Embed Size (px)
Citation preview

V. Fiscon
G. Portale
Chirurgia Generale Cittadella
-PADOVA-
I Reinterventi in Urgenza Dopo
Chirurgia Gastrica

‘’Revisional Surgery After Gastrectomy for Gastric Cancer’’
Etoh T et al, Surg Laparosc Endosc Percutan Tech 2010

� Post-operative bleedingDecrease in Hb >1g/dL in 24 hrs + blood loss drainage or
hematemesis or melena
� Esophageal anastomotic leak --- Duodenal stump fistulaLuminal content detected in drains or at the wound site
� Post-operative pancreatic fistulaDark-brown drainage fluid with amylase >3 times n.v.
� Chyle leakMilky fluid in drains >200ml/day with triglyceride lev >110 mg/dL
� Wound infection
� IleusJung M et al,
World J Surg 2012
‘’Definition and Classification of Complications of Gastrectomy for Gastric
Cancer Based on the Accordion Severity Grading System’’

‘’Revisional Surgery After Gastrectomy for Gastric Cancer’’
Etoh T et al, Surg Laparosc Endosc Percutan Tech 2010

Post-operative Abdominal Bleeding
Sites:- Anastomosis (>self-limited)
- Gastroduodenal artery
- Small arteries branching off the middle colic artery
- Short gastric vessels
- >> Spleen (!)
Causes:- Incomplete closure of titanium clips (falls off post-op)
- Heat of ultrasonic shears
- Inadvertent traction on the spleen
Emergency operation: 0.3-27% MORTALITY !
Surgery

‘’Diagnosis and Treatment of Abdominal Arterial Bleeding After Radical
Gastrectomy: Retrospective Analysis of 1875 Resections for Gastric Cancer’’
Yang J et al, J Gastrointest Surg 2016
2003-2013 1875 pts with D2 gastrectomy:
36 abdominal art. bleeding (1.9%); <24 hrs/>24 hrs: 6 (16.7%)/30 (83.3%) pts
Bleeding sites:
common hepatic a. and branches ----- 13 pts
splenic a. ----- 10 pts
peripancreatic aa. ----- 6 pts
other aa. ----- 5 pts
undetermined ----- 2 pts
Treatment:
‘early’ relaparotomy → 16.7% mortality
‘late’ TAE/stent (13 pts); relaparotomy (16 pts); 1 acute
collapse (†) → 36.7% mortality
TEA: trans-catheter arterial embolization

‘’Diagnosis and Treatment of Abdominal Arterial Bleeding After Radical
Gastrectomy: Retrospective Analysis of 1875 Resections for Gastric Cancer’’
Yang J et al, J Gastrointest Surg 2016

Post-operative Anastomotic Bleeding
‘’Endoscopic Treatment and Risk Factors of Post-operative
Anastomotic Bleeding After Gastrectomy for Cancer’’
Kim K et al, Int J Surg 2012
Retrospective Korean single center study 2002-2010
• 2,021 pts: 1,613 subtotal + 418 total gastrx;
• 37% lap
• 7 pts anast. bleeding (0.3%)
Mean time before bleeding: 2.9 dd
Mean hosp stay after endoscopic tx: 8.4 dd

Post-operative Anastomotic Bleeding
Kim K et al, Int J Surg 2012
NO significant
predictive factor on
m(x) analysis
- Age/BMI/Comorbidity
- Lap vs Open
- Type gastrx
- Type anastomosis
- Manual vs. stapler

Anastomotic Leakage (5-8%)
- Antibiotic therapy
- Percutaneous drainage
- Fully-covered self expanding metals stent (SEMS) to help
sealing the defect
- Anastomotic repair if conservative treatment fails
Peritoneal signs (pain, fever, etc) with/out Rx confirmation
Most leaks are minor (!)
Anast. site ‘good’ PRIMARY CLOSURE
Anast. site ‘poor’ Revision/resect. remnant

‘’Covered Self-expanding Stent Treatment for Anastomotic Leakage: Outcomes
in Esophagogastric and Esophagojejunal Anastomoses’’
Hoeppner et al, Surg Endosc 2014
2002-2013 35 pts: - 11 EG anastomosis
- 24 EJ anastomosis, 12 mediastinal + 12 abdominal
[19 first treat. + 5 after surgical failure] + 1 surg ok
EJ pts: 16 one stent; 6 two stents; 2 three stents
Total dd of stent treatment: 23 mediast, 25 abdom
Total dd of hospitalization: 50 mediast, 53 abdom
Sealing rates: 92% EJ mediastinal; 67% EJ abdominal
Complications: dislocation (6/24, 25%), bleeding (2/24, 8.3%),
perforation (3/24, 12.5%), stenosis (3/24, 12.5%)

‘’Self-expanding Metal Stent or Nonstent Endoscopic Therapy: Which is Better
for Anastomotic Leaks After Total Gastrectomy?’’
Shim CN al, Surg Endosc 2014
2002-2013 27 pts: *13 SEMS; 14 NSET ≈80% ≤2cm; all <70% circumf.
*SEMS: self expanding metal stents; NSET: non stent endoscopic therapy
*There were NO NSET-related complications*


‘’Endoscopic Management of Anastomotic Leakage After Gastrectomy
for Gastric Cancer: How Efficacious is it?’’
Kim YJ al, Scand J Gastroenterol 2013
5249 pts radical total/subtotal gastrectomy: 33 anastomotic leakage

‘’Endoscopic Management of Anastomotic Leakage After Gastrectomy
for Gastric Cancer: How Efficacious is it?’’
Kim YJ al, Scand J Gastroenterol 2013
The size of the tissue defect was the only factor significantly related to
complete/incomplete/failed closure

