Embed Size (px)
Citation preview
Hyperlipidemia Update
Alabama ACC Meeting, June 2016
Vera Bittner, MD, MSPH, FACC
Professor of Medicine
Section Head, General Cardiology, Prevention, and Imaging
Medical Director, Cardiac Rehabilitation and CCU
University of Alabama at Birmingham
Disclosures: Vera Bittner, MD, MSPH
UAB Contracts
Sanofi/Regeneron Steering Committee ODYSSEY
Amgen Investigator Pharmacoepidemiology
DalCor National Coordinator DalGene
Astra-Zeneca National Coordinator
Site PI
STRENGTH
ARTEMIS
Bayer Site PI COMPASS
Other
Eli Lilly 2 Advisory Boards
Amgen 1 Advisory Board
Pfizer TNT related manuscripts
PackHealth Review of grant proposal
ABIM CVD Question Writing
Committee
Outline
2013 ACC/AHA Cholesterol Guideline Recap
2016 ACC Consensus Decision Pathway on
Non-Statin Therapy
PCSK9 Inhibitors: The Holy Grail of Lipid Rx?
2013 ACC/AHA Cholesterol Guideline Principles
Treatment strategy based on net benefit
Risk assessment by pooled cohort risk equation– Individualized use of additional risk indicators
Benefit estimate largely based on RCT’s and their patient-level meta-analyses
