Embed Size (px)
Citation preview

Journal o f the Autonomic Nervous Symtem, 2 (1980) 205--222 © Elsevier/North-Holland Biomedical Press
Research Papers
205
IDIOPATHIC ORTHOSTATIC HYPOTENSION: CIRCULATING NORADRENALINE AND ULTRASTRUCTURE OF SAPtlENOUS VEIN
RICHARD L. KLEIN, JACK McC. BAGGETT, ASA THURESON-KLEIN and HERBERT G. LANGFORD
Department o f Pharmacology and Toxicolojy and Department o f Medicine, University o f Missiuippi Medical Center, 2500 North State Street, Jackson, ~rM. 39216 (U.S.A.)
(Received September 7th, 1979) (Accepted May ] 7th, 1980)
Keywords: idiopathic orthostatic hypotension -- human saphenous vein -- innervation -- ultrastructure
ABSTRACT
The present study indicates that patients who can be clinically classified as idiopathic orthostatic hypotensives of the peripheral type are heterogenems. There ~s the typical hypoadrenergic type characterized by low levels of cir- culatin~ noradrenaline, much reduced or absent noradrenaline stores, and correspondingly little or no noradrenergic innervation in the saphenous vein, a major capacit~Lce vessel, as confirmed by ultrastructural examination. In one patient of this type, an abnormally high occurrence of mast cells in the blood vessel wall was noted. There also exists a category of individuals of the hyperadrenergic type, analogous to certain diabetics with noradrenergic abnormalities. These patients also are characterized by low levels of circulat- ing noradrenalin,:, but noradrenaline stores are high; an exaggerated release of nemotransmitto~" or.curs in response to stimuli; the saphenous vein with noradrenergic innervation remains ultzastructurally normal; however, the effector cell responses are greatly b'lunted. In one patient of this type, the smooth muscle cells of the saphenous vein contained excessively high glyco- gen deposits. Further, it should be anticipated that a variety of intermediate types can be found as exemplified by one patient with variable, low to nor- real levels of circulating noradrenaline, a sluggish response to release neuro- transmitter upon postural challenge, and considerable innervation of saphenous vein but with the majority of axons and terminals undere~oing active degeneration.

206
INTRODUCTION
Orlhostatic hypotension occurs when the autoregulation of blood pressure is impaired in respon~ t o changes in postm'e. This condition may be secon- dary to a variety of diseases or drug treatments which affect the peripheral and/or central nervo.us system or cause volume depletion, but it may also be due to a primary disease [27]. A specific syndlome with a triad of charac- teristic symptoms including orthostatic hypotension, impotence and loss of sweating was first described as a clinical entity by Bradbury and Eggleston in 1925 [ 5]. Since then this syndrome has usually been called idiopathic ortho- static hypotension (IOH), because of the uncertainty regarding its anatomical and functional etiology.
The autonomic insufficiency associated with IOH can be present without prominent manifestations of central neurological deficits [15,22], and this may be associated with a marked depletion of noradrenaline in the sym- pathetic nerves of blood vessels [8,10,17]. In others there are characteristic .~ymmetrical lesions in specific areas of the central nervous system as origi- nally described by Shy a~ld Drager [24], who also suggested that the ortho- static hypotension was part of a multisystem or progressive disease. Based on circulating noradrenaline levels, a recent study [32] reports that the neuro- logical defect in IOH can be divided into two distinct clinical types. One is represented by individuals with documented central nervous system defects who are unable to activate their peripheral sympathetic nervous system. This is the Shy--Drager or central type which is reported to be characterized by' normal levels of circulating noradrenaline while the patient is recumbent. The second type includes individuals without demonstrable defects in the central nervous system but with autonomic nervou:~ system deficiencies. This is the peripheral type which according to the authors can be characterized by low levels of plasma noradrenaline while the patient is recumbent. Patients of both central and peripheral types fail to increase their circulating nor- adrenaline levels in response to postural challenge. Both types also have low levels of circulating dopamine ,5-hydroxylase acti¢ity; this enzyme converts dopamine to noradrenaline and must be released by exocytosis along with the neurotransmitter upon stimulation of sympathetic nerves.
Basic defects associated with t~le altered noradrenergic function in the peripheral type of IOH appear to include abnormalities in metabolism, storage and release of noradrenaline [10]. Presumably, presynaptic receptor feedback mechanisms or postsynaptic receptor and smooth muscle respon- siveness could also be involved, but there is no documentation for these in patients with IOH. Further, it is reasow.,t'4e that ultrastructural manifesta- tions could accompany abnormalities in peripheral sympathetic nervous sys- tem function either- at the pre- or postsynaptic level. Light microscopic histo- chemical studies have s~.own that iOH patients often have diminished cate- cb.olamine-specific fluorescence in their sympathetic vasomotor n~rves [ 17 ].
The present study was undertaken to demonstrate ultrastructurM abnor- malities, should they o~cur, in the noradrenergic varicosities or in other con-

