Embed Size (px)
Citation preview

1
Hypothermie accidentelle
Nicolas DeyeRéanimation Médicale et ToxicologiqueUniversité Paris VII, Inserm U942, Hôpital Lariboisière, [email protected]
HYPOTHERMIEACCIDENTELLE :quoi de neuf ?
Hypothermie accidentelle
Les vertus du froid !
Hypothermie accidentellespontanée et non contrôlée
(non intentionnelle)
Hypothermie thérapeutiqueinduite et contrôlée
Arrêt cardiaque +++Encéphalopathie néonatale

2
HYPOTHERMIA & CARDIAC ARREST
ACCIDENTAL HYPOTHERMIAPUBMED
0
200
400
600
800
1000
1200
1400
1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Acci
dent
al H
ypot
herm
ia
Year
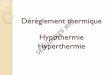
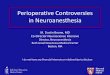
« AccidentalHypothermia » (MESH) : 575 articles0 « Guidelines » ; 6 essais contrôlés non randomisés« MountainRescue » : 59 articles3 « Guidelines »(ICAR MEDCOM) ; 0 essai contrôlé

3
ACCIDENTAL HYPOTHERMIAPUBMED
0
200
400
600
800
1000
1200
1400
1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Acci
dent
al H
ypot
herm
ia
Year
0
200
400
600
800
1000
1200
1400
1600
1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Non
ther
apeu
tic h
ypot
herm
ia
Year
NON THERAPEUTIC HYPOTHERMIAMESH
« AccidentalHypothermia » (MESH) : 575 articles0 « Guidelines » ; 6 essais contrôlés non randomisés« MountainRescue » : 59 articles3 « Guidelines »(ICAR MEDCOM) ; 0 essai contrôlé
Hypothermie accidentelle• EPIDEMIOLOGIE
• NORMOTHERMIE, HYPOTHERMIE &
THERMOREGULATION
• MESURE DE LA TEMPERATURE
• ELEMENTS CLINICO-BIOLOGIQUES
• PRONOSTIC, THERAPEUTIQUE
NEWS

4
Hypothermie accidentelle• EPIDEMIOLOGIE
• NORMOTHERMIE, HYPOTHERMIE &
THERMOREGULATION
• MESURE DE LA TEMPERATURE
• ELEMENTS CLINICO-BIOLOGIQUES
• PRONOSTIC, THERAPEUTIQUE
NEWS

5
Thermolyse :• Radiation (radiations électromagnétiques, infrarouges) 50-70%• Conduction (diffusion par contact physique) Négligeable• Convection (renouvellement surface et air au contact) 20-30%• Évaporation (sudation, perspiration) 15% (5, 10%)
Polderman K
55-60%20-27%10-15%air, eau
Danzl&Pozos, NEJM 1994
Baisse de thermogénèseAugmentation des pertes caloriques
Anomalies de thermorégulationAutres pathologies prédisposantes

6
Hypothermie accidentelle
Facteurs favorisant la survenue d’‛une HA ?
Danzl&Pozos, NEJM 1994
Hypothermie accidentelle
Mortalité selon la température extérieure à Paris de 1991-1995
Laaidi, Int J Biometeorol, 2006
Froid et santé publique (France)
Hypothermie = 1% des décès attribuables au froid dans les pays tempérés (hypothermie urbaine)
Décès par hypothermie rares en France :
- touche une partie réduite de la population(population défavorisée, âgée, avec FDR de diminution de la thermo-stabilité)
- prévention possible : Plan Urgence Hivernal

7
Hypothermie accidentelleHypothermie à Paris(n=81, 17 ans)
Co-morbidités : outdoor (extérieur) = OH, intoxicationindoor (domicile) = sepsis, troubles psychiatriques
Mégarbane B. ICM 2000
Hypothermie accidentelle
Étude des facteurs pronostiques de mortalité
OR
Hypothermie à domicile 7,4
Age ≥ 80 ans 2,4
Ventilation mécanique 2,0
Analyse multivariée (+ SAPS II)

