Embed Size (px)
DESCRIPTION
HYPERTENSION. Presented BY :. Objectives. Identify differential diagnosis of a case presented with the symptoms of lower limb oedema . Differentiate between different etiologies of hypertension. Discuss briefly between stages of hypertension. - PowerPoint PPT Presentation
Citation preview

Presented BY: 1-Mais Al-Joulany
2-Eman Al-Zaidi
3-Roaa al Khalifah
4 -Reham Ghazal5 -Horyah Al-Ismail
6-Ibtihal Al-Drees
7-Abeer Al-Hatim8 -Fatmah Al-Rojaiy
9 -Cady Al-Shammary

•Identify differential diagnosis of a case presented with the symptoms of lower limb oedema.
•Differentiate between different etiologies of hypertension.
•Discuss briefly between stages of hypertension.
•Enumerate and discuss the importance signs& symptoms in patients with hypertension.
•Investigate appropriately apatient with hypertension.
•Advice initial management plan for a patient with hypertension according to recent guidelines (NICE 127).
•Discuss non-drug management of hypertension.•Identify long term complications of hypertension.

A 50-year-old woman presents to your clinic for routine follow-up. She has a history of diabetes mellitus and hypertension for ~
20 years. She mentions that she has noted fatigue and increased swelling in her lower extremities during the past several weeks.
Medications: -Lisinopril 10 mg p.o. q.i.d.
-NPH insulin 20 units s.c. Q. a.m. and 10 units s.c. q. p.m. -Regular insulin 5 units s.c. Q. a.m..

On exam she appears to be in no apparent distress. Her height is153 cm and weight is 100kg .
Blood pressure is 165/98 mmHg, pulse 85/minute and respirations 20/minute .
Fundoscopic exam reveals diabetic retinopathy. There were no visible hemorrhages or papilledema .Cardiac exam was remarkable for an S1, S2 and S4 .Lungs were clear to auscultation and percussion .
Abdomen was obese, non-tender and without masses or bruits. Lower extremities had good pulses with 3+ pitting edema. Neurological exam is remarkable for decreased sensation in a stocking-glove distribution, otherwise intact.

Why Do We Care?

Significant morbidity and mortality
- CAD including MI and CHF
- Stroke
- Chronic kidney disease
Heart disease is still leading cause of death

comprehensive investiga tions for blood pressure assessment in 35 areas of Saudi Arabia.
Applying the criteria of W.H.O. of blood pressure > 160/95 mmHg as hypertensionmeasured systolic and diastolic blood pressure in 14,660 adult Saudis (6,162 males and 8,498 females)
they found prevalence Among the adults (> 18 years), 5.3% had systolic hypertension, while 7.9% had diastolic hypertension.
The majority (>75%) of those with hypertension were 40 years of age or older .In the age group 40-75 years, they found that a higher prevalence of:
-systolic hypertension : Females > Males (15.7%) -diastolic hypertension: Males > Females (8.2%)

Out of 65% of people over age 60 diagnosed with hypertension:
Only 1 in 4 of these individuals are taking adequate medication
Framingham data suggests that individuals who are normotensive at age 55 have a 90% lifetime risk of developing HTN

Acute
Deep vein
Chronic
Venous insufficiency
differential diagnosis of limb edema?
Unilateral Bilateral
Common Causes of Leg Edem

Chronic
Renal disease (nephrotic syndrome, glomerulonephritis
Liver disease
Diuretic-induced edema
Preeclampsia
Anemia
Chronic
Secondary lymphedema
(tumor, radiation, surgery, bacterial infection)
differential diagnosis of limb edema?
Unilateral Bilateral
Less Common Causes of Leg Edem
Acute
Bilateral deep vein thrombosis
Acute worsening of systemic cause
(heart failure, renal disease)

A term used to describe high blood pressure.
Blood pressure is a measurement of the force against the walls of the arteries as the heart pumps
blood through the body.
The risk of morbidity and mortality increases progressively with increasing systolic and diastolic
blood pressure ..

