Embed Size (px)
Citation preview

1586
Pulmonary arterial hypertension (PAH) is a rapidly pro-gressive disease characterized by obstructive remodeling
of distal pulmonary arteries (<500 μm), leading to a progres-sive elevation in pulmonary vascular resistance and subse-quent right heart failure and death. There is currently no cure for PAH, which has a very poor prognosis (mean survival of 2.8 years).1 It is well known that pulmonary arteries display complex structural and functional changes in PAH and that pulmonary endothelial cell (EC) dysfunction plays a crucial
role in the disease progression. Despite an increased knowl-edge in the past years about PAH pathobiological cellular and molecular mechanisms, we still do not know what initiates this disease and its characteristic pulmonary vascular remodeling.2
Editorial see p 1545 Clinical Perspective on p 1597
Pericytes are central regulators of vascular development, stabilization, maturation, and remodeling, modulating EC
Background—Pericytes and their crosstalk with endothelial cells are critical for the development of a functional microvasculature and vascular remodeling. It is also known that pulmonary endothelial dysfunction is intertwined with the initiation and progression of pulmonary arterial hypertension (PAH). We hypothesized that pulmonary endothelial dysfunction, characterized by abnormal fibroblast growth factor-2 and interleukin-6 signaling, leads to abnormal microvascular pericyte coverage causing pulmonary arterial medial thickening.
Methods and Results—In human lung tissues, numbers of pericytes are substantially increased (up to 2-fold) in distal PAH pulmonary arteries compared with controls. Interestingly, human pulmonary pericytes exhibit, in vitro, an accentuated proliferative and migratory response to conditioned media from human idiopathic PAH endothelial cells compared with conditioned media from control cells. Importantly, by using an anti–fibroblast growth factor-2 neutralizing antibody, we attenuated these proliferative and migratory responses, whereas by using an anti–interleukin-6 neutralizing antibody, we decreased the migratory response without affecting the proliferative response. Furthermore, in our murine retinal angiogenesis model, both fibroblast growth factor-2 and interleukin-6 administration increased pericyte coverage. Finally, using idiopathic PAH human and NG2DsRedBAC mouse lung tissues, we demonstrated that this increased pericyte coverage contributes to pulmonary vascular remodeling as a source of smooth muscle–like cells. Furthermore, we found that transforming growth factor-β, in contrast to fibroblast growth factor-2 and interleukin-6, promotes human pulmonary pericyte differentiation into contractile smooth muscle–like cells.
Conclusions—To the best of our knowledge, this is the first report of excessive pericyte coverage in distal pulmonary arteries in human PAH. We also show that this phenomenon is directly linked with pulmonary endothelial dysfunction. (Circulation. 2014;129:1586-1597.)
Key Words: cell communication ◼ endothelilal cells ◼ fibroblast growth factor 2 ◼ interleukin-6 ◼ pericytes ◼ pulmonary arterial hypertension ◼ transforming growth factor beta
© 2014 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.113.007469
Received November 12, 2013; accepted January 24, 2014.From the National Institute of Health and Medical Research, Unit 999, LabEx Laboratory of Excellence in Research on Medication and Innovative
Therapeutics, Centre Chirurgical Marie Lannelongue, Le Plessis-Robinson, France (N.R., L.T., M.L.H., A.H., C.P., R.T., C.S., E.F., A.S., D.M., P.D., M.H., C.G.); University Paris-Sud, School of Medicine, Kremlin-Bicêtre, France (N.R., L.T., M.L.H., A.H., C.P., R.T., C.S., E.F., A.S., D.M., P.D., M.H., C.G.); and Public Hospitals of Paris, Pneumology Service, Reference Center of Severe Pulmonary Hypertension, University Hospital Department Thorax Innovation, Hôpital de Bicêtre, Kremlin-Bicêtre, France (A.H., C.S., A.S., D.M., M.H.).
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/lookup/suppl/doi:10.1161/CIRCULATIONAHA. 113.007469/-/DC1.
Correspondence to Christophe Guignabert, PhD, Institut National de la Santé et de la Recherche Médicale, Unité Mixte de Recherche S999, Centre Chirurgical Marie Lannelongue, 133, Avenue de la Resistance, 92350 Le Plessis-Robinson, France. E-mail [email protected]
Increased Pericyte Coverage Mediated by Endothelial-Derived Fibroblast Growth Factor-2
and Interleukin-6 Is a Source of Smooth Muscle–Like Cells in Pulmonary Hypertension
Nicolas Ricard, PhD; Ly Tu, PhD; Morane Le Hiress, MSc; Alice Huertas, MD, PhD; Carole Phan, MSc; Raphaël Thuillet, BSc; Caroline Sattler, MD, MSc; Elie Fadel, MD, PhD;
Andrei Seferian, MD, MSc; David Montani, MD, PhD; Peter Dorfmüller, MD, PhD; Marc Humbert, MD, PhD; Christophe Guignabert, PhD
Hypertension
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

Ricard et al Pericytes in Pulmonary Arterial Hypertension 1587
proliferation, vascular tone, and immunity. They occupy a stra-tegic position at the interface between circulating blood and interstitial space and at close proximity to ECs and smooth muscle cells (SMCs). Pericytes play crucial key roles in vas-cular homeostasis by regulating the following: (1) EC growth, proliferation, differentiation, and migration3; (2) SMC contrac-tion and capillary blood flow; (3) immune cell functions4; and (4) their possible differentiation in SMCs5 and dendritic cells,6 acting as progenitor cells. Pericytes contain cGMP-dependent protein kinase, an important enzyme in SMC contraction,7 and they demonstrate tension development and contractility in vitro.8 Pericytes can transform into contractile smooth muscle (SM)–like cells under chronic hypoxic conditions.9 Morphologically, pericytes are polymorphic, elongated, multibranched cells. Different subsets of pericytes can be distinguished based on their morphology, distribution, and protein expression, sug-gesting tissue-specific functions.10 In particular, pericytes that are found along arterioles and capillaries express different degrees of neural glial antigen-2 (NG2), 3G5-ganglioside anti-gen (3G5),11 α-SM–actin, non-α-SM–actin, desmin, vimentin, tropomyosin, and cGMP-dependent protein kinase.12 Despite their crucial contribution to both structure and function of the vascular bed, there are no data on pericyte distribution and numbers in PAH. We investigated the following: (1) pulmo-nary vascular pericyte distribution in human and experimental PAH; (2) whether either fibroblast growth factor-2 (FGF-2) or interleukin-6 (IL-6) can modulate in vitro pulmonary pericyte behavior, including proliferation, migration, and differen-tiation; (3) whether the overexpression of endothelial-derived FGF-2 and IL-6 in PAH can explain the increased pericyte cov-erage; (4) the effects of elevated levels of FGF-2 or IL-6 on vascular pericyte coverage in a mouse model of retinal angio-genesis; (5) in vitro differentiative potential of pulmonary peri-cytes into SM-like cells; and (6) in vivo differentiation states of pericytes in chronically hypoxic NG2DsRedBAC transgenic mice, as well as in human remodeled distal pulmonary arteries.
MethodsStudy PopulationAn expanded Materials and Methods is in the online-only Data Supplement.
For the in vitro and in situ studies, we used lung specimens obtained during lung transplantation in patients with idiopathic PAH (iPAH) or heritable PAH and during lobectomy or pneumonectomy for local-ized lung cancer in control subjects (for clinical data, see Table I in the online-only Data Supplement). The lung specimens from the controls were collected at a distance from the tumor foci. This study was approved by the local ethics committee (Comité de Protection des Personnes Ile-de-France VII, Le Kremlin-Bicêtre, France). All patients gave informed consent before the study.
Isolation, Culture, and Functional Analyses of Human Pulmonary PericytesHuman pulmonary pericytes were isolated using an anti-3G5 anti-body, prepared from murine hybridoma (American Type Culture Collection, Molsheim, France), and anti–immunoglobulin M mag-netic beads (Dynal, Life Technologies, Saint-Aubin, France) on lung tissue fragment digested by collagenase type I (Life Technologies). Pulmonary pericytes were cultured in pericyte medium (Clinisciences, Nanterre, France). To characterize the pericyte cell phenotype, cells were labeled with anti-NG2 (Millipore, Saint-Quentin-en-Yvelines,
France), anti–α-SM-actin, and anti-CD31 antibody (Clinisciences). Corresponding fluorescent-labeled secondary antibodies were used (Interchim, Montluçon, France). Cells were observed using LSM 700 confocal microscopy (Zeiss, Marly-Le-Roy, France). Cells were used for the study between passages 3 and 6. Proliferation was assessed by 5-bromo-2-deoxyuridine incorporation13 and migration by a modified Boyden chamber migration assay.14 Pulmonary ECs and SMCs were isolated and cultured as described previously.15,16
Western Blot, ELISA, Gelatin Zymography, and ImmunostainingCells were homogenized and sonicated in PBS containing protease and phosphatase inhibitors, and 30 μg of protein was used to detect Cyclin D1, α-SM–actin, calponin and smooth muscle protein of 22kDa (SM22) (Clinisciences), and β-actin (Sigma-Aldrich, Saint-Quentin Fallavier, France) as described previously.13 Concentrations in platelet-derived growth factor (PDGF)-BB, IL-6, and FGF-2 in conditioned media were evaluated using Quantikine (R&D Systems, Lille, France) according to the instructions of the manufacturer. Gelatin zymography, immunohistochemistry, and immunocyto-fluorescent staining were performed as described previously.13,14,17 Quantification of pericyte number has been determined by counting all 3G5-positive (3G5+) cells into either the media or the adventitia of the vessels. Quantification by levels of fluorescence intensity or dis-tances between 3G5+ cells and the vessel lumen have been excluded. The 3G5+ cells that are visible into alveolar wall surrounding capil-laries were not counted.
Mouse Retinal Angiogenesis, NG2DsRedBAC Mice, and Rodent Models of PAHAnimal studies were approved by the administrative panel on animal care at the University Paris-Sud (Le Plessis-Robinson, France).
Newborn mice (OF1 strain; Janvier Labs, Saint Berthevin, France) were injected intraperitoneally at day 1 and day 3 after birth with vehicle (PBS) or IL-6 (10 ng) with IL-6 receptor (2.5 ng) or FGF-2 (10 ng) in the presence or absence of neutralizing antibody anti–IL-6 (10 μg; Peprotech, Neuilly-sur-Seine, France) or anti–FGF-2 (10 μg; Millipore) preincubated 30 minutes at 37°C. At day 5, retinas were pre-pared as described previously.18 Images were taken using an LSM700 confocal microscope and analyzed using Zen software (Zeiss).
NG2DsRedBAC transgenic mice (The Jackson Laboratory, Bar Harbor, ME) or young male Wistar rats (100 g; Janvier Labs) were studied at either 3 weeks after a single subcutaneous injection of monocrotaline (60 mg/kg) or vehicle15 or 3 weeks after chronic expo-sure to hypoxia (10% oxygen) or in room air.19 Animals were anes-thetized with isoflurane. A polyvinyl catheter was introduced into the right jugular vein and pushed through the right ventricle into the pulmonary artery. Another polyethylene catheter was inserted into the right carotid artery. After measurement of hemodynamic parameters, the thorax was opened, and the left lung was immediately removed for flow cytometry or immunofluorescence analyses. The right lung was fixed in the distended state with formalin buffer. The right ven-tricular hypertrophy index and the percentage of muscularized ves-sels were determined as described previously.17
Statistical AnalysesStatistical significance was tested using the nonparametric Mann-Whitney test or the nonparametric Kruskal-Wallis test with post hoc Dunn’s test.
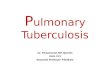
ResultsIncreased Pericyte Coverage on Pulmonary Arteries in Human and Experimental PAHIn human lung tissues, a 2-fold increase in pericyte number per vessel was observed in PAH specimens when compared with controls (Figure 1A) [≈96% of NG2+ cells coexpressed
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