8
Hypothermie accidentelle
Hypothermie accidentelle
Silfvast T. Resuscitation 2003
Hypothermie en Finlande
(23 AC réfractaires)n=75

9
Hypothermie accidentelle
Silfvast T. Resuscitation 2003
(23 AC réfractaires)n=75
Hypothermie en Finlande
Hypothermie accidentelle
HA & traumatologie Jurkovich(J Trauma 1987) : ISS > 25 & T° <32° = 100% mortalitéMartin (Shock 2005) : ISS, acidose, durée de VM & mortalité élevésWang(Crit Care Med 2005)
Polytraumatisme&hypothermie (< 32°C) = gravité extrême (mortalité : 35-50%)

10
Hypothermie accidentelle• EPIDEMIOLOGIE
• NORMOTHERMIE, HYPOTHERMIE &
THERMOREGULATION
• MESURE DE LA TEMPERATURE
• ELEMENTS CLINICO-BIOLOGIQUES
• PRONOSTIC, THERAPEUTIQUE
NEWS
Hypothermie accidentelleTempérature normale ?Villers. CNERM. 2003 36,6 0,4°CDeux compartiments thermiques :- Périphérique (peau, extrémités), 2 à 4 °C inférieur à- Central = “core” (tronc, tête sauf peau)
Holtzclaw. Sessler. 2000 37,0 0,6°CStrictement régulée (homéostasie thermique)
Variations circadiennes

11
Hypothermie accidentelle
Maintien de la température corporelle (homéothermie)
PRODUCTION OU GAIN DE CHALEUR
PERTES DE CHALEUR
Températurecentrale
THERMOGENESE THERMOLYSE
Thermorégulation
Hypothermie accidentelle
Homéothermie - Hypothermie
Zone de
thermorégulation
Zone de confort thermique
Homéothermie NEUTRALITE
CONTRAINTE CHAUDE
CONTRAINTE FROIDE
Dépassement de la thermorégulation Hyperthermie
Dépassement de la thermorégulation Hypothermie
Hypothermie = baisse de la températurecentrale ≤ 35°C

12
Hypothermie accidentelle
Systèmes mis en jeu en réponse au froid
Libérationthyroxine
Seuils : vasomoteur 1°C > frisson (35-36°C)
Frisson disparaît <30 (-32) °C
Fibres spino-thalamiques
Température, VO2, VCO2 et frissons = liés

13
Hypothermie accidentelle
Seuils de sensation du refroidissement cutané est fonction de la température ambiante
Hypothermie accidentelleCLASSIFICATION
• Hypothermie avec immersion suraiguë dans l'eau glacialeprivation d‘O2 possible jusqu'à 1 heure avec récupération neurologique complète
• Hypothermie d'immersion aiguë: eau froide,avalancherefroidissement rapide, pas d’‛épuisement énergétique ni hypovolémie(peu de mouvements entre secteurs vasculaires et extravasculaires nihyperdiurèse).
• Hypothermie aiguë intriquée, en quelques heuresmouvements entre les secteurs liquidiens et hyperdiurèse ++
(Lloyd AccidentalHypothermiaResuscitation 1996)
• Hypothermie subaiguë d'épuisementexposition prolongée (plusieurs heures) à froid moins sévère avec perte
énergétique, hypovolémie.
• Hypothermie subaiguë lente: personne âgée, fréquentes enmilieu urbain, exposition à froid modéré sur plusieurs jours, avec déplacementliquidien

