-
Feature Articles
Hypercapnic acidosis and mortality in acute lung injury*
David A. Kregenow, MD; Gordon D. Rubenfeld, MD; Leonard D.
Hudson, MD; Erik R. Swenson, MD
Hypercapnic acidosis (HA),more commonly referred toas permissive
hypercapnia,has been viewed as an ac-ceptable side effect of
lung-protectiveventilation that can be tolerated in aneffort to
avoid ventilator-associated lunginjury (16). Evidence is growing,
how-ever, that HA has favorable anti-inflam-matory and
antioxidative effects at thesubcellular, cellular, whole organ,
andwhole organism levels in hypoxic and in-flammatory conditions
(715). This hasled to speculation that HA may provideadditional
benefit to patients with a vari-ety of injuries and illnesses
(1618). To
date the only data available on HA inhumans with acute lung
injury (ALI)have been limited to trials of lung-protective
ventilation in which the effectsof HA have not been separated from
theeffects of changes in mechanical ventila-tion.
In 2000, the National Institutes ofHealth Acute Respiratory
Distress Syn-drome (ARDS) Network published thelargest
multiple-center randomized trialof patients with ALI (6). The ARDS
Net-work trial compared 12 vs. 6 mL/kg pre-dicted body weight tidal
volumes anddemonstrated a 9% absolute and a 22%relative reduction
in 28-day mortalityrate through the use of 6 mL/kg predictedbody
weight tidal volumes. Therefore, weused data from the ARDS Network
trial toseparate the effect of HA from lung-protective ventilation
in patients withALI.
MATERIALS AND METHODS
Study Design. Secondary analysis of ran-domized clinical trial
data.
Patients and Variables. The details of theinclusion and
exclusion criteria for the ARDSNetwork clinical trial on which this
analysis isbased have been published elsewhere (6). Pa-
tients were enrolled from March 1996 toMarch 1999 at ten
university centers. The en-rolled patients met the
American-EuropeanConsensus definition of ALI and ARDS includ-ing
acute hypoxic respiratory failure requiringmechanical ventilation,
bilateral patchy infil-trates on chest radiograph, and no evidence
ofleft atrial hypertension. The ARDS Networktrial compared
mechanical ventilation usingvolume-cycled assist control with a
tidal vol-ume of 12 mL/kg predicted body weight vs. 6mL/kg
predicted body weight. Hypercapniawas not a goal of the ventilator
strategy in thisstudy and was not a randomized intervention.Minute
ventilation was used to keep 7.30 arterial pH 7.45. At a maximum
respiratoryrate of 35 and pH 7.15, management ofacidosis with
sodium bicarbonate was at thediscretion of the investigator.
The ARDS Network and the Human Sub-jects Divisions of the
University of Washingtonand the VA Puget Sound Health Care
Systemapproved this study. Unless stated otherwise,mortality refers
to 28-day mortality rate andtidal volume in mL/kg refers to mL/kg
pre-dicted body weight as calculated in the parentclinical trial.
Partial pressures of oxygen werecorrected for altitude as in the
parent clinicaltrial.
Based on the experimental evidence (1921), we examined an early
(or acute) HA alongwith other data available early in a
patientscourse of treatment. We defined HA based on
*See also p. 229.From the Division of Pulmonary and Critical
Care
Medicine, Department of Medicine, University of Wash-ington,
Seattle, WA (DAK, GDR, LDH, ERS); and theSection of Pulmonary and
Critical Care, Department ofMedicine, Virginia Mason Medical
Center, Seattle, WA(DAK).
Supported, in part, by grants 5 T32 HL07287-24,1 F32
HL070510-01, NIH HL 24163, and ARDS NetContract No. NO1
HR46055.
None of the authors has any financial interests todisclose.
Copyright 2005 by the Society of Critical CareMedicine and
Lippincott Williams & Wilkins
DOI: 10.1097/01.CCM.0000194533.75481.03
Objective: We tested the hypothesis that hypercapnic acidosisis
associated with reduced mortality rate in patients with acutelung
injury independent of changes in mechanical ventilation.
Design: Secondary analysis of randomized clinical trial
datausing hypothesis-driven multivariate logistic regression.
Setting: Randomized, multiple-center trial (n 861) compar-ing 12
mL/kg to 6 mL/kg predicted body weight tidal volumespreviously
published by the National Institutes of Health AcuteRespiratory
Distress Syndrome (ARDS) Network.
Patients: Acute lung injury patients enrolled in a
randomized,multiple-center trial (n 861).
Interventions: None.Measurements and Main Results: The adjusted
odds ratio and
95% confidence intervals (CI) for 28-day mortality rate
associatedwith hypercapnic acidosis defined as day 1 pH 45 mm Hg
were 0.14 (95% CI 0.030.70, p .016) in the 12mL/kg predicted body
weight tidal volume group and 1.18 (95% CI0.592.35, p .639) in the
6 mL/kg predicted body weight tidal
volume group. Other definitions of hypercapnic acidosis
spanninga range of magnitudes suggest a dose-response
associationbetween hypercapnic acidosis and 28-day mortality in the
12mL/kg predicted body weight tidal volume group. None of
ourdefinitions of hypercapnic acidosis were associated with
reduc-tion in 28-day mortality in the 6 mL/kg predicted body weight
tidalvolume group.
