Embed Size (px)
Citation preview

Seminars in Fetal & Neonatal Medicine (2005) 10, 553e566
www.elsevierhealth.com/journals/siny
Hypoplastic left heart syndrome: From in-uterodiagnosis to school age
Jack Rychik a,b,*
a Fetal Heart Program, The Cardiac Center at The Children’s Hospital of Philadelphia, PA, USAb University of Pennsylvania School of Medicine, Philadelphia, PA, USA
KEYWORDSHypoplastic left heartsyndrome;Congenital heartdisease;Fetal diagnosis
Summary HLHS can be treated with successful survival outcome. Prenatal diagno-sis of the anomaly is now quite common. Our understanding of the developmental as-pects of HLHS during the second and third trimesters of gestation is advancing.Survivors of surgery are being closely followed and studied as they proceed forwardsin time. A number of morbidities are identified. Many questions concerning the path-ophysiological mechanisms of thesemorbidities exist. New therapies and treatmentswill certainly arise to meet the challenges these children face as they enter intoadulthood, and as our understanding of this unique cardiovascular state progresses.ª 2005 Elsevier Ltd. All rights reserved.
Introduction
In the current era, nearly all forms of congenitalheart disease are amenable to highly successfulreparative strategies. However, one of the mostpersistently difficult malformations to treat is whenthere is underdevelopment, or hypoplasia, of a ven-tricle. One such anomaly, the hypoplastic left heartsyndrome (HLHS), is defined as an anatomicalconstellation in which the left-sided structures(mitral valve, left ventricle, aortic valve, aorta)are inadequate and non-viable for support of thesystemic circulation.Without early neonatal surgicalintervention, this anomaly is uniformly fatal. Since
* Fetal Heart Program, The Children’s Hospital of Philadel-phia, 34th Street and Civic Center Boulevard, Philadelphia, PA19104, USA. Tel.: C1 215 590 2192; fax: C1 267 426 5082.
E-mail address: [email protected]
1744-165X/$ - see front matter ª 2005 Elsevier Ltd. All rights resdoi:10.1016/j.siny.2005.08.006
the early 1980s, a series of surgical interventionshave been developed, and have subsequentlyevolved, that allow for reconstruction of the circu-lation and survival.1e3 However, despite majorstrides in improving survival, surgical mortality re-mains at least 5e10% in the best of series with ongo-ing life-long morbidity.
This article will review the advances made indiagnosis and management of HLHS in the past twodecades, with emphasis on the progress made inunderstanding the fetal aspects of this anomaly,recent advances in surgical strategy, and some ofthe long-term complications that these childrenface as they grow into adulthood.
Prenatal diagnosis and perinatal course
HLHS occurs in approximately 200e300 per millionlivebirths.4 The anatomy typically consists of
erved.

554 J. Rychik
hypoplasia of the left ventricle with mitral atresiaor stenosis, aortic atresia or stenosis, and hypopla-sia of the ascending aorta. As fetal ultrasound tech-niques and obstetric ultrasound operator skill haveimproved over the past decade, prenatal detectionrates for HLHS have increased substantially. The di-agnosis is now commonly made prior to birth as itcan be determined from simple absence of the nor-mal ‘four-chamber’ heart. HLHS can be associatedwith chromosomal anomalies, most commonlyTurner’s syndrome (45, XO),5 although the majorityof patients do not have any identifiable chromo-somal or genetic association. Extracardiac anoma-lies can also be associated and have beendescribed in up to 28% of cases.6 The recurrencerate for bearing another child with left-sided heartdisease (e.g. bicuspid aortic valve, coarctation ofthe aorta) after having one child with HLHS is quitehigh compared with the recurrence rate for otherforms of heart disease. Recurrence of left-sidedcongenital heart disease (CHD) is reported to beanywhere from 2% to 13%.7 This lends credence tothe notion of a strong genetic componentor familialpredisposition to the disease. Specific gene locihave, however, not yet been identified. Multiple ge-notypic configurations are likely to contribute to theheterogeneous group of phenotypic anatomicalconfigurations called ‘HLHS’.
Features of in-utero diagnosis
HLHS is perceived to be a clinically silent diseasewhile in utero. Absence of a viable left ventricleleads to dilation and hypertrophy of the rightventricle. The right ventricle experiences an in-crease in volume load, as blood is diverted awayfrom the underdeveloped left side. Both the pul-monary and systemic vasculatures are perfused viathe right ventricle and pulmonary artery, withpatency of the ductus arteriosus assuring bloodsupply to the systemic circulation. Most fetuseswith HLHS are asymptomatic prior to birth and cometo gestational term without difficulty. Hydropsfetalis or fetal demise is unusual; when present, itis commonly due to causes other than heart failure.This suggests little physiological disturbance of thecardiovascular system while in utero, but a morecareful analysis reveals otherwise.
Fetuses with HLHS are typically small for gesta-tional age.8 Whether this is a genetically associ-ated finding or acquired during development,perhaps related to abnormal blood flow patterns,is unclear. Although the absence of hydrops inthe typical case suggests adequate cardiac output,evidence has recently been found for diminishedtotal cardiac output in the fetus with HLHS
compared with control normal subjects with twoventricles (A. Szwast, unpublished data). In a seriesof 40 normal fetuses, combined cardiac output ofboth ventricles as measured by Doppler echocardi-ography was 508G 88 ml/min/kg compared withcardiac output in an HLHS group of 18 fetuses of419G 122 ml/min/kg (P! 0.05). This suggests in-complete right ventricular compensation for ab-sence of the left ventricle in fetal HLHS, withapproximately 20% diminution in total combinedcardiac output as measured by Doppler techniques.The decrement in cardiac output may explain thelimitations in somatic growth seen in these fetuses.As we shall see, additional flow disturbances distin-guish the cardiovascular system of a fetuswith HLHSfrom a fetus with a normal two-ventricle heart.
Assessment of a fetus with HLHS via fetalechocardiography reveals normal umbilical arterialflow patterns, suggesting healthy placental func-tion. When performing fetal echocardiography, di-agnostic features to focus on include morphometricassessment of the left ventricle, mitral valve,aortic valve and ascending aorta. In cases of mitralatresia, the left ventricle may be completelyabsent. In cases of mitral stenosis, a small hypertro-phied left ventricle can be seen. Echocardiographicbrightness of the left ventricular endocardium sug-gests the presence of endocardial fibro-elastosis;a fibrotic change in the endocardial portion of themyocardium found in subjects with left-sidedobstructive disease. Colour Doppler flow mappingmay demonstrate a small amount of antegradeflow in cases of stenosis, or absence of flow acrossthe mitral or aortic valves in cases of atresia. Inthe presence of aortic atresia, the ascending aortamay be quite miniscule, functioning as a commoncoronary artery with retrograde perfusion via thetransverse aorta from the ductus arteriosus. Thetricuspid valve may be abnormal in a fetus withHLHS, and may be incompetent. A mild degree oftricuspid regurgitation is common, but severe re-gurgitation can also be seen. In such cases,hydrops may develop as a consequence of di-minished forward flow and elevated central venouspressure.9 Tricuspid regurgitation may progressduring gestation; when severe, it may result inright ventricular dysfunction.10 In those that sur-vive to term, severe tricuspid regurgitation isa risk factor for successful staged reconstruction.
Fetal blood flow patterns in HLHS:pulmonary vasculature and restrictiveatrial septum
Doppler echocardiography has allowed in situobservation of blood flow patterns of fetuses
Hypoplastic left heart syndrome 555
with HLHS. Investigation of these blood flowpatterns has resulted in a much clearer under-standing of this complex and unique physiology.