14
Hypothermie accidentelle
CDC (1999) et AHA (2005) :"légère" 34 – 35 °Cmodérée 30 – 34 °Csévère < 30 °C
CNERM (2003-2009) :"modérée" 32 – 35 °Csévère de 28 - 32°Cmajeure ou profonde < 28 °C
SFAR-SRLF (1997-2010) :"légère" 32 – 35°Cmodérée 28 – 32°Csévère 24 - 28°Cprofonde < 24 °C
ERC (2005) :"légère" 32 – 35°Cmodérée 30 – 32°Csévère < 30°C
DEFINITION (1)
Accidental HypothermiaDanzl & PozosNEJM 1994
VillersCNERM 2003-09
?
Circulation 2005
BriotRéanimation2010
Hypothermie accidentelle
ERC (2010) :
Légère 32 – 35 °CModérée 28 – 32 °CSévère ou "majeure" (± profonde) < 28°C
DEFINITION (2)
DanzlAccidental
HypothermiaTextbook 2007

15
Hypothermie accidentelle
"TH" Targetted
Management Temperature
NEJM 2010 Holzer, CCM 2011 Nunnally
Safar P. Textbook of Neuroanesthesia with Neurosurgical and Neuroscience Perspectives. 1997.Polderman K. Intensive Care Med. Part 2. 2004.Sterz F, Behringer W, Holzer M. Acute Cardiac Care. 2006.
Hypothermie thérapeutique légère <35°C (95°F), >32° (90°F)
HT induite par un peptide
analogue de la neurotensine
(NT77)
Expérimental (rat)
- NT = efficace pour induire l’‛HT-Meilleure pour prévenir l’‛ischémie neuronale (long terme) - TH prolongée (24H) + efficace que courte période (4H)
Crit Care Med 2004

16
Nature Novembre 2009
10 rats
Hypothermie accidentelle• EPIDEMIOLOGIE
• NORMOTHERMIE, HYPOTHERMIE &
THERMOREGULATION
• MESURE DE LA TEMPERATURE
• ELEMENTS CLINICO-BIOLOGIQUES
• PRONOSTIC, THERAPEUTIQUE
NEWS

17
Hypothermie accidentelle
Comment mesurer ? Comment monitorer ?
Diagnosticpréhospitalier ?Température épitympanique à sonde valide si pas d’‛AC et au contact du tympan(ne pas se fier aux thermomètres tympaniques infrarouges standard : temp. ambiante, cerumen, technique rigoureuse…)
Température vésicale(sans risque mais difficile…)
Température naso-pharyngée +
Température rectale et "thermomètre hypothermique"(sans risque mais… sonde souple insérée suffisamment de10-15cm)
Métraux plus fabriqué(400 euros)
700 euros

18
Pas de sonde oesophagienne(ni SNG)sauf si patient déjà en AC car risque d’‛arythmie (FV) si < 30°C (Ricard-Hibon SFAR 2006)
Pas de KT artériel pulmonaire(ni VV en territoire cave sup.)Physiologique mais risque de troublesdu rythme et de perforation cardiaque x 5 (Cohen, 1991, J CardioVascAnesth)
Diagnosticpréhospitalier ?
Pas de température cutanée (axillaire…) car = temp. périphérique (gradient vs centrale)
Pas de température cérébrale disponible en routine(hypothalamus, bulbe jugulaire)
ZeinerResu 10
Hypothermie accidentelle
AxillaireUrinaireTympanique
versus température sanglante (n=110) CCM 2007
Quel monitorage ?(recommandé dans l’‛HT et au bloc)