1588 Circulation April 15, 2014
3G5 (see Figure I in the online-only Data Supplement)]. This increase in pericyte coverage is uniform and independent of vessel diameter (Figure 1A), and no significant difference was noted between various forms and degrees of pulmonary vascular remodeling in patients with iPAH and heritable PAH (Figure 1B; see Figures II and III in the online-only Data Supplement). Proliferating cell nuclear antigen expression, usually absent in pulmonary pericytes in control patients, has been found in a small proportion of pulmonary pericytes in remodeled distal pulmonary arteries from patients with PAH (Figure 1C). Although NG2 and 3G5 are irregularly distrib-uted throughout the membrane and explain the patchy surface membrane staining, we noted that pericytes are polymorphic, elongated, and multibranched (Figure 1Da and 1Db). These
characteristics are clearly visible in the NG2DsRedBAC transgenic mice that express an optimized red fluorescent pro-tein variant (DsRed.T1) under the control of the mouse NG2 (Cspg4) promoter/enhancer (Figure 1Dc and 1Dd). In addi-tion, we found that pericytes are located in either media or adventitia layers of pulmonary vessels (Figure 1De and 1Df) and that they maintain close relationships with ECs despite the distance (Figure 1Db, 1Dd, and 1Df). Indeed, several pericyte–endothelial contact points (*) are clearly visible in the endothelium of remodeled distal pulmonary arteries in PAH. All these observations are consistent with recent find-ings obtained by Tigges et al20 in femoral arteries after injury.
These results are confirmed by similar observations obtained in experimental models of PAH, the models of
Figure 1. Increased pericyte coverage in pulmonary arteries in human pulmonary arterial hypertension (PAH). A, Representative images of 3G5-ganglioside antigen (3G5)-positive cells (white arrowhead) in lungs from patients with PAH and from control subjects. The bar graph represents medians with interquartile range of 15 vessels per vessel size category and per subject (n=10 control subjects and n=13 patients with PAH). B, Representative images of 3G5-positive cells (white arrowhead) in lungs from patients with PAH in various degrees of pulmonary vascular remodeling (a, mild; b, severe; c, occluded) and in a complex vascular lesion (d). C, Representative images of proliferating cell nuclear antigen-positive (#) and -negative (*) pericytes in lungs from patients with PAH and from control subjects. D, Representative images illustrating the endothelial/pericyte interactions in remodeled distal pulmonary arteries in PAH (a and b) and in chronically hypoxic NG2DsRedBAC mice (c and d). Pulmonary pericytes appear polymorphic, elongated, and multibranched. In addition, they are located in either media or adventitia layers of pulmonary vessels (e and f), and several pericyte-endothelial contact points (*) are visible (b, d, and f). **P<0.01; ***P<0.001 compared with control patients with the nonparametric Mann-Whitney test. Scale bar, 50 μm in all sections. L indicates lumen.
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

Ricard et al Pericytes in Pulmonary Arterial Hypertension 1589
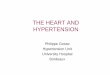
monocrotaline- and chronic hypoxia–induced pulmonary hypertension, in which a substantial increase in pericyte number per vessel was observed (up to 6- and 3-fold, respec-tively) (Figure 2A; see Figure I in the online-only Data Supplement). Using chronically hypoxic NG2DsRedBAC mice, we also showed a progressive accumulation of NG2+ cells around vessels starting at day 7 (Figure 2B), before increased mean pulmonary arterial pressure (see Figure IV in the online-only Data Supplement). Together with our human findings, these results strongly support the notion that pulmonary pericytes contribute to the pulmonary vascu-lar remodeling associated with PAH.
Excessive Release of Endothelial-Derived IL-6 and FGF-2 in PAH Actively Stimulates Migration and Proliferation of Human Pulmonary Pericytes In VitroImportant characteristics of dysfunctional pulmonary endothe-lium in PAH are represented by vasoconstriction/vasodilation imbalance on the one hand2 and hyperproliferative and apop-tosis-resistant EC phenotype on the other hand.13,21,22 Among the excessive release of endothelial-derived chemokines and growth factors, both IL-6 and FGF-2 play an integral role in mediating the structural and functional changes in the pul-monary vasculature in PAH.13,16,22–24 In addition, numerous
Figure 2. Increased pericyte coverage in experimental pulmonary hypertension. A, Representative images of 3G5-ganglioside antigen (3G5)-positive cells (red arrowhead) in lungs from monocrotaline-injected rats and control animals and lungs from rats exposed to chronic hypoxia or normoxia. The bar graph represents medians with interquartile range (10 vessels per animal; n=5 rats per condition). B, Representative images of neural glial antigen-2 (NG2)-positive cells (white arrowhead) in distal pulmonary arteries from NG2DsRedBAC mice exposed to chronic hypoxia or normoxia at various time points. The bar graph represents medians with interquartile range (10 vessels per NG2DsRedBAC mouse; n=5 animals per condition). *P<0.05; **P<0.01; ***P<0.001 compared with normoxia or vehicle or control patients with the nonparametric Mann-Whitney test. Scale bar, 50 μm in all sections. L indicates lumen.
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

