Embed Size (px)
Citation preview

ICD-10 and Hem/Onc
James S. Kennedy, MD, CCS
CDIMD – Physician Champions
1

Goals • Identify what is new or different in ICD-10 as
compared with ICD-9-CM, emphasizing its impact on • Physician and facility quality and cost-efficiency
measurement • Physician knowledge and work-flow • Physician office and hospital revenue cycles
• Review clinical aspects of the ICD-10 classification and terminology
• Outline St. Joseph’s ICD-10 strategy and plans for engaging the medical staff in ICD-10 documentation and coding integrity
2

Like Explaining the Phone Book Interesting Characters – Terrible Plot
Dictionary without Definitions

International Classification of Disease Versions
• First edition, known as the International List of Causes of Death, was adopted by the International Statistical Institute in 1893
• WHO took in 1948 when the Sixth Revision, which included causes of morbidity for the first time, was published. • 1977 - ICD-9
• 1993 - ICD-10
• 2015 (tentative) - ICD-11
4

Releases of the US Modifications
• ICD-9 • 1977 – Worldwide release
• 1979 – US Modification - Clinical & Mortality
• ICD-10 • 1993 – Worldwide release
• 1999 – US adoption for death certificates
• October 1, 2015 – Use of ICD-10-CM and ICD-10-PCS for clinical use
• ICD-11 • 2017 (if then) - Tentative roll out worldwide
• US adoption (ICD-11-CM and ICD-11-PCS) not likely before 2020 or even 2024
5

US Modifications – ICD-10-CM & PCS The Cooperating Parties
• CDC • Responsible for diagnoses
• CMS • Responsible for inpatient
procedures
• American Hospital Assn. • Responsible for interpreting
ICD-9 or ICD-10 (Coding Clinic)
• American HIM Assn. • Provides input from coding
community
6

ICD-10 Implementation Date October 1, 2015
7
Diagnoses Procedures
ICD-10-CM (Clinical Modification)
Used by all entities: (providers & facilities) for diagnoses To be used in all settings: – Hospital inpatients – Hospital outpatients – Physicians offices – Emergency department – Home health – Long-term care – Rehabilitation facilities
ICD-10-PCS (Procedure Coding System)
Used by inpatient facilities ONLY • Includes outpatient facility services
rendered within the prior 72 hours of writing the inpatient order
• Very different than ICD-9-CM or CPT
CPT • Physician and outpatient/observation
facility services still utilize CPT • CPT does not change!!

ICD-10 Basics
• ICD-10-CM/PCS (and ICD-9-CM) are NOT clinical languages (like SNOMED)
• ICD-9 and ICD-10 are useful for classifying healthcare data for administrative purposes, including reimbursement claims, health statistics, and other uses where data aggregation is advantageous
• ICD-10-CM/PCS is based ONLY on provider documentation of clinical language, not on a patient’s clinical characteristics
• The provider must use the magic words that drive ICD-10-CM/PCS code assignment
8

What’s Old? ICD-9-CM
9

What’s New ICD-10-CM
10

ICD-9 and ICD-10 Diagnoses and Procedures
Code Type ICD-9-CM ICD-10-CM ICD-10 PCS
Diagnosis 14,567 codes 69,832 codes
Inpatient Procedures
3,878 codes 71,920 codes
11

ICD-10-CM Changes • Addition of new conditions since last revision
• New categories for postprocedural disorders
• Addition of laterality (right, left, bilateral)
• Expansion of diabetes and injury codes
• New combination codes
• Greater specificity for current conditions
• Inclusion of trimester in pregnancy codes
• More space to accommodate expansion
12

ICD-10-CM Oncology Issues • Behavior (Histology):
• Malignant (primary, secondary, in-situ)
• Document any secondary sites
• Benign • Unspecified behavior • Of uncertain histological
behavior
• Laterality (specify right/left)
• Anatomical site (topography)
• Include estrogen receptor status (if applicable)
• History of: • Has the malignancy been
excised or eradicated? • Is there still treatment being
provided for the primary and/or metastatic site?
• Is there evidence of remaining malignancy at the primary site?
• Other complications or condition(s) associated with malignancy (dehydration, anemia, etc.)
13