19
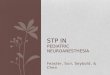
Hypothermie accidentelleTvésicale(n=398), Taxillaire(n=394), Tesophage(n=347) et Tsang (n=143) corrélées si variation thermique modérée (p<0,0001).
Corrélations plus étroites entre Tv / Ts (R2=0,95) et Tv / Te (R2=0,89) qu’‛entre Tv / Ta (R2=0,79).
Corrélations + étroites entre Te / Ts (R2=0,92) qu’‛entre Te / Ta (R2=0,78).
Moins bonne corrélation entre Ta et Ts (R2=0,73).
-3
-2
-1
0
1
2
3
31 32 33 34 35 36 37 38
Moyenne des températures Ts/Tv (°C)
Diff
éren
ce d
es te
mpé
ratu
res
Ts-T
v (°
C)
-3
-2
-1
0
1
2
3
31 32 33 34 35 36 37
Moyenne des températures Ts/Te (°C)
Diff
éren
ce d
es te
mpé
ratu
res
Ts-T
e (°
C)
-3
-2
-1
0
1
2
3
31 32 33 34 35 36 37 38
Moyenne des températures Ts/Ta (°C)
Diff
éren
ce d
es te
mpé
ratu
res
Ts-T
a (°
C)
Deye, Resuscitation, 2008
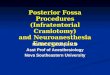
Hypothermie accidentelle
Temperature vessie / oesophagesi variations thermiquesrapides
30
31
32
33
34
35
36
37
38
03:3
0
04:0
0
04:3
0
05:0
0
05:3
0
06:0
0
06:3
0
07:0
0
07:3
0
Tem
pera
ture
(°C
)
Time
Tesophageal Tbladder
EMCOOLS
04:37 start cooling at 35.8°C to 33.0°C in 46 min = 3.7°C/h
warming
33°C
34.3°C

20
Hypothermie accidentelle
ECMO ≅ bulbe jugulaire >esophage≅ nasophar. > vessie ≅ rectalSurestimat° temp. au refroidissemt; sous estimat° au réchauffemt
NussmeierAnesthAnalg 2006
Fiabilité de la mesure de température ?Akata et al. J ThoracCardiovascSurg. 2007
N=20
Bulbe jugulaire : JBT (>) artère pulmonaire : PAT
Naso-pharyngienne: NPT >Foreheaddeep tissue : FHDTT
> vésicale : UBT
Tympanique (peu fiable : cerumen…)
Rectale (peu fiable isolation par matière fécale)
Cutanée : FSST (pas fiable)
Fiab
ilité
mes
ure
t°

21
Hypothermie accidentelle• EPIDEMIOLOGIE
• NORMOTHERMIE, HYPOTHERMIE &
THERMOREGULATION
• MESURE DE LA TEMPERATURE
• ELEMENTS CLINICO-BIOLOGIQUES
• PRONOSTIC, THERAPEUTIQUE
NEWS
Durrer B, Brugger H, Syme D.The Medical On Site Treatment of Hypothermia. 1998
Tempér. centrale ( C)
HT I Conscience conservée avec frissons 35 - 32
HT II Conscience altérée ; arrêt des frissons 32 - 28
HT III Coma 28 – 24
HT IV Mort apparente 24 – 15 ?
HT V Mort par hypothermieirréversible< 15 ? (< 9 ?)
SYMPTOMATOLOGIE CLINIQUE
Seuils (neuro : frissons / cardio : FV) : 32 / 30 /28°CGravité : disparition du frisson (30-32°C) = dépassement des défenses
Faire la part entre conséquence de l‘HA et autre cause associée:hypothermie = cause ou conséquence de l’‛état de mort apparente ?

22
Hypothermie accidentelle
Temperature thresholds where effects (and their intensity) appear are variable from a patient to another.
They are influenced by age, degree of hypothermia and co-morbidities (cardiovascular diseases).
Hypothermie accidentelle
Manifestations cliniquesNeurologiques, hémodynamiques, rénaux, immuno-hématologiques,
digestifs, métaboliques, pharmacologiques