Conclusions: Hypercapnic acidosis was associated with re-duced
28-day mortality in the 12 mL/kg predicted body weighttidal volume
group after controlling for comorbidities and severityof lung
injury. These results are consistent with a protective effectof
hypercapnic acidosis against ventilator-associated lung injurythat
was not found when the further ongoing injury was reducedby 6 mL/kg
predicted body weight tidal volumes. (Crit Care Med2006; 34:17)
KEY WORDS: hypercapnia; acidosis; respiratory; respiratory
dis-tress syndrome; adult; respiration; artificial;
hypoventilation; mor-tality
1Crit Care Med 2006 Vol. 34, No. 1
-
arterial blood gas data collected on the morn-ing following
randomization and institution ofmechanical ventilation according to
the studyprotocol (day 1). Although they reflect a singlepoint in
time, day 1 data have the advantage ofbeing the most complete set
of blood gas val-ues and avoid the survival bias of requiringserial
measurements to define HA. The datacollection protocol provided day
1 blood gasvalues from 7 hrs to as much as 31 hrs afterinstitution
of protocolized mechanical venti-lation. The day 1 blood gas values
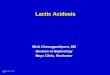
and defini-tions of HA and respiratory alkalosis areshown in Figure
1. Because there is no con-sensus definition of therapeutic HA, our
anal-ysis plan included assessing the effect of dif-ferent degrees
of HA. These were defined apriori. HA1 was defined as a pH 7.40
andPaCO2 40 mm to assess the effect of anydegree of HA. HA2 was
defined as a pH 7.35and PaCO2 45 mm Hg to exclude patientswhose
blood gas values would otherwise havebeen considered within normal
limits and toassess a more severe degree of HA. There weretoo few
patients with greater extremes of re-spiratory acidosis (e.g., pH
7.30 and PaCO250 mm Hg) to perform reliable analyses.
Finally, we hypothesized a priori that ex-tremes of acidosis,
even if associated with el-evated PaCO2, would indicate significant
met-abolic acidosis, comorbidities, and/or probableinevitable
irreversibility of the underlying dis-ease. These patients would
likely have suchoverwhelming cellular dysfunction that HAwould not
afford protection (10) or would bepoorly tolerated. Furthermore,
patients with apH 7.15 may have been given sodium bicar-bonate as
part of the trial at the discretion ofthe providers, but this
information was notrecorded. Thus, a third definition of HA
(HA3)with a lower limit of pH and upper limit ofPaCO2 consistent
with a simple but moderatelysevere acute respiratory acidosis was
examined(7.15 pH 7.35 and 45 mm Hg PaCO2 65 mm Hg). Respiratory
alkalosis was definedas pH 7.45 and PaCO2 35 mm Hg. Again,there
were too few patients with more extremerespiratory alkalosis (e.g.,
pH7.50 and PaCO230 mm Hg) to perform reliable
multivariateanalysis.
Since no direct measure of a metabolicacidosis was recorded for
the majority of pa-tients on day 1, arterial HCO3
values werecalculated from the arterial pH and PaCO2 val-
ues based on the Henderson-Hasselbalchequation. Calculated
arterial HCO3
valueswere compared with measured venous HCO3
values in those patients with serum chemis-tries recorded on day
1 using the method ofBland and Altman (22). Base excess was
thencalculated according to the formula base ex-cess (HCO3
10 [pH 7.40]) 24.Statistical Methods and Modeling Strat-
egy. The primary research question was toassess the independent
effect of HA on mor-tality rate. Because HA was not a
randomizedintervention, patients who achieved HA mightdiffer in
many ways from those who did notachieve HA. To account for these
factors andassess the independent effect of HA, we per-formed
hypothesis-driven multivariate logisticregression including
confounding variablesassociated with both HA and mortality. To
dothis we built a logistic regression model ac-counting for the
patients severity of illnessand the severity of his or her ALI and
analyzedeach tidal volume group separately. We usedAcute Physiology
and Chronic Health Evalua-tion (APACHE) III, a validated intensive
careunit severity of illness measure, to measurethe severity of
critical illness and account forage and comorbid illness (23). We
used pri-mary risk factor for ALI, a known predictor ofoutcome in
this patient population, to accountfor different mechanisms of ALI.
We used day1 PaO2/FIO2 and plateau pressure (Pplat) tomeasure the
severity of ALI. Bivariate analysesof these latter variables
confirmed that theywere related similarly to mortality and HA
anddid not identify other important confounders.The final logistic
regression model predictedmortality as a function of APACHE III
score,risk factor for ALI, PaO2/FIO2, and Pplat. Toanswer the
research question, we added thedifferent definitions of HA as a
binary covari-ate to this model.
Several secondary analyses were per-formed. To assess the effect
of gender, tidalvolume, and positive end-expiratory pressure(PEEP)
on day 1, these variables were added tothe final model separately
and together. Con-founding by metabolic acidosis was examinedby
adding base excess to the model to deter-mine whether metabolic
acidosis affected theassociation between HA and mortality. To
con-firm the finding that HA acts differently de-pending on whether
patients received lung-protective ventilation, we tested an
additionalmodel that included all patients plus tidal vol-ume
randomization and an interaction termbetween HA and tidal
volume.
