Embed Size (px)
Citation preview

Interventions for multistage treatment of hypoplastic left heart syndrome
Department of Cardiology, Polish Mother's Memorial Hospital, Research Institute, Lodz, Poland
Department of Paediatric Cardiology, University of Medical Sciences, Poznan, Poland
Tomasz Moszura
PINC in Krakow ‘14 11 th Peripheral Interventions Workshop 8 - 9 May 2014

Constant progress in surgical treatment of congenital heart defects in the last decade has significantly improved the prognosis for children with hypoplastic left heart syndrome (HLHS). However, due to specific anatomy and hemodynamics, complications still pose serious challenge in the treatment of patients with HLHS. Modern interventional procedures complement or occasionally replace surgical treatment.

Material and Methods
Between 2001 and 2013 we performed 161 percutaneous interventions in 135 patients with HLHS on all stages of palliation.
Patients were divided into 4 groups: prior to the first surgical treatment
including hybrid approach, after stage I - Norwood operation, after stage II - bidirectional
Glenn operation after stage III - Fontan operation

Prior to surgical treatment
Interventions were performed as initial treatment of HLHS:
Indication for the intervention/type of the intervention
(%)
Restrictive interatrial communication Balloon atrial septostomy
3
Contraindications for surgery Hybrid procedure 2,5
Borderline left ventricle Hybrid procedure 0.5
Total 6

Interventional treatment was successful in 4 In a newborn with intact interatrial septum,
cardiac arrest occurred several times directly after birth and in the catheterization laboratory. Attempts to create an interatrial communication failed and the baby died.
In 3 patients, intervention allowed for clinical and hemodynamic improvement and they underwent stage I Norwood operation on 10th, 13th and 17th day of life.
One neonate died due to intractable generalized infection with multiorgan failure.
Prior to surgical treatment Restrictive interatrial communication
p < 0.005*
p <0.04*
p <0.02*

In 4 patients, with contraindications for surgery:
sepsis, asphyxia, multiorgan failure with coagulation disorders, severe coexisting congenital anomalies.
In 1 patient with critical aortic stenosis, small mitral valve annulus and left ventricle, balloon valvuloplasty of the aortic valve was performed as initial treatment.
After prior surgical bilateral pulmonary artery
banding, patients were transferred to the
catheterization laboratory for stent implantation
of patent ductus arteriosus combined with
concomitant balloon atrial septostomy.
Prior to surgical treatment Hybrid Procedure

After Stage I – Norwood operation
After stage I Norwood operation 38 patients underwent 47 percutaneous interventions

After Stage I – Norwood operationStenosis aortic arch/isthmus
20 patients ranging in age between 2 and 9 months
In 15 patients, intervention was performed through femoral arterial access and in the remaining 5, via venous access.
Both low-pressure (Tyshak – NuMed Inc) and high-pressure (Advance – Cook, Opta – Cordis) balloons were used.
The size of the balloon was chosen according to the diameter of the descending aorta below the stenosis and was equal to or at most 2 mm larger

After Stage I – Norwood operationStenosis aortic arch/isthmus
p<0.00001*
p<0.0001*
p<0.04*
* t-Student test

After Stage I – Norwood operationStenosis of Sano shunt
All interventions were performed as emergency procedures.
The patients ranged in age from 1.5 to 5 months,
O2 saturations measured whilst on mechanical ventilation with 100% oxygen ranged from 28% to 67%.
The minimal diameter of the stenosis was 1.5 to 3 mm.
Interventional treatment involved the use of low or high-pressure balloon angioplasty and stent implantation.

After Stage I – Norwood operationStenosis of Sano shunt
p=0.0025*
p=0.002*
* t-Student test

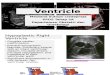
After Stage I – Norwood operationSecondary restriction of interatrial communication
Four infants aged 6 to 12 months. The pressure gradient ranged from 8 to 15 mmHg The mean left atrial
pressure ranged from 15 to 24 mmHg. In 2 static balloon atrial septostomy was performed, in the remaining 2
patients, stent was implanted (Palmaz Genesis, Cordis). The indication for this intervention was the presence on echocardiography of
a thick (> 2 mm) septum.