Four Statin Benefit Groups– ASCVD
– Primary LDL-C≥190 mg/dL (suggesting FH)
– DM, Age 40-75 yo, LDL-C 70-189 mg/dL
– Age 40-75, LDL-C 70-189 mg/dL,10y ASCVD risk ≥7.5%
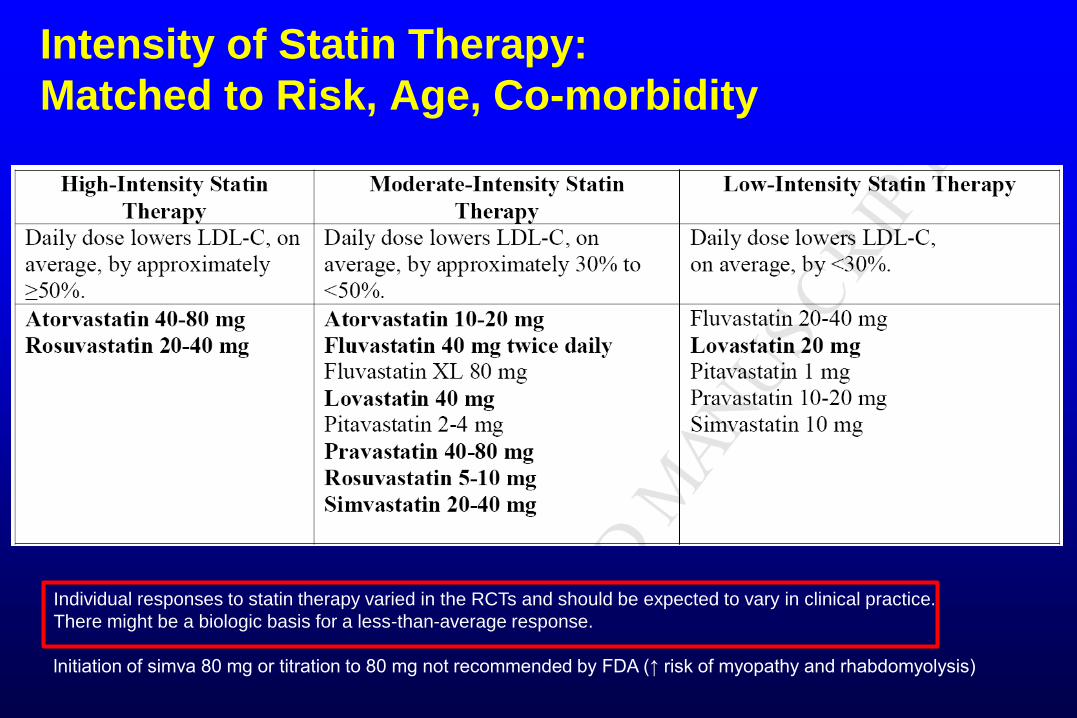
Intensity of Statin Therapy:
Matched to Risk, Age, Co-morbidity
Individual responses to statin therapy varied in the RCTs and should be expected to vary in clinical practice.
There might be a biologic basis for a less-than-average response.
lnitiation of simva 80 mg or titration to 80 mg not recommended by FDA (↑ risk of myopathy and rhabdomyolysis)
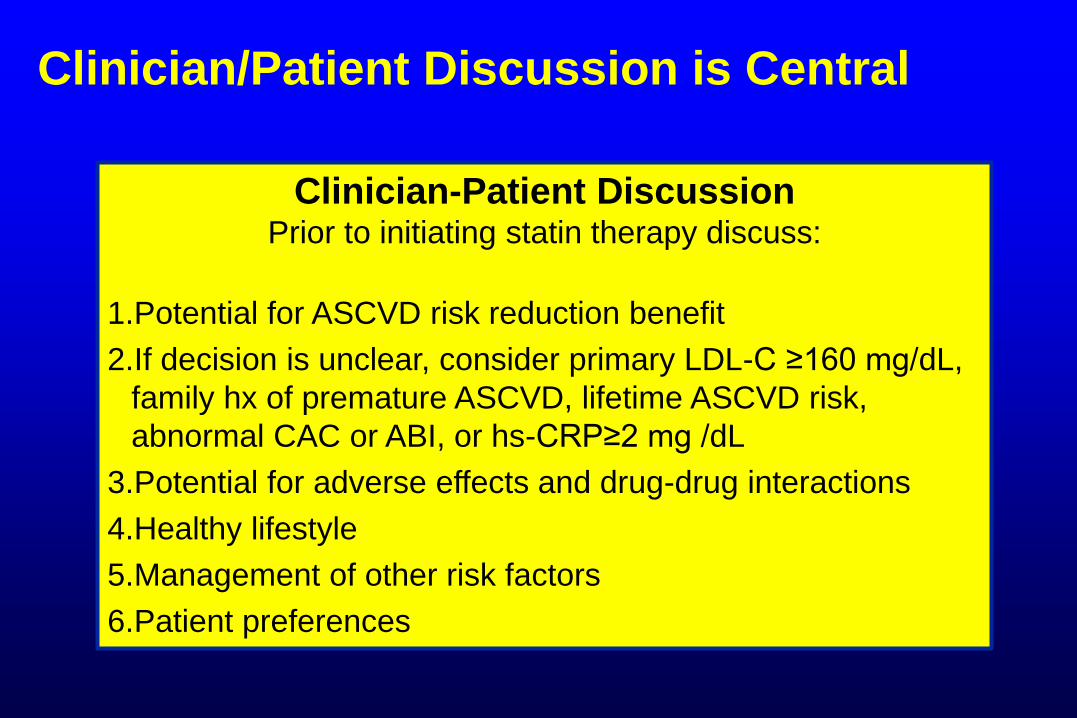
Clinician/Patient Discussion is Central
Clinician-Patient DiscussionPrior to initiating statin therapy discuss:
1.Potential for ASCVD risk reduction benefit
2.If decision is unclear, consider primary LDL-C ≥160 mg/dL,
family hx of premature ASCVD, lifetime ASCVD risk,
abnormal CAC or ABI, or hs-CRP≥2 mg /dL
3.Potential for adverse effects and drug-drug interactions
4.Healthy lifestyle
5.Management of other risk factors
6.Patient preferences
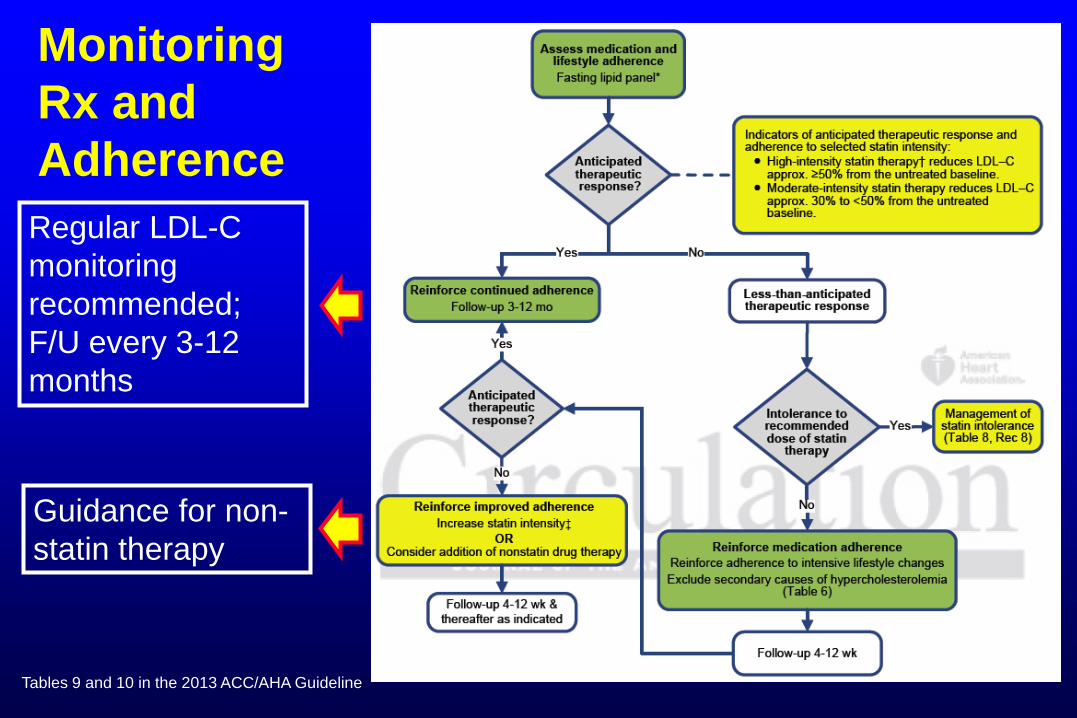