Statistical analyses were performed usingSTATA version 7.0
(Stata Corporation, CollegeStation TX). Results are reported as
mean SD unless otherwise indicated. Where indicatedin the tables,
continuous variables were com-pared with the two-sample Students
t-testwith equal variances, and categorical variableswere compared
with the Pearson chi-squaretest for independence.
Figure 1. Day 1 pH and PaCO2 values of the study population. HA,
hypercapnic acidosis; RA, respiratoryalkalosis; PBW, predicted body
weight.
2 Crit Care Med 2006 Vol. 34, No. 1
-
RESULTS
A total of 861 patients were studied inthe parent clinical
trial; 141 were ex-cluded due to missing arterial blood gason day
1, and 16 were excluded due tomissing data in other variables. The
de-mographics of the study population areshown in Table 1 and of
the excludedpatients in Table 2. Patients excluded dueto missing
data had lower mortality rateand statistically significantly lower
Pplat,FIO2, and, in the 6 mL/kg tidal volumegroup, lower PEEP
compared with thepatients included in the analysis. The re-maining
patients in each tidal volumegroup were characterized as
hypercapnicor nonhypercapnic based on the defini-tions of HA as
described. The character-istics of these four groups for HA1
areshown in Table 3. Similar data for HA2and HA3 are shown in
Tables 4 and 5,respectively. Patients from each of theten ARDS
Network centers were repre-sented in the 12 mL/kg HA1 group.
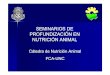
The results of the logistic regressionmodels for each tidal
volume group andeach definition of HA are shown in Figure2. The
odds ratio (OR) of mortality and95% confidence intervals (CI) of
the 12mL/kg and 6 mL/kg tidal volume groupsbased on the presence of
HA1 were 0.32(CI 0.130.79, p .013) and 1.07 (CI0.611.90, p .808),
respectively. In-
cluding more severe and restrictive defi-nitions of HA in the
model led to loweradjusted ORs in the 12 mL/kg tidal vol-ume group
(Fig. 2). For HA2, the adjustedOR of mortality in the 12 mL/kg
tidalvolume group was 0.14 (CI 0.030.70, p .016). Finally, HA3 was
associated withthe greatest reduction in adjusted OR ofmortality in
the 12 mL/kg tidal volumegroup (OR 0.06, CI 0.010.47, p .008). None
of the adjusted ORs for mor-tality related to HA in the 6 mL/kg
tidalvolume group were 1 or reached statis-tical significance (Fig.
2). Lastly, respira-tory alkalosis was not statistically
signif-icantly associated with mortality in eithertidal volume
group.
The additions of gender, day 1 tidalvolume, and/or PEEP did not
alter theassociation between HA and mortality.For example, the OR
of mortality associ-ated with PEEP in the 12 mL/kg tidalvolume
group with HA2 was 1.09 (95% CI0.951.25, p .229). HCO3
values cal-culated from blood gas data were highlycorrelated
with venous values for those inwhom data were available. (According
tothe method of Bland and Altman, thecalculated arterial HCO3
concentrationswere 0.87 mmol/L lower on average thanthe measured
venous values with an SD of2.14 mmol/L. The venous-arterial
differ-ence and SD are consistent with changes
in HCO3 concentration produced by the
loss of CO2 through the lungs and stan-dard measurement
imprecision, respec-tively.) The addition of base excess to
themodel did not alter the association be-tween HA and mortality.
When combinedinto a single model incorporating bothtidal volume
groups and an interactionbetween tidal volume group and HA1,HA1 and
tidal volume interacted signifi-cantly confirming a different
effect of HA1in the different ventilatory strategies (p.049).
Since excluded patients had a lowermortality than study
patients, we per-formed a conservative analysis assumingthat the
excluded patients did not haveHA and assigning them the average
PaO2/FIO2 of the non-HA patients. This is aconservative analysis
because it wouldtend to exaggerate any harmful effects ofHA and
minimize any protective effects.This did not alter the relationship
be-tween HA and mortality.
DISCUSSION
This study demonstrates that HA isassociated with reduced
mortality in pa-tients receiving 12 mL/kg tidal volumesand is not
associated with an effect onmortality in patients receiving 6
mL/kgtidal volumes in the ARDS Network clin-ical trial. These
results support the hy-pothesis that HA is protective, at least
insome patients, rather than simply a tol-erated side effect in the
management ofpatients with ALI. These findings are con-sistent with
the theory that ventilator-associated lung injury is occurring to
agreater extent in the 12 mL/kg tidal vol-ume group and that HA
mitigates thisinjury. They are also consistent with thetheory that
the lung-protective ventila-tion strategy considerably reduces
thisinjury to the point that a protective effectof HA is not
detectable (20, 21).
The acutely injured lung in the midstof an inflammatory response
has provenrefractory to targeted molecular inter-ventions designed
to reduce inflamma-tion. The only intervention that hasproven
effective in reducing mortality isthe reduction in tidal volume to
6mL/kg vs. 12 mL/kg demonstrated in theARDS Network Trial (6). Our
findings areconsistent with the growing basic scienceevidence
supporting the protective effectsof HA in states of lung injury.