1590 Circulation April 15, 2014
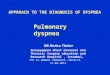
studies describe the importance of PDGF signaling for peri-cyte recruitment and the functional association between ECs and pericytes.25–27 To determine whether the excessive release of endothelial-derived FGF-2, IL-6, or PDGF-BB contrib-ute to this increase in pericyte coverage, we first investigated the effect of conditioned media of quiescent cultured human pulmonary ECs from patients with iPAH and controls. Using primary cultures of pulmonary pericytes (see Figure V in the online-only Data Supplement), we found that pericyte migra-tion and proliferation elicited by pulmonary EC media were greater with pulmonary ECs from patients than from controls (Figure 3A and 3B). In accordance with the increase in the chemotactic migratory behavior of pulmonary pericytes in the presence of iPAH EC media, we found an increase in matrix metalloproteinase levels (Figure 3C). FGF-2 and IL-6 levels were markedly elevated in the conditioned media of iPAH ver-sus control pulmonary ECs, whereas PDGF-BB levels were not different (Table). We next examined the effects of exogenous FGF-2 and IL-6 exposure on the migration and proliferative potentials of human pulmonary pericytes in primary culture. FGF-2 and IL-6 were 2 strong inducers of migration for cul-tured human pulmonary pericytes, but only FGF-2 was a mito-gen (Figure 3D and 3E). Consistent with these findings, Cyclin D1 expression dramatically increased during G1
/S-phase tran-sition, and we showed that FGF-2, but not IL-6, induced Cyclin D1 expression in cultured pulmonary pericytes (Figure 3F). In addition, we also showed that the use of anti–FGF-2 and anti–IL-6 neutralizing antibodies substantially attenuated the peri-cyte migration elicited by pulmonary EC media (Figure 3A). Furthermore, we found that anti–FGF-2 neutralizing antibody, but not the anti–IL-6 neutralizing antibody, reduced the prolif-erative effect of pulmonary EC media (Figure 3B).
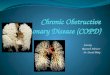
FGF-2 and IL-6 Regulate Pericyte Coverage In Vivo in a Mouse Model of Retinal AngiogenesisTo study the effect of FGF-2 and IL-6 on pericyte coverage in vivo, subsequent studies were performed using the mouse model of retinal angiogenesis. Because physiological develop-ment of blood vessels in the mouse retina occurs during the first postnatal week, this in vivo model of retinal angiogenesis offers the opportunity to study the functional importance of both factors in vivo.28 We increased the pericyte number per millimeter of vessel length by ≈35% to 40% when recombinant FGF-2 or IL-6 was administered to neonatal animals at days 1 and 3 (Figure 4A and 4B). Furthermore, both anti–FGF-2 neutralizing antibody and anti–IL-6 neutralizing antibody completely abolished the excessive pericyte coverage. Similar results were obtained with the number of pericytes per branch-ing point (see Figure VI in the online-only Data Supplement).
Transforming Growth Factor-β, In Contrast to FGF-2 and IL-6, Promotes Human Pulmonary Pericyte Differentiation into Contractile SM-Like CellsBecause the transforming growth factor-β (TGF-β) signal-ing pathway is activated in various experimental models of PAH and contributes to the progression of PAH,29–32 we next examined the following: (1) the pericytic activation state of the phosphorylated Smad2 signaling in situ; and (2) the effect of exogenous TGF-β on pericyte differentiation in vitro. Our
phosphorylated Smad2 immunofluorescence findings clearly showed that human PAH tissues are characterized by an over-activation of the TGF-β pathway in several different pulmo-nary vascular cells, including in pulmonary pericytes (45±3% of pulmonary pericytes in PAH tissues compared with 6±4% in control tissues) (Figure 5). In addition, TGF-β, in con-trast to FGF-2 and IL-6, promoted pericyte differentiation into contractile SM-like cells, as demonstrated by increased expressions of α-SM–actin, calponin, and SM22 (Figure 6A and 6B). Indeed, increased α-SM–actin, calponin, and SM22 expressions were associated with serum deprivation in cul-tured pulmonary pericytes, a phenomenon that was totally prevented by the addition of recombinant FGF-2, IL-6, and complete medium (Figure 6A and 6B).
Pulmonary Pericytes Contribute to the Structural Vascular Remodeling in PAH as a Potential Source of Contractile SM-Like Cells In Situ and In VivoTo determine whether the increase in pulmonary pericyte cov-erage in PAH could represent a local source of SM-like cells and actively contributes to the pulmonary vascular remodel-ing, we next examined the pericyte differentiation state in par-affined lung tissue sections of patients with PAH and controls. In control lungs, our immunohistochemical findings revealed that high 3G5 and vimentin protein levels (Figure 7A, white asterisks) were seen in all the examined pulmonary peri-cytes (Figure 7A). In addition, all 3G5+ cells were SM22 and α-SM–actin negative in control lungs (see Figure VII in the online-only Data Supplement). In contrast, PAH pulmonary pericytes around remodeled pulmonary arteries expressed dif-ferent levels of vimentin, including low expressing 3G5 and vimentin pericytes (Figure 7A, sharp sign). Furthermore, a small proportion of low expressing NG2 cells were positive for SM22 (Figure 7B, sharp sign) and α-SM–actin (Figure 7C, sharp sign). To assess the significance of this increased peri-cyte coverage in the pathogenesis, we followed up pericyte differentiation using chronically hypoxic NG2DsRedBAC mice by flow cytometry analyses (see Figure VIII in the online-only Data Supplement) and in situ immunofluores-cence. Consistent with our human findings, we noted a sub-stantial increase in the percentage of α-SM–actin+ pericytes at day 14, strongly supporting the notion that pulmonary peri-cytes contribute to the pulmonary vascular remodeling as a source of SM-like cells (Figure 7D and 7E; see Figures VIII and IX in the online-only Data Supplement).
DiscussionPericytes are found around precapillary arteries, capillaries, and postcapillary venules, and they occupy a strategic position at the interface between circulating blood and interstitial space and are at close proximity to ECs and SMCs. Herein, to the best of our knowledge, we report for the first time increased pericyte cov-erage of distal pulmonary arteries in experimental and human PAH. In PAH, we obtained evidences that pulmonary endothe-lial-derived FGF-2 and IL-6 partly contributes to this vascular abnormality. We found that both FGF-2 and IL-6 enhanced pulmonary pericyte migration in culture and that FGF-2 was a pericyte mitogen. In addition, we showed that exogenous FGF-2 or IL-6 increased the vascular pericyte coverage in a mouse
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

Ricard et al Pericytes in Pulmonary Arterial Hypertension 1591
Figure 3. Excessive release of endothelial-derived interleukin-6 (IL-6) and fibroblast growth factor-2 (FGF-2) in pulmonary arterial hypertension (PAH) increases migration and proliferation of human pulmonary pericytes in vitro. Migration (A) and proliferative potential (B) of human pulmonary pericytes in response to conditioned media from pulmonary endothelial cells (ECs) from control subjects and patients with idiopathic PAH (iPAH), with or without neutralizing antibodies anti–FGF-2 or anti–IL-6. The bar graph represents medians with interquartile range of n=4 to 6 human pulmonary ECs from different donors. C, Representative gelatin zymography. D, Migration potential of human pericytes in response to recombinant human platelet-derived growth factor-BB (PDGF-BB; 100 ng/mL) or IL-6 (10 ng/mL) with IL-6 receptor (IL-6R; 2.5 ng/mL) or FGF-2 (10 ng/mL) with or without neutralizing antibody anti–IL-6 or anti–FGF-2. The bar graph represents medians with interquartile range of n=4 to 5. E, Proliferative potential of human pericytes in response to 10% fetal calf serum (FCS) or recombinant IL-6 (10 ng/mL) with IL-6R (2.5 ng/mL) or FGF-2 (10 ng/mL) with or without neutralizing antibody anti–FGF-2. The bar graph represents medians with interquartile range. F, Representative Western immunoblots of Cyclin D1 and β-actin loading control and quantification of the Cyclin D1/β-actin ratios. The bar graph represents medians with interquartile range. *P<0.05; **P<0.01 compared with control ECs or basal condition or 1% FCS with the nonparametric Mann-Whitney test. #P<0.05; ##P<0.01 compared with iPAH ECs or the same treatment without the corresponding neutralizing antibody with the nonparametric Kruskal-Wallis test with post hoc Dunn’s test. Scale bar, 50 μm in all sections.
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

1592 Circulation April 15, 2014
model of retinal angiogenesis. Finally, using iPAH human and NG2DsRedBAC mouse lung tissues, we demonstrated that this increased pericyte coverage contributes to pulmonary vascular remodeling as a source of SM-like cells. Furthermore, we found that FGF-2, IL-6, and TGF-β affected the differentiative poten-tial of pulmonary pericytes into SM-like cells.
One of the major findings of the present study is the in situ demonstration that the pulmonary vascular remodeling is accompanied by an increase in pericyte density and cov-erage in distal pulmonary arteries in PAH. The number of pericytes is highly controlled and the pericytic coverage of
microvessels is dramatically affected under various patho-logical conditions.12,25,33 They are physiologically recruited to stabilize vessels in response to different signaling path-ways34: (1) the PDGF/PDGF receptor-β (PDGFR-β) sig-naling system; (2) the angiopoietin-1/Tie 2 signaling that facilitates direct interactions between pericytes and ECs; (3) sphingosine-1–phosphate-1 and endothelial differentia-tion sphingolipid G protein-coupled receptor 1; (4) vascular endothelial growth factor that suppresses PDGFR-β signaling through disruption of PDGFR-β/vascular endothelial growth factor receptor-2 complex formation35; and (5) TGF-β. Several alterations in the expression or activity of these signaling path-ways have been described in human and experimental models of PAH.2,23,29–32,36 However, little is known about the influence of these altered signaling pathways on pericyte density and functions, key phenomena for both pulmonary arteriole struc-tures and functions. Here, we obtained several evidences that the dysfunctional pulmonary endothelium in iPAH may partly contribute to the excessive pericytic envelope, notably through the overabundance of the endothelial-derived FGF-2 and IL-6. Indeed, we cannot exclude that other growth factors may also play a role in this phenomenon. In addition to the proliferation of resident pulmonary pericytes, several mechanisms could explain this increased pericyte coverage in PAH, including the differentiation of bone marrow–derived or tissue-resident pro-genitor cells, or pericyte recruitment from lost pulmonary ves-sels.20,37 In addition, we cannot exclude the fact that pulmonary
Table. Growth Factors Released by Pulmonary Endothelial Cells From Controls and From Patients With Idiopathic Pulmonary Arterial Hypertension
Controls iPAH
FGF-2 (pg/mL) 4.0 [1.7–14.4] (n=9) 11.2 [8.2–20.0] (n=9)*
IL-6 (pg/mL) 16.6 [11.1–61.3] (n=18) 70.9 [25.2–155.2] (n=13)*
PDGF-BB (pg/mL) 5.5 [0.9–20.0] (n=18) 2.7 [0.9–8.4] (n=13)†
Growth factor levels in conditioned media from cultures of pulmonary endothelial cells from patients with iPAH or controls after 24-hour incubation. Medians are shown as [25% percentile–75% percentile]. FGF-2 indicates fibroblast growth factor-2; IL-6, interleukin-6; iPAH, idiopathic pulmonary arterial hypertension; and PDGF, platelet-derived growth factor.
*P<0.05, iPAH vs controls. †Not significant.
Figure 4. Fibroblast growth factor-2 (FGF-2) and interleukin-6 (IL-6) increase pericyte coverage in vivo in a mouse retinal angiogenesis model. A, Representative images of pericytes (neural glial antigen-2–positive cells in red, white arrows) and endothelial cells (Isolectin B4–positive cells in green) of retina from 5-day-old mice treated with IL-6 (10 ng) with IL-6 receptor (2.5 ng) or FGF-2 (10 ng) with or without neutralizing antibody anti–IL-6 or anti–FGF-2. a indicates artery; and v, vein. B, Bar graph represents medians with interquartile range of 8 images per mice (n=3–5 mice from 2 litters). #P<0.05 compared with PBS with the nonparametric Kruskal-Wallis test with post hoc Dunn’s test. Scale bar, 50 μm in all sections.
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