Monitoring
Rx and
Adherence
Guidance for non-
statin therapy
Tables 9 and 10 in the 2013 ACC/AHA Guideline
Regular LDL-C
monitoring
recommended;
F/U every 3-12
months
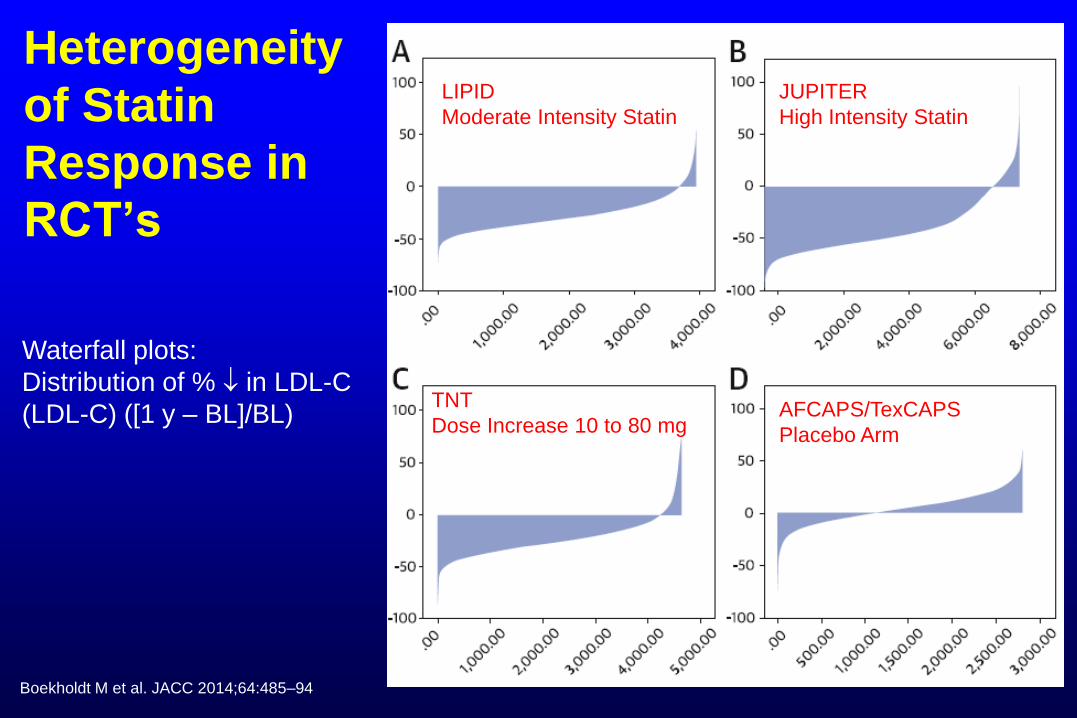
Heterogeneity
of Statin
Response in
RCT’s
JUPITER
High Intensity Statin
LIPID
Moderate Intensity Statin
TNT
Dose Increase 10 to 80 mgAFCAPS/TexCAPS
Placebo Arm
Boekholdt M et al. JACC 2014;64:485–94
Waterfall plots:
Distribution of % in LDL-C
(LDL-C) ([1 y – BL]/BL)
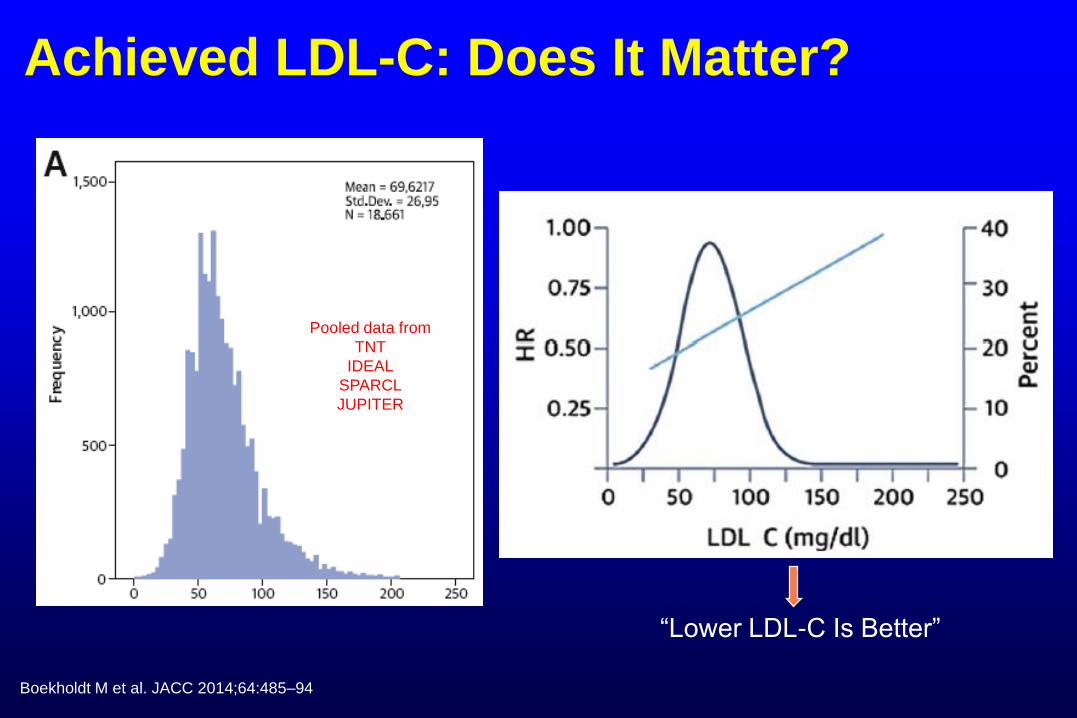
Achieved LDL-C: Does It Matter?
Boekholdt M et al. JACC 2014;64:485–94
Pooled data from
TNT
IDEAL
SPARCL
JUPITER
“Lower LDL-C Is Better”
Alternate Explanations
Lower LDL-C achieved with statins is better
Statin-responsive individuals have better
prognosis
– Differences in lipid metabolism
– Environmental factors
Adherent individuals have better prognosis
– Adherence as a personality trait
– Ability to tolerate high intensity statin
Individuals with lower baseline LDL-C have
better prognosis
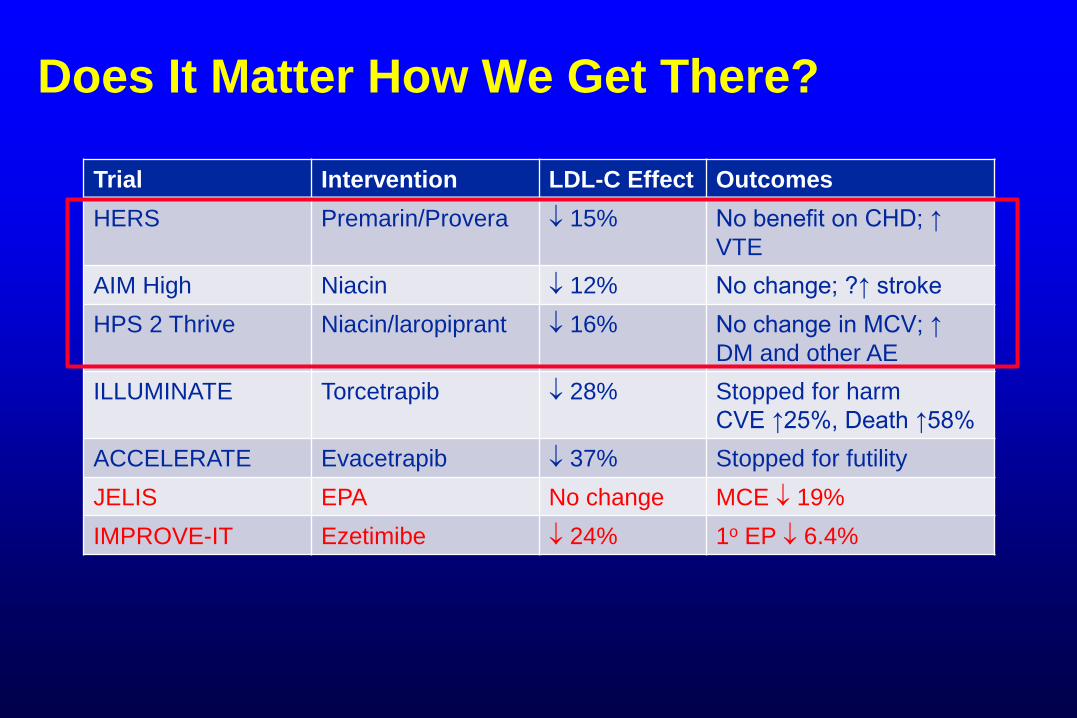
Does It Matter How We Get There?