The origi-nal concept of salutary acidosis, the pHparadox, arose
from models of ischemiaand reperfusion. It has been observed
re-
Table 1. Characteristics of the study population (6)
Variable 12 mL/kg 6 mL/kg
No. 429 432Age, years 52 18 51 17Female 0.41 0.40APACHE III
score 84 28 81 28Risk factor for ALI, n (%)
Trauma 37 (8) 54 (12)Sepsis 111 (26) 117 (27)Multiple
transfusions 15 (3) 10 (2)Aspiration 62 (14) 65 (15)Pneumonia 156
(36) 144 (33)Other 48 (11) 42 (10)
Day 1 physiologic valuesMinute ventilation, L/min 12.6 4.6 12.9
3.6Respiratory rate, min1 16 6 28 7Tidal volume, mL/kg 11.8 0.8 6.2
0.9Pplat, cm H2O 33 9 25 7pH 7.41 0.07 7.38 0.08PaCO2, mm Hg 35 8
40 10Base excess, mEq/L 2.1 5.7 1.6 5.4FIO2 0.51 0.18 0.57
0.19PEEP, cm H2O 8.6 3.7 9.6 3.7PaO2, mm Hg 77 19 76 23PaO2/FIO2
176 76 158 73
Mortality rate, % 40 31
APACHE, Acute Physiology and Chronic Health Evaluation; ALI,
acute lung injury; Pplat, plateaupressure; PEEP, positive
end-expiratory pressure.
3Crit Care Med 2006 Vol. 34, No. 1
-
peatedly that cells and organs near deathfrom ischemia and/or
anoxia survive andfunction better if reoxygenated in anacidic
milieu so that the intracellular ac-idosis resolves less abruptly.
This hasbeen demonstrated in the liver, heart,kidney, brain, and
lung (715, 1921).These effects are lost when the HA isbuffered by
NaHCO3 (13, 24, 25). Broc-card et al. (20) reported protection
fromventilator-induced lung injury by HA inisolated perfused rabbit
lungs. Sinclair etal. (21) extended this finding by demon-strating
that HA was protective in an invivo rabbit model of
ventilator-inducedlung injury. Furthermore, Laffey et al.(26) found
that HA with low tidal vol-umes in vivo can protect the lung
injuredby aerosolized endotoxin even when ap-plied after the onset
of the inflammatoryinjury.
There are many potential mechanismsby which HA might reduce lung
injury. Aunifying mechanism stems from the gen-erally suppressive
effects of acidosis onnearly all cellular and molecular pro-cesses
(for review, see Ref. 17). Specificmechanisms that have been
elucidatedinclude reduced tumor necrosis factor-release by alveolar
macrophages (27), re-duced neutrophil-endothelial cell adhe-sion
(28), reduced activity of xanthineoxidase leading to reduced free
radicalgeneration (29), reduced nuclear fac-tor-B (30), reduced
interleukin-8 andfree radical production from activatedneutrophils
(24), and suppression of ni-tric oxide production (31) by
inhibition ofinducible nitric oxide synthase. AlthoughCO2 and
acidosis are known to stimulatesurfactant synthesis and secretion,
Laffeyet al. (32) found no changes in surfactantchemistry with 12%
inspired CO2 in arabbit model of high tidal volume-induced lung
injury. The mechanism bywhich 6 mL/kg tidal volumes are associ-ated
with reduced mortality comparedwith 12 mL/kg is not known. It is
specu-lated that 6 mL/kg tidal volumes produceless local and
systemic inflammation dueto ventilator-associated lung injury.
Thereduced levels of serum interleukin-6found in the patients
ventilated with 6mL/kg tidal volumes in the ARDS Net-work trial
support this idea (5, 6). How-ever, the exact mechanism by which
tidalvolume affects mortality in ALI and themanner in which HA
modifies this rela-tionship can only be speculated on at
thistime.
There are several potential limitationsof evaluating the effects
of HA using a
Table 2. Characteristics of patients lacking day 1 blood gas
data and therefore excluded from theanalysis
Variable
12 mL/kg 6 mL/kg
Included Excluded Included Excluded
No. 369 60 351 81Age, years 52 18 54 17 51 17 52 17Female, % 42
35 40 38APACHE III score 85 28 79 31 82 28 78 17Risk factor for
ALI/ARDS, n (%)
Trauma 31 (8) 6 (10) 41 (12) 13 (16)Sepsis 95 (26) 16 (27) 96
(27) 21 (26)Multiple transfusions 15 (4) 0 (0) 7 (2) 3
(4)Aspiration 52 (14) 10 (17) 50 (14) 15 (19)Pneumonia 134 (36) 22
(37) 124 (35) 20 (25)Other 42 (11) 6 (10) 33 (9) 9 (11)
Day 1 physiologic valuesMinute ventilation, L/min 12.6 4.6 12.2
3.5 12.9 3.6 13.1 3.6Respiratory rate, min1 16 6 17 7 29 7 26
9Tidal volume, mL/kg 11.8 0.8 11.9 0.8 6.2 0.9 6.3 0.6Pplat, cm H2O
33 9 29 6
a 25 7 22 5a
pH 7.41 0.07 7.38 0.08PaCO2, mm Hg 35 8 40 10Base excess, mEq/L
2.1 5.6 1.6 5.4FIO2 0.51 0.18 0.47 0.13 0.57 0.19 0.49 0.14
a
PEEP, cm H2O 9 4 8 3 10 4 8 3a
PaO2, mm Hg 76 19 76 23PaO2/FIO2 175 76 157 73
Mortality rate, % 40 33 32 26
APACHE, Acute Physiology and Chronic Health Evaluation; ALI,
acute lung injury; ARDS, acuterespiratory distress syndrome; Pplat,
plateau pressure; PEEP, positive end-expiratory pressure.
ap .05 compared with patients included in the model.