Non- modifiable factors
Advanced age
especially those 60 years
and older
Race
Black people.
Gender-related risk
patterns
Men and postmenopaus
al women
Fetal factor & family history
Babies born with low birth
weight get high BP
Family history of hypertensi
on and CVS
diseases

Modifiable factors
Increase salt intake
causes increase blood volume,
increase cardiac output, increase
peripheral resistance
Increase alcohol
consumption
systolic BP is affected more.
Stress
increase sympathetic
activity
Obesity
lepton hormone derived from
adipose tissue, causes increase
sympathetic activity via
hypothalamus
Smoking


hypertensive crisis: ( BP >180/120 mm Hg ) may be categorized as either
- hypertensive emergency ) e xtreme BP elevation with
(a cute or progressing target organ damage - hypertensive urgency (severe BP elevation without acute
or progressing target organ injury). -Malignant hypertension when diastolic BP more than
130mmHg. Unless treated, it may lead to death due to
renal failure, heart failure or stroke.
-

- BP must be measured correctly
- Feet on floor
- Both arms if elevated
- Cuff bladder must circle at least 80% of the arm
- Arm supported at level of heart
- Back supported - Measure blood pressure in both arms

In clinic: - IF blood pressure ( 140/90 mmHg ) or higher confirm by . ambulatory blood pressure monitoring (ABPM)
> least 2 measurements/ hr during person’s waking hours
> average value of at least 14 measurements taken to confirm HTN
:At homeUse home blood pressure monitoring (HBPM) to confirm a diagnosis of hypertension
> blood pressure is recorded twice daily ( morning/evening )> blood pressure recording continues for at least 4 days, ideally for 7
daysDiscard the measurements taken on the first day and use the average value of all the remaining measurements to confirm a diagnosis of hypertension.

ABPM
HBPM

Postural hypotension
● In people with symptoms of postural hypotension (falls or postural dizziness):
− measure blood pressure with the person either supine or seated
− measure blood pressure again with the person standing for at least 1 minute prior to measurement.
● If the systolic blood pressure falls by 20 mmHg or more when the person is standing:
− review medication− measure subsequent blood pressures with the person
standing − consider referral to specialist care if symptoms of postural
hypotension persist.

1 )Primary (essential) Hypertension:Has no known cause (idiopathic)
Multi-factorial etiology: 1.Genetic Factors
- Positive Family History 2 .Environmental Factors
-Obesity -Increased Sodium Intake
-Stress - Increased Alcohol Intake
-95% of hypertensive patient fall into this category.

2 )Secondary Hypertension:
Due to an underlying medical condition
Renal
Endocrine Cardiovascular
Chronic alcohol abuse
Medications

Renal : -Polycystic disease
-Renal artery stenosis -Renin-producing tumors
-Chronic renal disease -Renal vasculitis
2 )Secondary Hypertension:

Endocrine: - Adrenocortical hyperfunction (Cushing syndrome,
primary aldosteronism,congenital adrenal hyperplasia) - Exogenous hormones (glucocorticoids, estrogen)
- Pheochromocytoma - Hypothyroidism
- Hyperthyroidism - Pregnancy-induced
2 )Secondary Hypertension:

Cardiovascular:
- Coarctation of aorta - Vasculitis
- Increased intravascular volume
2 )Secondary Hypertension:

Medications: -Steroids
- Oral contraceptives - Amphetamines and cocaine
- Nonsteroidal anti-inflammatory - Psychiatric: carbamazepine, lithium and tricyclic
antidepressants
2 )Secondary Hypertension:

1 )Severe headache
2 )Fatigue or confusion
3 )Vision problems
4 )Chest pain
5 )Difficulty breathing
6 )Irregular heartbeat
7 )Hematuria
8 )Lower limb edema

Patients with pheochromocytoma may have a history of paroxysmal headaches, sweating, tachycardia, palpitations, and orthostatic hypotension.
Note:

ECG
Uri
ne s
tick test f
or
pr
otei
n
& b
lood
Fasti
ng
bl
ood f
or (t
otal
&HDL c
holesterol +
Gl
uc
ose )
Serum
u
rea, crea
ti
ni
ne
& electr
oly
tic
Routine investigation

Aortic Coarctation - Arm to leg systolic Blood Pressure difference (abnormal if >20 mmHg)
- Chest X-Ray (notching of the lower rib borders)- Echocardiogram (Children)
- MRI Chest (Adults)Cushing's Disease
- 24 hour Urine Cortisol- Late night Salivary cortisol
- Low dose Dexamethasone Suppression Test Pheochromocytoma
- 24h Urine Metanephrine - Plasma free metanephrines
Optional laboratory tests:

X-rays: - May show cardiomegaly
X-RAY CHEST IN HEART FAILURE

● Refer people to specialist care the same day if they have:
− accelerated hypertension (BP > 180/110 mmHg ) with signs of papilloedema and/or retinal haemorrhage)
− suspected phaeochromocytoma (labile or postural hypotension,
headache, palpitations, pallor and diaphoresis).
● If nedded more investigations for secondary cause of hypertension.
Specialist investigations