Trial Intervention LDL-C Effect Outcomes
HERS Premarin/Provera 15% No benefit on CHD; ↑
VTE
AIM High Niacin 12% No change; ?↑ stroke
HPS 2 Thrive Niacin/laropiprant 16% No change in MCV; ↑
DM and other AE
ILLUMINATE Torcetrapib 28% Stopped for harm
CVE ↑25%, Death ↑58%
ACCELERATE Evacetrapib 37% Stopped for futility
JELIS EPA No change MCE 19%
IMPROVE-IT Ezetimibe 24% 1o EP 6.4%
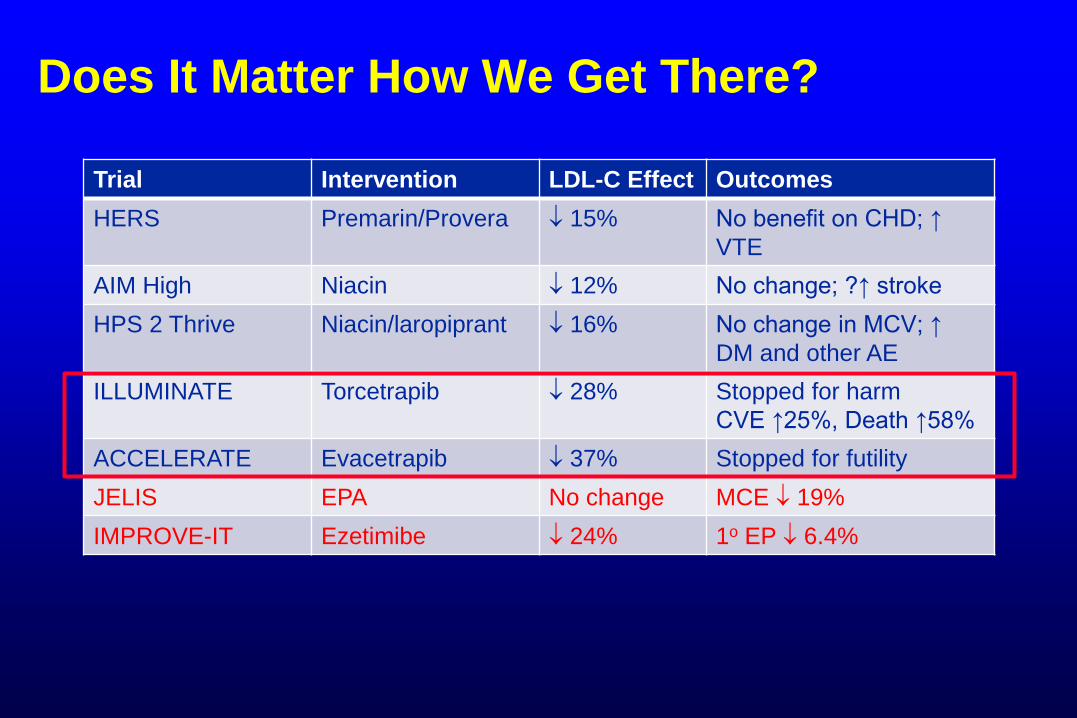
Does It Matter How We Get There?
Trial Intervention LDL-C Effect Outcomes
HERS Premarin/Provera 15% No benefit on CHD; ↑
VTE
AIM High Niacin 12% No change; ?↑ stroke
HPS 2 Thrive Niacin/laropiprant 16% No change in MCV; ↑
DM and other AE
ILLUMINATE Torcetrapib 28% Stopped for harm
CVE ↑25%, Death ↑58%
ACCELERATE Evacetrapib 37% Stopped for futility
JELIS EPA No change MCE 19%
IMPROVE-IT Ezetimibe 24% 1o EP 6.4%

Does It Matter How We Get There?
Trial Intervention LDL-C Effect Outcomes
HERS Premarin/Provera 15% No benefit on CHD; ↑
VTE
AIM High Niacin 12% No change; ?↑ stroke
HPS 2 Thrive Niacin/laropiprant 16% No change in MCV; ↑
DM and other AE
ILLUMINATE Torcetrapib 28% Stopped for harm
CVE ↑25%, Death ↑58%
ACCELERATE Evacetrapib 37% Stopped for futility
JELIS EPA No change MCE 19%
IMPROVE-IT Ezetimibe 24% 1o EP 6.4%

JACC Online April 2016
“Expert Consensus Documents are intended to provide guidance for clinicians
in areas where evidence may be limited, new and evolving, or lack sufficient
data to fully inform clinical decision making.” James L. Januzzi, MD, FACC
Questions for the Consensus Panel
In what patient populations should non-statin therapies be considered?
In what situations should non-statin therapies be considered?– When is the amount of LDL-C lowering (% LDL-C reduction
or LDL-C achieved on Rx) less than anticipated, less than desired, or inadequate?
– Which treatment options should be considered in patients who are truly statin intolerant?
If non-statin therapies are to be added, which agents or therapies should be considered and in what order?
Note: Severe hypertriglyceridemia not addressed!
Patient Groups Under Consideration
ASCVD
Uncomplicated ASCVD on maximally tolerated statin with less than anticipated response
ASCVD with co-morbidities– Diabetes
– ASCVD event within < 3 months
– ASCVD event on statin
– Poorly controlled major ASCVD risk factors
– Elevated Lp(a)
– CKD
ASCVD and 1o LDL-C elevation ≥190 mg/dL
Primary Prevention
Age ≥21, primary LDL-C ≥190
mg/dL
Age 40-75, DM, LDL-C 70-189
mg/dL
Age 40-75, LDL-C 70-189
mg/dL, 10 year risk ≥7.5%
What To Do When Therapeutic Response
Is Less Than Anticipated / Desired?
Re-assessment of lifestyle– Consider referral to registered dietitian
Maximize statin intensity, if not on high intensity therapy
Treat other risk factors
Assessment of statin adherence– Misunderstanding
– Statin related AE
– Drug-drug interactions
– Cost
Manage statin intolerance, if present
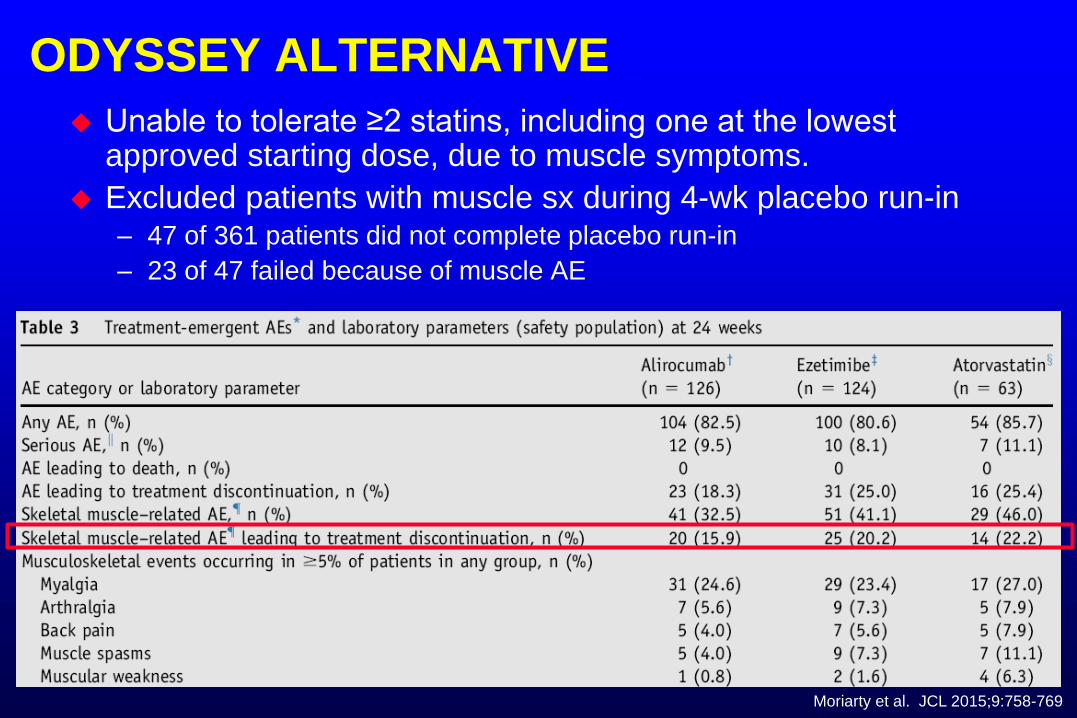
ODYSSEY ALTERNATIVE
Unable to tolerate ≥2 statins, including one at the lowest approved starting dose, due to muscle symptoms.
