91 Workbook Lesson 2.5 DEFINITIONS OF TERMS Esophagus — the tube that connects the mouth with the stomach. Duodenum — the first section of the small intestine located below the stomach. For a complete list of defined terms, see the Glossary . ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ ______________________________ What is a stomach ulcer? A peptic ulcer is a persistent wound in the lining (epithelium) of the stomach, small intestine or the lower esophagus that does not heal. The epithelium in the stomach is normally resistant to the acid produced during a meal, but the ulcer exposes sensitive tissues. As a result, people with stomach ulcers experience pain, especially during a meal. Ulcers in the small intestines ( duodenal ulcer) are found where food exits from the stomach into the small intestines. In this case, the pain starts about 2–3 hours after a meal when the digested food enters the duodenum. Unlike stomach and LESSON 2.5 WORKBOOK Do bacteria cause stomach ulcers? Applying Koch's postulates This lesson continues to grapple with the problem of arriving at causation from correlation by looking at another infectious agent that presents challenges to fulfilling Koch’s postulates, Helicobacter pylori . H. pylori is thought to cause stomach ulcers, and its discovery revolutionized how we treat ulcers. However, Koch’s postulates have never been fully established for this infectious agent, begging the question — will the future reveal another 'cause' of stomach ulcers? Figure 1: Peptic ulcers are found in different regions of the gastrointestinal tract: the stomach, the duodenum, and occasionally, the lower esophagus.
W o r k b o o k Lesson 2.5
DEFINITIONS OF TERMS
stomach.
Duodenum — the first section of the small intestine located
below
the stomach.
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________
What is a stomach ulcer?
A peptic ulcer is a persistent wound in the lining (epithelium) of
the stomach, small intestine or the lower esophagus that does not
heal. The epithelium in the stomach is normally resistant to the
acid produced during a meal, but the ulcer exposes sensitive
tissues. As a result, people with stomach ulcers experience pain,
especially during a meal.
Ulcers in the small intestines (duodenal ulcer) are found where
food exits from the stomach into the small intestines. In this
case, the pain starts about 2–3 hours after a meal when the
digested food enters the duodenum. Unlike stomach and
LESSON 2.5 WORKBOOK Do bacteria cause stomach ulcers? Applying
Koch's postulates
This lesson continues to grapple with the problem of arriving at
causation from correlation by looking at another infectious agent
that presents challenges to fulfilling Koch’s postulates,
Helicobacter pylori. H. pylori is thought to cause stomach ulcers,
and its discovery revolutionized how we treat ulcers. However,
Koch’s postulates have never been fully established for this
infectious agent, begging the question — will the future reveal
another 'cause' of stomach ulcers?
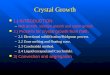
Figure 1: Peptic ulcers are found in different regions of the
gastrointestinal tract: the stomach, the duodenum, and
occasionally, the lower esophagus.
W o r k b o o k Lesson 2.5
DEFINITIONS OF TERMS
Peritonitis — inflammation of the peritoneum, the thin tissue that
lines the inner wall of the
abdomen and covers most of the abdominal organs.
For a complete list of defined terms, see the Glossary.
1. A large study of biopsy samples from patients with ulcers
conducted in the 1950s failed to observe H. pylori because
.a the scientists examined samples from healthy patients.
.b an inadequate staining technique was used leaving the bacteria
‘invisible’.
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________
duodenal ulcers, esophageal ulcers generally cause symptoms before
meals or when a person is laying down. In all cases, symptoms may
include vomiting and in extreme cases infection in the abdomen,
which results from bacteria entering the sterile areas of the body
through the ulcer. But even the less severe symptoms should be
treated because ulcers may lead to the development of cancers. Up
until 1982, genetics, stress and/or diet were thought to cause
ulcers.
A crazy idea at the time — do bacteria cause stomach ulcers?
The hypothesis that ulcers are caused by bacteria, originated first
in the 19th century. In 1875, German scientists found spiral-shaped
bacteria in the lining of the human stomach but they were unable to
culture them, and the results were eventually forgotten. A couple
of decades later, Professor W. Jaworski, who worked at a University
in Poland, investigated human stomach samples. He found bacteria
with a spiral shape and was the first to suggest a possible role of
the spiral bacteria in the pathogenesis of gastric diseases. But
his work was published in a textbook written in Polish and went
unnoticed. Later on, other studies also observed curved rods in the
stomach of many patients with peptic ulcers and stomach
cancer.