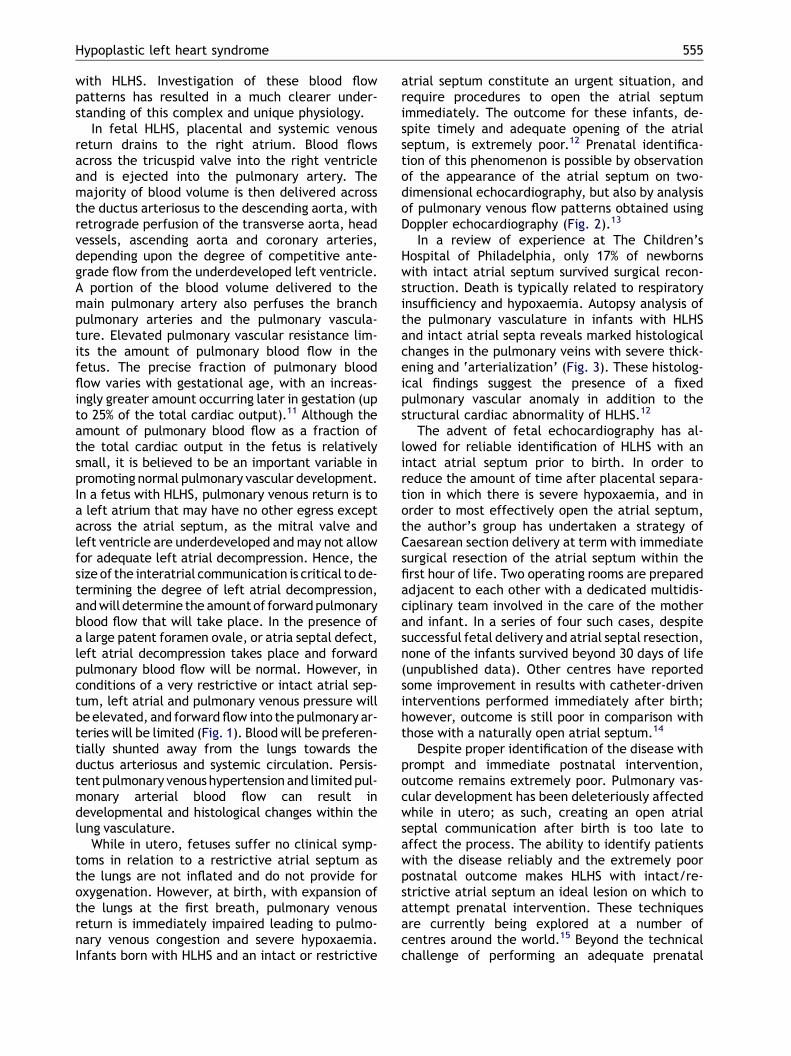
In fetal HLHS, placental and systemic venousreturn drains to the right atrium. Blood flowsacross the tricuspid valve into the right ventricleand is ejected into the pulmonary artery. Themajority of blood volume is then delivered acrossthe ductus arteriosus to the descending aorta, withretrograde perfusion of the transverse aorta, headvessels, ascending aorta and coronary arteries,depending upon the degree of competitive ante-grade flow from the underdeveloped left ventricle.A portion of the blood volume delivered to themain pulmonary artery also perfuses the branchpulmonary arteries and the pulmonary vascula-ture. Elevated pulmonary vascular resistance lim-its the amount of pulmonary blood flow in thefetus. The precise fraction of pulmonary bloodflow varies with gestational age, with an increas-ingly greater amount occurring later in gestation (upto 25% of the total cardiac output).11 Although theamount of pulmonary blood flow as a fraction ofthe total cardiac output in the fetus is relativelysmall, it is believed to be an important variable inpromoting normal pulmonary vascular development.In a fetus with HLHS, pulmonary venous return is toa left atrium that may have no other egress exceptacross the atrial septum, as the mitral valve andleft ventricle are underdeveloped andmay not allowfor adequate left atrial decompression. Hence, thesize of the interatrial communication is critical tode-termining the degree of left atrial decompression,andwill determine the amountof forwardpulmonaryblood flow that will take place. In the presence ofa large patent foramen ovale, or atria septal defect,left atrial decompression takes place and forwardpulmonary blood flow will be normal. However, inconditions of a very restrictive or intact atrial sep-tum, left atrial and pulmonary venous pressure willbeelevated, and forwardflow into the pulmonary ar-teries will be limited (Fig. 1). Blood will be preferen-tially shunted away from the lungs towards theductus arteriosus and systemic circulation. Persis-tentpulmonary venoushypertension and limitedpul-monary arterial blood flow can result indevelopmental and histological changes within thelung vasculature.
While in utero, fetuses suffer no clinical symp-toms in relation to a restrictive atrial septum asthe lungs are not inflated and do not provide foroxygenation. However, at birth, with expansion ofthe lungs at the first breath, pulmonary venousreturn is immediately impaired leading to pulmo-nary venous congestion and severe hypoxaemia.Infants born with HLHS and an intact or restrictive
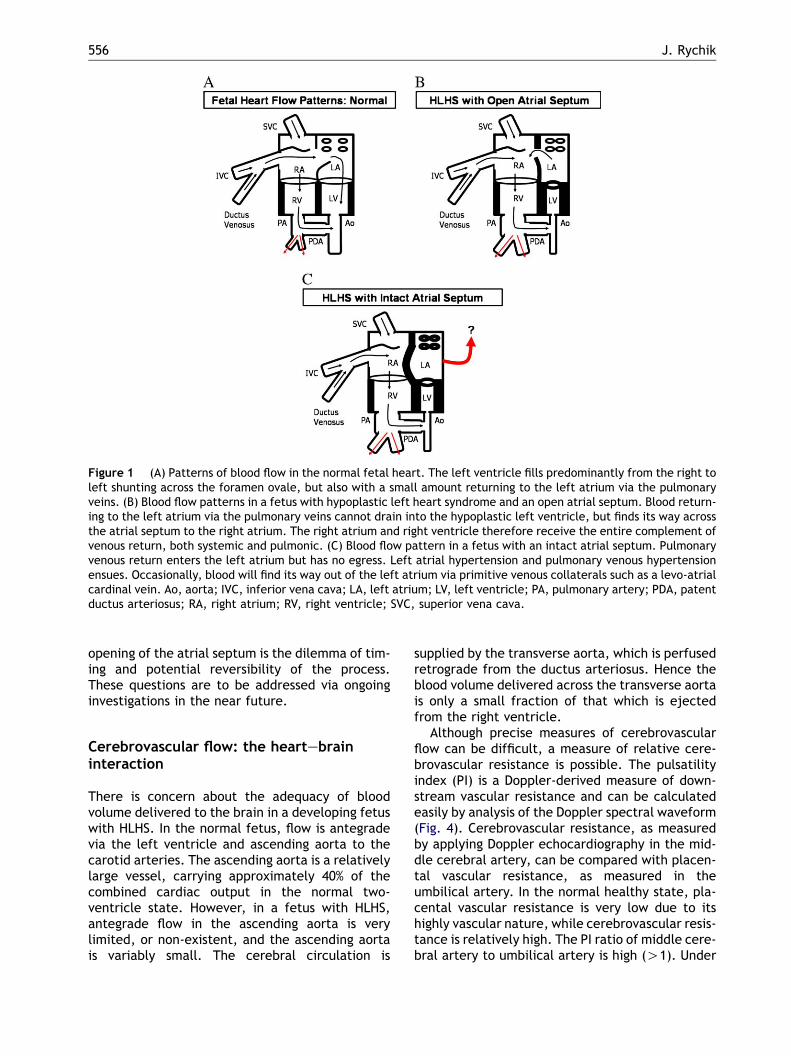
atrial septum constitute an urgent situation, andrequire procedures to open the atrial septumimmediately. The outcome for these infants, de-spite timely and adequate opening of the atrialseptum, is extremely poor.12 Prenatal identifica-tion of this phenomenon is possible by observationof the appearance of the atrial septum on two-dimensional echocardiography, but also by analysisof pulmonary venous flow patterns obtained usingDoppler echocardiography (Fig. 2).13
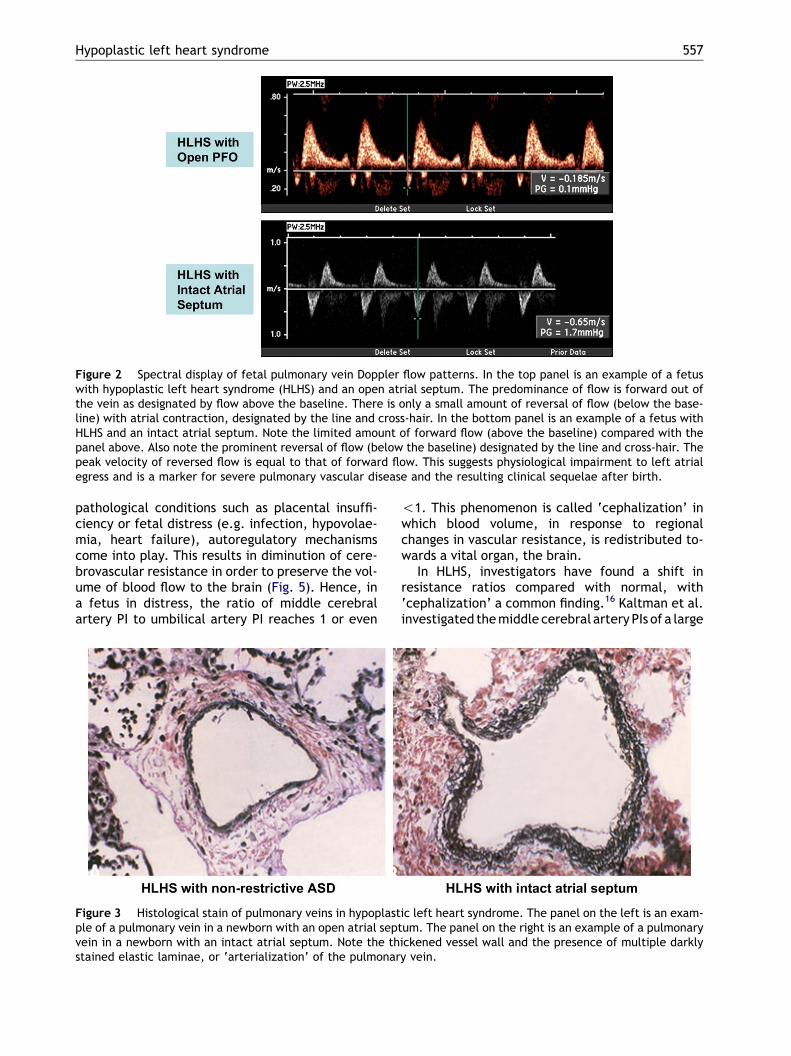
In a review of experience at The Children’sHospital of Philadelphia, only 17% of newbornswith intact atrial septum survived surgical recon-struction. Death is typically related to respiratoryinsufficiency and hypoxaemia. Autopsy analysis ofthe pulmonary vasculature in infants with HLHSand intact atrial septa reveals marked histologicalchanges in the pulmonary veins with severe thick-ening and ‘arterialization’ (Fig. 3). These histolog-ical findings suggest the presence of a fixedpulmonary vascular anomaly in addition to thestructural cardiac abnormality of HLHS.12
The advent of fetal echocardiography has al-lowed for reliable identification of HLHS with anintact atrial septum prior to birth. In order toreduce the amount of time after placental separa-tion in which there is severe hypoxaemia, and inorder to most effectively open the atrial septum,the author’s group has undertaken a strategy ofCaesarean section delivery at term with immediatesurgical resection of the atrial septum within thefirst hour of life. Two operating rooms are preparedadjacent to each other with a dedicated multidis-ciplinary team involved in the care of the motherand infant. In a series of four such cases, despitesuccessful fetal delivery and atrial septal resection,none of the infants survived beyond 30 days of life(unpublished data). Other centres have reportedsome improvement in results with catheter-driveninterventions performed immediately after birth;however, outcome is still poor in comparison withthose with a naturally open atrial septum.14