ICD-10-CM Basic Oncology Rules • Chapter 2 of the ICD-10-CM contains the codes for
most benign and all malignant neoplasms. • Certain benign neoplasms, such as prostatic adenomas,
may be found in other specific body system chapters.
• To properly code a neoplasm one must determine from the record if the neoplasm is
• Benign • In-situ • Malignant
• Note also any secondary (metastatic) sties
• Uncertain histologic behavior.
14

ICD-10-CM Chapter 2 Neoplasm Table
15

Overlapping Boundaries
• A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere.
• For multiple neoplasms of the same site that are not contiguous such as tumors in different quadrants of the same breast, codes for each site should be assigned.
16

Disseminated and Unspecified Sites • Disseminated malignant
neoplasm, unspecified • Code C80.0, Disseminated
malignant neoplasm, unspecified, is for use only in those cases where the patient has advanced metastatic disease and no known primary or secondary sites are specified.
• It should not be used in place of assigning codes for the primary site and all known secondary sites.
• Malignant neoplasm without specification of site
• Code C80.1, Malignant (primary) neoplasm, unspecified, equates to Cancer, unspecified. This code should only be used when no determination can be made as to the primary site of a malignancy.
• This code should rarely be used in the inpatient setting.
17

ICD-10-CM Physician Impact
• Claim payment for ancillaries • “Medical necessity” for ordered services is based on an
ICD-9-CM (ICD-10-CM code after October 1, 2015)
• Since payers typically do not release what diagnosis codes support medical necessity, only through payer testing and denials management can revenue losses be mitigated
18

General Equivalence Mapping
Coding should be based on documentation, not mapping
19

General Equivalence Mapping
20
Coding should be based on documentation, not mapping

General Equivalence Mapping
21
Coding should be based on documentation, not mapping

Physician VBP Cost Efficiency
Determine by Care Quality
Observed Cost • Risk Adjusted Cost = -------------------------- Expected Cost Determined by Documentation and ICD-9-CM/ICD-10-CM Code Submission
22

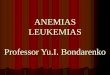
HCC Methodology
Risk factor
No chronic conditions
Base payment
Cancer lung Metastatic
bone cancer
Protein calorie
malnutrition (PCM)
Pressure ulcer, hip
65 y/o female 0.328 0.328 0.328 0.328 0.328
Hx of Breast CA 0.000
Cancer breast present or Rx’d 1.053
Metastasis to bone 2.276 2.276 2.276
Protein calorie malnutrition (PCM) 0.856 0.856
Pressure ulcer, hip 1.153
Total RAF score 0.328 1.381 2.604 3.560 4.713
Predicted
Annual Cost $3280 $13,810 $26,040 $35,560 $47,130

ICD-10-CM - Current malignancy vs. personal history of malignancy • When a primary malignancy has been excised but further
treatment, such as an additional surgery for the malignancy, radiation therapy or chemotherapy is directed to that site, the primary malignancy code should be used until treatment is completed
• For liquid cancers, indicate whether the malignancy is active, in remission, or in relapse
• For solid cancers, any patient receiving adjuvant treatment should be documented as being active, not a “history of malignancy”
• When a primary malignancy has been previously excised or eradicated from its site, there is no further treatment (of the malignancy) directed to that site, and there is no evidence of any existing primary malignancy, a code from category Z85, Personal history of malignant neoplasm, should be used to indicate the former site of the malignancy.
24
Source: ICD-10 Official Guidelines for Coding and Reporting

“History of” vs. Presence of Cancer Coding Clinic, 3rd Q, 2009, pp 3-4 Question: A patient had a malignant breast neoplasm excised three years ago and has completed radiation and chemotherapy.
• Currently there is no evidence of residual disease on exam, on radiographic images or histologically.
• However, the patient is receiving consolidative treatment for breast cancer with Herceptin indicated for five years.
• How is the disease and treatment coded?
Answer: Assign code 174.9, Malignant neoplasm of female breast, unspecified, as the first-listed diagnosis, since Herceptin is considered cancer treatment. Assign code V58.69, Long-term (current) use of other medications, for the Herceptin maintenance.
• Herceptin therapy is not antineoplastic chemotherapy, but is a biological adjuvant treatment for women with breast cancers that are HER2 positive.
• Herceptin is a type of targeted cancer therapy also referred to as a monoclonal antibody.. Herceptin is used to decrease the risk of the cancer recurring, stop cell growth and prevent cancer cells from continuing to grow.