Ricard et al Pericytes in Pulmonary Arterial Hypertension 1593
pericytes from PAH exhibit an altered cellular phenotype. The tissue sections and cells studied were from treated patients, so we cannot exclude the possibility that treatments may alter pericyte coverage. However, we reported a similar increase in pericyte coverage around remodeled vessels in the 2 well-recognized and widely used monocrotaline- and chronic hypoxia–induced pulmonary hypertension models, supporting the idea that this increase in the number of pericytes and ves-sel coverage in distal pulmonary arteries was directly linked to the pathogenesis of PAH. Consistent with this notion, both recombinant FGF-2 and IL-6/IL-6 receptor administration increased pericyte coverage in our murine retinal angiogen-esis model. Because ECs undergo molecular changes during pulmonary vascular remodeling in PAH, a better understand-ing of their importance for this process is important and will lead to novel knowledge in the pathogenesis of the disease.
Numerous studies describe the importance of PDGF sig-naling for pericyte recruitment and the functional association between ECs and pericytes on the one hand12,25–27,37 and for pathogenesis of PAH on the other.2,22,38–40 Genetic knockdown of either Pdgfb or Pdgfrb in developing mouse embryos gen-erate lethal microvascular leakage and hemorrhage.25,26 Enge et al25 reported that mice deficient in PDGF-B specifically in the endothelium have pericyte deficiency, demonstrating the critical role of the endothelial-derived PDGF-B for proper pericyte coverage on vessels. Importantly, it has been reported that tyrosine kinase inhibitors, such as imatinib and sunitinib,
may reduce pericyte density and attenuate angiogenesis and thereby are protective in solid tumor models.27,41–43 Inhibition of PDGFR-β can have potential benefits in experimental and human patients with PAH, but its profile of safety and particu-larly severe side effects raise many concerns regarding its use in clinical practice.38–40 In the present study, we did not find any differences in the PDGF-BB levels in the conditioned media of iPAH versus control pulmonary ECs (Table). We cannot exclude a pathogenic role for PDGF in this abnormal pericyte envelope in PAH, because PDGF can be sequestered and stored as a complex in the extracellular matrix and then released by proteolytic processes.2 In this way, production of matrix metalloproteinase-2 by pericytes and ECs actively con-tributes to vessel sprouting.44 A number of other crucial media-tors contribute and modulate pericyte coverage on vessels, and we noted that FGF-2 and IL-6 levels were markedly elevated in the conditioned media of iPAH versus control pulmonary ECs.
Pericytes have a unique synergistic relationship with micro-vascular ECs, and a complex paracrine mode of interaction exists between these 2 cell types.12,37 However, there are no data on the morphological and functional characteristics of pulmo-nary pericytes in PAH. Here, we show that they are located in either media or adventitia layers of pulmonary vessels in PAH and that they maintain close relationships with ECs despite the distance. The role of intrinsic EC abnormalities leading to altered EC phenotype in iPAH has emerged recently. Accumulating data from multiple groups clearly indicate that several structural and functional abnormalities are present in ECs and play direct functional consequences for the characteristic progressive pul-monary vascular obstruction in PAH.13,16,21,22,45–47 In particular, dysfunctional PAH ECs display to varying degrees an imbal-anced production of several mediators leading toward an excess of vasoconstriction, SM hyperplasia, and pulmonary vascular remodeling.2,48,49 Among these factors, we showed that FGF-2 is markedly overproduced by iPAH pulmonary ECs in walls of dis-tal arteries and in isolated primary cells compared with controls. This overexpression of endothelial-derived FGF-2 contributes significantly not only to SM hyperplasia by a paracrine action but also to the abnormal endothelial phenotype by an autocrine action.13,16,22 Here, we showed that overabundance of FGF-2 in iPAH EC conditioned media contributed also to exaggerated migration and proliferative potentials of pulmonary pericytes in culture. Consistent with our observations, we also showed that the administration of recombinant FGF-2 in neonatal mice increased pericyte envelope of blood vessels in the mouse retina. In addition, a key role of IL-6 in the progression of the disease has been demonstrated experimentally. Delivery of exogenous IL-6 protein in rats or mice is sufficient to result in pulmonary vascular remodeling and pulmonary hypertension or to exagger-ate the response to the hypoxic condition.50,51 Furthermore, IL-6 overexpressing mice spontaneously develop pulmonary hyper-tension and pulmonary vascular remodeling, whereas Il6 knock-out mice are more resistant to the development of pulmonary hypertension induced by chronic hypoxia.23,24 Consistent with these findings, we found that the overabundance of IL-6 in iPAH EC conditioned media contributed also to the increased pericyte migration in culture and pericyte coverage of blood vessels in the mouse retina model. All these elements support the idea that key proliferative and migratory endothelial-derived factors in
Figure 5. Increased phosphorylated Smad2 (p-Smad2) levels in pulmonary pericytes in human pulmonary arterial hypertension (PAH). Representative images of p-Smad2 (light blue) in pericytes (3G5-ganglioside antigen-positive cells in red, white arrowheads) in lungs from patients with PAH and from control subjects. Scale bar, 50 μm in all sections.
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

1594 Circulation April 15, 2014
PAH could promote pericytic coverage, thus contributing to pul-monary SM hyperplasia and vascular remodeling in PAH.
Pericytes are considered by many to be multipotent cells, because they maintain plasticity and are able to transdifferenti-ate into other cell types, including vascular SMCs, fibroblasts, adipocytes, chondrocytes, and osteoblasts.12,37 Such versatil-ity is crucial physiologically to recruit and stabilize vessels, but whether or not defects in this ability could contribute to remodel blood vessels is unknown. Among the well-known contributing factors, TGF-β is considered as a strong inducer of pericyte differentiation into SM-like cells. Indeed, TGF-β induces α-SM–actin in the immortalized neural crest stem cell line Monc-152 and induces α-SM–actin and SM22 expres-sions in the mesenchymal cell line 10T1/2.53,54 Consistent with
these findings, we found that exogenous TGF-β promoted pericyte differentiation into contractile SM-like cells in cul-ture, increasing expression of α-SM–actin, calponin, and SM22. In contrast to TGF-β, exogenous FGF-2 and IL-6 main-tained pulmonary pericytes in a noncontractile state in culture and prevented the pericyte differentiation induced by serum deprivation. Our findings are consistent with those found by Thanabalasundram et al55 that nicely demonstrated the impor-tance of FGF-2 and TGF-β for pericyte differentiation and the modulation of the blood–brain barrier integrity. Importantly, we found an overactivation of the TGF-β pathway in several different pulmonary vascular cells in remodeled PAH vessels, including in pulmonary pericytes. However, additional studies are needed to better understand the source and the pathogenic
Figure 6. Fibroblast growth factor-2 (FGF-2) and interleukin-6 (IL-6) keep pulmonary pericytes under the noncontractile phenotype, whereas transforming growth factor-β (TGF-β) induces pulmonary pericyte differentiation into contractile smooth muscle (SM)-like cells. A, Representative images of α-smooth muscle-actin, calponin, and SM22 labeling in pulmonary smooth muscle cells and pulmonary pericytes in complete medium or 1% fetal calf serum (FCS) with TGF-β (10 ng/mL), FGF-2 (10 ng/mL), or IL-6 (100 ng/mL) with IL-6 receptor (25 ng/mL). Scale bar, 100 μm. B, Representative Western blots and quantification of the α-SM-actin/β-actin, calponin/β-actin, and SM22/β-actin ratios. The bar graph represents medians with interquartile range (n=4 control subjects). *P<0.05 compared with complete medium (CM) with the nonparametric Mann-Whitney test. #P<0.05; ##P<0.01 compared with 1% FCS with the nonparametric Kruskal-Wallis test with post hoc Dunn’s test. Scale bar, 100 μm in all sections.
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