After Stage I – Norwood operationSecondary restriction of interatrial communication
Four infants aged 6 to 12 months. The pressure gradient ranged from 8 to 15 mmHg The mean left atrial
pressure ranged from 15 to 24 mmHg. In 2 static balloon atrial septostomy was performed, in the remaining 2
patients, stent was implanted (Palmaz Genesis, Cordis). The indication for this intervention was the presence on echocardiography of
a thick (> 2 mm) septum.
p<0.008*p<0.008*
* t-Student test

After Stage II – bidirectional Glenn operation
After second stage BDG operation 133 patients were referred to our catheterization laboratory.
In this group we attempted 85 interventions among 64 patients:

After Stage II – bidirectional Glenn operationpulmonary artery stenosis
Patients age ranged from 10 to 66 months
Isolated balloon angioplasty – 4 pts Stent implantation – 34 pts Prior balloon angioplasty – 9 pts
Access through:right internal jugular vein – 32 ptsleft subclavian vein – 1 ptImplantation during surgery – 1 pt
Pharmacotherapy:100 IU/kg heparin100 IU/kg low-molecular heparin (4 hours after the intervention) Acetylic acid 3 mg/kg
15
96
4

After Stage II – bidirectional Glenn operationpulmonary artery stenosis
3,6 ± 1,33
8,65 ± 1,62
0123456789
10
Before the intervention After the intervention
MM
Diameter of the stenosis
2,73 ± 3,82
0,24 ± 0,61
0
0,5
1
1,5
2
2,5
3
Before the intervention Af ter the intervention
mmHG
Pressure gradient
75 ± 9
77 ± 6
74
74,5
75
75,5
76
76,5
77
77,5
Before the intervention Af ter the intervention
%
O2 saturation
19,79 ± 5,97
16,64 ± 3,64
1515,5
1616,5
1717,5
1818,5
1919,5
2020,5
Before the intervention Af ter the intervention
mmHg
Systolic pressure before the stenosis
p = 0,0529**
p <0,0001** p = 0,0002
p = 0,0018*
* t-Student test ** Wilcoxon test

After Stage II – bidirectional Glenn operation Veno-venous collaterals
12 pts, 14 collaterals age ranged from 18 to 55 months 8 collaterals - coils (13) 6 collaterals - AVP (6), ADO (1) In 3 pts additional blood flow
to pulmonary arteries was closed: 1 Sano shunt 2 B-T shunts
74 ± 8
79 ± 5
71
72
73
74
75
76
77
78
79
%
Before the intervention After the intervention
O2 saturation

After Stage III – Fontan operation
After third stage Fontan operation we attempted 19 interventions among 64 patients:
Indication for the intervention/type of the intervention
Number of interventions
(%)
Extracardiac fenestration Closure with ASO Closure with Starflex Closure with CP covered stent Balloon angioplasty
9 (5.6)4 (2.5)1 (1.2)1 (0.6)
Stenosis of extracardiac tunnel Balloon angioplasty Stent implantationStenosis of pulmonary artery Stent implantation
2 (1.2)1 (0.6)1 (0.6)
Total 19 (11.8)

After Stage III – Fontan operation
In all 14 patients, closure of extracardiac fenestration was succesfull.
One patient, with distal stenosis of the extracardiac tunnel, had implantation of a covered Cheatham-Platinum stent, resulting in complete closure of the fenestration and normalization of the tunnel diameter
In 2 patients, balloon angioplasty of stenosed extracardiac tunnel was performed and in 1 patient, a Cheatham-Platinum stent was implanted. Complete normalization of the tunnel dimensions and a decrease in pressure gradient were achieved.
In 1 patient, stent implantation of the left pulmonary artery resulted in widening of the stenosis and a decrease of venous pressure in the tunnel from mean of 15 mmHg to 13 mmHg.
One patient, with a failing Fontan circulation, required widening of the fenestration, resulting in a decrease of venous pressure in the tunnel from mean of 22 mmHg to 16mmHg and a decrease in symptoms, urine loss of protein and ascites, with significant desaturation from 88% to 73%.