Despite proper identification of the disease withprompt and immediate postnatal intervention,outcome remains extremely poor. Pulmonary vas-cular development has been deleteriously affectedwhile in utero; as such, creating an open atrialseptal communication after birth is too late toaffect the process. The ability to identify patientswith the disease reliably and the extremely poorpostnatal outcome makes HLHS with intact/re-strictive atrial septum an ideal lesion on which toattempt prenatal intervention. These techniquesare currently being explored at a number ofcentres around the world.15 Beyond the technicalchallenge of performing an adequate prenatal
556 J. Rychik
Figure 1 (A) Patterns of blood flow in the normal fetal heart. The left ventricle fills predominantly from the right toleft shunting across the foramen ovale, but also with a small amount returning to the left atrium via the pulmonaryveins. (B) Blood flow patterns in a fetus with hypoplastic left heart syndrome and an open atrial septum. Blood return-ing to the left atrium via the pulmonary veins cannot drain into the hypoplastic left ventricle, but finds its way acrossthe atrial septum to the right atrium. The right atrium and right ventricle therefore receive the entire complement ofvenous return, both systemic and pulmonic. (C) Blood flow pattern in a fetus with an intact atrial septum. Pulmonaryvenous return enters the left atrium but has no egress. Left atrial hypertension and pulmonary venous hypertensionensues. Occasionally, blood will find its way out of the left atrium via primitive venous collaterals such as a levo-atrialcardinal vein. Ao, aorta; IVC, inferior vena cava; LA, left atrium; LV, left ventricle; PA, pulmonary artery; PDA, patentductus arteriosus; RA, right atrium; RV, right ventricle; SVC, superior vena cava.
opening of the atrial septum is the dilemma of tim-ing and potential reversibility of the process.These questions are to be addressed via ongoinginvestigations in the near future.
Cerebrovascular flow: the heartebraininteraction
There is concern about the adequacy of bloodvolume delivered to the brain in a developing fetuswith HLHS. In the normal fetus, flow is antegradevia the left ventricle and ascending aorta to thecarotid arteries. The ascending aorta is a relativelylarge vessel, carrying approximately 40% of thecombined cardiac output in the normal two-ventricle state. However, in a fetus with HLHS,antegrade flow in the ascending aorta is verylimited, or non-existent, and the ascending aortais variably small. The cerebral circulation is
supplied by the transverse aorta, which is perfusedretrograde from the ductus arteriosus. Hence theblood volume delivered across the transverse aortais only a small fraction of that which is ejectedfrom the right ventricle.
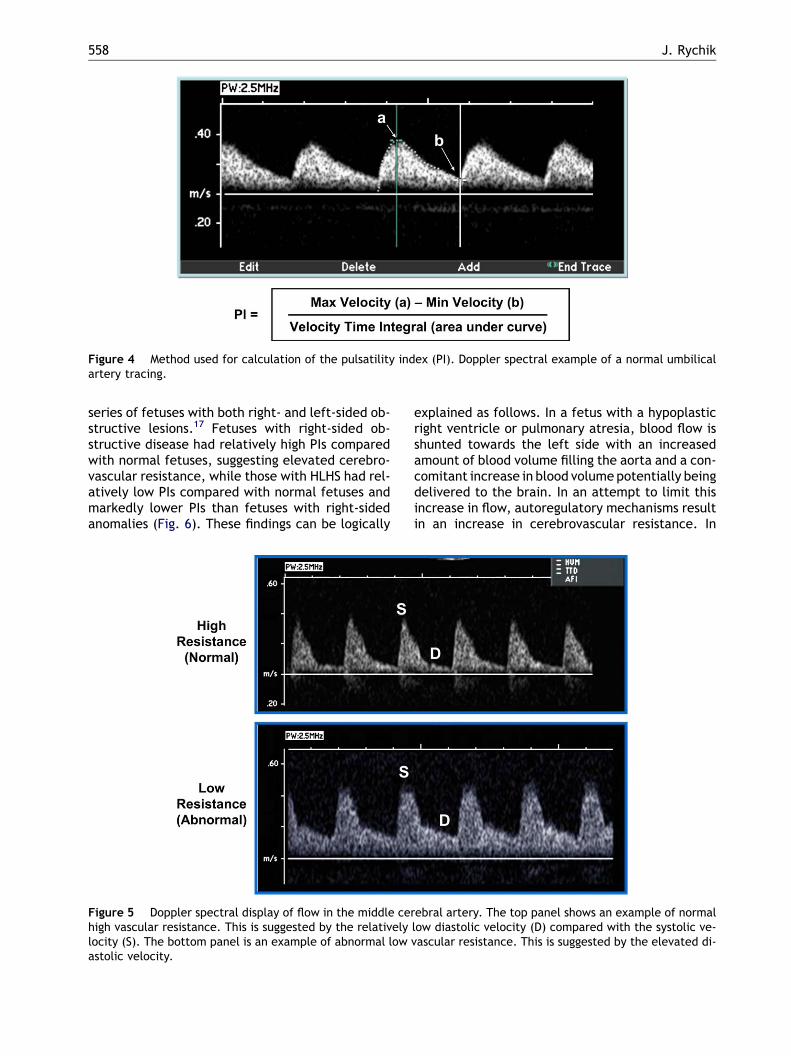
Although precise measures of cerebrovascularflow can be difficult, a measure of relative cere-brovascular resistance is possible. The pulsatilityindex (PI) is a Doppler-derived measure of down-stream vascular resistance and can be calculatedeasily by analysis of the Doppler spectral waveform(Fig. 4). Cerebrovascular resistance, as measuredby applying Doppler echocardiography in the mid-dle cerebral artery, can be compared with placen-tal vascular resistance, as measured in theumbilical artery. In the normal healthy state, pla-cental vascular resistance is very low due to itshighly vascular nature, while cerebrovascular resis-tance is relatively high. The PI ratio of middle cere-bral artery to umbilical artery is high (O1). Under
Hypoplastic left heart syndrome 557
Figure 2 Spectral display of fetal pulmonary vein Doppler flow patterns. In the top panel is an example of a fetuswith hypoplastic left heart syndrome (HLHS) and an open atrial septum. The predominance of flow is forward out ofthe vein as designated by flow above the baseline. There is only a small amount of reversal of flow (below the base-line) with atrial contraction, designated by the line and cross-hair. In the bottom panel is an example of a fetus withHLHS and an intact atrial septum. Note the limited amount of forward flow (above the baseline) compared with thepanel above. Also note the prominent reversal of flow (below the baseline) designated by the line and cross-hair. Thepeak velocity of reversed flow is equal to that of forward flow. This suggests physiological impairment to left atrialegress and is a marker for severe pulmonary vascular disease and the resulting clinical sequelae after birth.