Ricard et al Pericytes in Pulmonary Arterial Hypertension 1595
role of TGF-β in PAH. In contrast with control lung speci-mens, we were also able to find, in PAH remodeled vessels, a small proportion of pulmonary pericytes expressing low levels of NG2 or 3G5 together with α-SM–actin and SM22. Consistent with our human findings, a substantial increase in the percentage of pulmonary pericytes expressing α-SM-actin has been observed in chronically hypoxic NG2DsRedBAC mice. Although other lineage tracing reporter strategies could be used to permanently label all pericyte-derived cells, we chose to use NG2DsRedBAC mice, which allowed us to study the early steps of the pericyte differentiation into contractile
SM-like cells. Although additional experiments are required to identify the involved factors, these findings clearly support the idea that pulmonary pericytes are a potential in situ source of SM-like cells that could contribute to PAH pulmonary vascu-lar remodeling. Interestingly, Qiao et al56 also recently dem-onstrated that the endothelial-to-mesenchymal transition is another mechanism contributing to SM hyperplasia in PAH. Activation of proteases intervenes in proteolytic processing of the extracellular matrix, with release of growth factors (FGF-2, TGF-β, vascular endothelial growth factor, and PDGF) stored in their heparin-like glycosaminoglycans, actively contributing
Figure 7. Pulmonary pericytes are a source of contractile smooth muscle-like cells in remodeled pulmonary arteries in experimental and human pulmonary arterial hypertension (PAH). A, Representative images of pericytes (3G5-ganglioside antigen labeling in white) and vimentin (in red) in control and idiopathic PAH (iPAH) human lungs. * indicates vimentin-positive pericytes; # indicates vimentin-negative pericytes. B, Representative images of pericytes (neural glial antigen-2 [NG2] labeling in white) and SM22 (in red) in PAH human lungs. * indicates SM22-negative pericytes; # indicates SM22-positive pericytes. C, Representative images of pericytes (NG2 labeling in white) and α-smooth muscle (SM)–actin (in red) in iPAH human lungs. * indicates α-SM–actin-negative pericytes; # indicates α-SM–actin-positive pericytes. D, Flow cytometry analyses of α-SM–actin expression in pulmonary pericytes in NG2DsRedBAC mice exposed to chronic hypoxia or normoxia at various time points. The bar graph represents medians with interquartile range (n=5 animals per condition). E, Representative images of pericytes (NG2DsRed) and α-SM–actin (in white) in chronically hypoxic NG2DsRedBAC mice. * indicates α-SM–actin-negative pericytes; # indicates α-SM–actin-positive pericytes. **P<0.01 compared with normoxia with the nonparametric Mann-Whitney test. Scale bars, 20 μm (A through C) and 50 μm (E).
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

1596 Circulation April 15, 2014
to changes of the cellular microenvironment, which can also result in modification of the pericyte differentiation state.
Interestingly, altered vessel pericyte coverage has been reported in 1 case of pulmonary hypertension associated with an Adams-Oliver syndrome.57 Although a possible role of the bone morphogenetic protein pathway is strongly suspected in this disease,58 we did not find any differences between patients with PAH carrying a BMPR2 mutation and noncarriers.
In summary, to the best of our knowledge, our study pro-vides the first in situ demonstration of an overabundance of the pericyte envelope around the distal pulmonary arteries in experimental and human PAH. Furthermore, our findings underscore for the first time that, among the different potential mechanisms contributing to this phenomenon, both endothe-lial-derived FGF-2 and IL-6 may play a critical role in this pro-cess. We also showed that this increase in pulmonary pericyte coverage in PAH could represent a local source of SM-like cells and actively contributes to the pulmonary vascular remodeling.
Acknowledgments We thank Dr William Stallcup for kindly providing one of the NG2 antibodies. We also thank Dr Elodie Gouadon for her very help-ful technical assistance. Drs Ricard, Tu, Le Hiress, Huertas, and Guignabert were responsible for conception and design; all authors contributed to the analysis and interpretation; and Drs Ricard, Huertas, and Guignabert drafted the manuscript.
Sources of FundingThis research was supported by grants from the French National Institute for Health and Medical Research and French National Agency for Research grant ANR_12_JSV1_0004_01.
DisclosuresNone.
References 1. Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin
V, Yaïci A, Weitzenblum E, Cordier JF, Chabot F, Dromer C, Pison C, Reynaud-Gaubert M, Haloun A, Laurent M, Hachulla E, Cottin V, Degano B, Jaïs X, Montani D, Souza R, Simonneau G. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hyper-tension in the modern management era. Circulation. 2010;122:156–163.
2. Voelkel NF, Gomez-Arroyo J, Abbate A, Bogaard HJ, Nicolls MR. Pathobiology of pulmonary arterial hypertension and right ventricular failure. Eur Respir J. 2012;40:1555–1565.
3. Orlidge A, D’Amore PA. Inhibition of capillary endothelial cell growth by pericytes and smooth muscle cells. J Cell Biol. 1987;105:1455–1462.
4. Stark K, Eckart A, Haidari S, Tirniceriu A, Lorenz M, von Brühl ML, Gärtner F, Khandoga AG, Legate KR, Pless R, Hepper I, Lauber K, Walzog B, Massberg S. Capillary and arteriolar pericytes attract innate leukocytes exiting through venules and “instruct” them with pattern-recognition and motility programs. Nat Immunol. 2013;14:41–51.
5. Nehls V, Drenckhahn D. Heterogeneity of microvascular pericytes for smooth muscle type alpha-actin. J Cell Biol. 1991;113:147–154.
6. Krautler NJ, Kana V, Kranich J, Tian Y, Perera D, Lemm D, Schwarz P, Armulik A, Browning JL, Tallquist M, Buch T, Oliveira-Martins JB, Zhu C, Hermann M, Wagner U, Brink R, Heikenwalder M, Aguzzi A. Follicular dendritic cells emerge from ubiquitous perivascular precursors. Cell. 2012;150:194–206.
7. Joyce NC, DeCamilli P, Boyles J. Pericytes, like vascular smooth muscle cells, are immunocytochemically positive for cyclic GMP-dependent pro-tein kinase. Microvasc Res. 1984;28:206–219.
8. Kelley C, D’Amore P, Hechtman HB, Shepro D. Microvascular pericyte contractility in vitro: comparison with other cells of the vascular wall. J Cell Biol. 1987;104:483–490.
9. Meyrick B, Fujiwara K, Reid L. Smooth muscle myosin in precursor and mature smooth muscle cells in normal pulmonary arteries and the effect of hypoxia. Exp Lung Res. 1981;2:303–313.
10. Sims DE. Diversity within pericytes. Clin Exp Pharmacol Physiol. 2000;27:842–846.
11. Nayak RC, Berman AB, George KL, Eisenbarth GS, King GL. A mono-clonal antibody (3G5)-defined ganglioside antigen is expressed on the cell surface of microvascular pericytes. J Exp Med. 1988;167:1003–1015.
12. Armulik A, Abramsson A, Betsholtz C. Endothelial/pericyte interactions. Circ Res. 2005;97:512–523.
13. Tu L, Dewachter L, Gore B, Fadel E, Dartevelle P, Simonneau G, Humbert M, Eddahibi S, Guignabert C. Autocrine fibroblast growth factor-2 signal-ing contributes to altered endothelial phenotype in pulmonary hyperten-sion. Am J Respir Cell Mol Biol. 2011;45:311–322.
14. El-Bizri N, Guignabert C, Wang L, Cheng A, Stankunas K, Chang CP, Mishina Y, Rabinovitch M. SM22alpha-targeted deletion of bone morpho-genetic protein receptor 1A in mice impairs cardiac and vascular develop-ment, and influences organogenesis. Development. 2008;135:2981–2991.
15. Guignabert C, Raffestin B, Benferhat R, Raoul W, Zadigue P, Rideau D, Hamon M, Adnot S, Eddahibi S. Serotonin transporter inhibition prevents and reverses monocrotaline-induced pulmonary hypertension in rats. Circulation. 2005;111:2812–2819.
16. Izikki M, Guignabert C, Fadel E, Humbert M, Tu L, Zadigue P, Dartevelle P, Simonneau G, Adnot S, Maitre B, Raffestin B, Eddahibi S. Endothelial-derived FGF2 contributes to the progression of pulmonary hypertension in humans and rodents. J Clin Invest. 2009;119:512–523.
17. Guignabert C, Tu L, Izikki M, Dewachter L, Zadigue P, Humbert M, Adnot S, Fadel E, Eddahibi S. Dichloroacetate treatment partially regresses estab-lished pulmonary hypertension in mice with SM22alpha-targeted overex-pression of the serotonin transporter. FASEB J. 2009;23:4135–4147.
18. Ricard N, Bidart M, Mallet C, Lesca G, Giraud S, Prudent R, Feige JJ, Bailly S. Functional analysis of the BMP9 response of ALK1 mutants from HHT2 patients: a diagnostic tool for novel ACVRL1 mutations. Blood. 2010;116:1604–1612.
19. Guignabert C, Alvira CM, Alastalo TP, Sawada H, Hansmann G, Zhao M, Wang L, El-Bizri N, Rabinovitch M. Tie2-mediated loss of per-oxisome proliferator-activated receptor-gamma in mice causes PDGF receptor-beta-dependent pulmonary arterial muscularization. Am J Physiol Lung Cell Mol Physiol. 2009;297:L1082–L1090.
20. Tigges U, Komatsu M, Stallcup WB. Adventitial pericyte progenitor/mes-enchymal stem cells participate in the restenotic response to arterial injury. J Vasc Res. 2013;50:134–144.
21. Masri FA, Xu W, Comhair SA, Asosingh K, Koo M, Vasanji A, Drazba J, Anand-Apte B, Erzurum SC. Hyperproliferative apoptosis-resistant endo-thelial cells in idiopathic pulmonary arterial hypertension. Am J Physiol Lung Cell Mol Physiol. 2007;293:L548–L554.
22. Tu L, De Man FS, Girerd B, Huertas A, Chaumais MC, Lecerf F, François C, Perros F, Dorfmüller P, Fadel E, Montani D, Eddahibi S, Humbert M, Guignabert C. A critical role for p130Cas in the progression of pulmo-nary hypertension in humans and rodents. Am J Respir Crit Care Med. 2012;186:666–676.
23. Savale L, Tu L, Rideau D, Izziki M, Maitre B, Adnot S, Eddahibi S. Impact of interleukin-6 on hypoxia-induced pulmonary hypertension and lung inflammation in mice. Respir Res. 2009;10:6.
24. Steiner MK, Syrkina OL, Kolliputi N, Mark EJ, Hales CA, Waxman AB. Interleukin-6 overexpression induces pulmonary hypertension. Circ Res. 2009;104:236–44, 28p following 244.
25. Enge M, Bjarnegård M, Gerhardt H, Gustafsson E, Kalén M, Asker N, Hammes HP, Shani M, Fässler R, Betsholtz C. Endothelium-specific platelet-derived growth factor-B ablation mimics diabetic retinopathy. EMBO J. 2002;21:4307–4316.
26. Lindahl P, Johansson BR, Levéen P, Betsholtz C. Pericyte loss and microan-eurysm formation in PDGF-B-deficient mice. Science. 1997;277:242–245.
27. Shen J, Vil MD, Prewett M, Damoci C, Zhang H, Li H, Jimenez X, Deevi DS, Iacolina M, Kayas A, Bassi R, Persaud K, Rohoza-Asandi A, Balderes P, Loizos N, Ludwig DL, Tonra J, Witte L, Zhu Z. Development of a fully human anti-PDGFRbeta antibody that suppresses growth of human tumor xenografts and enhances antitumor activity of an anti-VEGFR2 antibody. Neoplasia. 2009;11:594–604.
28. Pitulescu ME, Schmidt I, Benedito R, Adams RH. Inducible gene target-ing in the neonatal vasculature and analysis of retinal angiogenesis in mice. Nat Protoc. 2010;5:1518–1534.
29. Graham BB, Chabon J, Gebreab L, Poole J, Debella E, Davis L, Tanaka T, Sanders L, Dropcho N, Bandeira A, Vandivier RW, Champion HC, Butrous G, Wang XJ, Wynn TA, Tuder RM. Transforming growth factor-β signaling promotes pulmonary hypertension caused by Schistosoma man-soni. Circulation. 2013;128:1354–1364.
30. Long L, Crosby A, Yang X, Southwood M, Upton PD, Kim DK, Morrell NW. Altered bone morphogenetic protein and transforming growth
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