Excluded patients with muscle sx during 4-wk placebo run-in – 47 of 361 patients did not complete placebo run-in
– 23 of 47 failed because of muscle AE
Moriarty et al. JCL 2015;9:758-769

Don’t Underestimate The Impact of The Media …
Danish population
N=674,900 initiated statins
1995-2010
Statin use increased from <1% to 10%
Discontinuation rate increased from 6 to 18%
Nielsen and Nordestgaard. European Heart Journal (2016) 37, 908–916
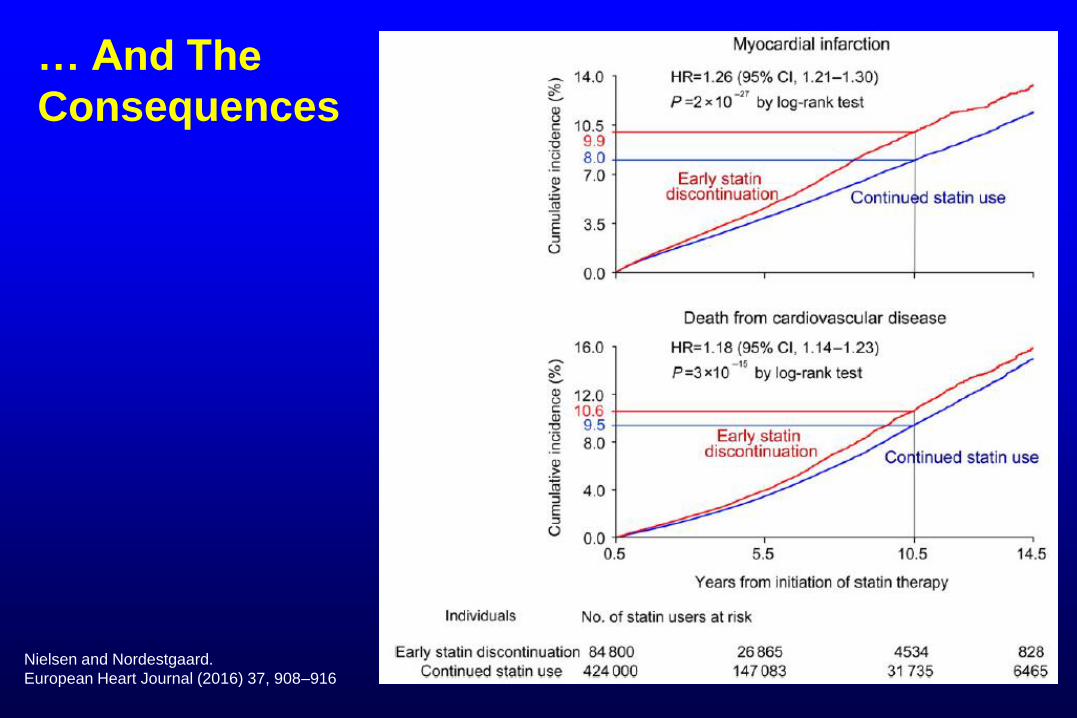
… And The
Consequences
Nielsen and Nordestgaard.
European Heart Journal (2016) 37, 908–916
Statin Intolerance App

What Non-Statins Are Recommended?
Soluble fiber / stanols / sterols
Ezetimibe
Bile acid sequestrants– Use only if TG <300 mg/dL
PCSK9 inhibitors
FH only: Mipomersin / Lomitapide / Apheresis
Niacin NOT RECOMMENDED– “On the basis of currently available evidence of non-efficacy
