Embed Size (px)
Citation preview

Klinika anesteziologie, resuscitace a intenzivní medicíny
1. lékařské fakulty UK a Všeobecné fakultní nemocnice v Praze
Adresa: U nemocnice 2; 128 08 Praha 2
www.karim-vfn.cz
Hyperdynamický septický šok není
(absolutní) kontraindikací ECMO
Martin Balík
KARIM 1 LF UK a VFN, Praha

www.karim-vfn.cz
Poruchy srdeční funkce v sepsi a septickém šoku
Low SVR, hypotension Varon J, Marik PE (2008) Irwin and Rippe's intensive care
medicine. In: Irwin RS, Rippe JM (eds). 6th edn. Wolters
Kluwer Health/Lippincott Williams & Wilkins, Philadelphia,
pp 1855-1869
Diastolic and systolic
dysfunction:
- 15 to 60% of patients may
develop cardiomyopathy
Rudiger A, Singer M (2007) Mechanisms of sepsis-
induced cardiac dysfunction. Crit Care Med 35 (6):1599-
1608
Vieillard-Baron A, Caille V, Charron C, Belliard G, Page B,
Jardin F (2008) Actual incidence of global left ventricular
hypokinesia in adult septic shock. Crit Care Med 36
(6):1701-1706
Autonomic dysfunction
- receptor downregulation
Cariou A, Pinsky MR, Monchi M, Laurent I, Vinsonneau C,
Chiche JD, Charpentier J, Dhainaut JF (2008) Is
myocardial adrenergic responsiveness depressed in
human septic shock? Intensive Care Med 34 (5):917-922
Chronotropic dysfunction:
- inadequately high HR
- low HR variability
Annane D, Trabold F, Sharshar T, Jarrin I, Blanc AS,
Raphael JC, Gajdos P (1999) Inappropriate sympathetic
activation at onset of septic shock: a spectral analysis
approach. Am J Respir Crit Care Med 160 (2):458-465
Schmidt HB, Werdan K, Muller-Werdan U (2001)
Autonomic dysfunction in the ICU patient. Curr Opin Crit
Care 7 (5):314-322
www.karim-vfn.cz
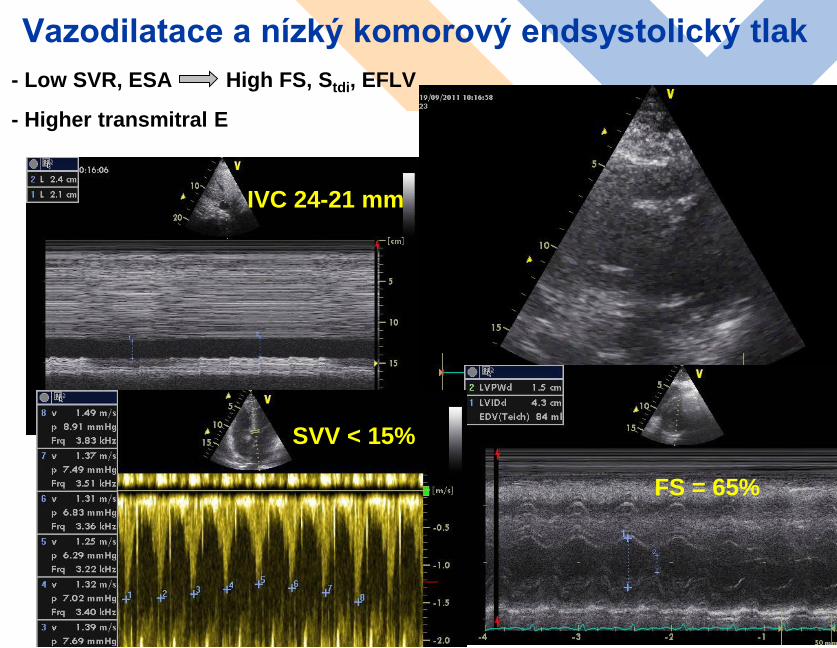
Vazodilatace a nízký komorový endsystolický tlak
- Low SVR, ESA High FS, Stdi, EFLV
- Higher transmitral E
3
FS = 65%
SVV < 15%
IVC 24-21 mm
www.karim-vfn.cz
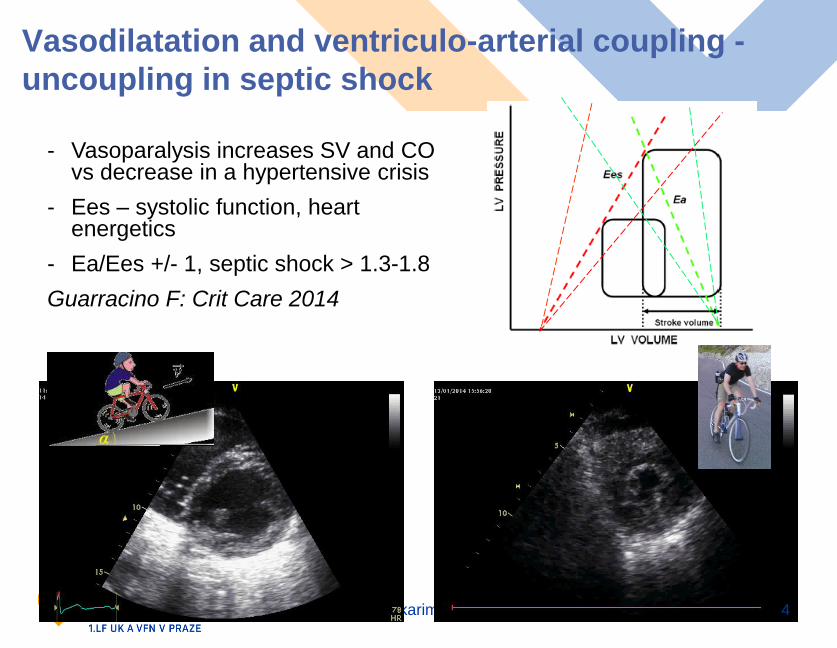
Vasodilatation and ventriculo-arterial coupling -
uncoupling in septic shock
4
- Vasoparalysis increases SV and CO vs decrease in a hypertensive crisis
- Ees – systolic function, heartenergetics
- Ea/Ees +/- 1, septic shock > 1.3-1.8
Guarracino F: Crit Care 2014