23
Hypothermie accidentelle
Manifestations cliniquesBriot et al. Réanimation 2010.
Diminution progressive des activités enzymatiquesTempérature corporelle Signes neurologiques Signes respiratoires Signes cardiovasculaires
35–32°C (hypothermie légère) Baisse de la vigilanceDysarthrie
Polypnée transitoire Tachycardie et HTA transitoires
32–28°C (hypothermie modérée) État stuporeuxArrêt du frissonHypertonie
Bradypnée progressive Bradycardie progressiveAnomalies électriques (risque de fibrillation)
28–24°C (hypothermie sévère) ComaTrismusMydriase aréactive
Bradypnée extrême Abolition des pouls périphériquesBradycardie extrême
<24°C (hypothermie profonde) Coma aréactif Arrêt respiratoire Arrêt circulatoire
infectious
cardiovascular
coagulation
metabolic
electrolytes
sepsis, pneumonia, immunosuppression
coagulopathy, hemorrhage, platelets, WBC (neutro)
Hyperglycemia; cortisol , ASAT, amylase, nor-
adrenalin acidosis (lactates, fatty acid)
ischemia, CI , brady-arrythmias
Potential side effects of hypothermia
Risks
shivering, vasoconstrict°, rhabdomyolysis, coma
renal: hyperdiuresis hypovolemia
Polderman K. Int Care Med 2004.CCM. 2009 pharmacokinetic
respiratory pCO2, pO2 , congestion
K, Ph, Mg, Ca

24
Hypothermie accidentelle
CONSEQUENCES VISCERALES DE L’‛HYPOTHERMIE : NEURO-MUSCULAIRES
Accidental HypothermiaDanzl & PozosNEJM 1994
Épuisement après phase de lutte contre la déperdition de chaleur
Après phase initiale d’‛augmentation de la consommation d’‛O2 de 40-100%,Baisse de5-10% de laVO2 (cérébrale, cardiaque)par baisse de 1°C quand la température< 30-31°C
HA légère
HA modérée-sévère
HA profonde
Hypothermie accidentelle
CONSEQUENCES VISCERALES DE L’‛HYPOTHERMIE : SNC
AccidentalHypothermiaDanzl&PozosNEJM 1994
- Trouble des fonctionssupérieures et de laconscience, léthargie
- Coma (<31-32°C)- Disparition des réflexes
sous-corticaux (risqued’‛inhalation)
- Ralentissement del’‛activité cérébrale àl’‛EEG jusqu’‛à EEG plat

25
INTEREST OF PRE ARREST COOLING
Accidental hypothermia
Therapeutic hypothermia(cardiac arrest, neonatal HIE, CPB)
Protective hypothermia: before CA (accidentalhypoth.)Preservativehypothermia: beforereperfusionResuscitativehypothermia: during/afterreperfusion(before ROSC= early: intra-arrestcooling ; after ROSC= late)
Hypothermie accidentelle
Brain
KidneysLiverGI
1. Flush2. CPB
SpinalCord
LVRV
Preservativehypothermia

26
Hypothermie accidentelle
Joshi B, et al.AnesthAnalg
2010
Autorégulation fonctionnelle (Mx≅ 0 ; meanvelocity index par Doppler)
Anomalies de l’‛autorégulation(Mx 0.3-0.5)
n=11
Hypothermie accidentelle
MODIFICATIONS PHYSIOLOGIQUES ASSOCIEES A L’‛HYPOTHERMIEConséquences cardio-circulatoires
Mattu A. Am J Emerg Med 2002DanzlPozos NEJM 1994
; CVP, SvO2
; ischemia

27
Hypothermie accidentelle
Onde en dos de chameau (onde Δ inversée) ou onde "J" d’‛Osborn : ressaut avec épaulement du bas de la portion descendante de R en forme de crochetage, le + souvent en inféro-latéral (DII et V6). Apparaît si <32ºC et s'accentue si de température (80% si <30°C). Caractéristique mais non spécifique (hypercalcémie, TBI, Prinzmetal). Peut mimer 1 onde de Pardee (aspect d’‛IDM), hyperkaliémie, SDB, repol. précoce
Hypothermie accidentelle
J
ST-
Respecter la bradycardie (atropine, amines, antiarythmiques inefficaces)
Parasitage par les frissons ou les trémulations. Bradycardie sinusale,de PR et QT. TDC.AC/FA lente, TDRV (si < 28°C)Rôle de la T° < 30°C dans la genèse de substrats pro-arythmiques (pacing)
Conséquence d’‛une augmentation du courant des canaux potassiques épicardiquepar rapport au courant endocardique (gradient de voltage trans-mural)
Fox &Sadick. InternalMedicine J. 2008Mareedu. ClinicalMedicine&Research. 2008 Matei. Anesthesiology. 2010
Hsieh. Circ J. 2009

