-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
1/30
Hypoxic Ischemic
Encephalopathy
Prof. Saad S Al-AniSenior Pediatric Consultant
Head of Pediatric DepartmentKhorfakkan Hospital . Sharjah
[email protected]
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
2/30
05/26/2010Khorfakkan Hospital Pediatric
Department 2
Ischemia
refers to blood flow to cells or organs that is insufficient
tomaintain their normal function
Definitions
Anoxia
is a term used to indicate the consequences of complete lack of
oxygen as aresult of a number of primary causes
Hypoxia
refers to an arterial concentration of oxygen that is less than
normal
Biagioni E, Mercuri E, Rutherford M, et al: Combined use of
electroencephalogram and magnetic resonance
imaging in full-term neonates with acute encephalopathy.
Pediatrics2001;107:461
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
3/30
05/26/2010Khorfakkan Hospital Pediatric
Department 3
Hypoxic-ischemic encephalopathy
Is an important cause of permanent
damage to CNS cells that may result inneonatal death or be
manifested lateras cerebral palsy or mental deficiency
Nelson Textbook of Pediatrics 19thed.2010 . pages 566 - 568
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
4/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 4
25-30%of survivors are left with permanentneurodevelopmental
abnormalities (cerebralpalsy, mental retardation).
Dixon G, Badawi N, Kurinczuk JJ, et al: Early developmental
outcomes afternewborn encephalopathy. Pediatrics2002;109:26-33
Fifteen to 20%of infants with hypoxic-ischemic encephalopathy
die in the neonatalperiod
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
5/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 5
Effects of Asphyxia
System Effect
I. Central nervous system
1.Hypoxic-ischemic encephalopathy
2.Infarction
3. Intracranial hemorrhage
4.Seizures
5. Cerebral edema
6. Hypotonia
7. Hypertonia
II.Cardiovascular
1.Myocardial ischemia
2. Poor contractility3. Cardiac stun
4. Tricuspid insufficiency
5. Hypotension
Cowan F, Rutherford M, Groenendaal F, et al: Origin and timing
of brainlesions in term infants with neonatal encephalopathy.
Lancet 2003;361:736-
42.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
6/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 6
Effects of Asphyxia
System Effect (cont.)
III. Pulmonary
1. Pulmonary hypertension
2. Pulmonary hemorrhage3. Respiratory distress syndrome
IV. Renal
Acute tubular or corticalnecrosis
V. Adrenal
Adrenal hemorrhage
VI. Gastrointestinal
1. Perforation
2. Ulceration with hemorrhage3. Necrosis
Cowan F, Rutherford M, Groenendaal F, et al: Origin and timing
of brainlesions in term infants with neonatal encephalopathy.
Lancet 2003;361:736-
42.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
7/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 7
Effects of Asphyxia
System Effect (cont.)
VII. Metabolic
1. Inappropriate secretion of antidiuretic hormone
2. Hyponatremia3. Hypoglycemia
4. Hypocalcemia
5. Myoglobinuria
VIII. Integument
Subcutaneous fat necrosis
IX. HematologyDisseminated intravascular coagulation
Cowan F, Rutherford M, Groenendaal F, et al: Origin and timing
of brainlesions in term infants with neonatal encephalopathy.
Lancet 2003;361:736-
42.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
8/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 8
Asphyxia
is considered in infants with:1. Fetal acidosis (pH
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
9/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 9
Causes Of Fetal Hypoxia
(1)Inadequate oxygenation of maternal bloodas a result of:
I. Hypoventilation during anesthesia
II. Cyanotic heart disease
III. Respiratory failureIV. Carbon monoxide poisoning
(2) low maternal blood pressure
as a result of the hypotension that may:
I. Complicate spinal anesthesia
II. Result from compression of the vena cava and aorta by the
gravid
uterus
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
10/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 10
Causes Of Fetal Hypoxia(cont.)
(4) Premature separation of the placenta
Johnson MV: MRI for neonatal encephalopathy in full-term
infants. Lancet 2003;361:713-4
(3) Inadequate relaxation of the uterusto permit placental
filling as a result of uterine tetany caused by the
administration of excessive oxytocin
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
11/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 11
Causes Of Fetal Hypoxia(cont.)