In 1954, a large study failed to observe the bacteria in 1,180
stomach biopsies. Unfortunately, this was the result of a technical
limitation: the researchers used staining technique that was
insufficient in visualizing the bacteria. A couple of decades
later, a different staining technique allowed scientists to better
visualize bacteria in samples from patients with gastric ulcers.
Later, this bacterium was named Helicobacter pylori. At the time,
conventional thinking was that no bacterium could live in the
stomach given its acidity is similar to that of a car battery. The
idea was that the strong acid destroys bacterial structures,
specifically proteins, killing the bacteria. For this reason, most
scientists and doctors were quite skeptical of the idea that the
bacteria in the samples were more than contamination from poor
technique.
Figure 2: H. pylori is a spiral shaped bacteria.
Figure 3: Microscopic images of H. pylori cells (dark brown
spirals) on biopsy samples from an ulcer patient.
W o r k b o o k Lesson 2.5
DEFINITIONS OF TERMS
Bacterial colony — a cluster of billions of bacterial cells that
originated from one single cell,
and are visible with a naked eye on the agar surface.
Endoscopy — a procedure used to examine a patient's
digestive tract. It is performed with an endoscope, a flexible tube
equipped with a camera
and light to provide pictures of the digestive tract.
For a complete list of defined terms, see the Glossary.
2. Marshall and Warren had a hard time culturing H. pylori in the
lab because
.a they did not know what was the optimal type of media to grow the
microbes.
.b they did not know for how long to incubate them.
.c there was not enough information in the literature about H.
pylori growth under lab conditions.
.d all of the above. ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________
Two of the doctors who observed bacteria in patients' samples,
Robin Warren and Barry Marshall, contended that stomach ulcers were
caused by infection with this bacterium rather than stress or spicy
food, as had been assumed before. To test whether the bacterium was
causing ulcers they sought to apply Koch's postulates.
Their first step was to look for an association between the H.
pylori and ulcers. So they carefully studied biopsy samples from
patients with ulcers, and over, and over again they could see the
bacteria present in their biopsy samples. Years later, numerous
research groups
confirmed their findings, and identified H. pylori in almost all
patients with ulcers.
Their next step was attempting to isolate the bacteria from the
patients’ samples as a pure culture. However, growing the bacteria
under normal laboratory conditions proved very challenging — they
tried numerous types of liquid medium and agar plates but nothing
grew! With some luck, they unintentionally left their plates
incubating for 5 days, instead of the usual 1–2 days, over one
Easter weekend and returned to growing bacterial colonies.
Apparently these bacteria grow slower than most, but now that they
could grow H. pylori, Warren and Marshall wanted to prove that it
could cause a disease in healthy animals. But at this step Warren
and Marshall ran into another problem, one that they could not
solve: they could not find an animal model that was colonizable by
H. pylori.
This left many scientists questioning how H. pylori might be
related to ulcers. For example, was H. pylori causing or caused by
gastric issues, or was it merely a bystander? So, to prove his
theory Dr. Marshall did something no one should ever do — he drank
a beaker of H. pylori culture. A few days later, he became ill with
nausea and vomiting, and an endoscopy, performed about ten days
later, revealed signs of irritation, and the presence of H. pylori.
But before developing ulcers, he took antibiotics to clear the
infection.
Figure 4: Barry Marshall (on the left) and Robin Warren (on the
right) while working together in Perth in the 1980s.
Figure 5: Currently, the only organism H. pylori is known to infect
are humans, which makes it hard to prove causation.
W o r k b o o k Lesson 2.5
DEFINITIONS OF TERMS
For a complete list of defined terms, see the Glossary.
3. When planning a scientific investigation, what factors play a
role in the decision?
.a time
.d all of the above ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
A few years later, the first therapy for the treatment of duodenal
ulcers was invented, and with some modifications has been used ever
since to treat ulcers. It is a cocktail of two antibiotics in
combination with a drug that inhibits acid production. This was a
major breakthrough because treating ulcers with acid lowering drugs
alone did not permanently cure the disease, but using the
antibiotics did! In 1994, the National Institutes of Health (NIH)
published an opinion stating that most recurrent duodenal and
stomach ulcers were caused by H. pylori and recommended that
antibiotics be included in the treatment regimen.
Antibiotics are not bacteria specific, so we still can't exclude
the possibility that the treatment works for reasons we are unaware
of. This means that there is still no direct proof that H. pylori
causes stomach ulcers, so ulcers join the list of diseases for
which Koch's postulates could not be fulfilled.
Marshall and Warren rewrote the textbooks with reference to what
causes gastritis and gastric ulcers. In recognition of their
discovery, they were awarded the 2005 Nobel Prize in Physiology or
Medicine.