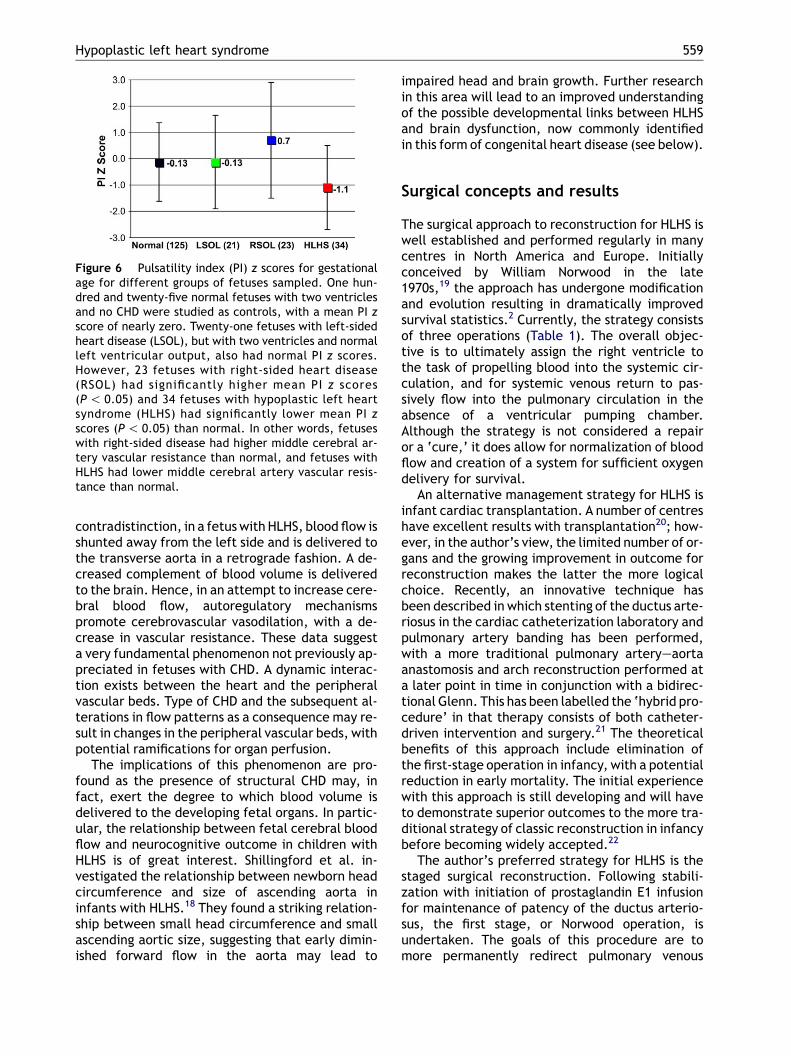
pathological conditions such as placental insuffi-ciency or fetal distress (e.g. infection, hypovolae-mia, heart failure), autoregulatory mechanismscome into play. This results in diminution of cere-brovascular resistance in order to preserve the vol-ume of blood flow to the brain (Fig. 5). Hence, ina fetus in distress, the ratio of middle cerebralartery PI to umbilical artery PI reaches 1 or even
!1. This phenomenon is called ‘cephalization’ inwhich blood volume, in response to regionalchanges in vascular resistance, is redistributed to-wards a vital organ, the brain.
In HLHS, investigators have found a shift inresistance ratios compared with normal, with‘cephalization’ a common finding.16 Kaltman et al.investigated themiddle cerebral arteryPIs of a large
Figure 3 Histological stain of pulmonary veins in hypoplastic left heart syndrome. The panel on the left is an exam-ple of a pulmonary vein in a newborn with an open atrial septum. The panel on the right is an example of a pulmonaryvein in a newborn with an intact atrial septum. Note the thickened vessel wall and the presence of multiple darklystained elastic laminae, or ‘arterialization’ of the pulmonary vein.
558 J. Rychik
Figure 4 Method used for calculation of the pulsatility index (PI). Doppler spectral example of a normal umbilicalartery tracing.
series of fetuses with both right- and left-sided ob-structive lesions.17 Fetuses with right-sided ob-structive disease had relatively high PIs comparedwith normal fetuses, suggesting elevated cerebro-vascular resistance, while those with HLHS had rel-atively low PIs compared with normal fetuses andmarkedly lower PIs than fetuses with right-sidedanomalies (Fig. 6). These findings can be logically
explained as follows. In a fetus with a hypoplasticright ventricle or pulmonary atresia, blood flow isshunted towards the left side with an increasedamount of blood volume filling the aorta and a con-comitant increase in blood volumepotentially beingdelivered to the brain. In an attempt to limit thisincrease in flow, autoregulatory mechanisms resultin an increase in cerebrovascular resistance. In
Figure 5 Doppler spectral display of flow in the middle cerebral artery. The top panel shows an example of normalhigh vascular resistance. This is suggested by the relatively low diastolic velocity (D) compared with the systolic ve-locity (S). The bottom panel is an example of abnormal low vascular resistance. This is suggested by the elevated di-astolic velocity.
Hypoplastic left heart syndrome 559
contradistinction, in a fetuswith HLHS, blood flow isshunted away from the left side and is delivered tothe transverse aorta in a retrograde fashion. A de-creased complement of blood volume is deliveredto the brain. Hence, in an attempt to increase cere-bral blood flow, autoregulatory mechanismspromote cerebrovascular vasodilation, with a de-crease in vascular resistance. These data suggesta very fundamental phenomenon not previously ap-preciated in fetuses with CHD. A dynamic interac-tion exists between the heart and the peripheralvascular beds. Type of CHD and the subsequent al-terations in flow patterns as a consequence may re-sult in changes in the peripheral vascular beds, withpotential ramifications for organ perfusion.
The implications of this phenomenon are pro-found as the presence of structural CHD may, infact, exert the degree to which blood volume isdelivered to the developing fetal organs. In partic-ular, the relationship between fetal cerebral bloodflow and neurocognitive outcome in children withHLHS is of great interest. Shillingford et al. in-vestigated the relationship between newborn headcircumference and size of ascending aorta ininfants with HLHS.18 They found a striking relation-ship between small head circumference and smallascending aortic size, suggesting that early dimin-ished forward flow in the aorta may lead to
Figure 6 Pulsatility index (PI) z scores for gestationalage for different groups of fetuses sampled. One hun-dred and twenty-five normal fetuses with two ventriclesand no CHD were studied as controls, with a mean PI zscore of nearly zero. Twenty-one fetuses with left-sidedheart disease (LSOL), but with two ventricles and normalleft ventricular output, also had normal PI z scores.However, 23 fetuses with right-sided heart disease(RSOL) had significantly higher mean PI z scores(P! 0.05) and 34 fetuses with hypoplastic left heartsyndrome (HLHS) had significantly lower mean PI zscores (P! 0.05) than normal. In other words, fetuseswith right-sided disease had higher middle cerebral ar-tery vascular resistance than normal, and fetuses withHLHS had lower middle cerebral artery vascular resis-tance than normal.
impaired head and brain growth. Further researchin this area will lead to an improved understandingof the possible developmental links between HLHSand brain dysfunction, now commonly identifiedin this form of congenital heart disease (see below).
Surgical concepts and results
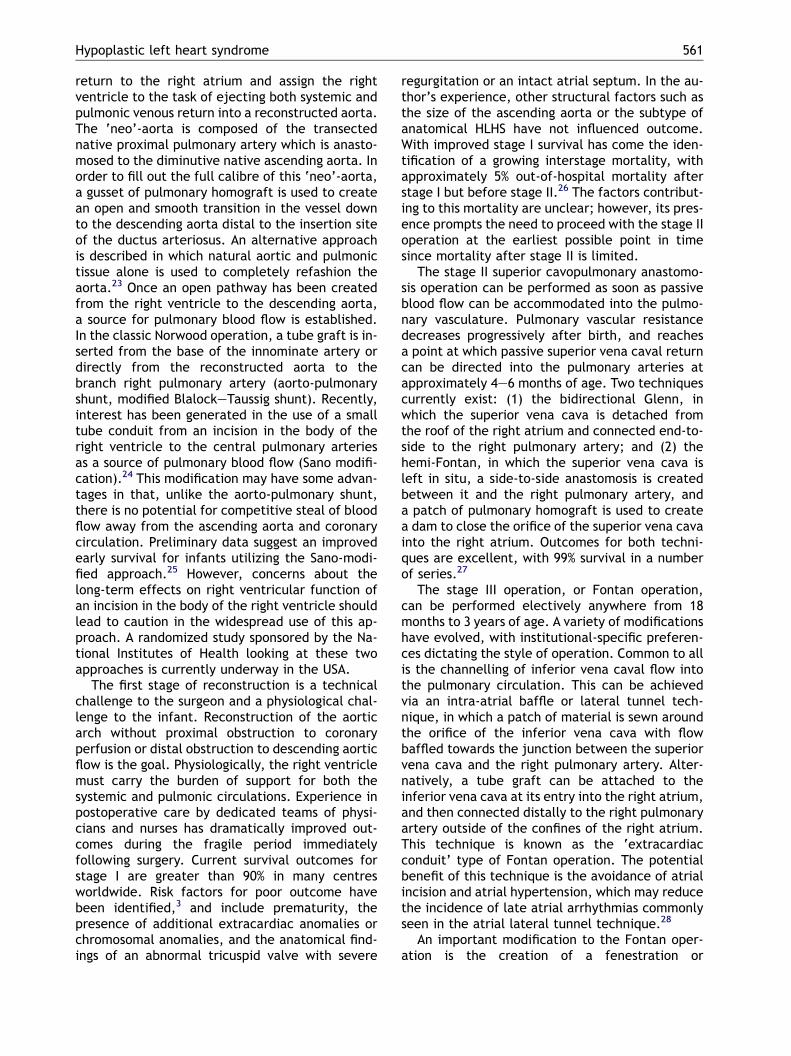
The surgical approach to reconstruction for HLHS iswell established and performed regularly in manycentres in North America and Europe. Initiallyconceived by William Norwood in the late1970s,19 the approach has undergone modificationand evolution resulting in dramatically improvedsurvival statistics.2 Currently, the strategy consistsof three operations (Table 1). The overall objec-tive is to ultimately assign the right ventricle tothe task of propelling blood into the systemic cir-culation, and for systemic venous return to pas-sively flow into the pulmonary circulation in theabsence of a ventricular pumping chamber.Although the strategy is not considered a repairor a ‘cure,’ it does allow for normalization of bloodflow and creation of a system for sufficient oxygendelivery for survival.
