Embed Size (px)
Citation preview

HYPOGLYCEMIA MANAGEMENT IN THE EMERGENCY DEPARTMENT
Silu Zuo, Pharm.D.
PGY1 Pharmacy Resident
UW Medicine

Patient Case
CC: JT is a 53 y/o female presenting to ED with profound hypoglycemia and unresponsiveness during nuclear medicine study
HPI: Progressive hypoglycemia over past several
years, at times resulting in loss of consciousness Recent CT scan showed possible neuroendocrine
tumor on pancreas nuclear medicine study to further assess
At nuclear medicine, was unresponsive with BG of 20

Patient Case
PMH: Epilepsy, complex partial Turner's syndrome Hypoglycemia Osteoporosis Macrocytic anemia

Patient Case
Medications: Alendronate 70 mg PO Q7 days Benztropine 0.5 mg PO BID Carbamazepine 400 mg PO BID Depakote 500 mg PO EC BID Glucagon 1mg Injection PRN hypoglycemia Glucose 40% oral gel 15 gram tube PO PRN
hypoglycemia Olanzapine 15 mg PO QHS Potassium chloride ER 20 MEQ PO daily Sertraline Hcl 100mg PO daily Topiramate 25 mg PO BID

Patient Case
Vitals BP 102/53 HR 88 RR 18 SpO2 100% RA
To be continued….

Glucose Homeostasis

Glucose Homeostasis
↓ blood glucose
↑ blood glucose

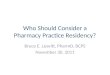
Glucose Homeostasis
The pancreas is a major player Alpha cells: secrete glucagon Beta cells: secrete insulin Delta cells: secrete somatostatin
Important role in maintaining balance of both insulin and glucagon
Other counter-regulatory hormones Adrenaline (epinephrine) Cortistol

Glucose Homeostasis

Hypoglycemia
Normal blood glucose (fasting): 70-110 mg/dL
Small excursions above range post-prandially
Hypoglycemia – “Whipple’s triad” 1) Symptoms consistent with hypoglycemia 2) Low plasma glucose concentration (<70
mg/dL) 3) Relief of those symptoms after the
plasma glucose level is raised
Harper's Illustrated Biochemistry, 29e. New York, NY: McGraw-Hill; 2012.

Hypoglycemia

Hypoglycemia
Hypoglycemia can be very dangerous if untreated Brain cannot make glucose or store very
much glycogen requires a continuous supply of glucose from blood circulation
Serious hypoglycemia Seizure, loss of consciousness, coma, death
Harrison's Principles of Internal Medicine, 18e. New York, NY: McGraw-Hill; 2012.

Hypoglycemia
Causes Drugs
Insulin or insulin secretagogue, alcohol Gatifloxacin (removed from market), pentamidine,
quinine, indomethacin, others Critical illness
Hepatic, renal or cardiac failure, sepsis Hormone deficiency
Cortisol, glucagon, epinephrine (in insulin-deficient diabetes)
Non–islet cell tumor
J Clin Endocrinol Metab 94:709, 2009.

Hypoglycemia
Causes Endogenous hyperinsulinism
Insulinoma Functional beta-cell disorder
(noninsulinoma pancreatogenous hypoglycemia, post gastric bypass)
Insulin or insulin receptor antibody Insulin autoimmune hypoglycemia
Accidental, surreptitious, or malicious hypoglycemia
J Clin Endocrinol Metab 94:709, 2009.

Treatment
Oral carbohydrate replacement IV glucose/dextrose Glucagon Octreotide Diazoxide

UWMC Hypoglycemia Protocol

UWMC Hypoglycemia Protocol

UWMC Hypoglycemia Protocol

Oral Carbohydrates
Glucose 15-20 g orally – preferred initial treatment in conscious individual with hypoglycemia
Examples of 15 g of carbohydrates: 4 ounces of juice 4 ounces of nondiet soda 8 ounces of skim milk 3-4 glucose tablets 5-6 Life Savers candies
After treatment, eat snack with protein/fat to prevent recurrence
Clinical Diabetes 2012 Jan;30(1):38

IV Glucose/Dextrose
“IV glucose” = IV dextrose 50% (50g/100mL) Dose = 12.5-25 g (25 g/50 mL = 1 amp) IV
push Dextrose 5%, 10%, 20%, 30%, 40%, 50%,
70% 5-10% can give via peripheral IV
10% at fast rate may cause irritation and ↑ risk of extravasation
Concentrations >10% (hypertonic) may cause thrombosis if infused via peripheral veins administer via central line
AVOID extravasation (vesicant)
UpToDate.

Glucagon
Dose: 1 mg IV/IM/SQ, may repeat in 15 mins
IV dextrose should be administered as soon as it is available; if patient fails to respond to glucagon, IV dextrose must be given.
Role: patients without IV access (especially severe hypoglycemia, unconscious patients
Glucagon Emergency KitGlucagon HypoKitGlucaGen HypoKit (glucagon) [prescribing information]. Glucagon Emergency Kit [prescribing information].