Table 3. Characteristics of model population by tidal volume and
hypercapnic acidosis
Variable
12 mL/kg 6 mL/kg
No HA1 HA1 No HA1 HA1
No. 332 37 247 104Age, years 52 18 50 20 51 16 49 18Female, % 41
54 41 38APACHE III score 85 27 84 35 82 28 81 27Risk factor for
ALI/ARDS, n (%)
Trauma 27 (8) 4 (11) 24 (10) 17 (16)Sepsis 83 (25) 12 (32) 71
(29) 25 (24)Multiple transfusions 11 (3) 4 (11) 5 (2) 2
(2)Aspiration 51 (15) 1 (3) 42 (17) 8 (8)Pneumonia 122 (37) 12 (32)
80 (32) 44 (42)Other 38 (11) 4 (11) 25 (10) 8 (8)
Day 1 physiologic valuesMinute ventilation, L/min 12.8 4.7 10.9
3.6a 13.2 3.8 12.3 3.1a
Respiratory rate, min1 16 6 16 7 29 7 30 7Tidal volume, mL/kg
11.9 0.7 11.4 1.5a 6.3 0.9 6.0 0.9a
Pplat, cm H2O 32 8 40 12a 24 6 28 7a
pH 7.42 0.06 7.34 0.08a 7.41 0.07 7.31 0.08a
PaCO2, mm Hg 34 7 48 5a 35 6 51 9a
Base excess, mEq/L 2.3 5.7 0.2 4.4a 2.3 5.4 0.0 4.8a
FIO2 0.50 0.17 0.66 0.20a 0.53 0.17 0.65 0.21a
PEEP, cm H2O 8 3 12 5a 9 3 11 4a
PaO2, mm Hg 77 19 70 15a 77 24 73 17
PaO2/FIO2 181 76 126 53a 168 75 132 63a
Mortality rate, % 41 35 30 35
APACHE, Acute Physiology and Chronic Health Evaluation; ALI,
acute lung injury; ARDS, acuterespiratory distress syndrome; Pplat,
plateau pressure; PEEP, positive end-expiratory pressure; HA1
isdefined as pH 7.40 and PaCO2 40 mm Hg.
ap .05 compared with patients without HA1.
4 Crit Care Med 2006 Vol. 34, No. 1
-
secondary analysis of clinical trial data.These include bias due
to patient selec-tion, center effect, exposure measure-ment, and
unmeasured confounders. It ispossible that excluding patients
enrolledin the trial but lacking day 1 blood gasdata biased the
study results. This couldoccur if excluded patients had HA butdied
before having a blood gas measuredon day 1, or they lacked HA but
had lowermortality rate. Our conservative analysisassigning the
excluded patients withlower mortality to the non-HA group sug-gests
that this bias does not explain ourresults. There was no evidence
of a centereffect as all ARDS Network centers con-tributed HA
patients to this analysis. Ofcourse, it is possible that physicians
whomanage patients with HA also use othertreatments that themselves
are benefi-cial. This seems unlikely given that pa-tients were
cared for by many physiciansat multiple levels of training in a
multi-ple-center study. In the ARDS Networkstudy analyzed here, the
magnitude andrange of HA were limited (Fig. 1) whencompared with
greater hypercapnia em-ployed in animal studies in which
protec-tion was afforded by HA even with 57mL/kg tidal volumes
(26). We based ourexposure measure of HA on a single arte-rial
blood gas on day 1. We consideredassessing sustained HA as an
exposure;however, there were only three patientswith sustained HA
defined as pH 7.35and PaCO245 mm Hg on days 1 and 3 inthe 12 mL/kg
tidal volume group. Thiswas insufficient to perform reliable
mul-tivariate logistic regression. The exposuremeasure we used has
the potential toinclude patients with only transient HA
Table 4. Characteristics of model population by tidal volume and
hypercapnic acidosis (HA)2
Variable
12 mL/kg 6 mL/kg
No HA2 HA2 No HA2 HA2
No. 356 13 298 53Age, yrs 52 18 44 17 52 17 46 16a
Female, % 41 69 40 45APACHE III score 85 27 91 47 82 28 81
27Risk factor for ALI/ARDS
Trauma 29 (8) 2 (15) 35 (12) 6 (11)Sepsis 89 (25) 6 (46) 85 (29)
11 (21)Multiple transfusions 14 (4) 1 (8) 6 (2) 1 (2)Aspiration 52
(15) 0 (0) 44 (15) 6 (11)Pneumonia 130 (37) 4 (31) 98 (33) 26
(49)Other 42 (12) 0 (0) 30 (10) 3 (6)
Day 1 physiologic valuesMinute ventilation, L/min 12.6 4.6 12.1
4.5 13.0 3.7 12.2 2.7Respiratory rate, min1 16 6 20 10a 29 7 32
6a
Tidal volume, mL/kg 11.8 0.8 10.8 2.0a 6.3 0.9 5.9 0.9a
Pplat, cm H2O 32 8 47 15a 24 6 29 6a
pH 7.42 0.06 7.27 0.10a 7.40 0.07 7.28 0.09a
PaCO2, mm Hg 34 7 52 5a 37 7 56 10a
Base excess, mEq/L 2.1 5.7 1.5 6.0 2.0 5.3 0.4 5.5a
FIO2 0.50 0.17 0.75 0.21a 0.55 0.18 0.69 0.20a
PEEP, cm H2O 8 3 14 6a 9 4 12 4a
PaO2, mm Hg 77 19 63 13a 77 23 71 15
PaO2/FIO2 178 75 100 38a 164 75 119 51a
Mortality rate, % 40 31 31 38
APACHE, Acute Physiology and Chronic Health Evaluation; ALI,
acute lung injury; ARDS, acuterespiratory distress syndrome; Pplat,
plateau pressure; PEEP, positive end-expiratory pressure; HA2
isdefined as pH 7.35 and PaCO2 45 mm Hg.