An alternative management strategy for HLHS isinfant cardiac transplantation. A number of centreshave excellent results with transplantation20; how-ever, in the author’s view, the limited number of or-gans and the growing improvement in outcome forreconstruction makes the latter the more logicalchoice. Recently, an innovative technique hasbeen described in which stenting of the ductus arte-riosus in the cardiac catheterization laboratory andpulmonary artery banding has been performed,with a more traditional pulmonary arteryeaortaanastomosis and arch reconstruction performed ata later point in time in conjunction with a bidirec-tional Glenn. This has been labelled the ‘hybrid pro-cedure’ in that therapy consists of both catheter-driven intervention and surgery.21 The theoreticalbenefits of this approach include elimination ofthe first-stage operation in infancy, with a potentialreduction in early mortality. The initial experiencewith this approach is still developing and will haveto demonstrate superior outcomes to the more tra-ditional strategy of classic reconstruction in infancybefore becoming widely accepted.22
The author’s preferred strategy for HLHS is thestaged surgical reconstruction. Following stabili-zation with initiation of prostaglandin E1 infusionfor maintenance of patency of the ductus arterio-sus, the first stage, or Norwood operation, isundertaken. The goals of this procedure are tomore permanently redirect pulmonary venous
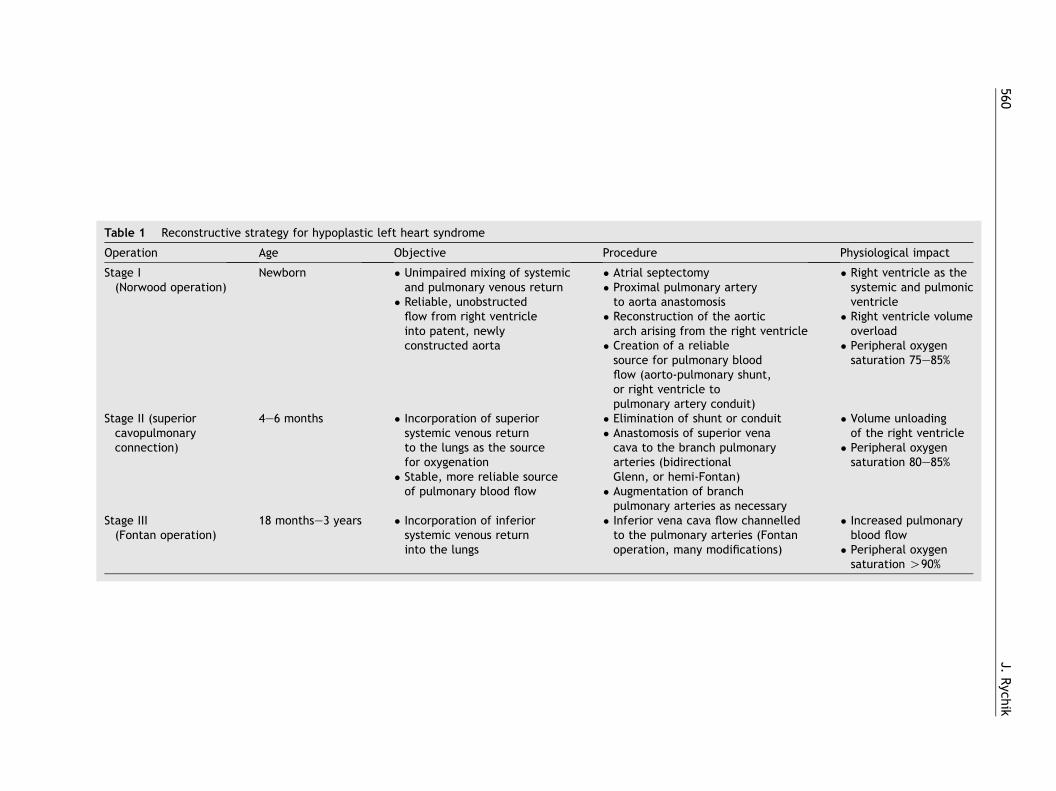
Table 1
Operation ure Physiological impact
Stage I(Norwoo
l septectomyimal pulmonary arteryrta anastomosisnstruction of the aorticarising from the right ventricletion of a reliablece for pulmonary blood(aorto-pulmonary shunt,ght ventricle toonary artery conduit)
� Right ventricle as thesystemic and pulmonicventricle
� Right ventricle volumeoverload
� Peripheral oxygensaturation 75e85%
Stage II (scavopulconnect
ination of shunt or conduittomosis of superior venato the branch pulmonary
ries (bidirectionaln, or hemi-Fontan)entation of branchonary arteries as necessary
� Volume unloadingof the right ventricle
� Peripheral oxygensaturation 80e85%
Stage III(Fontan
ior vena cava flow channellede pulmonary arteries (Fontanation, many modifications)
� Increased pulmonaryblood flow
� Peripheral oxygensaturation O90%
560J.
Rych
ik
Reconstructive strategy for hypoplastic left heart syndrome
Age Objective Proced
d operation)Newborn � Unimpaired mixing of systemic
and pulmonary venous return� Reliable, unobstructedflow from right ventricleinto patent, newlyconstructed aorta
� Atria� Proxto ao
� Recoarch
� Creasourflowor ripulm
uperiormonaryion)
4e6 months � Incorporation of superiorsystemic venous returnto the lungs as the sourcefor oxygenation
� Stable, more reliable sourceof pulmonary blood flow
� Elim� AnascavaarteGlen
� Augmpulm
operation)18 monthse3 years � Incorporation of inferior
systemic venous returninto the lungs
� Inferto thoper
Hypoplastic left heart syndrome 561
return to the right atrium and assign the rightventricle to the task of ejecting both systemic andpulmonic venous return into a reconstructed aorta.The ‘neo’-aorta is composed of the transectednative proximal pulmonary artery which is anasto-mosed to the diminutive native ascending aorta. Inorder to fill out the full calibre of this ‘neo’-aorta,a gusset of pulmonary homograft is used to createan open and smooth transition in the vessel downto the descending aorta distal to the insertion siteof the ductus arteriosus. An alternative approachis described in which natural aortic and pulmonictissue alone is used to completely refashion theaorta.23 Once an open pathway has been createdfrom the right ventricle to the descending aorta,a source for pulmonary blood flow is established.In the classic Norwood operation, a tube graft is in-serted from the base of the innominate artery ordirectly from the reconstructed aorta to thebranch right pulmonary artery (aorto-pulmonaryshunt, modified BlalockeTaussig shunt). Recently,interest has been generated in the use of a smalltube conduit from an incision in the body of theright ventricle to the central pulmonary arteriesas a source of pulmonary blood flow (Sano modifi-cation).24 This modification may have some advan-tages in that, unlike the aorto-pulmonary shunt,there is no potential for competitive steal of bloodflow away from the ascending aorta and coronarycirculation. Preliminary data suggest an improvedearly survival for infants utilizing the Sano-modi-fied approach.25 However, concerns about thelong-term effects on right ventricular function ofan incision in the body of the right ventricle shouldlead to caution in the widespread use of this ap-proach. A randomized study sponsored by the Na-tional Institutes of Health looking at these twoapproaches is currently underway in the USA.