Other Coding Rules
Primary malignancy previously excised • When a primary malignancy has been previously
excised or eradicated from its site and there is no further treatment directed to that site and there is no evidence of any existing primary malignancy, a code from category Z85, Personal history of malignant neoplasm, should be used to indicate the former site of the malignancy.
• Any mention of extension, invasion, or metastasis to another site is coded as a secondary malignant neoplasm to that site. The secondary site may be the principal or first-listed with the Z85 code used as a secondary code.
26

Leukemia, Multiple Myeloma, and Malignant Plasma Cell Neoplasms Remission versus personal history
• The categories for leukemia, and category C90, Multiple myeloma and malignant plasma cell neoplasms, have codes indicating whether or not the leukemia has achieved remission.
• There are also codes Z85.6, Personal history of leukemia, and Z85.79, Personal history of other malignant neoplasms of lymphoid, hematopoietic and related tissues.
• If the documentation is unclear as to whether the leukemia has achieved remission, the provider should be queried.
27

Leukemia Risk Adjustment Active/Remission/Relapse/Cure • APR-DRGs assign lower weights for leukemias that are:
• Chronic (vs. acute) • “In remission” (vs. “not having achieved remission” or “in relapse”) • “Cured” or with a “history of” – meaning that they are completely
cured (no tumor cells at all) or not receiving any treatment
28

Leukemia Remission/Relapse/Cure Definition • Remission - A remission (complete remission) is usually defined as the patient
having no evidence of leukemia after treatment. This means the bone marrow contains fewer than 5% blast cells, the blood cell counts are within normal limits, and there are no signs or symptoms of the disease.
• A molecular complete remission means no evidence of leukemia cells in the bone marrow is found, even when using very sensitive lab tests, such as polymerase chain reaction (PCR). Even when leukemia is in remission, this does not always mean that it has been cured.
• Active disease - Active disease means that either there is evidence that the leukemia is still present during treatment or that the disease has relapsed (come back) after treatment.
• For a patient to be in relapse, more than 5% of the bone marrow must be made up of blast cells
• Minimal residual disease - Minimal residual disease (MRD) is a term used after treatment when leukemia cells can’t be found in the bone marrow using standard lab tests (such as looking at cells under a microscope), but they can still be detected with more sensitive tests (such as flow cytometry or PCR)
• ICD-9-CM and ICD-10 do not recognize the term “minimal residual disease” • The physician must state whether the leukemia is “active”, “in remission”, or “in relapse”
29
Source: American Cancer Society - http://tinyurl.com/kxz6xcq -

Clinical Terminology Remission Category Definition
Complete remission (CR)*
Bone marrow blasts <5 percent; absence of blasts with Auer rods; absence of extramedullary disease; absolute neutrophil count >1.0 x 109/L (1000/µL); platelet count >100 x 109/L (100,000/µL); independence of red cell transfusions
CR with incomplete recovery (CRi)•
All CR criteria except for residual neutropenia (<1.0 x 109/L (1000/µL)) or thrombocytopenia (<100 x 109/L (100,000/µL))
Morphologic leukemia-free stateΔ
Bone marrow blasts <5 percent; absence of blasts with Auer rods; absence of extramedullary disease; no hematologic recovery required
Partial remission (PR)
Relevant in the setting of phase I and II clinical trials only; all hematologic criteria of CR; decrease of bone marrow blast percentage to 5 to 25 percent; and decrease of pretreatment bone marrow blast percentage by at least 50 percent
Cytogenetic CR (CRc)◊ Reversion to a normal karyotype at the time of morphologic CR (or CRi) in cases with an abnormal karyotype at the time of diagnosis; based on the evaluation of 20 metaphase cells from bone marrow
Molecular CR (CRm)§ No standard definition; depends on molecular target
30