28
Hypothermie accidentelle
Dysfonction systolique mais pas de dysfonction diastolique (12 cochons jusqu’‛à 25°C) : Qc, MAP, VES, indices de contractilité, VTDVG, VTSVG RVS, CaO2 et CvO2 (VO2 )PTDVG constanteAprès réchauffement, VO2 se normalise ; le Qc revient aux valeurs initiales : tachycardie compensatrice ; MAP, VES, RVS restent + bas qu’‛initialement ;; TnT
DYSFONCTION MYOCARDIQUE & HYPOTHERMIE
Filseth et al. 2010. Critical Care
Rôles de la diminution de sensibilité au calcium, accumulation de calcium avec augmentation de la phosphorylation de la cTnI
Han et al. 2010. Am J PhysiolHeartCircPhysiolKontratiev et al. 2008. Cryobiology
Hypothermie accidentelle
6 groupes de rats (3 NT, 3 HT avec adrécroissante : groupes 4 et 5 ; 6 = saline)
Adré pendant l’‛HT : vasoconstriction (5>4>6)avec absence d’‛augmentation du Qc et du VES (groupe 5,6 vs 4)
Dissociation entre les réponses myocardique et vasculaire à basse température
Rôles de la dysfonction myocardique en HT et du changement d’‛affinité des récepteurs adrénergiques (dépendant de T ) ?
HR : NS
MAP4,5 > 6
Han et al. 2008. Cryobiology

29
32 swinesFV = 8 min sans RCPIdem pour défibrillation retardéeIdem pour RASC avec survie H24Coronary perfusion = NSCause : changement mécanique, électrophysio ou métabolique ?
Rhee. 2005Resuscitation
35°C 33°C 30°C
Hypothermie accidentelle
MODIFICATIONS PHYSIOLOGIQUES ASSOCIEES A L’‛HYPOTHERMIEConséquences respiratoires de l’‛hypothermie DanzlPozosNEJM 1994
GDS : Baisse PaO2, PaCO2, AlcaloseHypopnée puis apnée (<25°C)Altération de la régulation du pH (+ 0,015 U / -1°C)
100
80
60
40
20
0
20
16
12
8
4
20 40 60 80 100
SO2(%)
CO2(ml/100ml)
PaO2 mm Hg

30
Hypothermie & PoumonHypoventilation alvéolaireDisparition des reflexes pharyngo-laryngés (coma) : risque
d'inhalationDiminution de l’‛activité ciliaire de l’‛épithélium bronchiqueEffondrement des capacités de résorbtion liquidienne de
l’‛épithélium alvéolaire (SakumaApplPhysiol 1996)
Modification de l’‛humidification des voies aériennes si VM (diminution si filtre humidificateur et majoration si humidificateur chauffant+++) (Lellouche ICM 2006)
Lésion inflammatoire de la barrière capillaro-alvéolairependant le réchauffement (Taniguchi ICM 2007)
Œdème pulmonaire ++Hypotherme< 30°C = détresse respiratoire
Indication large d’‛intubation et de ventilation
HYPOTHERMIE : solubilité plasmatique O2et CO2
pH-Statcorrection à la température réelle
(en VM : on hypoventile)
α-Statrespect de l’‛alcalose hypocapnique ; interprétation GDS = en normothermie
n = 8 strokes
Best CBF