ap .05 compared with patients without HA2.
Table 5. Characteristics of model population by tidal volume and
hypercapnic acidosis (HA)3
Variable
12 mL/kg 6 mL/kg
No HA3 HA3 No HA3 HA3
No. 358 11 306 45Age, years 52 18 44 18 51 17 45 16a
Female, % 41 82a 39 44APACHE 85 27 82 52 82 29 78 24Risk factor
for ALI/ARDS, n (%)
Trauma 29 (8) 2 (18) 35 (11) 6 (13)Sepsis 91 (25) 4 (36) 86 (28)
10 (22)Multiple transfusions 14 (4) 1 (9) 6 (2) 1 (2)Aspiration 52
(15) 0 (0) 45 (15) 5 (11)Pneumonia 130 (36) 4 (36) 104 (34) 20
(44)Other 42 (12) 0 (0) 30 (10) 3 (7)
Day 1 physiologic valuesMinute ventilation, L/min 12.7 4.6 10.7
3.1 13.0 3.7 12.1 2.8Respiratory rate, min1 16 6 17 8 29 7 31
7a
Tidal volume, mL/kg 11.8 0.8 10.7 3.1 6.2 0.9 5.9 0.8a
Pplat, cm H2O 32 8 44 14a 25 7 28 6a
pH 7.42 0.07 7.31 0.04a 7.39 0.08 7.30 0.05a
PaCO2, mm Hg 35 8 51 6a 38 9 53 5a
Base excess, mEq/L 2.2 5.7 0.4 4.1 1.9 5.6 0.2 3.6a
FIO2 0.51 0.17 0.71 0.20a 0.55 0.19 0.66 0.19a
PEEP, cm H2O 8 3 13 6a 9 4 11 3a
PaO2, mm Hg 77 19 62 13a 77 23 72 16
PaO2/FIO2 178 75 103 40a 162 75 125 52a
Mortality rate, % 41 18 31 33
APACHE, Acute Physiology and Chronic Health Evaluation; ALI,
acute lung injury; ARDS, acuterespiratory distress syndrome; Pplat,
plateau pressure; PEEP, positive end-expiratory pressure; HA3
isdefined as 7.15 pH 7.35 and 45 mm Hg PaCO2 65 mm Hg.
ap .05 compared with patients without HA3.
Figure 2. Adjusted odds ratios for mortality. OR,odds ratio; CI,
confidence interval; *predictedbody weight. Adjusted for Acute
Physiology andChronic Health Evaluation III score, risk factorfor
acute lung injury, day 1 PaO2/FIO2, and Pplat.
5Crit Care Med 2006 Vol. 34, No. 1
-
while also excluding patients who tran-siently failed to meet
these criteria. Nev-ertheless, the finding that HA on day 1 inthe
12 mL/kg arm of the study was asso-ciated with better survival and
the evi-dence of increasing effect with increasingdegrees of HA
suggests that some protec-tion by HA is afforded early in the
courseof ALI even if it is not sustained. Furthersupport for a
protective effect of even ashort duration of HA is evident in
manyanimal studies, where a benefit from ac-idosis accrues in only
several hours (1322, 24, 2632). Unmeasured confoundingvariables are
a universal problem withmultivariate analyses of cohort studies.We
did not have data on the use of so-dium bicarbonate, accurate
estimates ofCO2 production, or deadspace ventilation.Since there
were limitations in the toler-able limits of low pH in the ARDS
Net-work trial, our ability to test the hypoth-esis that HA is
beneficial is limited sinceextremes were avoided. If greater
ex-tremes of HA had been allowed in thisstudy, it is possible that
that either morebenefit or more harm may have beendetected. Most
patients do not have apure respiratory acidosis, so some pa-tients
with HA had a combined respira-tory and metabolic acidosis. In
addition,although we treated it as a single entity,patients may
develop HA by differentmechanisms including reduced
minuteventilation, increased CO2 production,increased deadspace
ventilation, and in-creased shunt fraction. Each of thesemechanisms
may have varying degrees ofpathophysiological significance.