Patient, Case Cont’d
Time
Blood Glucose
Notes
1214 165 After IV glucose 12.5 g
1250 17 D50% 12.5 g, D5/NS 100 mL/hr
1326 76
1348 33 D50% 12.5 g
1413 168
1428 134
1452 107
1536 99
1600 114 Central line placed, D10 100 mL/hr

Octreotide
Somatostatin analogue Provides more potent inhibition of growth
hormone, glucagon, and insulin as compared to endogenous somatostatin
May reduce recurrent hypoglycemia as with dextrose-alone therapy
Should be used with IV dextrose/oral carbohydrates
Dose: (ideal dose not well established) SQ: 50-100 mcg, repeat every 6 hours PRN IV: up to 125 mcg/hour has been usedPharmacol Rev. 2003 Mar;55(1):105-31.
Ann Emerg Med, 2000, 36(2):133-6.

Octreotide
Design Prospective, double-blind, placebo-controlled trial
Patients • 40 adult patients presenting to ED with hypoglycemia (BG≤60 mg/dL)• Taking a sulfonylurea or a combination of insulin and sulfonylurea• Admitted to hospital for at least 24 hrs• Exclusions: pregnancy, not taking insulin/SU
Intervention/Comparator
Intervention (N=22)Standard treatment (1 ampule of 50% dextrose IV and oral carbs) + 1 dose of octreotide 75 mcg SQ
Comparator (N=18)Standard treatment + placebo (1 mL of 0.9% NS SQ)
Ann Emerg Med 2008; 51(4):400-406.

Octreotide
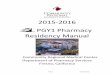
Results
Reduced rate of recurrent hypoglycemia
Ann Emerg Med 2008; 51(4):400-406.

Octreotide
Warnings/precautions: Cholelithiasis – may inhibit gallbladder
contractility Glucose regulation Hypothyroidism – may suppress TSH
secretion Pancreatitis – may change absorption of
fats Adverse effects: bradycardia, dizziness,
hyperglycemia, diarrhea, constipation
Sandostatin [prescribing information].

Diazoxide
Antidote for hypoglycemia due to hyperinsulinemia; vasodilator
Opens ATP-dependent K+ channels on pancreatic beta cells hyperpolarization of the beta cell inhibition of insulin release
Binds to a different site on the potassium channel than the sulfonylureas
Dose: 3-8 mg/kg/day PO in divided doses Q8H Starting dose 3 mg/kg/day PO divided in 2-
3 doses

Diazoxide
No randomized, controlled studies Few case reports
Pentamidine-induced hypoglycemia Sulfonylurea-induced hypoglycemia
Pharmacol Rev. 2003 Mar;55(1):105-31.

Diazoxide
Contraindications: hypersensitivity to diazoxide or to other thiazides
Warnings/precautions: Heart failure – antidiuretic actions, may ↑
fluid retention Gout – may cause hyperuricemia Renal dysfunction
Adverse effects: hypotension, hyperglycemia
Diazoxide [prescribing information].

Patient Case, Cont’d
Time Blood Glucose
Notes
1633 131 Diazoxide __ mg
1817-2012 84-111 Transferred to MICU
2117-2353 61/55/78 D50% 25 g x 3 amps
0246 74 D50% 25 g x 1 amp, changed to D20%
1345 73 D50% 25 g x 1 amp, changed to to D50%/0.45%NS

Patient Case, Cont’d
Post-ED, admitted to MICU with close follow-up from Endocrinology
Continued to IV dextrose infusion with PRN D50% and Q3-6H BG checks
Extensive workup for neuroendocrine tumor: Labs:
Low insulin, c-peptide, and high betahydroxybutyrate does not suggest insulinoma
High pro-insulin may mimic effects of insulin and likely cause of low BG
Octreotide scan – negative findings Endoscopic US Biopsy of pancreatic mass: Positive for
neoplasia neuroendocrine tumor Sent to Harborview for surgical management

References Bender DA, Mayes PA. Chapter 20. Gluconeogenesis & the Control of Blood Glucose. In: Murray RK,
Bender DA, Botham KM, Kennelly PJ, Rodwell VW, Weil P. eds. Harper's Illustrated Biochemistry, 29e. New York, NY: McGraw-Hill; 2012.
Cryer PE, Davis SN. Chapter 345. Hypoglycemia. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson J, Loscalzo J. eds. Harrison's Principles of Internal Medicine, 18e. New York, NY: McGraw-Hill; 2012.
Cryer PE, Axelrod L, Grossman AB, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009 Mar;94(3):709-28.
American Diabetes Association. Hypoglycemia? Low Blood Glucose? Low Blood Sugar? Clinical Diabetes 2012 Jan;30(1):38.
UptoDate. Instant glucose and intravenous dextrose: Drug information. LexiComp.
GlucaGen HypoKit (glucagon) [prescribing information]. Princeton, NJ: Novo Nordisk Inc; December 2011.
Glucagon Emergency Kit [prescribing information]. Indianapolis, IN: Eli Lilly and Company; February 18, 2005.
Doyle ME, Egan JM. Pharmacological agents that directly modulate insulin secretion. Pharmacol Rev. 2003 Mar;55(1):105-31.
McLaughlin SA, Crandall CS, and McKinney PE, “Octreotide: An Antidote for Sulfonylurea-Induced Hypoglycemia,” Ann Emerg Med, 2000, 36(2):133-6.
Fasano CJ, O'Malley G, Dominici P, et al: Comparison of octreotide and standard therapy versus standard therapy alone for the treatment of sulfonylurea-induced hypoglycemia. Ann Emerg Med 2008; 51(4):400-406.
Sandostatin [prescribing information]. East Hanover, NJ: March 2012.
Diazoxide [prescribing information]. Baker Norton Pharmaceuticals, Miami, FL, 1997.