Clinical Terminology Treatment Failure Category Definition
Resistant disease (RD)
Failure to achieve CR or CRi (general practice; phase II/III trials), or failure to achieve CR, CRi or PR (phase I trials); only includes patients surviving ≥7 days following completion of initial treatment, with evidence of persistent leukemia by blood and/or bone marrow examination
Death in aplasia
Deaths occurring ≥7 days following completion of initial treatment while cytopenic; with an aplastic or hypoplastic bone marrow obtained within 7 days of death, without evidence of persistent leukemia
Death from indeterminate cause
Deaths occurring before completion of therapy, or <7 days following its completion; or deaths occurring ≥7 days following completion of initial therapy with no blasts in the blood, but no bone marrow examination available
Relapse¥ Bone marrow blasts ≥5 percent; or reappearance of blasts in the blood; or development of extramedullary disease
31

Pediatric Leukemia (ALL) Definitions of Cure
• With improved contemporary therapy, we reassess long-term outcome in patients completing treatment for childhood acute lymphoblastic leukemia (ALL) to determine when cure can be declared with a high degree of confidence
• Multiple studies were cited • These findings demonstrate that with contemporary effective
therapy that excludes cranial irradiation, approximately 6% of children with ALL may relapse after completion of treatment, and those who remain in remission at 4 years post treatment may be considered cured (that is, less than 1% chance of relapse)
32

Pediatric Leukemia (AML) Definitions of Cure
• BACKGROUND: A better understanding of when cure can be declared in childhood acute myeloid leukemia (AML) would reduce anxiety and improve quality of life of AML survivors. The authors determined the likelihood that patients with AML would maintain long-term remission after the completion of therapy.
• METHODS: The cumulative risk of relapse, the time to relapse, event-free survival, and overall survival were analyzed for 604 patients with AML who were enrolled in 7 successive clinical trials divided into 3 treatment eras (1976-1991, 1991-1997, and 2002-2008)
• CONCLUSIONS: Children with AML who receive treatment with contemporary therapy and remain in remission 4 years from diagnosis probably are cured. Although late relapses and late deaths from other causes are rare, long-term follow-up of survivors is necessary for the timely management of late adverse effects.
33

Cancer Cachexia
• Involves ongoing loss of skeletal muscle mass (with or without loss of fat mass) that
○ cannot be fully reversed by conventional nutritional support
○ leads to progressive functional impairment
• Pathophysiology characterized by
○ negative protein and energy balance
○ driven by abnormal metabolism
• Diagnosed by weight loss that is
○ >5% or
○ >2% in patients already showing depletion according to current body weight for height (BMI <20kg/m2) or skeletal muscle mass
34
European School of Oncology Task Force

Malnutrition – 2012 Definition
http://www.tinyurl.com/2012Malnutrition
35

Figure 1. Etiology-based malnutrition definitions.
White J V et al. JPEN J Parenter Enteral Nutr 2012;36:275-
283
Copyright © by The American Society for Parenteral and Enteral Nutrition 36

Malnutrition Diagnosis 2 out of 6 • Insufficient energy intake
• Weight loss
• Loss of muscle mass
• Loss of subcutaneous fat
• Localized or generalized fluid accumulation that may sometimes mask weight loss
• Diminished functional status as measured by handgrip strength
• 2 out of 6 criteria used based on inflammatory status
• Prealbumin and albumin are no longer criteria for malnutrition
37

Malnutrition Criteria
• Acute vs. chronic illness
• Severe vs. non-severe disease
• Albumin/prealbumin don’t matter
http://tinyurl.com/2012malnutrition