and potential harms, the Committee judged that there are no clear indications for the routine use of niacin preparations as additional non-statin therapies, and niacin is therefore not recommended for use in any of the clinical situations addressed below.”
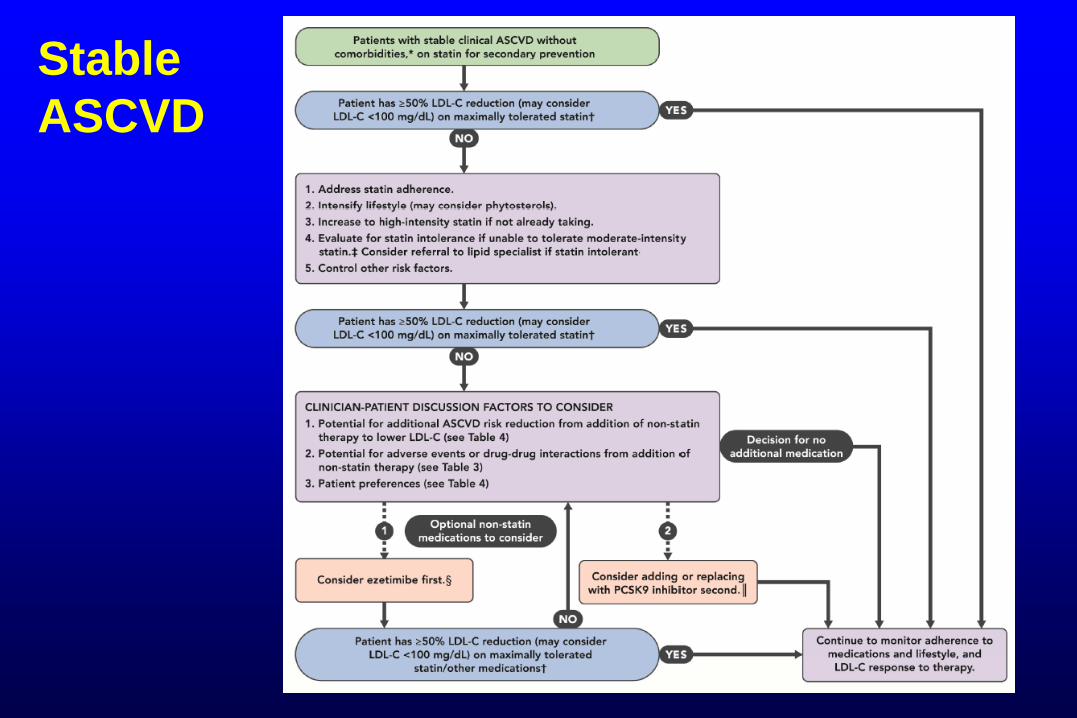
Stable
ASCVD
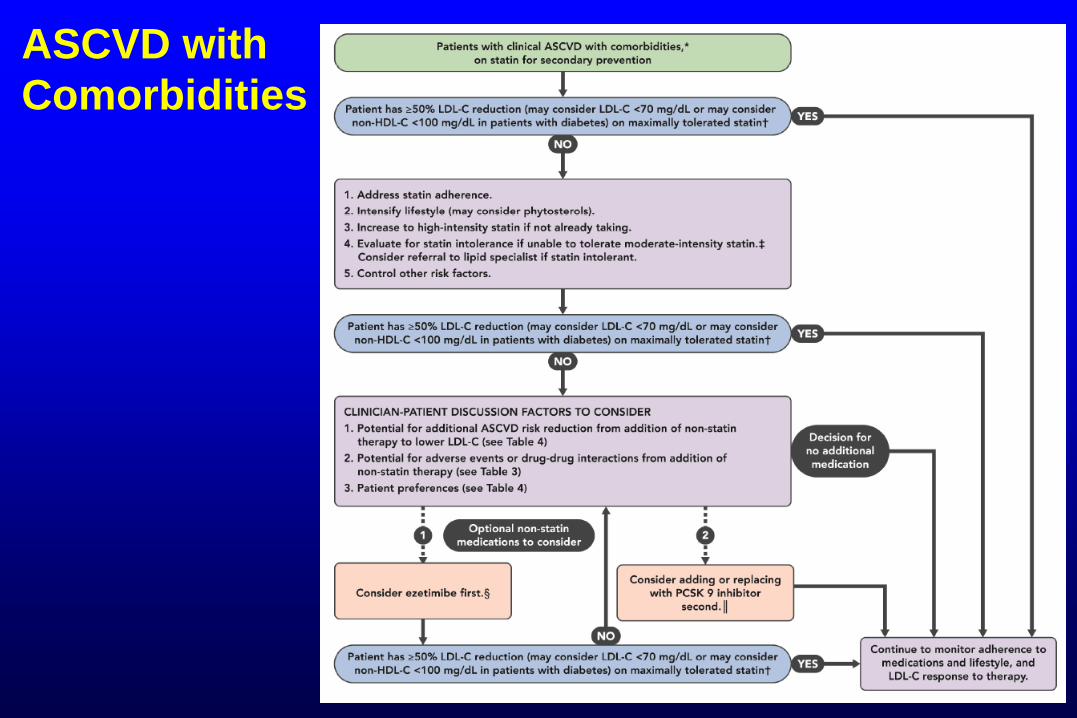
ASCVD with
Comorbidities
Take Home
Statins first, at appropriate intensity
Consider non-statins, if
– Less than desired response to statins
– Statin intolerance
Non-statins under consideration:
– Soluble fiber / stanols / sterols
– Ezetimibe
– Bile acid sequestrants
– PCSK9 inhibitors
PCSK9 Inhibition
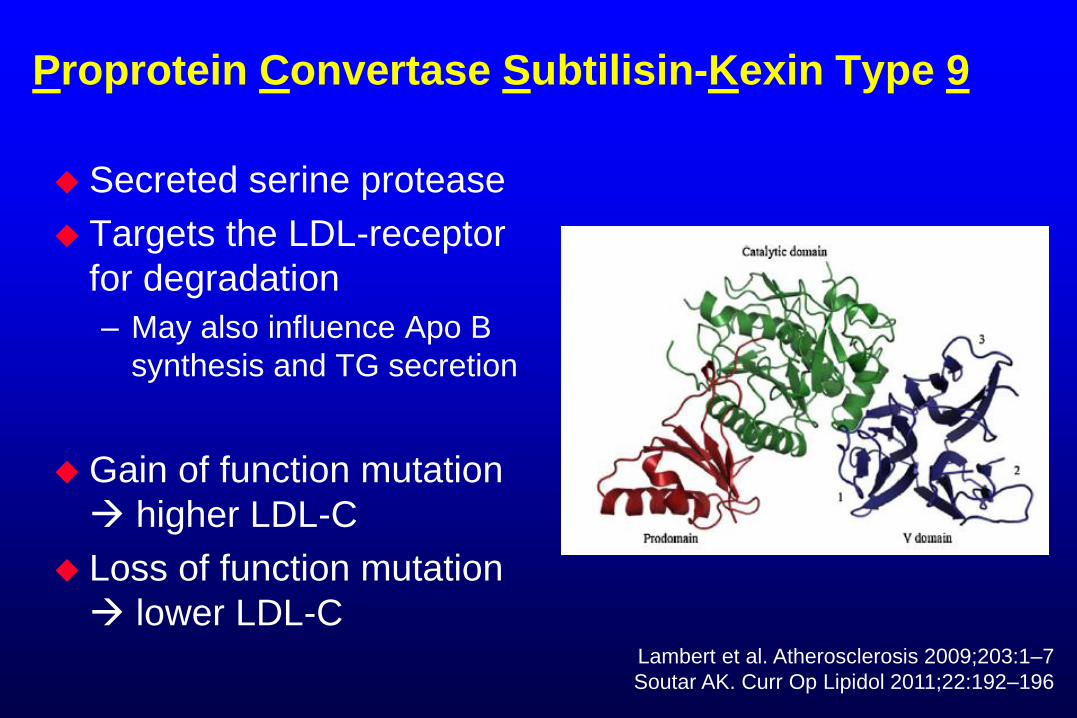
Proprotein Convertase Subtilisin-Kexin Type 9
Secreted serine protease
Targets the LDL-receptor
for degradation
– May also influence Apo B
synthesis and TG secretion
Gain of function mutation
higher LDL-C
Loss of function mutation
lower LDL-CLambert et al. Atherosclerosis 2009;203:1–7
Soutar AK. Curr Op Lipidol 2011;22:192–196
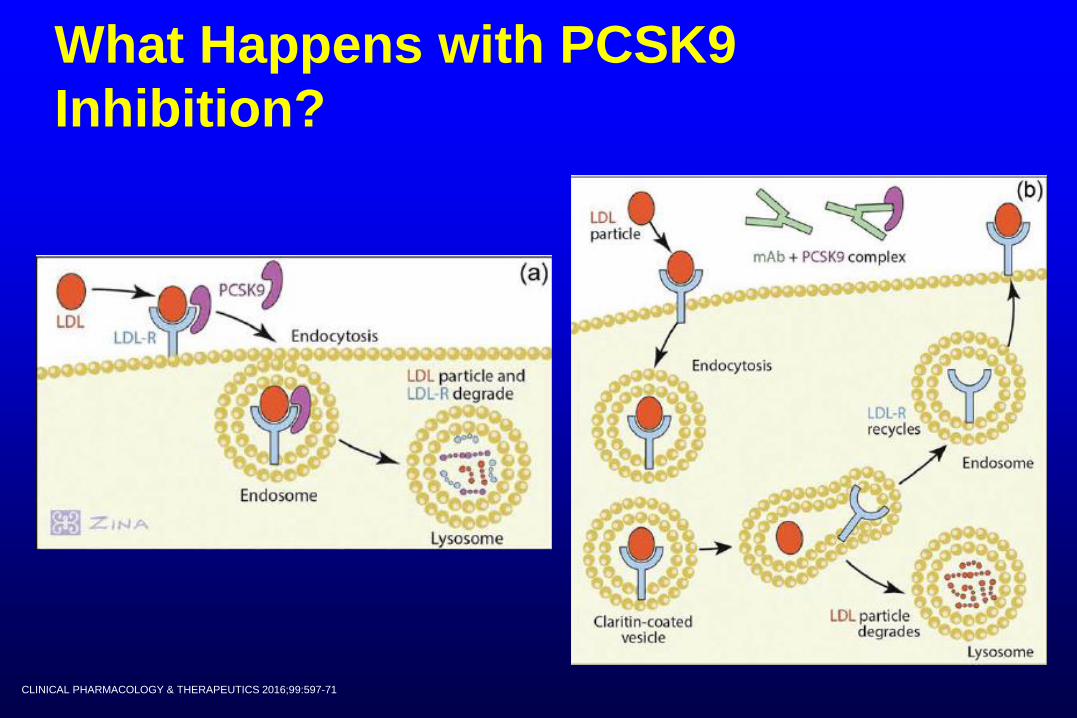
What Happens with PCSK9
Inhibition?