Thesevariables need to be considered and quan-tified in future
studies where HA exists inlow tidal volume groups.
Nevertheless,although inability to control for these
confounders is an important limitation ofthis study, we believe
that the likely di-rection of the bias introduced by the lackof
these variables actually strengthensour results. For an unmeasured
variableto account for the observed protectiveeffect of HA, it
would have to be associ-ated with HA and with reduced
mortalityrate. Many common clinical variablesmight be associated
with our definition ofHA, such as increased deadspace (33),CO2
production, shunt fraction, and met-abolic acidosis (23), but these
are all gen-erally associated with increased mortalityrate.
Therefore, failing to account forthese variables biases our
assessment ofthe effect of HA toward harm, strength-ens the
conclusions about a protectiveeffect in patients receiving 12
mL/kg, andraises the possibility that a beneficial ef-fect of HA
was obscured in the 6 mL/kggroup. We considered including
respira-tory rate and minute ventilation in themodel; however,
because of the volumecontrol ventilator protocol used in thetrial,
they were inextricably linked to HAand their effects cannot be
separated.Last, although Hough et al. (34) foundslightly higher
intrinsic PEEP in the 6mL/kg tidal volume group, the small
dif-ference between 6 and 12 mL/kg tidalvolume groups (median 1.3
vs. 0.5 cmH2O) is likely clinically insignificantgiven the lack of
effect on mortality ofhigher PEEP (8 vs. 13 cm H2O) testeddirectly
in patients with ALI (35).
CONCLUSION
This secondary analysis of data fromthe ARDS Network trial of
lower tidalvolume provides evidence in support ofthe theory that HA
exerts a protectiveeffect in ALI. This effect appears to
bemodulated by the ventilatory approach.Because of the study
limitations, it isimportant to appreciate that, althoughthese
clinical observations support a bodyof basic science on the
beneficial effectsof HA, they do not confirm them. Confir-mation
awaits further clinical studies andan appropriately designed
randomizedtrial of HA coupled with lung-protectiveventilation in
patients with ALI. Based onthe data available in this and other
stud-ies, we propose that greater extremes ofHA than those found in
the ARDS Net-work trial of 12 vs. 6 mL/kg tidal volumeswould likely
be needed to measure anyeffect of HA on outcome in ALI
patientsreceiving lung protective ventilation. Theoptimal dose,
duration, and type (lowered
minute ventilation vs. inspired CO2) ofHA remain unanswered by
this analysis.In addition, measurement of variablessuch as
deadspace fraction and CO2 pro-duction will be important in trials
inves-tigating HA in ALI.
REFERENCES
1. Hickling KG, Walsh J, Henderson S, et al:Low mortality rate
in adult respiratory dis-tress syndrome using low- volume,
pressure-limited ventilation with permissive hyper-capnia: A
prospective study. Crit Care Med1994; 22:15681578
2. Amato MB, Barbas CS, Medeiros DM, et al:Beneficial effects of
the open lung ap-proach with low distending pressures inARDS: A
prospective randomized study onmechanical ventilation. Am J Respir
CritCare Med 1995; 152:18351846
3. Gentilello LM, Anardi D, Mock C, et al: Per-missive
hypercapnia in trauma patients.J Trauma 1995; 39:84652
4. Amato MB, Barbas CS, Medeiros DM, et al:Effect of a
protective-ventilation strategy onmortality in the acute
respiratory distresssyndrome. N Engl J Med 1998; 338:347354
5. Ranieri VM, Suter PM, Tortorella C, et al:Effect of
mechanical ventilation on inflam-matory mediators in patients with
acute re-spiratory distress syndrome: A randomizedcontrolled trial.
JAMA 1999; 282:5461
6. Ventilation with lower tidal volumes as com-pared with
traditional tidal volumes for acutelung injury and the acute
respiratory distresssyndrome. The Acute Respiratory
DistressSyndrome Network. N Engl J Med 2000; 342:13011308
7. Kitakaze M, Weisfeldt ML, Marban E: Acido-sis during early
reperfusion prevents myo-cardial stunning in perfused ferret
hearts.J Clin Invest 1988; 82:920927
8. Orchard C, Kentish J: Effects of changes ofpH on the
contractile function of cardiacmuscle. Am J Physiol 1990;
258:C967C981
9. Currin RT, Gores GJ, Thurman RG, et al:Protection by acidotic
pH against anoxic cellkilling in perfused rat liver: evidence for a
pHparadox. FASEB J 1991; 5:207210
10. Nomura F, Aoki M, Forbess JM, et al: Effectsof hypercarbic
acidotic reperfusion on recov-ery of myocardial function after
cardioplegicischemia in neonatal lambs. Circulation1994;
90:1132111327
11. Caldwell-Kenkel JC, Currin RT, Coote A, etal: Reperfusion
injury to endothelial cellsafter cold storage of rat livers:
protection bymildly acidic pH and lack of protection
byantioxidants. Transpl Int 1995; 8:7785
12. Moore TM, Khimenko PL, Taylor AE: Resto-ration of normal pH
triggers ischemia-reperfusion injury in lung by Na/H ex-change
activation. Am J Physiol 1995; 269:H1501H1505
13. Cardenas VJ Jr, Zwischenberger JB, Tao W, etal: Correction
of blood pH attenuates
H ypercapnic aci-dosis was asso-ciated with re-duced 28-day
mortality in
the 12 mL/kg predicted body
weight tidal volume group
after controlling for comor-
bidities and severity of lung
injury.