(6) Uterine vessel vasoconstrictionby cocaine
(7) placental insufficiency from numerous causesincluding
toxemia and postmaturity.
Johnson MV: MRI for neonatal encephalopathy in full-term
infants. Lancet 2003;361:713-4
(5) Impedance to the circulation of blood
through the umbilical cord as a result of compression or
knotting of
the cord
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
12/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 12
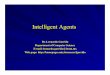
Fetal hypoxia
Nelson Textbook of Pediatrics (on 20 November 2003) 2003
Elsevier
Abnormal Doppler velocimetry.On an umbilical artery Doppler flow
velocity waveform
The umbilical placental impedance is so high that the diastolic
componentshows flow in a reverse direction. This finding is an
indication of severe
intrauterine hypoxia and intrauterine growth restriction.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
13/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 13
Causes of after birth hypoxia
(1)Anemiasevere enough to lower the oxygen content of the blood
to
a critical level, as after severe hemorrhage or hemolytic
disease
(2) Shocksevere enough to interfere with the transport of oxygen
to vital
organs as a result of
i. Overwhelming infection
ii. Massive blood loss
iii. Intracranial or adrenal hemorrhage
Crowley P: Prophylactic corticosteroids for preterm birth.
CochraneDatabase Syst Rev2002;Issue 1. De Felice C, Toti P, Laurini
RN, et al:
Early neonatal brain injury in histologic chorioamnionitis. J
Pediatr2001;138:101
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
14/30
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
15/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 15
The initial circulatory responseof the fetus
* is increased shunting through the ductus venosus, ductus
arteriosus, and foramen ovale
* with transient maintenance of perfusion of the brain, heart,
and
adrenals in preference to the lungs (because of pulmonary
vasoconstriction), liver, kidneys, and intestine.
Pathophysiology
Within minutes of the onset of total fetal hypoxia:
1.Bradycardia
2. Hypotension
3. decreased cardiac output
4. severe metabolic as well as respiratory acidosis occur
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
16/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 16
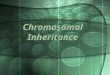
. Hon EH:An Atlas of Fetal Heart Rate Patterns. New Haven,CT,
Harty Press, 1968.)
Patterns of periodic fetal heart rate (FHR)deceleration
Ashows early deceleration occurring during the peak of
uterinecontractions as a result of pressure on the fetal head
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
17/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 17
. Hon EH:An Atlas of Fetal Heart Rate Patterns. New Haven,CT,
Harty Press, 1968.)
Patterns of periodic fetal heart rate (FHR)deceleration
(cont.)
B, Late deceleration caused by uteroplacental insufficiency
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
18/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 18
. Hon EH:An Atlas of Fetal Heart Rate Patterns. New Haven,CT,
Harty Press, 1968.)
Patterns of periodic fetal heart rate (FHR)deceleration
(cont.)
C, Variable deceleration as a result of umbilical cord
compression
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
19/30
05/26/2010 Khorfakkan Hospital PediatricDepartment 19
Clinical Manifestations
Hypoxic-Ischemic Encephalopathy in Term Infants
Signs: Stage 1 Stage 2 Stage 3
I. Level of consciousness
Hyperalert , Lethargic Stuporous coma
II.Muscle tone
Normal Hypotonic Flaccid
III. PostureNormal Flexion Decerebrate
Biagioni E, Mercuri E, Rutherford M, et al: Combined use
ofelectroencephalogram and magnetic resonance imaging in
full-term
neonates with acute encephalopathy. Pediatrics2001;107:461
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
20/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 20
Clinical Manifestations
Hypoxic-Ischemic Encephalopathy in Term Infants(cont.)
Signs: Stage 1 Stage 2 Stage 3
IV. Tendonreflexes
Clonus ,Hyperactive Hyperactive Absent
V. Myoclonus
Present Present Absent
VI. Moro reflexStrong Weak Absent
Biagioni E, Mercuri E, Rutherford M, et al: Combined use
ofelectroencephalogram and magnetic resonance imaging in
full-term
neonates with acute encephalopathy. Pediatrics2001;107:461
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
21/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 21
Clinical Manifestations
Hypoxic-Ischemic Encephalopathy in Term Infants(cont.)