1 )Weight reduction (BMI, 18.5 to 24.9 kg/m2)2 )Adoption of the Dietary Approaches to Stop
Hypertension (DASH) eating plan: - Low content of saturated fat, cholesterol, and total fat
- Focuses on fruits, vegetables, and fat-free or low-fat dairy products
- Rich in whole grains, fish, poultry, beans, seeds, and nuts - Contains fewer sweets, added sugars and sugary
beverages, and red meats -Dietary sodium restriction ideally to 1.5 g/day
•

4 )Regular aerobic physical activity.5 )Moderate alcohol consumption (2 or fewer
drinks/day).6 )Smoking cessation
7 )Do not offer calcium, magnesium or potassium
supplements as a method of reducing blood pressure


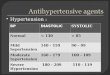
thiazide diuretics
calcium antagonists
(CA)
ACE inhibitors
angiotensin receptor
antagonists (ARB)
β-blockers (BB).
*Will lower BP and reduce the complications of HTN
HNT Drugs

● Where to start? - Hydrochlorothiazide 12.5 mg
- Chlorthalidone 12.5 mg
●How much ? - Up to 25 mg, unclear benefit beyond that
●Cost? Cheap!
●Side effects -- hypokalemia, glucose intolerance
I) Thiazide diuretics:

●Where to start? - Lisinopril 10 mg QD
- Benazapril 10 mg QD - Enalapril 5 mg QD
●How much? - Up to 80 mg (only 40 mg for enalapril)
●Cost -- cheap!
●Side effects -- cough
2 )ACE Inhibitors

●Where to start? - Amlodipine 5 mg QD
- Diltiazem ER 120 mg QD - Nifedipine ER 30 mg QD
●How much? - Amlodipine 10 mg QD
- Diltiazem ER 540 mg QD - Nifedipine ER 120 mg QD
●Cost? - Amlodipine is generic
- Diltiazem=cheap! - Nifedipine-less cheap
●Side effects? - edema
- constipation
3 )CCBs

●Where to start? - Not with beta blockers
●Why not? - Possible increase in stroke risk, particularly in
elderly patients
- first-line alternatives in patients who are 60 years and older, especially for stroke prevention.
3 )Beta Blockers

●Where to start? - Metoprolol 25 mg BID
- Atenolol 25 mg QD
●How much? - Up to 100 mg ●Cost -- cheap!
●Side effects -- bradycardia, fatigue, depression
3 )Beta Blockers

●ARBs (losartan is generic but still pricey)
●Alpha blockers
●Aldosterone antagonists
Even More Meds
ACE inhibitors and ARBs not as effective in African-Americans

indications and contraindicationsof medications

Too many choices, just tell me what to do!

indications and contraindicationsof medications

Labs: Potassium and Creatinine, maybe sodium
●at initiation of treatment ● 2-4 weeks after starting
● Again after every dose adjustment ● Annually


Organs affected
Heart
brain
eyes
Kidney
Blood vessels

1)Atherosclerosis :
formation of fibro fatty lesions in the intimal lining of the large and medium sized arteries such as aorta and its branches, coronary arteries and cerebral arteries
2)Stroke or Heart Attack :
If an atherosclerotic plaque breaks off inside the artery, or the blood vessel ruptures, a blood clot can form within the artery. If this blocks blood flow to the brain it can lead to a stroke. If it blocks blood flow to the heart it can result in a heart attack.

3)Aneurysm:
This is when the blood vessels have been weakened to such an extent that part of the blood vessel wall ‘balloons’ or bulges. The most common locations for an aneurysm include the main artery that
carries blood from the heart, arteries in the brain, legs, intestines, and the arteries leading to the spleen
4)Vascular dementia:
High blood pressure can cause the blood vessels that supply your brain with blood to narrow or become damaged. If the brain is not supplied with enough oxygen due to stroke, cells in the brain may be damaged causing adverse effects on a person’s memory, thinking, or language skills. This condition is called vascular dementia

5 )Hypertensive retinopathy:


-Kumar & Clark's Clinical Medicine (Saunders, 2009)
-Davidson's Principles and Practice of Medicine 21st Edition
-Pharmacotherapy 7th edition McGraw Hill Dipiro
-NICE quick reference HTN

Thanks!!Have a Nice Day
^_^