Evolving Pediatric Definitions Classification Variable Grade Definition
Gomez (1955) Median WFA (%) Mild 75%–90% WFA
Moderate 60%–74% WFA Severe <60% WFA
Waterlow (wasting) 1972
Median WFH (%)
Mild 80%–89% WFH
Moderate 70%–79% WFH Severe <70% WFH
Waterlow (stunting) 1972
Median HFA (%)
Mild 90%–94% HFA
Moderate 85%–90% HFA
Severe <85% HFA
WHO (wasting) WFH (z scores below median WFH) Moderate z score between −2 and −3
Severe z score <−3
WHO (stunting) HFA (z scores below median HFA) Moderate z score between −2 and −3
Severe z score <−3
Kanawati & McLaren 1970
MUAC divided by HC Mild <0.31
Moderate <0.28
Severe <0.25
Cole (2007) BMI z-scores for age Grade 1 Less than negative 1 Grade 2 Between -2 and -3
Grade 3 Less than negative 3 BMI, body mass index; HC, head circumference; HFA, height-for-age; MUAC, mid–upper arm circumference; WFA, weight-for-age; WFH, weight-for-height; WHO, World Health Organization.

Game Changer Pediatric Malnutrition - 2013
• Published in JPEN in 2013
• http://www.tinyurl.com/2013pedmalnutrition
• Approved by the American Academy of Pediatrics

2013 Pediatric Malnutrition Dependent on BMI z-scores
Malnutrition Severity BMI z-Score
Mild Less than -1
Moderate Between -2 and -3
Severe Less than -3
Note: z-scores are determine by: Age < 2 yrs – WHO charts Age 2-20 yrs – CDC charts
Z-score is determined by age-related BMI charts furnished by the WHO or the CDC

Another Game Changer Pediatric Malnutrition - 2014
• Refinement published in JPEN in 2014
• http://www.tinyurl.com/2014pedmalnutrition
• Approved by the American Academy of Pediatrics

Criteria with 2 points available Parameter Mild Moderate Severe
Weight gain velocity
Age < 2
Less than 75% of the norm for expected weight gain
Less than 50% of the norm for expected weight gain
Less than 25% of the norm for expected weight gain
Weight Loss Age 2-20 5% usual body weight
7.5% usual body weight
10% usual body weight
Deceleration in weight for length/height z score
Decline of 1 z score
Decline of 2 z score
Decline of 3 z score
Inadequate nutrient intake
51%–75% estimated energy/protein need
26%-50% estimated energy/protein need
≤25% estimated energy/protein need

What About Marasmus and Kwashiokor?
• Marasmus - a state in which virtually all available body fat stores have been exhausted due to starvation.
• Conditions that produce marasmus in developed countries tend to be chronic and indolent, such as cancer, chronic pulmonary disease, and anorexia nervosa
• Patients appear starved or “cachetic” • Kwashiorkor - an acute form of protein-energy
malnutrition characterized by edema, irritability, anorexia, ulcerating dermatoses, and an enlarged liver with fatty infiltrates.
• Occurs mainly in connection with acute, life-threatening illnesses such as trauma and sepsis, and chronic illnesses that involve acute-phase inflammatory responses.
• Now called “severe acute malnutrition” http://www.who.int/nutrition/topics/malnutrition/en/index.html
44
Very rare in the United States Probably should not be coded unless deemed to be valid by the provider Surveillance for kwashiorkor is on the 2015 OIG Work Plan

What about Cachexia?
• Sarcopenia • Loss of muscle mass and muscle strength
• Cachexia:
• A multifactorial syndrome characterized by severe body weight, fat and muscle loss and increased protein catabolism due to underlying diseases
• The result of the complex interplay between underlying disease, disease-related metabolic alterations and, in some cases, the reduced availability of nutrients
• Clinical indicators in cancer patients – weight loss that is • >5% or
• >2% in patients already showing depletion according to current body weight for height (BMI <20kg/m2) or skeletal muscle mass
45
1 Muscaritoli M, Anker SD, Argiles J, et. al. Consensus definition of sarcopenia, cachexia, and pre-cachexia. Clinical Nutrition 2010:29(2), pp 154-159. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20060626
2 Aapro, M. et. al. Early recognition of malnutrition and cachexia in the cancer patient: a position paper of a European School of Oncology Task Force. Ann Oncol (2014) 25 (8): 1492-1499. Available at: http://www.tinyurl.com/CaCachexia.