www.karim-vfn.cz
Impact of vasoparalysis on cardiac function
(…..plus direct effect of sepsis on heart….)
Low SVR maintains lower LVESV and higher LV_EF
Critical decrease of SVR and afterload = possible relation to circulatory failure in non-dilated LV with preserved LV_EF
Dilated LV better maintainSV and CO (Parker M, Ann Intern Med, 1984)
LV size more important(Huang SJ, et al: Critical Care 2013)
5

www.karim-vfn.cz 6

www.karim-vfn.cz
Septic heart
Septic cardiomyopathy 15-60% (Vieillard-Baron A: Crit Care 2013)
VA or VAV-ECMO according to „inadequate cardiac output“ (GUH Prague)
Successful Use of Extra-corporeal Membrane Oxygenation in a Patient with
Streptococcal Sepsis: A Case Report and Review of Literature
Pořízka M.1, Kopecký P.1, Prskavec T.2, Kunstýř J.1., Rulíšek J.1, Balík M.1
Prague Medical Report 2015, 116(1):57-63.

www.karim-vfn.cz
VA-ECMO for septic cardiomyopathy
(hypodynamic septic shock)
Immature
granulocytes

www.karim-vfn.cz
VA-ECMO for profound vasoparalysis ?
(hyperdynamic septic shock)
From hypodynamic to
hyperdynamic septic shock
(+72-96h from drop of SV/CI)
MAP = CO * SVR
Chasing MAP with high CO !
Evidence in children (low BMI)
Adults require high ECMO blood
flows and cannulas up to 51F
(central ECMO with sternotomy)
Adding another peripheral ECMO ?

www.karim-vfn.cz
10Male 24y (BW 75kg), 3month
history of cough, febrile,
dyspneic
Respiratory failure, paO2/FiO2 82,
agressive IPPV, proning
Septic shock with EF_LV 30%, CI 2.1
l/min.m2, NAD 2.2 ug/kg.min, AVP
4 IU/h, lactate 5.6 mmol/l….
What would you do now?

www.karim-vfn.cz
Possible answers (single-best-answer)
1.) left semi-prone position, lung recruitment maneuver
2.) dobutamine or levosimendan
3.) cannulate VA-ECMO
4.) cannulate VV-ECMO and give inotropics (dobutamine….)
11
TTE 6h after admission……..

www.karim-vfn.cz
O2
pump
oxygenator
a. fem.
ivc
Refractory septic shock on VA-ECMO…..+48h….
Harlequin syndrome
CO increases to 6.4 l/min….develops Harlequin syndrome with
6.3 l/min ECMO flow (total CO 12.7 l/min)
What would you do now ?
- Switch from VA
to VA-V ECMO
- CO 6.2 l/min
- ECMO 6.3 l/min
2 of these return
to VJIdx
- total CO 10.5
l/min

www.karim-vfn.cz
Refractory septic shock on VA-ECMO…..+96h
(D6)….critical vasoparalysis- From hypodynamic to hyperdynamic septic shock
- MSSA with Panton-Valentine toxin, ESBL Klebsiella.pn., aspirate PCR +
Mycobacterium tuberculosis
- Restoration of cardiac function, CO 6.5 l/min + VA-V ECMO 4.3 l/min + 2
l/min venous return…..NAD 0.5…1.5….2.1…+AVP 2-4 IU/h…..rising
lactate, already on CRRT + RCA, liver dysfunction, bone marrow
suppression (thrombopenia, no rise in leucocytes….)
13
What would
you do ?
- Axillar VA-ECMO added
(3.5 l/min CO)
- Restoration of perfusion
pressures with total CO
= 14.3 l/min
- MAP = CO x SVR !

www.karim-vfn.cz
Separation of the VV and VA techniques not
feasible
- If admitted to an ICU with only VV
facility, i.e.„only respiratory support“
the patients would have died
- Unified „code ECLS“ !
- Most frequent indications to VA-ECMO
(….VAV, VVA) in „respiratory failure“
- Septic cardiomyopathy
- Myocarditis
- ACP on an aggressive IPPV with
circulatory failure (LCO)
- Septic embolisations (ACP)
- Embolisations of „post-ECMO“ thrombi
(ACP)
14
All provided
informed consent

www.karim-vfn.cz
Závěry pro léčbu septického šoku
- Terapie zdroje + časná identifikace agens
- Problém PRELOAD: používat funkční hemodynamiku,
dynamické parametry, echokardiografii
- Dg. plnicí tlaky (diastologie)
- CO až CCO v kombinaci s echo u pokračující nestability
- Terapie arytmií
- AS cílová < 125/min, opatrně <110/min
- Dekatecholaminizace (AVP…..)
- Konzultace ECMO centra při refrakterním šoku
- Časný záchyt hypodynamické sepse a indikace k EC
podpoře oběhu (VA-ECMO)
- Indikace k podpoře při „neadekvátním CO“
15

www.karim-vfn.cz
Děkuji za pozornost !
Department of Anaesth. and Intensive Care
1St. Medical Faculty of Charles University,
General University Hospital
U nemocnice 2; 128 08, Prague, EU
T: +420 224 962 243
F: +420 224 962 118
www.karim-vfn.cz

