Ricard et al Pericytes in Pulmonary Arterial Hypertension 1597
factor-beta signaling in rat models of pulmonary hypertension: potential for activin receptor-like kinase-5 inhibition in prevention and progression of disease. Circulation. 2009;119:566–576.
31. Ma W, Han W, Greer PA, Tuder RM, Toque HA, Wang KK, Caldwell RW, Su Y. Calpain mediates pulmonary vascular remodeling in rodent models of pulmonary hypertension, and its inhibition attenuates pathologic fea-tures of disease. J Clin Invest. 2011;121:4548–4566.
32. Mata-Greenwood E, Meyrick B, Steinhorn RH, Fineman JR, Black SM. Alterations in TGF-beta1 expression in lambs with increased pulmonary blood flow and pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol. 2003;285:L209–L221.
33. Schrimpf C, Duffield JS. Mechanisms of fibrosis: the role of the pericyte. Curr Opin Nephrol Hypertens. 2011;20:297–305.
34. Carmeliet P, Jain RK. Molecular mechanisms and clinical applications of angiogenesis. Nature. 2011;473:298–307.
35. Greenberg JI, Shields DJ, Barillas SG, Acevedo LM, Murphy E, Huang J, Scheppke L, Stockmann C, Johnson RS, Angle N, Cheresh DA. A role for VEGF as a negative regulator of pericyte function and vessel maturation. Nature. 2008;456:809–813.
36. Burgos A, Kaplan R, Rodriguez N, Meza V, Morelatto R, Piccinni D. Malignant melanoma of the oral cavity (in Spanish). Rev Fac Cien Med Univ Nac Cordoba. 2008;65:70–3.
37. Díaz-Flores L, Gutiérrez R, Madrid JF, Varela H, Valladares F, Acosta E, Martín-Vasallo P, Díaz-Flores L Jr. Pericytes. Morphofunction, interac-tions and pathology in a quiescent and activated mesenchymal cell niche. Histol Histopathol. 2009;24:909–969.
38. Ghofrani HA, Morrell NW, Hoeper MM, Olschewski H, Peacock AJ, Barst RJ, Shapiro S, Golpon H, Toshner M, Grimminger F, Pascoe S. Imatinib in pulmonary arterial hypertension patients with inadequate response to established therapy. Am J Respir Crit Care Med. 2010;182:1171–1177.
39. Humbert M. Impression, sunset. Circulation. 2013;127:1098–1100. 40. Schermuly RT, Dony E, Ghofrani HA, Pullamsetti S, Savai R, Roth M,
Sydykov A, Lai YJ, Weissmann N, Seeger W, Grimminger F. Reversal of experimental pulmonary hypertension by PDGF inhibition. J Clin Invest. 2005;115:2811–2821.
41. Bergers G, Song S, Meyer-Morse N, Bergsland E, Hanahan D. Benefits of targeting both pericytes and endothelial cells in the tumor vasculature with kinase inhibitors. J Clin Invest. 2003;111:1287–1295.
42. Pietras K, Pahler J, Bergers G, Hanahan D. Functions of paracrine PDGF signaling in the proangiogenic tumor stroma revealed by pharmacological targeting. PLoS Med. 2008;5:e19.
43. Ruan J, Luo M, Wang C, Fan L, Yang SN, Cardenas M, Geng H, Leonard JP, Melnick A, Cerchietti L, Hajjar KA. Imatinib disrupts lymphoma angiogenesis by targeting vascular pericytes. Blood. 2013;121:5192–5202.
44. Virgintino D, Girolamo F, Errede M, Capobianco C, Robertson D, Stallcup WB, Perris R, Roncali L. An intimate interplay between preco-cious, migrating pericytes and endothelial cells governs human fetal brain angiogenesis. Angiogenesis. 2007;10:35–45.
45. de Man FS, Tu L, Handoko ML, Rain S, Ruiter G, François C, Schalij I, Dorfmüller P, Simonneau G, Fadel E, Perros F, Boonstra A, Postmus PE, van der Velden J, Vonk-Noordegraaf A, Humbert M, Eddahibi S, Guignabert C. Dysregulated renin-angiotensin-aldosterone system contributes to pulmo-nary arterial hypertension. Am J Respir Crit Care Med. 2012;186:780–789.
46. Eddahibi S, Guignabert C, Barlier-Mur AM, Dewachter L, Fadel E, Dartevelle P, Humbert M, Simonneau G, Hanoun N, Saurini F, Hamon M, Adnot S. Cross talk between endothelial and smooth muscle cells in pul-monary hypertension: critical role for serotonin-induced smooth muscle hyperplasia. Circulation. 2006;113:1857–1864.
47. Xu W, Erzurum SC. Endothelial cell energy metabolism, proliferation, and apoptosis in pulmonary hypertension. Compr Physiol. 2011;1:357–372.
48. Christman BW, McPherson CD, Newman JH, King GA, Bernard GR, Groves BM, Loyd JE. An imbalance between the excretion of thrombox-ane and prostacyclin metabolites in pulmonary hypertension. N Engl J Med. 1992;327:70–75.
49. Giaid A, Yanagisawa M, Langleben D, Michel RP, Levy R, Shennib H, Kimura S, Masaki T, Duguid WP, Stewart DJ. Expression of endothelin-1 in the lungs of patients with pulmonary hypertension. N Engl J Med. 1993;328:1732–1739.
50. Miyata M, Sakuma F, Yoshimura A, Ishikawa H, Nishimaki T, Kasukawa R. Pulmonary hypertension in rats. 2. Role of interleukin-6. Int Arch Allergy Immunol. 1995;108:287–291.
51. Golembeski SM, West J, Tada Y, Fagan KA. Interleukin-6 causes mild pul-monary hypertension and augments hypoxia-induced pulmonary hyper-tension in mice. Chest. 2005;128(Suppl 6):572S–573S.
52. Chen S, Lechleider RJ. Transforming growth factor-beta-induced differ-entiation of smooth muscle from a neural crest stem cell line. Circ Res. 2004;94:1195–1202.
53. Song S, Ewald AJ, Stallcup W, Werb Z, Bergers G. PDGFRbeta+ peri-vascular progenitor cells in tumours regulate pericyte differentiation and vascular survival. Nat Cell Biol. 2005;7:870–879.
54. Ding R, Darland DC, Parmacek MS, D’Amore PA. Endothelial-mesenchymal interactions in vitro reveal molecular mechanisms of smooth muscle/peri-cyte differentiation. Stem Cells Dev. 2004;13:509–520.
55. Thanabalasundaram G, Schneidewind J, Pieper C, Galla HJ. The impact of pericytes on the blood-brain barrier integrity depends critically on the peri-cyte differentiation stage. Int J Biochem Cell Biol. 2011;43:1284–1293.
56. Qiao L, Nishimura T, Shi L, Sessions D, Thrasher A, Trudell JR, Berry GJ, Pearl RG, Kao PN. Endothelial fate-mapping in mice with pulmonary hyperten-sion. Circulation. November 7, 2013. doi:10.1161/CIRCULATIONAHA. 113.003734. http//:circ.ahajournals.org/. Accessed February 3, 2014.
57. Patel MS, Taylor GP, Bharya S, Al-Sanna’a N, Adatia I, Chitayat D, Suzanne Lewis ME, Human DG. Abnormal pericyte recruitment as a cause for pulmonary hypertension in Adams-Oliver syndrome. Am J Med. Genet A. 2004;129A:294–299.
58. Baskar S, Kulkarni ML, Kulkarni AM, Vittalrao S, Kulkarni PM. Adams-Oliver syndrome: Additions to the clinical features and possible role of BMP pathway. Am J Med. Genet A. 2009;149A:1678–1684.
CLINICAL PERSPECTIVEPulmonary vascular remodeling, occurring mostly in the small to midsized pulmonary arterioles (<500 μm), is a hallmark of most forms of pulmonary hypertension and frequently leads to progressive functional decline in patients despite treatment with currently available therapies. In the present study, to the best of our knowledge, we report for the first time increased pericyte coverage of distal pulmonary arteries in experimental (in chronic hypoxia and monocrotaline-induced pulmonary hypertension) and human (patients carrying or not a bone morphogenetic protein receptor 2 mutation) pulmonary arterial hypertension (PAH), an abnormality that is a potential source of smooth muscle–like cells involved in the PAH pulmonary vascular remodeling. We obtained evidence that dysfunctional endothelial cells from patients with idiopathic PAH, through an aberrant release of key growth factors and chemoattractants (ie, fibroblast growth factor-2 and interleukin-6), contrib-ute to this vascular abnormality. In vitro, we found that exogenous or endothelial-derived fibroblast growth factor-2 and interleukin-6 enhance pulmonary pericyte migration and that fibroblast growth factor-2 is also a pericyte mitogen. In addi-tion, we demonstrated, in human lungs from patients with PAH and in a murine model of pulmonary hypertension, that these pericytes can differentiate into smooth muscle–like cells, expressing contractile proteins. We also found that transforming growth factor-β1 is overactivated in pulmonary pericytes from patients with idiopathic PAH and promotes human pulmonary pericyte differentiation into contractile smooth muscle–like cells. We thus suspect that neutralization of fibroblast growth factor-2, interleukin-6, and transforming growth factor-β1 may prevent pericyte recruitment and differentiation in idiopathic and heritable PAH and thus may be beneficial against the disease progression. Additional investigations are required to deter-mine whether pulmonary pericytes contribute to other forms of pulmonary hypertension.
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from