The first stage of reconstruction is a technicalchallenge to the surgeon and a physiological chal-lenge to the infant. Reconstruction of the aorticarch without proximal obstruction to coronaryperfusion or distal obstruction to descending aorticflow is the goal. Physiologically, the right ventriclemust carry the burden of support for both thesystemic and pulmonic circulations. Experience inpostoperative care by dedicated teams of physi-cians and nurses has dramatically improved out-comes during the fragile period immediatelyfollowing surgery. Current survival outcomes forstage I are greater than 90% in many centresworldwide. Risk factors for poor outcome havebeen identified,3 and include prematurity, thepresence of additional extracardiac anomalies orchromosomal anomalies, and the anatomical find-ings of an abnormal tricuspid valve with severe
regurgitation or an intact atrial septum. In the au-thor’s experience, other structural factors such asthe size of the ascending aorta or the subtype ofanatomical HLHS have not influenced outcome.With improved stage I survival has come the iden-tification of a growing interstage mortality, withapproximately 5% out-of-hospital mortality afterstage I but before stage II.26 The factors contribut-ing to this mortality are unclear; however, its pres-ence prompts the need to proceed with the stage IIoperation at the earliest possible point in timesince mortality after stage II is limited.
The stage II superior cavopulmonary anastomo-sis operation can be performed as soon as passiveblood flow can be accommodated into the pulmo-nary vasculature. Pulmonary vascular resistancedecreases progressively after birth, and reachesa point at which passive superior vena caval returncan be directed into the pulmonary arteries atapproximately 4e6 months of age. Two techniquescurrently exist: (1) the bidirectional Glenn, inwhich the superior vena cava is detached fromthe roof of the right atrium and connected end-to-side to the right pulmonary artery; and (2) thehemi-Fontan, in which the superior vena cava isleft in situ, a side-to-side anastomosis is createdbetween it and the right pulmonary artery, anda patch of pulmonary homograft is used to createa dam to close the orifice of the superior vena cavainto the right atrium. Outcomes for both techni-ques are excellent, with 99% survival in a numberof series.27
The stage III operation, or Fontan operation,can be performed electively anywhere from 18months to 3 years of age. A variety of modificationshave evolved, with institutional-specific preferen-ces dictating the style of operation. Common to allis the channelling of inferior vena caval flow intothe pulmonary circulation. This can be achievedvia an intra-atrial baffle or lateral tunnel tech-nique, in which a patch of material is sewn aroundthe orifice of the inferior vena cava with flowbaffled towards the junction between the superiorvena cava and the right pulmonary artery. Alter-natively, a tube graft can be attached to theinferior vena cava at its entry into the right atrium,and then connected distally to the right pulmonaryartery outside of the confines of the right atrium.This technique is known as the ‘extracardiacconduit’ type of Fontan operation. The potentialbenefit of this technique is the avoidance of atrialincision and atrial hypertension, which may reducethe incidence of late atrial arrhythmias commonlyseen in the atrial lateral tunnel technique.28
An important modification to the Fontan oper-ation is the creation of a fenestration or

562 J. Rychik
communication between the systemic venouspathway and the pulmonary venous chamber. Inthe author’s experience, a 4e5-mm fenestrationcreated at the time of the Fontan operation resultsin excellent postoperative outcome and a smoothpostoperative course.29 The fenestration results inoxygen saturation that is slightly diminished due toright to left shunting, but ventricular filling andcardiac output are markedly enhanced; hence,such patients have improved oxygen delivery.30
While early peripheral oxygen saturations are inthe mid-80% range, the fenestration commonlyundergoes spontaneous closure over time. In theauthor’s experience, over three-quarters of fenes-trations close spontaneously or are insignificantlysmall within 1 year of surgery.31 Thereafter, oxy-gen saturation levels are O90%. Survival followingFontan operation in the current era is excellentwith 99% survival.
School age: how are these childrendoing?
The overall success of the strategy for reconstruc-tive surgery for HLHS has resulted in a largenumber of children who are survivors; the majorityare now at middle school. Most of the mortalityfollowing reconstruction of HLHS takes place soonafter stage I or as an interstage death prior to thesuperior cavopulmonary connection. Late mortal-ity after reconstruction is relatively uncommon.However, with an increasing number of childrensurviving the rigors of surgery, a number of morbid-ities have been identified (Table 2).
Exercise limitation is a common finding in chil-dren with HLHS after Fontan operation. The abilityto increase cardiac output in response to thedemands of exercise is limited.32 The absence ofa pulmonary pumping chamber to deliver a normalcomplement of blood to the lungs and the presenceof a morphological right ventricle as the systemicventricle contribute to an inability to appropriatelyincrease stroke volume to match needs to the samedegree seen in the normal two-ventricle heart. In
addition, the heart rate response to exercise is typ-ically blunted after Fontan operation due to sinusnode dysfunction. Many children with HLHS enjoya number of sports activities, but they frequentlytire easily and rarely enter high-level competition.Each child is encouraged to participate in sportsand to seek out their own level of comfort, withno strict restrictions imposed.
Atrial arrhythmias are common after Fontanoperation and are likely to be related to themultiple incisions and suture lines present. Sinusnode dysfunction with sinus bradycardia or junc-tional rhythm can be present as a consequence ofthe stage II or stage III operations, as theseoperations require manipulation near the sinusnode with potential trauma to it or interruption ofthe arterial supply of the sinus node.33 Atrial fluttercan be seen as a consequence of scarred atrial tis-sue and may sometimes be difficult to treat.
Children after Fontan operation have a predilec-tion towards thrombus formation.34 The cause ofthis phenomenon is multifactorial. A generalizedlow cardiac output state with stasis of blood andlow flow velocity within the atria are contributingfactors. Synthetic patch material is used for thelateral tunnel or conduit systemic venous pathway,which may act as a thrombogenic source. Atrial ar-rhythmias may predispose to clot formation. Anumber of investigators have documented abnor-malities in coagulation proteins after Fontan oper-ation.35 Recently, coagulation abnormalities havebeen discovered in infants with single-ventricleanatomy prior to Fontan operation, raising the pos-sibility that these abnormalities are primary andassociated, but not secondarily caused by thephysiology of the Fontan circulation.36 Nonethe-less, these children are at increased risk for strokeand pulmonary embolism. Recommendations forantiplatelet or anticoagulative therapies are con-troversial, with varying viewpoints on the correctmanagement style and efficacy of these agents.37
Prophylactic treatment strategies range from dailyaspirin (as an antiplatelet agent) to warfarin. Stud-ies investigating the efficacy of these treatmentsare currently underway.
Table 2 Morbidities in children with hypoplastic left heart syndrome after Fontan operation
Morbidity Frequency
Exercise intolerance Majority, to varying degreesArrhythmia 25e50%, to varying degreesThrombo-embolic disease (e.g. pulmonary embolism, stroke) Approximately 10%Protein-losing enteropathy !5%Neurocognitive disabilities (e.g. learning differences, attention deficit/hyperactivity disorder)
10e70%, to varying degrees

Hypoplastic left heart syndrome 563
Another enigmatic morbidity seen after Fontanoperation is protein-losing enteropathy. Abnormalenteric protein loss can occur spontaneously,monthsor years after Fontan surgery, resulting in markedhypoproteinaemia. Clinically, these patients presentwith diarrhoea, abdominal discomfort, and periph-eral oedema with ascites as a consequence of lowserum protein levels.38 The disease occurs in 3e13%of cases,with nearly 50%mortality 5 years after diag-nosis.39 The precise pathophysiologicalmechanism isunknown. Interventions that improve and maximizecardiac output, such as creation of a fenestration,have resulted in successful management of the dis-ease, suggesting that the physiology of low cardiacoutput and high central venous pressure unique tothe Fontan circulation may predispose to the ail-ment.40 However, questions remain regarding whycertain patients suffer fromprotein-losing enteropa-thy and others with similar haemodynamics do not,raising the possibility of a predisposition to the dis-ease in select patients, but only after the haemody-namics of the Fontan circulation are imposed.
Of great interest has been the identification ofneurocognitive difficulties in many of the childrenwith HLHS now entering school age.41 A number ofstudies have demonstrated that these childrenface a variety of neurodevelopmental difficulties.In one series, mean scores on standardized psycho-metric tests for a groupofHLHS childrenwere signif-icantly lower than the normal population, with 18%scoring less than 70 on intelligence quotient testing.Of note, nearly 70% met criteria for attention defi-cit/hyperactivity disorder based on neurological ex-amination.42 In another study, children with HLHSafter Fontan operation were compared with otherchildren with a single ventricle after Fontan opera-tion. Test scores for the HLHS group were found tobe lower than those for the non-HLHS group, butwere in the low-average range.43 Most interestingly,similar deficiencies have been identified in childrenwith HLHS undergoing a strategy of heart transplan-tation,44 suggesting that these deficits may not nec-essarily be related to the style of treatment but aredirectly associated with HLHS.
