic Abscess
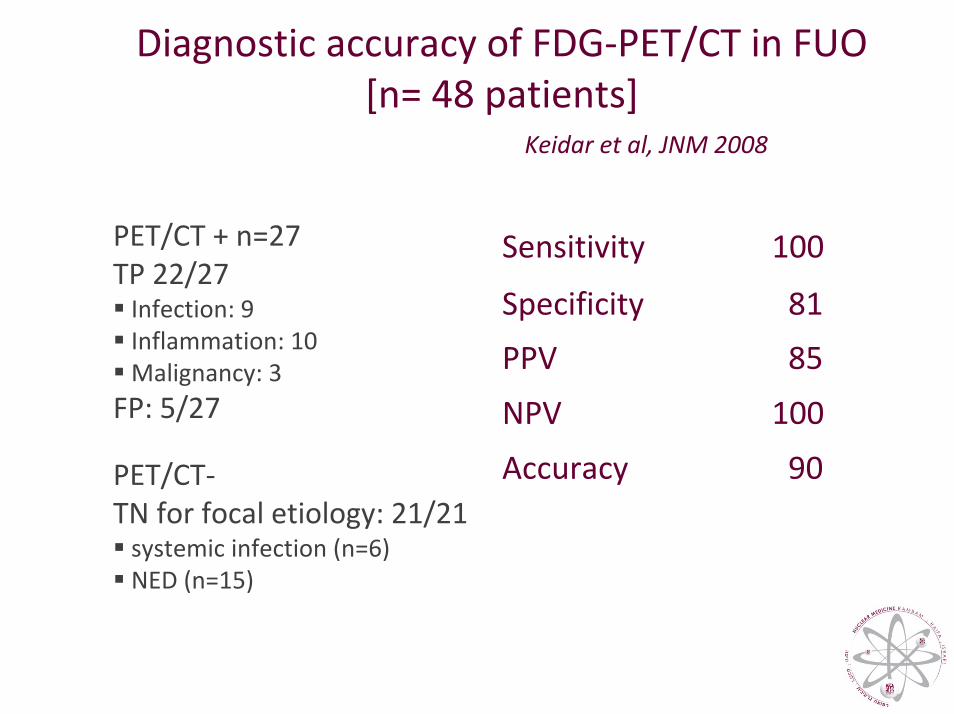
Diagnostic accuracy of FDG‐PET/CT in FUO [n= 48 patients]
100Sensitivity
81Specificity
85PPV
100NPV
90Accuracy
PET/CT + n=27 TP 22/27Infection: 9 Inflammation: 10Malignancy: 3
FP: 5/27
PET/CT‐TN for focal etiology: 21/21systemic infection (n=6)NED (n=15)
Keidar et al, JNM 2008
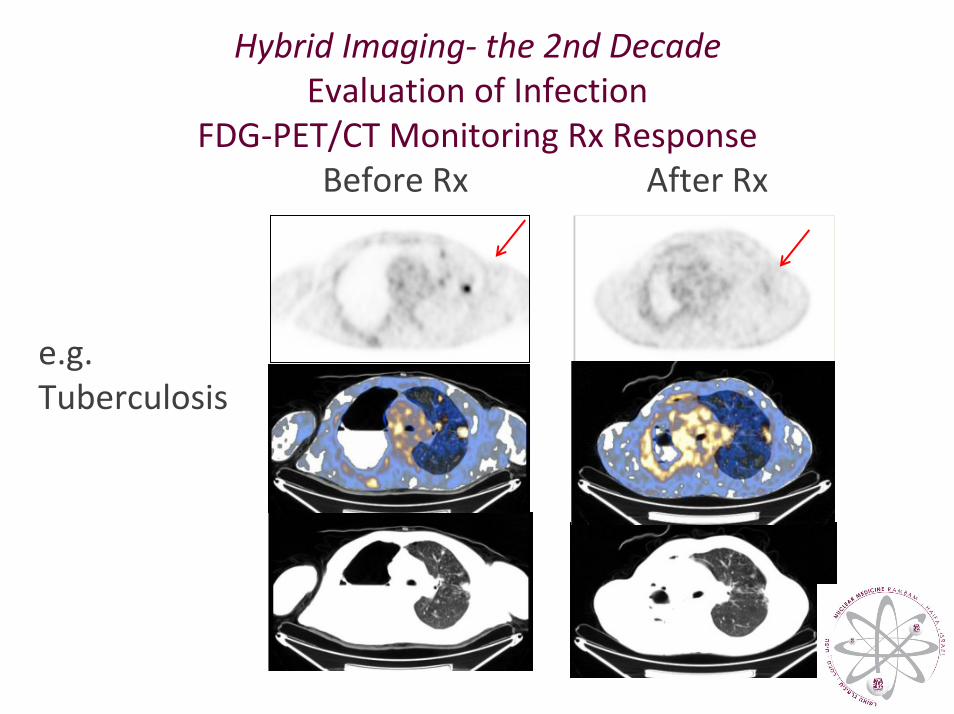
Hybrid Imaging‐ the 2nd DecadeEvaluation of Infection
FDG‐PET/CT Monitoring Rx Response Before Rx After Rx
e.g.Tuberculosis
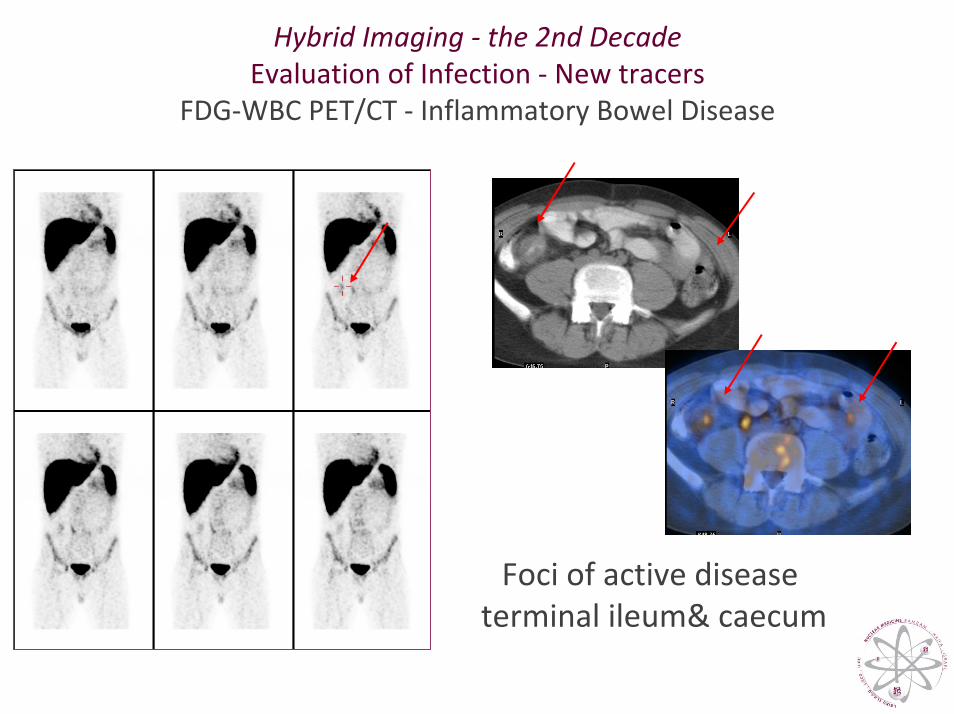
Hybrid Imaging ‐ the 2nd DecadeEvaluation of Infection ‐ New tracers
FDG‐WBC PET/CT ‐ Inflammatory Bowel Disease
Foci of active disease terminal ileum& caecum
Hybrid Imaging ‐ The Simple Principle Improved localization of radiotracer foci
SPECT/PETImproved contrast & resolutionHigher lesion detectability & sensitivity
The SPECT/CT and PET/CT cascade (Adding specificity)
• Precise lesion localization & characterization• Better image interpretation• Higher diagnostic confidence • Accurate diagnosis (localization & extent of disease)• Improved clinical decision making
The Simple Principle ‐ A Big Difference
New (Expensive) Technologies
• Can save healthcare cost if they have a higher diagnostic accuracy
• Most expensive aspect of disease management is the treatment rather than diagnosis
• More accurate diagnosis results in more appropriate and less expensive treatment
“Elements of Danger – The Case of Medical Imaging”
Lauer MS, NEJM August 27, 2009
“We must approach imaging with … humility”
• Only with a strong evidence base (large body of data coming from well‐powered randomized trials clearly showing net benefit) we should feel comfortable recommending [tests] in spite of the fact that they come with their own elements of danger.
• “We have to think and talk explicitly about the elements of danger in exposing our patients to radiation.”
Thus, the task is not so much to see what no one has seen yet, but to think what nobody has thought yet, about what everybody sees.
Spinoza
Thank you!





