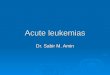
Severity of Illness Determinants Secondary Diagnoses (APR-DRG)
Encounter for Chemotherapy
Leukemia in “Remission”; “History of” Ca
4
3
2
1
0
Leukemia, New Dx or Relapse
Other active malignancies
Pancytopenia due to Chemotherapy Neutropenia, anemia, and/or thrombocytopenia alone has no effect
If pancytopenic, these must also be documented as to be coded
Severe malnutrition
Shock due to IL-2 capillary leak syndrome
7.82
1.92
1.20
1.01
0

Pressure Sores
47
Stage 1 Pressure sores still have weight

New in ICD-10-CM Chronic Non-Pressure Ulcer Codes
• Requires dynamic staging much like pressure ulcers • Different methodology • Note if present on admission
L97111 Non-pressure chronic ulcer of right thigh limited to breakdown of skin
L97112 Non-pressure chronic ulcer of right thigh with fat layer exposed
L97113 Non-pressure chronic ulcer of right thigh with necrosis of muscle
L97114 Non-pressure chronic ulcer of right thigh with necrosis of bone
L97119 Non-pressure chronic ulcer of right thigh with unspecified severity
http://en.wikipedia.org/wiki/File:Neuropathic_heel_ulcer_diabetic.jpg

Skin Ulcers
• Queries may be needed in this circumstance

Admission Review of Systems “Immunocompromised State” • Review of Systems
• Constitutional: Negative. Negative for fever, fatigue and unexpected weight change.
• HENT: Negative. Negative for congestion, sore throat and rhinorrhea.
• Eyes: Negative. Negative for redness. • Respiratory: Negative. Negative for cough and wheezing. • Cardiovascular: Negative. Negative for palpitations. • Gastrointestinal: Negative. Negative for nausea, vomiting,
abdominal pain, diarrhea and constipation. • Endocrine: Negative. • Genitourinary: Negative. • Musculoskeletal: Negative. Negative for joint swelling and
arthralgias. • Skin: Negative. Negative for pallor and rash.
• Allergic/Immunologic: Positive for immunocompromised state.
• Neurological: Negative. Negative for numbness and headaches. • Psychiatric/Behavioral: Negative. Negative for behavioral
problems.
50
ICD-9-CM or ICD-10 does not allow coding of the “immunocompromised host” or “immunocompromised state” when it is due to chemotherapy If it is documented to the disease itself (e.g. uncontrolled diabetes, malnutrition, etc.), documenting and coding it adds relative weight

“Immunocompromised Host” Definition
High Level Immunosupression • With combined primary immunodeficiency
disorder (e.g., severe combined immunodeficiency)
• Receiving cancer chemotherapy • Within 2 months after solid organ
transplantation • With HIV infection with a CD4 T-
lymphocyte count <200 cells/mm3 for adults and adolescents and percentage <15 for infants and children (Definition of AIDS)
• Receiving daily corticosteroid therapy with a dose ≥20 mg (or >2 mg/kg/day for patients who weigh <10 kg) of prednisone or equivalent for ≥14 days, and receiving certain biologic immune modulators, that is, a tumor necrosis factor-alpha (TNF-α) blocker or rituximab
Low Level Immunosupression
• Asymptomatic HIV-infected patients with CD4 T-lymphocyte counts of 200–499 cells/mm3 for adults and adolescents and percentage 15–24 for infants and children,
• Those receiving a lower daily dose of systemic corticosteroid than for high-level immunosuppression for ≥14 days or receiving alternate-day corticosteroid therapy
• those receiving methotrexate (MTX) ≤0.4 mg/kg/week, azathioprine ≤3 mg/kg/day, or 6-mercaptopurine ≤1.5 mg/kg/day
Source: Rubin LG, Levin MJ, et. al. 2013 IDSA Clinical Practice Guideline for Vaccination of the Immunocompromised Host. Clinical Infectious Diseases. Available online at: http://tinyurl.com/ln2b9wx, accessed May 24, 2014
51