CLINICAL PHARMACOLOGY & THERAPEUTICS 2016;99:597-71
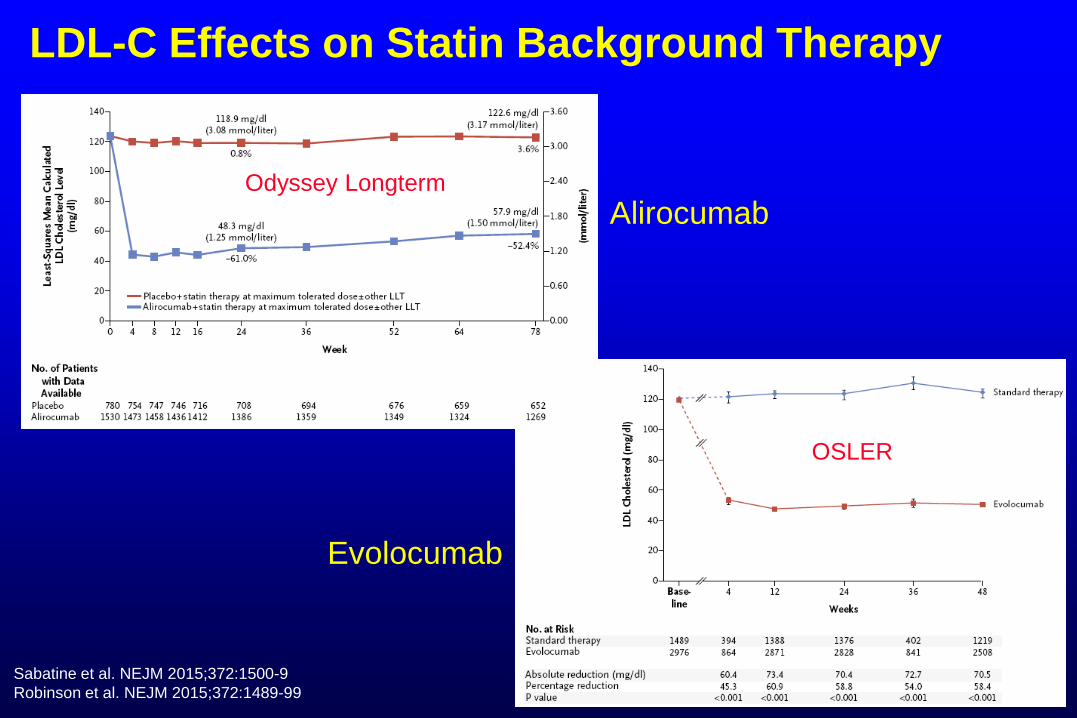
LDL-C Effects on Statin Background Therapy
OSLER
Odyssey Longterm
Sabatine et al. NEJM 2015;372:1500-9
Robinson et al. NEJM 2015;372:1489-99
Alirocumab
Evolocumab
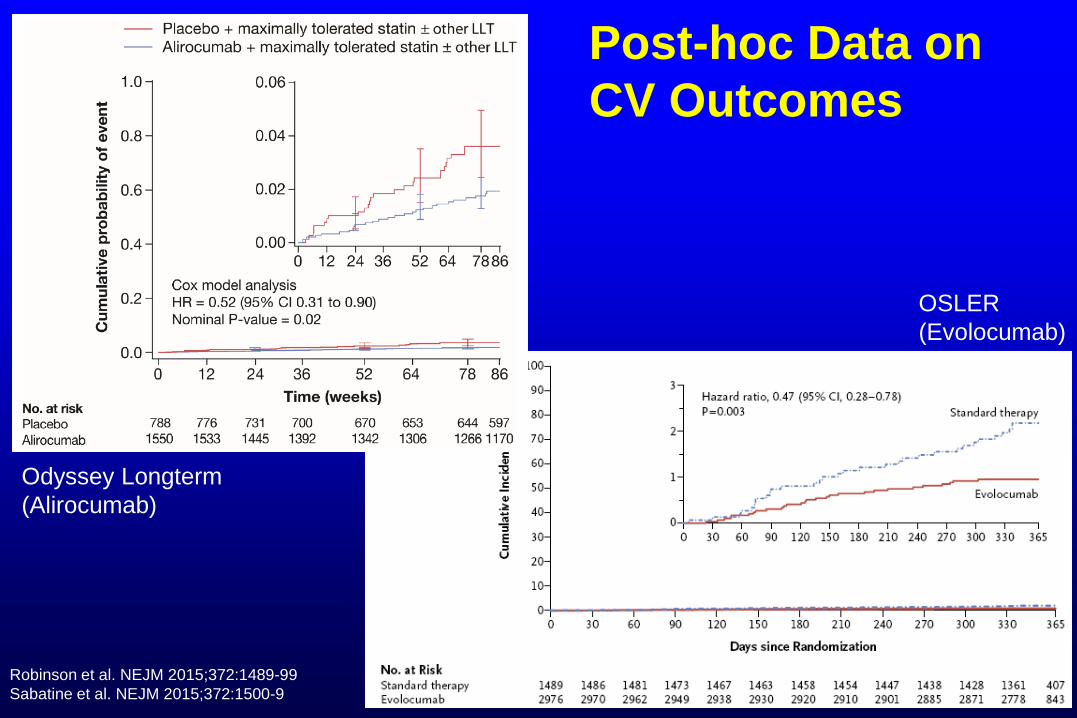
Post-hoc Data on
CV Outcomes
Robinson et al. NEJM 2015;372:1489-99
Sabatine et al. NEJM 2015;372:1500-9
Odyssey Longterm
(Alirocumab)
OSLER
(Evolocumab)
Safety
Alirocumab
– Nasopharyngitis, injection site reactions, influenza
Evolocumab
– Nasopharyngitis, URI, influenza, back pain, and
injection site reactions
Self-reported cognitive AE*
– Alirocumab vs placebo: 1.2% vs 0.5%
– Evolocumab vs placebo: 0.9% vs 0.3%
*Deliria, confusion; cognitive and attention disorders and disturbances; dementia and amnestic conditions; disturbances in thinking and
perception; mental impairment disorders
Percentages quoted in ACC Non-statin Consensus document 2016
FDA Approval
Alirocumab (Praluent)
Adjunct to diet and maximally
tolerated statin to treat adults with
HeFH or clinical ASCVD who need
more LDL-C reduction.