The challenges of designing experiments to move from correlation to
causation
When conducting research, scientists or doctors make observations
that intrigue them or call what they know into question. After
looking at what others have found out about a phenomenon, they can
synthesize a hypothesis. Based on this hypothesis, experiments can
be planned and performed to test its validity. Finally, the data is
used to make conclusions, and update biological models.
There is no single correct experiment to address a question or a
hypothesis: deciding what experiment to run is very challenging,
and is based on many factors such as time, resources, importance of
prompt discovery of a treatment or a vaccine, or whether or not we
have the necessary equipment or methodology. As we will see, how
the experiments are constructed limits the scope of our
conclusions, a factor often missed by reports of scientific
findings in the news. This brings us to an important point — if we
don't know the used methodology we can't interpret results of an
experiment! This is why, it is worth spending the time needed to
understand how an experiment was done, so we can make our own
conclusions.
Figure 6: Amoxicillin is one of the antibiotics in the triple
therapy used to treat ulcers. Like most antibiotics, it inhibits
the growth of other bacterial species.
W o r k b o o k Lesson 2.5
DEFINITIONS OF TERMS
Acid reflux — mucosal damage of the esophagus caused by stomach
acid flowing into the
esophagus from the stomach.
For a complete list of defined terms, see the Glossary.
4. The following describe ulcers EXCEPT:
.a it’s a persistent wound in the epithelium of the stomach, small
intestine or the lower esophagus that does not heal
.b stomach ulcers are painful because of the strong acid secreted
into the stomach during a meal
.c duodenal ulcers are found in the large intestine below the
stomach
.d none of the above ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________
Case study: Is excessive acid production causing ulcers?
“Dr. Annis was a gastroenterologist working in a busy clinic in the
late 1960s. For the past two weeks, she had diagnosed five of her
patients with stomach ulcers. She had treated all of them within
the past few months, and they all complained of persistent acid
reflux related to excess acid production. All five patients had
previously refused to take antacids but instead were opting out for
natural remedies such as change in diet, herbal teas, etc.
As she was going through their medical records, she wondered: did
they get ulcers because of the higher than normal acid production?
She did a literature search on the topic but she could not find any
reports that supported or rejected her suspicions. She decided to
call some of her colleagues across the country, and ask them
whether they have had similar cases. All of her colleagues agreed
to review their patients’ medical records and to discuss their
findings with each other.
A few weeks later, all of the doctors reported such cases in their
practices: in total there were 44 patients who suffered with severe
acid reflux symptoms for months, used antacids only occasionally or
never, and were eventually diagnosed with stomach ulcers.
The question that Dr. Annis asked earlier, came up again: did they
get ulcers because of the excessive stomach acid production? All
the doctors agreed that they needed to investigate this because it
looked that there was correlation between long term exposure to
high acid levels and ulcers. But was there causation? Did the acid
really cause the ulcers?
Dr. Medina suggested that they went back and look through their
records for another group of patients: the ones who took antacids
regularly. Did they still get ulcers? This way, they could compare
the two groups, and try to come up with some answers. Everyone
agreed.
They all came back together a month later. This time the patients’
records were confusing. Most of the patients who were taking
antacids followed their own regimen based on their personal
preferences for dosage per day, type of antacid medication, etc.
Some even took breaks from the medication for a few days or weeks.
It was very difficult to sort through the data and come up with any
conclusion.
But the doctors did not want to give up. What they needed was a
better study. But whom would they include? Dr. Johnson proposed
that they recruit new patients with severe acid reflux who have
never gotten any treatment but do not have ulcers yet, and start
all of them on consistent regimen with the same antacid. He also
suggested that since there are other factors suspected to cause
ulcers, such as stress, diet and weight, they should recruit people
who have similar stress levels, diet, and weight range. Once
W o r k b o o k Lesson 2.5
DEFINITIONS OF TERMS
Control group — during an experiment, the subjects in a control
group are treated
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________
they started treatment, they should do follow-ups every few months
with endoscopies, to look directly at the stomach lining, and
measure the number of stomach ulcers, if any. If most people did
not develop ulcers or develop very few, then the excessive stomach
acid production will be proven as the cause for ulcers.