Signs: Stage 1 Stage 2 Stage 3
VII. Pupils
Mydriasis Miosis Unequal Poor light reflex
VIII. Seizures
None Common Decerebration
IX. ElectroencephalographicNormal Low voltage changing Burst
suppression
to seizure activity to isoelectric
Biagioni E, Mercuri E, Rutherford M, et al: Combined use
ofelectroencephalogram and magnetic resonance imaging in
full-term
neonates with acute encephalopathy. Pediatrics2001;107:461
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
22/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 22
Clinical Manifestations
Hypoxic-Ischemic Encephalopathy in Term Infants(cont.)
Signs: Stage 1 Stage 2 Stage 3
X. Duration
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
23/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 23
Treatment
Therapy is supportive and directed at the organ system
manifestations
Careful attention to:
Ventilatory status and adequate oxygenation
Blood volume,
Hemodynamic status
Acid-base balance
Possible infectionis important
Dixon G, Badawi N, Kurinczuk JJ, et al: Early
developmentaloutcomes after newborn encephalopathy. Pediatrics
2002;109:26-33.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
24/30
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
25/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 25
Phenytoin(20 mg/kg loading dose) or lorazepam(0.1 mg/kg) maybe
needed for refractory seizures.
Treatment (cont.)
Seizure activity may be severe and refractory to the usual doses
ofanticonvulsants
Phenobarbital, the drug of choice, is given with an intravenous
loadingdose (20 mg/kg); additional doses of 10 mg/kg (up to 40-50
mg/kg total)
may be needed.
Phenobarbital levelsshould be monitored 24 hr after the loading
doseand maintenance therapy (5 mg/kg/24 hr) are begun
Dixon G, Badawi N, Kurinczuk JJ, et al: Early
developmentaloutcomes after newborn encephalopathy. Pediatrics
2002;109:26-33.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
26/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 26
Prognosis
The outcome of hypoxic-ischemic encephalopathy ranges from
complete
recovery to death
The prognosis depending on:
1.Whether the metabolic and cardiopulmonary complications
(hypoxia, hypoglycemia, shock) can be treated
2. Infant's gestational age
(outcome is poorest if the infant is preterm)
3. Severity of the encephalopathy
Battin MR, Dezoete A, Gunn TR, et al: Neurodevelopmental outcome
of infantstreated with head cooling and mild hypothermia after
perinatal asphyxia.
Pediatrics2001;107:480.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
27/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 27
Severe encephalopathycharacterized by :
1.Flaccid coma
2.Apnea
3.Absence oculocephalic reflexes
4. Refractory seizures
Is associated with a poor prognosis
Prognosis (Cont.)
Battin MR, Dezoete A, Gunn TR, et al: Neurodevelopmental outcome
of infantstreated with head cooling and mild hypothermia after
perinatal asphyxia.
Pediatrics2001;107:480.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
28/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 28
1. A low Apgar score at 20 min
2. Absence of spontaneous respirations at 20 min of age
3. Persistence of abnormal neurologic signs at 2 wk of age
predict death or severe cognitive and motor deficits
Prognosis (Cont.)
Battin MR, Dezoete A, Gunn TR, et al: Neurodevelopmental outcome
of infantstreated with head cooling and mild hypothermia after
perinatal asphyxia.
Pediatrics2001;107:480.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
29/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 29
Brain death
after neonatal hypoxic-ischemic encephalopathy is diagnosed
by:
1. Clinical findings of coma unresponsive to pain, auditory, or
visual stimulation
2. Apnea with Pco2 rising from 40 to over 60 mm Hg
3. Absent brainstem reflexes
(pupil, oculocephalic, oculovestibular, corneal, gag,
sucking)
Prognosis (Cont.)
Battin MR, Dezoete A, Gunn TR, et al: Neurodevelopmental outcome
of infantstreated with head cooling and mild hypothermia after
perinatal asphyxia.
Pediatrics2001;107:480.
-
8/10/2019
hypoxicischemicencephalopathy-100526095658-phpapp02.ppt
30/30
05/26/2010
Khorfakkan Hospital Pediatric
Department 30
Thank you