MDC 4 – Pneumonia MS-DRG Pneumonia Classifications
Simple pneumonia and pleurisy
MS-DRG 193, 194, 195 (RW 1.0)
Respiratory infections and inflammations
MS-DRG 177, 178, 179 (RW 1.6)
• Viral pneumonia (adenovirus, RSV,
parainfluenza, SARS-associated
coronavirus, influenza)
• Pneumonia due to pneumococcus,
streptococcus, H. flu, mycoplasma, and
chlamydia
• CAP, HAP, lobar, or bronchopneumonia for
which an etiologic organism in the complex
pneumonia category is not explicitly
documented
• Mycoplasma, chlamydia pneumonia
• Pleurisy: adhesions lung or pleura,
calcification pleura, acute, sterile,
diaphragmatic, fibrous, interlobar,
thickening of pleura
• Gram-negative pneumonia
• Salmonella, proteus, serratia,
klebsiella, E. coli, pseudomonas
• Pulmonary tuberculosis
• Fungus and other odd organisms
• Histoplasmosis, blastomycosis,
candidiasis, coccidiomycosis,
tularemia, etc.
• Aspiration PNA, lipoid PNA exogenous,
“detergent asthma”
• Empyema with/without fistula, infected
bacterial pleural effusions, pleurisy with
effusions
• Lung abscess, gangrenous or necrotic
PNA
• Mediastinitis
Note that CAP, HCAP, HAP, or nosocomial pneumonia group to 193, 194, 195

Risk Factors for Higher-Weighted Pneumonias
• Immunocompromised state • Alcoholism • Corticosteroid use • Malignancy • Malnutrition
• Cystic fibrosis • Pseudomonas
• Lung cancer • Higher incidence of GNR & MRSA
• Pleural effusions requiring drainage • pH < 7.20 or glucose < 60 mg/dl
• Necrotizing pneumonia or lung abscess

Pneumonia Antibiotic Utilization Rules of Thumb for >3 days use
• 193–195 Simple pneumonia
“community-acquired pneumonia” • Levaquin – or other fluroquinolone • Claforan®/Rocephin® + Zithromax® combo • Oselatmivir – Influenza w/o bacterial infection
• 177–179 Respiratory infections & inflammations • Doxycycline – Legionnaire’s disease • Clindamycin = anaerobes or staph aureus • Ceftaroline (Teflaro®) – MRSA • Daptomycin – specified gram-positive organisms • Zosyn/Unasyn = Gram-negative rods, aspiration • Zyvox = MRSA, other specified Gram-positives • Aminoglycosides – Gram-negative rods • Fortaz® or Maxipime® – Pseudomonas • Carbepenams – aspiration, pseudomonas, other GNRs • Vancomycin – MRSA or enterococcus (rare) • Amphotericin or fluconazole – Fungus • INH, Rifampin, Ethambutol – Possible TB
Just because a
physician chooses
these antibiotics does
not mean he or she
does not suspect a
more serious cause
Uncertain diagnoses may be coded if documented at the time of discharge
Usually administered
for more than three
days after admission

Medicare-Severity DRG Options MS-DRG
MDC TYPE MS-DRG Title Weights Payment
Base = $7000
Geometric Mean LOS
177 04 MED RESPIRATORY INFECTIONS & INFLAMMATIONS W MCC
1.9492 $13,644 6.2
178 04 MED RESPIRATORY INFECTIONS & INFLAMMATIONS W CC
1.3909 $9,736 5.0
179 04 MED RESPIRATORY INFECTIONS & INFLAMMATIONS W/O CC/MCC
0.9693 $6,785 3.7
193 04 MED SIMPLE PNEUMONIA & PLEURISY W MCC 1.4491 $10,144 4.9 194 04 MED SIMPLE PNEUMONIA & PLEURISY W CC 0.9688 $6,782 3.8 195 04 MED SIMPLE PNEUMONIA & PLEURISY W/O CC/MCC 0.7044 $4,931 2.9
871 18 MED SEPTICEMIA OR SEVERE SEPSIS W/O MV 96+ HOURS W MCC
1.8072 $12,650 5.1
Diagnosis-Related Group methodology • CC = Comorbidity/Complication; MCC = Major CC • Relative weight x base rate = Payment