Children who undergo the reconstructive ap-proach for HLHS are required to have three oper-ations with consequential courses of deephypothermic circulatory arrest; a variable that canimpact negatively on neurocognitive outcome. How-ever, emerging data indicate that the deficienciesseen inHLHSmay be influenced by other factors. Thedurationof deephypothermic circulatory arrest doesnot appear to correlate with the neurodevelopmen-tal deficits found. Structural abnormalities of thebrain have been identified in HLHS prior to surgery,including holoprosencephaly and agenesis of the
corpus callosum.45 A more subtle abnormality ofbrain dysgenesis noted is that of an underdevelopedoperculum, the region of the cortical mantle at thejuncture of the frontal, parietal and temporal lobes.Deficiencies in this region are associated with feed-ing and swallowing difficulties, and this is of interestas many infants exhibit problems with feeding afterstage I surgery.46 Periventricular leukomalacia,a non-specific sign of cerebral white matter injuryas seen on magnetic resonance imaging, is presentin up to 16% of neonates with complex congenitalheart disease prior to surgery, but in over 50% aftersurgery.47,48 This raises the possibility that neonateswith HLHS have a fragile central nervous system,with inherent deficiencies present that may be fur-ther impacteduponby thepotential neurological ‘in-jury’ of the procedures required for heart surgery.Recent data on the response tobrain injury after car-diopulmonary bypass demonstrate a relationshipwith a gene polymorphism of the apo-lipoprotein E,a molecule that plays an important role in neuronalrepair. Following heart surgery, infants with apo-li-poprotein E epsilon 2 allele are at greater risk of hav-ing significantly lower psychomotor developmentindices at 1 year of age than infants with the othergenotypes for this protein.49 These data further sup-port the notion of certain patients being at risk forneurodevelopmental dysfunctionwith a predilectiontowards poor response tonervous system injury, suchas cardiopulmonary bypass. Whether infants withHLHS are at such an increased risk is speculative atthis point. Linking the data on fetal cerebrovascularflow patterns and cerebrovascular resistance in thefetus with HLHS with the subtle structural findingsand genetic predisposition to injury that exists mayultimately result in stratification of the infant atmost significant risk for neurological injury. Specificchanges in neuroprotective strategy may then beimplemented for these high-risk patients.
Putting it all into perspective:counselling a family carryinga fetus with HLHS
Considering the outcome data on morbidity andmortality as we know it today, how should onecounsel the family of a fetus with HLHS? Geo-graphic, cultural and religious factors influencethe response when a family is faced with the newsof carrying a fetus with HLHS. Unfortunately,because of the history related to poor outcome inthe past, many practitioners are unaware of thecurrent survival statistics for HLHS. National orregional experiences may also impact either

564 J. Rychik
positively or negatively on the statistics and datatransmitted to the family. Not all centres areuniformly able to offer the same survival statisticsbased on their own experiences. This raises thequestion of regionalization of care and referral tocentres of excellence specifically identified as ableto treat this anomaly. The facts support the notionthat survival is possible for the majority when theprocedure and postoperative care are performedby experienced hands. Lack of knowledge byprimary obstetricians andmaternalefetal medicineexperts concerning these recent statistics can re-sult in inaccurate transfer of information to fami-lies. While excellent operative statistics can now bequoted, counselling sessions should focus moreextensively on the issues of long-term morbidityand the risks of unknown beyond the second decadeof life, for which few data are available. In theauthor’s view, counselling must be offered byknowledgeable physicians/nurses in a non-biasedfactual manner, providing as much objective in-formation as possible. Family support should beoffered regardless of the decisions made.
Development of a multidisciplinary approach tocounselling these families is helpful. The author’sgroup has constructed a Fetal Heart Program thatincludes cardiologists, nurses, cardiac surgeons andmaternalefetal medicine specialists, all of whomcontribute to the evaluation and assistance of thesefamilies as they make their way forward in gesta-tion. Bringing potential parents into contact withother families those have gone through the decisionprocess can be helpful. For those families whochoose to continue the pregnancy, delivery can besafely performed vaginally with prostaglandin ini-tiated after birth. The author’s group routinelyperform serial fetal echocardiographic studies forfetuses with HLHS at 4-week intervals after initialprenatal diagnosis to survey for any changes intricuspid valve regurgitation, or restriction in theatrial septum. These serial sessions also offer theopportunity for further educational and psycholog-ical support for the parents and other familymembers. A dedicated nurse co-ordinator in ourprogramme assists with shepherding the familiesthrough the prenatal process, creating a smoothtransition to the environment of the intensive careunit. Recent data suggest that such a process canalleviate some of the stress related to carryinga fetus with HLHS.50 Prenatal diagnosis of HLHS hasalso been shown to result in improved physiologicalstate prior to surgery51 and improved surgical out-come.52 The potential impact of prenatal diagnosisof HLHS on some of the long-termmorbidities listedabove, particularly neurocognitve outcome, is un-known; however, a positive influence is expected.
References
1. Spray TL. Stage I reconstruction. In: Rychik J, Wernovsky G,editors. Hypoplastic left heart syndrome. Boston/Dordrecht/London: Kluwer Academic Publishers; 2003.p. 89e105.
2. Mahle WT, Spray TL, Wernovsky G, Gaynor JW, Clark 3rd BJ.Survival after reconstructive surgery for hypoplastic leftheart syndrome: a 15-year experience from a single institu-tion. Circulation 2000;102(Suppl. 3):III136e41.
3. Gaynor JW, Mahle WT, Cohen MI, Ittenbach RF,DeCampli WM, Steven JM, et al. Risk factors for mortalityafter the Norwood procedure. Eur J Cardiothorac Surg2002;22:82e9.
4. Hoffman JI, Kaplan S, Liberthson RR. Prevalence of congen-ital heart disease. Am Heart J 2004;147:425e39.
5. Natowicz M, Kelley RI. Association of Turner’s syndromewith hypoplastic left heart syndrome. Am J Dis Child1987;141:218e20.
6. Natowicz M, Chatten J, Clancy R, Conard K, Glauser T,Huff D, et al. Genetic disorders and major extra-cardiacanomalies associated with the hypoplastic left heart syn-drome. Pediatrics 1988;82:698e706.
7. Boughman JA, Berg KA, Astemborski JA, Clark EB,McCarter RJ, Rubin JD, et al. Familial risks of congenitalheart defects assessed in a population based epidemiologicstudy. Am J Med Genet 1987;26:839e49.
8. Rosenthal GL. Patterns of prenatal growth among infantswith cardiovascular malformations: possible fetal hemody-namic effects. Am J Epidemiol 1996;143:505e13.
9. Hornberger LK, Sahn DJ, Kleinman CS, Copel JA, Reed KL.Tricuspid valvediseasewith significant tricuspid insufficiencyin the fetus: diagnosis and outcome. J Am Coll Cardiol 1991;17:167e73.
10. Levin MD, Gaynor JW, Tian Z, Cohen MS, Donaghue DD,Spray TL, et al. Prevalence of perinatal atrioventricularvalve regurgitation in the single ventricle: from the fetus,through birth, and initial palliative surgery. J Am Soc Echo-cardiogr 2004;17:495 [abstract].
11. Rasanen J, Wood DC, Weiner S, Ludomirski A, Huhta JC.Role of the pulmonary circulation in the distribution ofhuman fetal cardiac output during the second half of preg-nancy. Circulation 1996;94:1068e73.
Practice points
1) Currently multiple techniques for pallia-tion of HLHS with relatively good survival
2) Neurocognitive testing and surveillance isindicated in children with HLHS
Research directions
1) Improved understanding of the develop-ment of HLHS during fetal life
2) Long-term follow up and adult outcome ofsurvivors of HLHS
Hypoplastic left heart syndrome 565
12. Rychik J, Rome JJ, Collins MH, DeCampli WM, Spray TL. Thehypoplastic left heart syndrome with intact atrial septum:atrial morphology, pulmonary vascular histopathology andoutcome. J Am Coll Cardiol 1999;34:554e60.
13. Chintala K, Tian Z, Donaghue DD, Thomas RL, Rychik J.Fetal pulmonary venous Doppler patterns in hypoplasticleft heart syndrome: relationship to atrial septal restric-tion. J Am Coll Cardiol 2004;43(Suppl. A):381A [abstract].
14. Vlahos AP, Lock JE, McElhinney DB, van der Velde ME. Hypo-plastic left heart syndrome with intact or highly restrictiveatrial septum: outcome after neonatal transcatheter atrialseptostomy. Circulation 2004;109:2326e30.
15. Marshall AC, van der Velde ME, Tworetzky W, Gomez CA,Wilkins-Haug L, Benson CB, et al. Creation of an atrial sep-tal defect in utero for fetuses with hypoplastic left heartsyndrome and intact or highly restrictive atrial septum. Cir-culation 2004;110:253e8.
16. Donofrio MT, Bremer YA, Schieken RM, Gennings C, Morton LD,Eidem BW, et al. Autoregulation of cerebral blood flow in fe-tuses with congenital heart disease: the brain sparing effect.Pediatr Cardiol 2003;24:436e43.