J Am Coll Cardiol. 2011 June 14; 57(24): 2437–2443.Late Status of Fontan Patients with Persistent Surgical Fenestration
Andrew M. Atz, MD,1 Thomas G. Travison, PhD,2 Brian W. McCrindle, MD, MPH,3 Lynn Mahony, MD,4 Michael Quartermain, MD,5 Richard V. Williams, MD,6 Roger E. Breitbart, MD,7 Minmin Lu, MS,2 Elizabeth Radojewski, RN,3Renee Margossian, MD,7 Wesley Covitz, MD,8 and Welton M. Gersony, MD9,

J Am Coll Cardiol. 2011 June 14; 57(24): 2437–2443.Late Status of Fontan Patients with Persistent Surgical Fenestration
Post Fontan Medical HistoryFenestr
ation
No fenestration
Weight for age at study, percentile
29±28 35±31 0.2
Height for age at study, percentile
36±30 42±33 0.2
Cardiac surgical procedures 0.3±0.6 0.4±1.0 0.8
Catheter interventions 0.5±1.2 0.5±1.0 0.3
Stroke 0% 2% 1.0
Thrombosis 4% 8% 0.3
PLE 3% 4% 1.0*
Arrhythmia 21% 20% 0.5*
Functional Health Assessed by Child Health Questionnaire (CHQ50)
Physical Summary Score 46±10 45±12 0.4*
Psychosocial Summary Score 46±11 48±11 0.8*
Echocardiography
Echo EF, % 58±10 59±10 0.6*
Mass:volume ratio z score 1.2±0.5 1.2±0.4 0.5*
dP/dt, mm Hg/s1575±1
0261374±9
080.3*
Exercise Testing
Resting O2 saturation (%) 89±5 95±4 <.001*
Peak VO2 (ml/kg/min) 25±6 27±6 0.2*
% Predicted peak VO2 63±14 67±15 0.1*
VO2 at VAT (ml/kg/min) 16±4 18±6 0.1*
% Predicted VO2 at VAT 67±14 77±22 0.1*
BNP (pg/ml) 34±72 25±44 1.0*

Complications Complications directly related to attempted treatment occurred in
4,3% (7/161) of percutaneous interventions in all patients with HLHS.
In 5 patients complications appeared during stent implantation.
In 4 patients after BDG operation, stenting of bifurcation and/or proximal left pulmonary artery caused:
1 compression of left main bronchus, 2 factures with stent fragmentation, 1 compression of native aorta and coronary arteries during stent
redilatation.

Complicationscompression of the left main bronchus
Palmaz Genesis 7 x 24 mm 9 months later – O2 sat. 70-75% Stent redilatation to 10 mm RPA=LPA 16/14/15 mmHg, MG – 2 Increase of O2 sat. 90%

Complicationscompression of the left main bronchus
Readmitted 7 days later – cyanosis, increased respiratory effort, asymmetrical breath sounds
Chest X-ray, bronchscopy, chest ango-TK
Stenosis of the left main bronchus due to stent redilatation

Complicationscompression of the left main bronchus
Balloon angioplasty (6 mm, 8 mm) of the left main bronchus
Discharged on 30th day of hospitalization in good general condition, with symmetrical breath sounds

Complicationscompression of the left main bronchus
Redilatation of stent in the LPA in case of close proximity to the left main bronchus.
Simultaneous double balloon inflation.

Complicationsstent facture with fragmentation
RPA 34/29/31 mm Hg Palmaz-Genesis 7 x 24 mm Stent redilatation with 12 x 30 high-pressure balloon RPA 22/19/20mm Hg

Complicationsstent facture with fragmentation
• 9F long vascular sheath • CP 8Z22 on 8 x 20 mm OPTA high-pressure balloon• Stents redilatation with 10 x 20 mm TYSHAK balloon• RPA 22/19/20mm Hg

Conclusions
Among all patients with HLHS treated percutaneously the biggest group were children after second stage palliation.
Percutaneous interventions allowed for hemodynamic stabilization prior to the next step treatment, statistically relevant increase in O2 saturation, pulmonary vessel growth and decrease of pulmonary pressure, decrease in the number of surgical interventions.
The most frequent complications in patients after second stage palliation were related to stent implantation to the left pulmonary artery.

THANK YOU