However, Dr. Lu interjected that if they treated all patients with
antacids, they would not be able to prove that the antacid made the
difference because there could always be other factors. But if they
prescribed medication to some people and not others, then they
could draw better conclusions on the effect of antacids. She agreed
with the plan Dr. Johnson proposed for selecting the patients, but
she proposed changes in the experimental design. She suggested that
the patients be randomly split into two groups: one experimental,
which would get the antacid, and one control group, which would get
sugar pills instead. The sugar pills would have no effect on acid
neutralization. This way, if the experimental group developed less
ulcers than the control group, the doctors would be more confident
drawing the conclusion that excess stomach acid is a contributing
factor in stomach ulcers. By giving the control group sugar pills,
instead of nothing, they would not have to tell the patients in
which group they were placed, eliminating any possible
psychological factors. Then every few months, they would perform
endoscopies on the patients from both groups and measure the number
of ulcers per patient.
The rest of the doctors agreed with the proposed plan.
Dr. Annis reminded everyone that the outcome they hoped for, that
people in the experimental group would have less ulcers if any
compared to the people in the control group, was not the only
possible one. In fact, there were three other possible outcomes.
What do you think they might be?”
What people are you going to include in the study? There is no
perfect group of people when it comes to studies. Do you select a
wide age range? Do you include only people that have the condition?
Do you include only people of one gender, age, and race? How many
people do you include? Do you need to exclude people with other
factors or diseases that might bias your results? Each of these
choices has pros and cons — a narrow selection of people helps to
control for unforeseen factors which may have an effect, while a
wide selection might be better when you want to know if your
findings are relevant to everyone.
Figure 7: Stomach endoscopy revealing typical stomach lining.
W o r k b o o k Lesson 2.5
DEFINITIONS OF TERMS
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________ ______________________________
______________________________
How are you going to measure changes in the ulcers? It is critical
that you 'look' for the ulcers, or any measure of disease, in a way
that gives the most detail possible. Do you measure the number of
ulcers by asking patients to report symptoms? Do you look at the
stomach with an endoscope? Do you count the number of ulcers or the
size? Each of these choices has pros and cons. For example, the
less invasive a measurement is, the easier it will be for the
patients, but it may not be accurate enough. Or, what if antacid
treatment effectively gets rid of symptoms but does not promote
healing of the ulcer?
How will the people be grouped and treated? This is not a
straightforward decision and just like choosing participants there
is no perfect way to group them. Do you assign groups to balance as
many factors as you can (age, race, gender, height, weight, etc.),
or do you assign the groups randomly? What if you miss a factor
that matters? What if the randomly assigned groups are not evenly
split? Each of these choices has pros and cons — controlling
grouping can help when you know a lot about other contributing
factors, while a wide selection might be better when the other
factors are less well-known.
What will be your ‘control group’? To prove causation most
experiments need a control because there is no way to know what a
normal or untreated group should be unless you measure it. At its
heart, this is the key ingredient for distinguishing causation from
correlation — you need to be able to compare the results of an
untreated (control) group with a group that is treated in order to
conclude whether a treatment works or not. So, what will be the
difference between your treatment (experimental) and your control
group? Do you give the same drug to both groups but in different
doses? Do you administer the treatment only once or over a period
of time? Do you give the control group a placebo, like a sugar pill
which will have no effect on the condition, so the control group
thinks they are getting the treatment as well? Again, each of these
choices has pros and cons, and the decision will be based on the
current circumstances. For example, most often scientists or
doctors prefer to give only placebo or no treatment at all to a
control group. This will allow for a relative straightforward
interpretation of the results. However, if the disease you want to
treat is highly lethal or debilitating, withholding treatment from
the control group may be considered unethical. In such a case,
giving different low doses of a drug to the control group may be a
better option.
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
___________________________________________________________________________________________
W o r k b o o k Lesson 2.5
TERM DEFINITION
Acid reflux Mucosal damage of the esophagus caused by stomach acid
flowing into the esophagus from the stomach.
Bacterial colony A cluster of billions of bacterial cells that
originated from one single cell, and are visible with a naked eye
on the agar surface.
Control group During an experiment, the subjects in a control group
are treated identically to the experimental group with the
exception of the tested factor, e.g., a drug, a procedure or
another factor.
Duodenum The first section of the small intestine located below the
stomach.
Endoscopy A procedure used to examine a patient's digestive tract.
It is performed with an endoscope, a flexible tube equipped with a
camera and light to provide pictures of the digestive tract.
Esophagus The tube that connects the mouth with the stomach.
Hypothesis A testable explanation of a phenomenon.
Peritonitis Inflammation of the peritoneum, the thin tissue that
lines the inner wall of the abdomen and covers most of the
abdominal organs.
Placebo Medically ineffective treatment such as a sugar pill.