Supplemental material – Ricard et al.
1
SUPPLEMENTAL MATERIAL
Increased Pericyte Coverage Mediated By Endothelial Derived FGF-2 and IL-6 is a Source of Smooth Muscle-like Cells in Pulmonary Hypertension
Running title: Ricard et al.; Pericytes in pulmonary arterial hypertension
Nicolas Ricard1,2, Ly Tu1,2, Morane Le Hiress1,2, Alice Huertas1,2,3, Carole Phan1,2,
Raphaël Thuillet1,2, Caroline Sattler1,2,3, Elie Fadel1,2, Andrei Seferian1,2,3, David Montani1,2, Peter Dorfmüller1,2, Marc Humbert1,2,3, Christophe Guignabert1,2.
1INSERM UMR_S 999, LabEx LERMIT, Centre Chirurgical Marie Lannelongue, Le Plessis-
Robinson, France; 2Univ Paris-Sud, School of medicine, Kremlin-Bicêtre, France; 3AP-HP, Service de Pneumologie, Centre de Référence de l’Hypertension Pulmonaire Sévère,
DHU Thorax Innovation, Hôpital de Bicêtre, France.
SUPPLEMENTAL METHODS
1. Functional analyses of human pulmonary pericytes
a. Conditioned media from human pulmonary endothelial cells (ECs)
ECs were seeded in 6-well plates (200,000 cells per well) overnight. Cells were then washed
and incubated with 1mL of basic pericyte medium supplemented with 0.3% fetal calf serum
(FCS) for 24h. Conditioned media were then centrifuged and supernatants were stocked at -
80°C until use.
b. Migration assay
Gelatin-coated inserts with 8 µM pore size (BD Biosciences, Le Pont de Claix, France) were
used. 50,000 pulmonary pericytes were plated in the upper well of the insert in complete
pericyte culture medium (Clinisciences) overnight and then starved for 1h. The lower
chambers were then filled with conditioned medium from ECs or pericyte culture medium
(Clinisciences) supplemented with 0.3% FCS and human recombinant PDGF-BB (100ng/mL)
(R&D Systems) or FGF-2 (10ng/mL) (Sigma-Aldrich) or IL-6 (10ng/mL) with IL-6R (2.5
ng/mL) (Peprotech, Neuilly-sur-Seine, France), with, when indicated, neutralizing antibody

Supplemental material – Ricard et al.
2
against IL-6 (Peprotech) or against FGF-2 (Millipore) preincubated 30 min at 37°C. IL-6R is
important for the binding of IL-6 to its membrane-bound gp130. Therefore, the use of IL-6R
in conjunction with IL-6 has been used for our in vitro and in vivo. After 6 h, the inserts were
removed and inner side was wiped with cotton swaps. Migrated cells were stained with
Crystal violet (Wescor, Utah, USA) and DAPI (Life technologies) for counting.
c. Proliferation assay
Pericyte proliferation was assessed using Delfia cell proliferation kit (Perkin Elmer). 5,000
pulmonary pericytes were seeded in each well of a 96 wells plate in complete pericyte culture
medium (Clinisciences) for 6 h and starved overnight. Medium was then replaced with
conditional medium from ECs or pericyte culture medium (Clinisciences) supplemented with
0.3% FCS and human recombinent FGF-2 (10ng/mL) (Sigma-Aldrich) or IL-6 (10ng/mL)
with IL-6R (2.5 ng/mL) (Peprotech) or 10% FCS, with, when indicated, neutralizing antibody
against IL-6 (Peprotech) or against FGF-2 (Millipore) preincubated 30 min at 37°C.
For Cyclin D1 Western blotting, pericytes were seeded in complete medium and then starved
overnight. Medium was then replaced with basic pericyte medium (Clinisciences)
supplemented with 0.3% FCS and human recombinant FGF-2 (Sigma-Aldrich) or IL-6 with
IL-6R (Peprotech) at the indicating doses or 10% FCS for 24h. Cells were then lysed and
equal quantities of proteins were loaded on Nu-Page Tris-Acetate Mini Gels (Life
technologies). Proteins were then transferred on nitrocellulose membrane and incubated with
anti Cyclin D1 antibody (Ozyme, Saint-Quentin-en-Yveline, France). Normalization was
done using anti-β-actin antibody (Sigma-Aldrich). Acquisition was done using ChemiDoc
XRS+ (BioRad, Marnes-la-Coquette, France) and quantification with ImageLab software
(Biorad).