Initiate 75 mg SQ every 2 weeks
May ↑ dose to 150 mg every 2
weeks
Evolocumab (Repatha)
Adjunct to diet and maximally tolerated statin to treat adults with HeFH or clinical ASCVD who need more LDL-C reduction
Adjunct to diet and other LDL-lowering Rx (e.g., statins, ezetimibe, LDL apheresis) in patients with HoFH who need more LDL-C reduction
ClinicL ASCVD or HeFH: 140 mg SQ every 2 weeks or 420 mg SQ monthly
HoFH: give 420 mg SQ monthly (three 140 mg injections within 30 min)
Cost
US
– Evolocumab: about $14,100/year
– Alirocumab: about $14,600/year
– Manufacturer coupons
– Formulary varies by insurance plan
» e.g. CVS Caremark carries only Evolocumab
UK
– Evolocumab: agreed upon list price $5,780/year
– Alirocumab: agreed upon list price $5,780/year
http://www.fiercepharma.com/pharma/nice-gives-tentative-broad-approval-to-both-repatha-praluent; dated 5/6/2016; accessed 5/26/2016
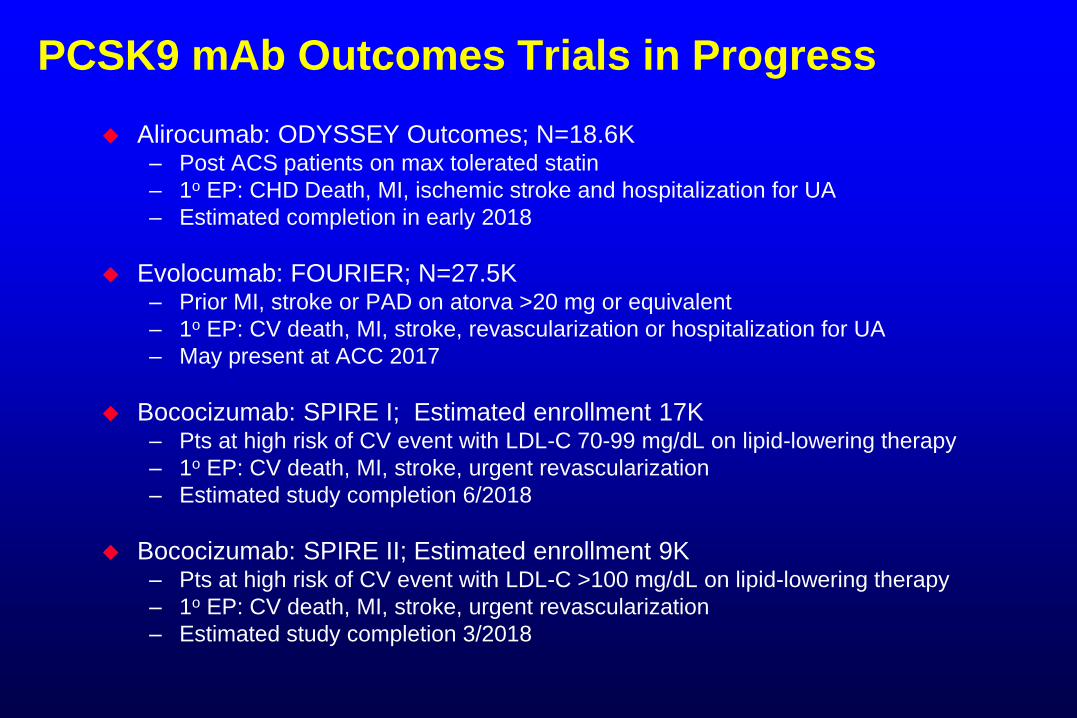
PCSK9 mAb Outcomes Trials in Progress
Alirocumab: ODYSSEY Outcomes; N=18.6K– Post ACS patients on max tolerated statin
– 1o EP: CHD Death, MI, ischemic stroke and hospitalization for UA
– Estimated completion in early 2018
Evolocumab: FOURIER; N=27.5K– Prior MI, stroke or PAD on atorva >20 mg or equivalent
– 1o EP: CV death, MI, stroke, revascularization or hospitalization for UA
– May present at ACC 2017
Bococizumab: SPIRE I; Estimated enrollment 17K– Pts at high risk of CV event with LDL-C 70-99 mg/dL on lipid-lowering therapy
– 1o EP: CV death, MI, stroke, urgent revascularization
– Estimated study completion 6/2018
Bococizumab: SPIRE II; Estimated enrollment 9K– Pts at high risk of CV event with LDL-C >100 mg/dL on lipid-lowering therapy
– 1o EP: CV death, MI, stroke, urgent revascularization
– Estimated study completion 3/2018
Thank You










![Welcome [doclibrary-kccg.cornwall.nhs.uk]doclibrary-kccg.cornwall.nhs.uk/DocumentsLibrary/... · Three project stakeholder groups review. NHS Kernow senior management team review](https://img.pdfslide.net/doc/110x75/5fbfcdf9d7c4497eeb738032/welcome-doclibrary-kccg-doclibrary-kccg-three-project-stakeholder-groups-review.jpg)

