31
HYPOTHERMIE : solubilité plasmatique O2et CO2
pH-Statcorrection à la température réelle
(en VM : on hypoventile)
α-Statrespect de l’‛alcalose hypocapnique ; interprétation GDS = en normothermie
NS J1-2
MABP NS
2010
16 études : pH-stat en pédiatrie et α-stat chez l’‛adulte ?6 en faveur de α-stat, 3 pour pH-stat, 4 NS pour le métabolisme cérébral3 en faveur de α-stat, 3 pour pH-stat, 3 NS pour le devenir neurologique
Meilleure autorégulation cérébrale en α-stat et plus simple
Briot et al. Réanimation 2010.Tremey et Vigue B. AFAR. 2004.
2011n=8
Lowerthresholdnormocapniaisassociatedwithdecreasedcerebralperfusion/oxygenation but not interstitialmetabolites. UpperthresholdpCO2 increasescerebral perfusion and reducedcerebral lactate.

32
Hypothermie accidentelle
Immuno-hematological effects
• Thrombocytopenia (+), thrombopathy.• Coagulation disorders: increase in bleeding time, APTT
and PTT (+). If acidosis, increased disorders.• Bleeding. DIC • Rise in Ht : 2% / -1°C. Hypercoagubility.• Leukocytopenia (+ neutrophil).• Impaired coagulation cascade and impaired platelet,
leukocyte, neutrophil and macrophage functions.• Suppression of pro-inflammatory mediator release.• Increased risk of infection (pneumonia principally).
Polderman K. Intensive Care Med. Part 2. 2004. CCM 2009.Dirkmann et al. AnesthAnalg. 2008.
Straub et al. Europ J CardiothoracSurg 2008.
Side effects of ≤ 35°C AH
Hypothermie accidentelle

33
Hypothermie accidentelle
Accidental HypothermiaDanzl & PozosNEJM 1994
Renal effects• Hypothermia-induced hyper-
diuresis (initial 50% renalblood flow) leading tohypovolemia / oliguria withrenal failure (if no treatment).
• Then renal blood flow (cardiac blood flow)
• Tubular dysfunction andelectrolytes disorders: loss and
levels of K, Mg, Ph, Ca
Side effects of ≤ 35°C AH
HA légère
HA modérée
HA profonde
Hypothermie accidentelle
Side effects of ≤ 35°C AH
Polderman K. Intensive Care Med. Part 2. 2004. Critical Care Med 2009.Deye N, et al. Acute cardiacfailure&neuroprotection. 2007.
Metabolic effects• Decreases in O2 consumption and cellular needs, CO2
production and overall metabolism (80% if < 28°C) except for"fat metabolism": in serum lactate levels, metabolic acidosisand production of free fatty acids, ketones and glycerol.
• Decrease in insulin sensitivity and secretion: insulin resistanceand rise in serum glucose levels.
• Increases of endogen adrenaline, noradrenaline, T3, T4 andcortisol (< 35°C) levels.

34
Hypothermie accidentelle
Side effects of ≤ 35°C AH Splanchnic
• Impaired bowel function and intestinal motility (ileus).• Pancreatitis, increase in serum amylase levels.• Increase in liver enzymes (particularly
aminotransferases).
Pharmacokinetics
• Changes in drug effects and drug metabolism : alteredclearance of various medications (muscle paralyzers,propofol, fentanyl, phenytoin, pentobarbital, verapamil,propanol and volatile anesthetics, etc).
Hypothermie accidentelle
(Zhou 2008)
Seder CCM 2008 (fexofenadine) NishidaBiolPharm Bull 2007
(Tortorici, Poloyac)

35
Hypothermie accidentelle
• Défaillance circulatoire : hypovolémique, cardiogénique.
• Troubles du rythme cardiaque.
• Pneumonie d’‛inhalation / SDRA
• Rhabdomyolyse.
• Insuffisance rénale aiguë.
• Thromboses veineuses périphériques
• Coma postanoxique (AC).
Donc : principales complications