Supplemental material – Ricard et al.
3
d. In vitro pericyte differentiation
Pericytes were seeded in complete medium overnight. Complete medium was then replaced
with basic pericyte medium supplemented with 1% FCS and TGF-β1 (1 or 10ng/mL)
(Peprotech) or IL-6 (10 or 100ng/mL) with IL-6R (2.5 or 25ng/mL) (Peprotech) or FGF-2 (1
or 10ng/mL) (Sigma-Aldrich) for 24h. For immunocytochemistry, cells were fixed with cold
methanol and labeled using anti-SM22 (Clinisciences) or anti-calponin (Clinisciences) or anti-
α-SM actin (Clinisciences) antibodies. For Western blotting, cells were then lysed and equal
quantities of proteins were loaded on a Nu-Page Tris-Acetate Mini Gels (Life technologies).
Proteins were then transferred on nitrocellulose membrane and incubated with anti-SM22
(Clinisciences) or anti-Calponin (Clinisciences) or anti-α-SM actin (Clinisciences) antibodies.
Normalization was done using anti-β-actin antibody (Sigma-Aldrich). Acquisition was done
using ChemiDoc XRS+ (BioRad) and quantification with ImageLab software (Biorad).
2. Gelatin Zymography and Immunostaining
a. Gelatin Zymography
Conditioned media collected from the upper compartments of the Boyden Chambers to
evaluate production of MMPs in pulmonary pericytes migrating in response to EC
conditioned media were used for gelatin zymography. The supernatants were subjected to
electrophoresis in an 8% SDS-PAGE gel co-polymerized with gelatin (1 mg/ml, Sigma-
Aldrich). The gelatinolytic activities were detected as transparent bands against the
background of Coomassie Brilliant Blue-stained gelatin.
b. Immunostaining
Paraffin sections of rat lung were stained with 3G5 antibody, prepared from murine
hybridoma (ATCC) (overnight 4°C) followed by staining using vectastain ABC (Abcys,
Courtaboeuf, France) according to the manufacturer’s instructions and counterstained with

Supplemental material – Ricard et al.
4
Hematoxylin and Eosin (Sigma-aldrich). Representative images were taken with Eclipse 80i
microscope (Nikon) and vessel sizes were measured using NIS_Elements BR 2.30 software.
Cryosections or paraffin sections of human, rat or mouse lung were labelled with anti-3G5,
prepared from murine hybridoma (ATCC), anti-CD31, anti-vimentin, anti-SM22
(Clinisciences), anti-NG2 (Abcam), anti-α-SM-actin (Clinisciences), anti-phosphorylated-
Smad2 (Ozyme), anti PCNA (Dako, Les Ulis, France), anti-α-SM-actin AlexaFluor 700
conjugated (R&D systems) antibodies, followed by corresponding secondary fluorescent-
labeled antibodies (Interchim). Nucleus were labelled using DAPI (Life technologies).
Mounting was done using ProLong Gold antifade reagent (Life technologies). Images were
taken using LSM700 confocal microscope (Zeiss).
3. Flow cytometry analyses
Mouse lungs were digested by Collagenase type I (Gibco, Life Technologies). Cells in
homogenate were fixed and permeabilized using IntraPrep reagents (Beckman Coulter,
Villepinte, France) according to the manufacturer’s instructions. Cells were then incubated
with anti-α-SM-actin AlexaFluor 700 conjugated antibody (R&D systems) according to the
manufacturer’s instructions. Flow cytometry was performed on a MACSQuant analyser
(Miltenyi, Paris, France). The data were analyzed using MACSQuantify (Miltenyi).

Supplemental material – Ricard et al.
5
SUPPLEMENTAL TABLE
PAH n=13 Control n=10 Age, yrs 37.6 ± 3.58 55.7 ± 6.54 Sex, M/F ratio 0.63 0.2 Mutation in BMPR2 gene, n Carrier No-‐carrier
5 8
NA NA
NYHA functional class, n Class I Class II Class III Class IV
0 7 5 1
NA NA NA NA
6-‐MWD, m 426 ± 54.14 NA mPAP, mmHg 66 ± 6.47 NA CI, L/min/m² 3.1 ± 0.56 NA PVR mmHg/L/min 12.7 ± 1.67 NA PCWP, mmHg 10 ± 1.42 NA Specific PAH therapy ERA PDE5i Prostanoids CCB No treatment
13 13 13 0 0
NA NA NA NA NA
Supplemental table 1: Characteristics of controls and patients with PAH before lung transplantation. CI=cardiac index; mPAP=mean pulmonary artery pressure; NA= no applicable; NYHA=New York Heart association; PCWP=pulmonary capillary wedge pressure; PVR= pulmonary vascular resistance
SUPPLEMENTAL FIGURES

Human
Rat
A
B
Merged CD31 3G5
DAPI
CD31 NG2
DAPI
Merged
Merged
Merged
Merged CD31 NG2
DAPI
Merged CD31 3G5
DAPI
CD31 NG2
DAPI
Merged Merged CD31 3G5
DAPI
CD31 NG2
DAPI
CD31 3G5
DAPI
Supplemental Fig. S1: Colocalization of 3G5 and NG2 in human and rat lungs. NG2 (white) and 3G5 (red) colocalized in (A) human and (B) rat lungs. Scale bar = 50 µm in all sections.

iPAH hPAH 0
5
10
15
20
Per
icyt
e nu
mbe
r per
ves
sel
≤100 101-199 ≥200
Vessel diameter (µm)
Supplemental Fig. S2: Pericyte coverage in pulmonary arteries is not significantly different between idiopathic (iPAH) and heritable (hPAH) PAH. Bar graph represents medians of 15 vessels per vessel size category and per subject (n=8 iPAH subjects and n=5 hPAH patients).
iPAH hPAH iPAH hPAH

d
3G5 CD31 DAPI
DIC
c
b a
f e
3G5 CD31 DAPI
DIC
3G5 CD31 DAPI
DIC
3G5 CD31 DAPI
DIC
3G5 CD31 DAPI
DIC
3G5 CD31 DAPI
DIC
PAH
Supplemental Fig. S3: Localisation of 3G5 positive cells in different forms and degrees of pulmonary vascular remodeling in PAH patients: mild (a, b), severe (c, d), occluded (e, f). Scale bar = 50µm in all sections.

0
10
20
30
40
RVS
P (m
m H
g)
Supplemental Fig. S4: Values of right ventricular systolic pressures (RVSP) of NG2DsRedBAC mice exposed to hypoxia (10% fiO2) or kept in room air for 3 weeks. Bar graph represents medians. n = 5 mice. * p-value < 0.05 , ** p-value < 0.01 compared with mice kept in room air.
Normoxia
Chronic Hypoxia
Day-2 Day-7 Day-14 Day-21
* **

NG2 3G5 α-SM actin CD31
Endo
thel
ial c
ells
Pe
ricyt
es
A
B
Supplemental Fig. S5: Caracterisation of cultured human pulmonary pericytes. A: Representative images of primary cultured human pulmonary pericytes. Pericytes are positive for pericytic markers NG2 and 3G5 and negative for smooth muscle cell marker α-SM-actin and for endothelial cell markers CD31. B: Representative images of colocalization of NG2 and 3G5 on primary cultured human pulmonary pericytes. Scale bar = 20 µm in all sections.

0
0,1
0,2
0,3
0,4
0,5
Per
icyt
e nu
mbe
r / b
ranc
hing
poi
nt
* *
PBS IL-6/IL-6R FGF-2
PBS IL-6/IL-6R FGF-2
Supplemental Fig. S6: FGF-2 and IL-6 increase pericyte coverage in vivo in mice retinal angiogenesis model. Representative images of pericytes (NG2 positive cells in red, white arrowheads) and endothelial cells (Isolectin B4 positive cells in green) of retina from 5 days old mice treated with IL-6 (10 ng) with IL-6R (2.5 ng) or FGF-2 (10 ng). Bar graph represents medians of 8 images per mice (n = 4-5 mice from 2 litters). * p-value < 0.05 compared with PBS. Scale bar = 50 µm in all sections.

α-SM-actin 3G5 CD31 DAPI
α-SM-actin CD31 DAPI
3G5 SM22 DAPI
SM22 DAPI
A
B
Supplemental Fig. S7: Pulmonary pericytes present a non-contractile phenotype in control subjects. Representation images of 3G5, α-SM-actin (upper panel) and SM22 (lower panel) on human pulmonary tissue from control subjects. 3G5 positive cells (red) are negative for α-SM-actin (white, upper panel) and SM22 (green, lower panel). Scale bar = 20 µm in all sections.

DsR
ed
NG2-DsRed mice:
SS
C
FSC
WT mice:
DsR
ed
α-S
M-a
ctin
α-
SM
-act
in
FSC
2,75%
7,10%
FSC
Chronic Hypoxia
Normoxia
Day-21
SS
C
FSC
A
B
Supplemental Fig. S8: Flow cytometry gating strategy for the analysis of α-SM-acting staining in pericytes from NG2DsRed mice. A: No DsRed+ cells were detected in lungs of wild-type (WT) mice. B: Gating of DsRed positive cells from NG2DsRedBAC mice and analyses of α-SM-actin staining in DsRed+ cells.

* #
# *
*
*
#
#
NG2-DsRed DAPI α-SM-actin
NG2DsRed mice
Chronic Hypoxia Day-14
Chronic Hypoxia Day-21
Supplemental Fig. S9: Pulmonary pericytes are a source of contractile smooth muscle-like cells in remodeled pulmonary arteries in chronically hypoxic NG2DsRedBAC mice. Representative images of α-SM-actin staining in pulmonary arteries from NG2DsRedBAC exposed to chronic hypoxia. Scale bar = 50 µm.

and Christophe GuignabertCaroline Sattler, Elie Fadel, Andrei Seferian, David Montani, Peter Dorfmüller, Marc Humbert
Nicolas Ricard, Ly Tu, Morane Le Hiress, Alice Huertas, Carole Phan, Raphaël Thuillet,Hypertension
Like Cells in Pulmonary−Factor-2 and Interleukin-6 Is a Source of Smooth Muscle Increased Pericyte Coverage Mediated by Endothelial-Derived Fibroblast Growth
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2014 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.113.007469
2014;129:1586-1597; originally published online January 30, 2014;Circulation.
http://circ.ahajournals.org/content/129/15/1586World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2014/01/30/CIRCULATIONAHA.113.007469.DC1.htmlData Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on January 16, 2015http://circ.ahajournals.org/Downloaded from