17. Kaltman JR, Di H, Tian Z, Rychik J. Impact of congenitalheart disease on cerebrovascular blood flow dynamics inthe fetus. Ultrasound Obstet Gynecol 2005;25:32e6.
18. Shillingford AJ, Marino BS, Ittenbach RF, Fedec A, Rychik J,Clancy RR, et al. Microcephaly is common in neonateswith hy-poplastic left heart syndrome. Pediatr Cardiol 2005;25:581A.
19. Norwood WI, Lang P, Hansen DD. Physiologic repair of aorticatresia e hypoplastic left heart syndrome. N Engl J Med1983;308:23e6.
20. Chrisant MR, Naftel DC, Drummond-Webb J, Chinnock R,Canter CE, Boucek MM, et al. Fate of infants with hypoplasticleft heart syndrome listed for cardiac transplantation: amul-ticenter study. J Heart Lung Transplant 2005;24:576e82.
21. Akintuerk H, Michel-Behnke I, Valeske K, Mueller M, Thul J,Bauer J, et al. Stenting of the arterial duct and banding ofthe pulmonary arteries: basis for combined Norwood stage Iand II repair in hypoplastic left heart. Circulation 2002;105:1099e103.
22. Galantowicz M, Cheatham JP. Lessons learned from the de-velopment of a new hybrid strategy for the management ofhypoplastic left heart syndrome. Pediatr Cardiol 2005;26:190e9.
23. Ishino K, Stumper O, De Giovanni JJ, Silove ED, Wright JG,Sethia B, et al. The modified Norwood procedure for hypo-plastic left heart syndrome: early to intermediate results of120 patients with particular reference to aortic arch repair.J Thorac Cardiovasc Surg 1999;117:920e30.
24. Sano S, Ishino K, Kado H, Shiokawa Y, Sakamoto K, Yokota M,et al. Outcome of right ventricle-to-pulmonary artery shunt infirst-stage palliation of hypoplastic left heart syndrome:a multi-institutional study. Ann Thorac Surg 2004;78:1951e7.
25. Pizarro C, Mroczek T, Malec E, Norwood WI. Right ventricleto pulmonary artery conduit reduces interim mortality afterstage 1 Norwood for hypoplastic left heart syndrome. AnnThorac Surg 2004;78:1959e63.
26. Mahle WT, Spray TL, Gaynor JW, Clark 3rd BJ. Unexpecteddeath after reconstructive surgery for hypoplastic left heartsyndrome. Ann Thorac Surg 2001;71:61e5.
27. Karl TR. The bidirectional cavopulmonary shunt. In:Rychik J, Wernovsky G, editors. Hypoplastic left heart syn-drome. Boston/Dordrecht/London: Kluwer Academic Pub-lishers; 2003. p. 129e49.
28. Nurnberg JH, Ovroutski S, Alexi-Meskishvili V, Ewert P,Hetzer R, Lange PE. New onset arrhythmias after the ex-tracardiac conduit Fontan operation compared with the
intraatrial lateral tunnel procedure: early and midterm re-sults. Ann Thorac Surg 2004;78:1979e88.
29. Gaynor JW, Bridges ND, Cohen MI, Mahle WT, DeCampli WM,Steven JM, et al. Predictors of outcome after the Fontan op-eration: is hypoplastic left heart syndrome still a risk factor?J Thorac Cardiovasc Surg 2002;123:237e45.
30. Hijazi ZM, Fahey JT, Kleinman CS, Kopf GS,Hellenbrand WE. Hemodynamic evaluation before and afterclosure of fenestrated Fontan. An acute study of changes inoxygen delivery. Circulation 1992;86:196e202.
31. Yang SG, Clark BJ, Gaynor JW, Spray TL, Rychik J. Rate ofspontaneous closure of fenestration in the modified Fontanoperation. Circulation 1999;100(Suppl. 1):I-399.
32. Joshi VM, Carey A, Simpson P, Paridon SM. Exercise perfor-mance following repair of hypoplastic left heart syndrome:a comparison with other types of Fontan patients. PediatrCardiol 1997;18:357e60.
33. Cohen MI, Rhodes LA. Sinus node dysfunction and atrialtachycardia after the Fontan procedure: the scope of theproblem. Semin Thorac Cardiovasc Surg Pediatr Card SurgAnnu 1998;1:41e52.
34. Coon PD, Rychik J, Novello RT, Ro PS, Gaynor JW, Spray TL.Thrombus formation after the Fontan operation. AnnThorac Surg 2001;71:1990e4.
35. Odegard KC, McGowan Jr FX, Zurakowski D, Dinardo JA,Castro RA, del Nido PJ, et al. Procoagulant and anticoagu-lant factor abnormalities following the Fontan procedure:increased factor VIII may predispose to thrombosis. JThorac Cardiovasc Surg 2003;125:1260e7.
36. Odegard KC, McGowan Jr FX, Zurakowski D, DiNardo JA,Castro RA, del Nido PJ, et al. Coagulation factor abnormal-ities in patients with single-ventricle physiology immedi-ately prior to the Fontan procedure. Ann Thorac Surg2002;73:1770e7.
37. Jacobs ML, Pourmoghadam KK, Geary EM, Reyes AT,Madan N, McGrath LB, et al. Fontan’s operation: is aspirinenough? Is coumadin too much? Ann Thorac Surg 2002;73:64e8.
38. Rychik J, Spray TL. Strategies to treat protein-losing enter-opathy. Semin Thorac Cardiovasc Surg Pediatr Card SurgAnnu 2002;5:3e11.
39. Mertens L, Hagler DJ, Sauer U, Somerville J, Gewillig M. Pro-tein-losing enteropathy after the Fontan operation: an in-ternational multicenter study. J Thorac Cardiovasc Surg1998;115:1063e73.
40. Rychik J, Rome JJ, Jacobs ML. Late surgical fenestration forcomplications after the Fontan operation. Circulation 1997;96:33e6.
41. Wernovsky G, Shillingford AJ, Gaynor JW. Central nervoussystem outcomes in children with complex congenital heartdisease. Curr Opin Cardiol 2005;20:94e9.
42. Mahle WT, Clancy RR, Moss EM, Gerdes M, Jobes DR,Wernovsky G. Neurodevelopmental outcome and lifestyle as-sessment in school-aged and adolescent children withhypoplastic left heart syndrome. Pediatrics 2000;105:1082e9.
43. Goldberg CS, Schwartz EM, Brunberg JA, Mosca RS, Bove EL,Schork MA, et al. Neurodevelopmental outcome of patientsafter the fontan operation: a comparison between childrenwith hypoplastic left heart syndrome and other functionalsingle ventricle lesions. J Pediatr 2000;137:646e52.
44. Ikle L,HaleK,FashawL,BoucekM,RosenbergAA.Developmen-tal outcome of patients with hypoplastic left heart syndrometreated with heart transplantation. J Pediatr 2003;142:20e5.
45. Glauser TA, Rorke LB, Weinberg PM, Clancy RR. Congenitalbrain anomalies associated with the hypoplastic left heartsyndrome. Pediatrics 1990;85:984e90.

566 J. Rychik
46. Clancy R. Neurological issues. In: Rychik J, Wernovsky G,editors. Hypoplastic left heart syndrome. Boston/Dordrecht/London: Kluwer Academic Publishers; 2003. p. 251e73.
47. Mahle WT, Tavani F, Zimmerman RA, Nicolson SC, Galli KK,Gaynor JW, et al. An MRI study of neurological injury beforeand after congenital heart surgery. Circulation 2002;106(Suppl. 1):I109e14.
48. Galli KK, Zimmerman RA, Jarvik GP, Wernovsky G,Kuypers MK, Clancy RR, et al. Periventricular leukomalaciais common after neonatal cardiac surgery. J Thorac Cardio-vasc Surg 2004;127:692e704.
49. Gaynor JW, Gerdes M, Zackai EH, Bernbaum J,Wernovsky G, Clancy RR, et al. Apolipoprotein E genotype
and neurodevelopmental sequelae of infant cardiac sur-gery. J Thorac Cardiovasc Surg 2003;126:1736e45.
50. Sklansky M, Tang A, Levy D, Grossfeld P, Kashani I,Shaughnessy R, et al. Maternal psychological impact of fetalechocardiography. J Am Soc Echocardiogr 2002;15:159e66.
51. Verheijen PM, Lisowski LA, Stoutenbeek P, Hitchcock JF,Brenner JI, Copel JA, et al. Prenatal diagnosis of congenitalheart disease affects preoperative acidosis in the newbornpatient. J Thorac Cardiovasc Surg 2001;121:798e803.
52. Tworetzky W, McElhinney DB, Reddy VM, Brook MM,Hanley FL, Silverman NH. Improved surgical outcome afterfetal diagnosis of hypoplastic left heart syndrome. Circula-tion 2001;103:1269e73.