Duodenal Stump Fistula: causes
- Intraoperatively neglected duodenal wall injury by coagulation
or ultrasonic device
- Duodenal stump under pressure for obstruction/malrotation
of the J-J anastomosis or incorrect closure of the meso

Duodenal Stump Fistula: treatment strategies
Surgical procedures:
- Duodenostomy
- Roux-en-Y duodeno-jejunostomy
- Rectus abdominis muscle flap
Percutaneous approach:
- Abscess drainage
- Transhepatic biliary drainage
- Fistula obliteration by cyanoacrylate

Further.....
- Enteral and/or total parenteral nutritionto allow a faster fistula healing and a lower morbidity rate
- Somatostatin (and analogues) to reduce fistula output and shorten healing times
Duodenal Stump Fistula: treatment strategies

‘’Duodenal Fistula After Elective Gastrectomy for Malignant Disease’’
Cozzaglio L et al, J Gastrointest Surg 2010
Retrospective Italian multicenter study
11 centers, 1991-2006
3,785 pts (1,613 total + 2,172 sub-total); 21 cases lap or video-assisted
68 DFs (1.6%), mortality rate 16%
age; serum albumin
- Median time DF onset: day 7 (0-22)
- Median daily output: 290 ml (40-2,200)
- Healing rate 84% after a median of 19 dd (1-1,000)
DF onset/daily output did NOT affect DF time to healing or mortality

Treatment strategies
26 sepsis
1 failure to heal
Surgery:- Peritoneal drainage
- Duodenal suture
- Tube
duodenostomy
- (1) R-en-Y
Somatostatin/Octreotide use: did NOT affect time of DF healing or outcome
31%
Only : 20 (29%)

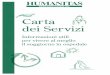
‘’Duodenal Stump Fistula After Gastric Surgery for Malignancies: a
Retrospective Analysis of Risk Factors in a Single Center’’
Orsenigo E et al, Gastric Cancer 2014
1987-2012: 1287 tot/sub-tot gastrectomies x k
Study design:
- 32 (2.5%) pts DSF (duodenal stump fistula)
- 506 pts UPC (uneventful post-op course)
- 268 pts OSC (other major surg. compl.)

STF: duodenal stump fistula Orsenigo E et al, Gastric Cancer 2014
Time trends
Start lap experience, without
routine manual owersewing
5.1%
2.1%2.3% 2.1%
1.2%

Orsenigo E et al, Gastric Cancer 2014
Univariate analysis of surgical variables

Orsenigo E et al, Gastric Cancer 2014
Multivariate analysis for DSF risk factors

Duodenal Stump Fistula
1. Mortality has decreased from 40% (early ‘80s) to 16%
2. Medical therapy is preferred to surgery as first
treatment
3. Surgery is indicated to drain an abscess or to close
defect large/persistent
4. Abdominal sepsis, bleeding or fistulas in neighboring
organs mandate for surgery
5. NG tube suction and fasting has been abandoned in
favor of enteral feeding (related to DF healing)

Post-operative Pancreatic Fistula 1,7-8%
- Frequently followed by contamination pancreatic abscess
- Bleeding from major arteries of abscess can be fatal
- Pancreas-related complications >>> Major cause of mortality!
- Pre-op risk factors: BMI, elderly age
- If uncontrollable by conservative treatment, surgical drainage and
irrigation is necessary
Etoh T et al, Surg Laparosc Endosc Percutan Tech 2010

Other complications…
Bowel obstruction - band lysis
- segmental resection of intestine
- bypass surgery
Bowel perforation - primary closure of perforation site
+ bypass surgery
- segmental resection of intestine

‘’Endoscopic Therapies for Leaks and Fistulas After Bariatric Surgery’’
Swanstron L et al, Surg Innov 2014
Roux-en-Y by pass: 2-5%; Lap sleeve gastrx: 2-3%
Morbidity: 50% Mortality: 5-10%
Up to 50% (!) of pts may be ASYMPTOMATIC (!) with leaks detected only on X-rays

Swanstron L et al, Surg Innov 2014
Early leak:
- Drainage + antimicrobials + nil per os, nutritional (enteral/parenteral) support
closure in 90% of pts within 5 weeks
- Surgical repair with drainage → similar results
But…if surgery is performed after 3 dd or with significant peritoneal contamination
UNLIKELY to succeed (!)
STENTING: - Risk of migration (>40%; lower with covered stents, similar plastic vs.
metallic); repeated endoscopies; bleeding and erosions
- No consensus on timing of removal
GLUE (fibrin or cyanoacrylate): Frequently require multiple applications
CLIPS: Large ‘over the scope’
ENDOSCOPIC SUTURING: Anecdotal…

‘’Endoscopic Management of Bariatric Surgery Complications’’
[Bleeding]
Cai JX et al, Surg Laparosc Endosc Percutan Tech 2016
< 48 hrs after: R-Y Gastric Bypass (1-5%); Sleeve Gastrectomy (0-9%)
Sites: Staple-line; jejuno-jejunostomy; gastric pouch
Management: Conservative tx in stable pts (fluid resusc + PPI + transf.)
Endoscopic therapy (epinephrine inj., thermal coag.,
clipping) but risk of perforation (!) at staple-line or
anastomosis if thermal forces are applied
Reintervention (<20%)

‘’Costs of Leaks and Bleeding After Sleeve Gastrectomy’’
Bransen J et al, Obes Surg 2015
2006-2013: 1260 pts SG
Additional cost: Leak 9284 Euro
Bleeding 4267 Euro

CONCLUSIONI
I Reinterventi in Urgenza Dopo
Chirurgia Gastrica
• Elevata morbilità e mortalità
• Aggressività diagnostica
• Diagnosi precoce
• Approccio multidisciplinare