6 Crit Care Med 2006 Vol. 34, No. 1
-
changes in hemodynamics and organ bloodflow during permissive
hypercapnia. CritCare Med 1996; 25:827834
14. DArmini AM, Lemasters JJ, Egan TM, et al:Effect of perfusion
pH on rat lung viability onnon-heart beating donors. Eur J
Cardiotho-rac Surg 1997; 12:787791
15. Hurtado C, Pierce GN: Inhibition of Na/H
exchange at the beginning of reperfusion iscardioprotective in
isolated, beating adultcardiomyocytes. J Mol Cell Cardiol 2000;
32:18971907
16. Laffey JG, Kavanagh BP: Carbon dioxide andthe critically
illToo little of a good thing?Lancet, 1999; 354:12831286
17. Kregenow DA, Swenson ER: Hypercapnic ac-idosis: Implications
for permissive and ther-apeutic hypercapnia. Eur Respir J 2000;
20:611
18. Swenson ER: Therapeutic hypercapnic acido-sis: Pushing the
envelope. Am J Respir CritCare Med 2004; 169:89
19. Laffey JG, Tanaka M, Engelberts D, et al:Therapeutic
hypercapnia reduces pulmonaryand systemic injury following in vivo
lungreperfusion. Am J Respir Crit Care Med 2000;162:22872294
20. Broccard AF, Hotchkiss JR, Vannay C, et al:Protective
effects of hypercapnic acidosis onventilator-induced lung injury.
Am J RespirCrit Care Med 2001; 164:802806
21. Sinclair SE, Kregenow DA, Lamm WJ, et al:Hypercapnic
acidosis is protective in an in
vivo model of ventilator-induced lung injury.Am J Respir Crit
Care Med 2002; 163:403408
22. Bland JM, Altman DG: Statistical methodsfor assessing
agreement between two meth-ods of clinical measurement. Lancet
1986;1(8476):307310
23. Knaus WA, Wagner DP, Draper EA, et al: TheAPACHE III
prognostic system. Risk predic-tion of hospital mortality for
critically illhospitalized adults. Chest 1991; 100:16191636
24. Coakley RJ, Taggart C, Greene C, et al: Am-bient pCO2
modulates intracellular pH, in-tracellular oxidant generation, and
interleu-kin-8 secretion in human neutrophils.J Leukoc Biol 2002;
71:603610
25. Laffey JG, Engelberts D, Kavanagh BP: Buff-ering hypercapnic
acidosis worsens acutelung injury. Am J Respir Crit Care Med
2000;161:141146
26. Laffey JG, Honan D, Hopkins N, et al: Hyper-capnic acidosis
attenuates endotoxin inducedacute lung injury. Am J Respir Crit
Care Med2004; 169:4656
27. Bidani A, Wang CZ, Saggi SJ, et al: Evidencefor pH
sensitivity of tumor necrosis factor-alpha release by alveolar
macrophages. Lung1998; 176:111121
28. Serrano CV Jr, Fraticelli A, Paniccia R, et al:pH dependence
of neutrophil-endothelial celladhesion and adhesion molecule
expression.Am J Physiol 1996; 271:C962C970
29. Shibata K, Cregg N, Engelberts D, et al: Hy-percapnic
acidosis may attenuate acute lunginjury by inhibition of endogenous
xanthineoxidase. Am J Respir Crit Care Med 1998;158:15781584
30. Takeshita K, Suzuki Y, Nishio K, et al: Hy-percapnic
acidosis attenuates endotoxin-induced nuclear factor-[kappa] B
activation.Am J Respir Cell Mol Biol 2003; 29:124132
31. Adding LC, Agvald P, Persson MG, et al: Reg-ulation of
pulmonary nitric oxide by carbondioxide is intrinsic to the lung.
Acta PhysiolScand 1999; 167:167174
32. Laffey JG, Engelberts D, Duggan M, et al:Carbon dioxide
attenuates pulmonary im-pairment resulting from
hyperventilation.Crit Care Med 2003; 31:26342640
33. Nuckton TJ, Alonso JA, Kallet RH, et al: Pul-monary dead
space fraction as a risk factorfor death in the acute respiratory
distresssyndrome. N Engl J Med 2002; 346:12811286
34. Hough CL, Kallet RH, Ranieri VM, et al:Intrinsic positive
end-expiratory pressure inAcute Respiratory Distress Syndrome
(ARDS)Network subjects. Crit Care Med 2005; 33:527532
35. Brower RG, Lanken PN, MacIntyre N, et al:National Heart,
Lung, and Blood InstituteARDS Clinical Trials Network. Higher
versuslower positive end-expiratory pressures in pa-tients with the
acute respiratory distress syn-drome. N Engl J Med 2004;
351:327336
7Crit Care Med 2006 Vol. 34, No. 1