56

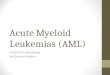
Pediatric Hematology Red Cell Ranges
57
Characteristic Male (n = 5070) Female (n = 5175)
Mean SD 95% CI Mean SD 95% CI Hemoglobin, g/dL•
1 to 2 years 12.01 0.82 10.37 13.65 12.02 0.8 10.42 13.62 3 to 5 years 12.35 0.77 10.81 13.89 12.39 0.77 10.85 13.93 6 to 8 years 12.88 0.8 11.28 14.48 12.82 0.77 11.28 14.36
9 to 11 years 13.28 0.84 11.6 14.96 13.1 0.78 11.54 14.66 12 to 14 years 14.14 1.08 11.98 16.3 13.29 1 11.29 15.29 15 to 19 years 15.07 1.03 13.01 17.13 13.15 1 11.15 15.15
Hematocrit, percent 1 to 2 years 36 2 32 40 36 2 32 40 3 to 5 years 37 2 33 41 37 2 33 41 6 to 8 years 38 2 34 42 38 2 34 42
9 to 11 years 39 2 35 43 39 2 35 43 12 to 14 years 42 3 36 48 40 3 34 46 15 to 19 years 45 3 39 51 39 3 33 45
Anemia - defined as a reduction in red blood cell (RBC) mass, manifested often by a reduction in the hematocrit or hemoglobin by over 2 standard deviation • Mean values vary by
age and gender • Values less than
those in red usually signify anemia
Hollowell JG, van Assendelft OW, Gunter EW, et al. Hematological and iron-related analytes-reference data for persons aged 1 year and over: United States, 1988-94. Vital Health Stat 2005; 11:1

Anemia Specificity APR-DRG impact • Anemia alone usually doesn’t add weight.
• Most anemias with specified causes do add weight
58

Anemia Specificity APR-DRG impact • Anemia alone usually doesn’t add weight.
• Most anemias with specified causes do add weight
59

Pancytopenia vs. Aplastic Anemia • Pancytopenia
• Anemia
• Thrombocytopenia
• Leukopenia
• DRG implications • Documented alone – low
weight
• If due to or induced by chemotherapy or another drug – high weight
• Myelosuppression does not have a code
• Aplastic anemia • Aplastic anemia is
characterized by diminished or absent hematopoietic precursors in the bone marrow, most often due to injury to the pluripotent stem cell.
• The designation "aplastic anemia" is a misnomer because the disorder is defined as pancytopenia rather than anemia
60

Meditech 5.67
61

Pancytopenia vs. Individual Elements
62

DRG Impact
• Principal Diagnosis – Atrial Fibrillation • With neutropenia, anemia, and thrombocytopenia
• MS-DRG 310 – Cardiac arrhythmia and conduction disorder without CC/MCC – RW 0.5893 - $5,893 bundled payment
• With pancytopenia s/p chemotherapy • MS-DRG 309 – Cardiac arrhythmia and conduction disorder
with CC – RW 0.7865 - $7,865 bundled payment
• With pancytopenia due to or induced by chemotherapy or with aplastic anemia due to any drug
• MS-DRG 308 – Cardiac arrhythmia and conduction disorder with MCC – RW 1.2107 - $12,107 bundled payment
63

Root Cause Analysis Provider Issues
• Providers (particularly surgeons) often focus on the principal reason for admissions and do not document additional diagnoses in their admission, progress, or discharge notes with needed specificity
• Problem lists, which are sometimes imported into progress notes as diagnoses, are often not updated as the admission progresses
• Diagnoses that have resolved or not addressed may be carried over into the chart as active issues
• Ancillary (laboratory, pathology, dietary, or imaging) reports are copied into inpatient notes without provider interpretation as documented in the progress note or problem list
• Documentation conflict resolution is not always apparent • Attending physicians do not always rectify inconsistencies between consultant
opinions, resulting in conflicting diagnoses at discharge.

Provider Issues Toxic Encephalopathy
• Patient has ifosfamide neurotoxicity resulting in sedation treated with methylene blue
• Qualifies clinically as a toxic encephalopathy which by itself has a SOI of 3
• Documentation in this record would have increased the SOI from a 2 to a 3
65

66

67

Next Steps
• Ongoing chart review and feedback
• Others