207
stituent~ of blood vessel walls. The saphenous vein was chosen ~m a perti- nent example of a capacitance vessel expected to be affected in IOH. This information could help to explain some of the heterogeneity in physiological and pharmacological responses commonly experienced in patients with IO~1.
METHODS
Subjects Six consenting patients previously diagnosed as having IOH were admitted
to the Clinical Research Center to be further evaluated on the bases of clinical symptoms, ultrastructural features of saphenous vein biopsies; and therapeutic response. None of the patients s~owed any evidence of dis. orders known to be associated with secondary or thostatic hypote~.sion at the time of adraission. Criteria for the diagnosis of IOH of the peripheral type were: (1) t~e absence of neurological deficits in the central nervous system such as tremor, extrapyramidal rigidity and akinesia as confirmed by neuro- logical consultation; (2) a history of precipitous falls in blood pressure of ~40 mm Hg upon standing, with narrowing of pulse pressure and leading to dizziness or syncope, which markedly affected the patients' life style and work; and (3) these were accompanied by various combinations of abnor- malities in the baroreceptor reflex; a pulse rate which decreased, did not change or increased inadequately; impotence; sweating; anhydrosis; and sphincter difficulties. Three of the six patients were chosen for more detailed comparison based on specific a_~omalies found in their blood vessel walls and a particular combination of blood pressure, pulse rate and eatecholamine response to postural challenge and/or pharmacological treatment. A brief case summary of each is given below. The remaining 3 patients more or less fit into one of these categories based on the data obtained. Pieces of saphenous veins from patients undergoing surgery for various reasons (traffic accident injury, tumor removal or coronary bypass) were used as controls.
Patient EG, UMC No. 030116. This patient was a 78-year-old wEite female. She was followed for 20 years at the University Hospital. When she was originally seen at the age of 58, she complained of chronic diarrhea of 12 years' duration and recurrent episodes of weakness and syncope on stand- ing. Blood pressure was 80/60 supine, falling to 60/30 sitting, and was essen- tially unobtainable standing. There was no cardio-acceleration. She was treated with a variety of therapies over the years. The only ~herapy tha t was effective was fludrocortisone. She was usually maintained on 0.1--0.3 mg daily dose of this drug with mociest improvement in her symptoms. There was no evidence of motor or sensory disease.
Patient CH, UMC No. 400350. This was a 63-year-old white female initi- ally admitted to the University Hospital in 1977. Past history was un- remarkable. For 3--4 years she had marked dizziness on standing. Except for recurrent urinary tract infections, she was otherwise asymptomatic. Typical blood pressures were in the range of 90/60 supine with a pulse rate of 66 ~upine. Blood pressure was frequently unobtainable after 5 min standing,

208
~md there was no cardio.acceler~fion. Crea.~inine and glucose were within normal limits. Plasma renin activity was 0.(32 ng/ml/h supine and 0.04 ng/ ml/h after 5 rain standing. After 2 h sitting it was 0.07 ng/ml/h. She was studied b'y Ibrahim's protocol aria the results suggested a problem with efferent sympathetic fibers. There was no evidence oi" motor ~r sensory disease.
Patient ~W, UMC No. 403608. This patient was a 50-year-old white male who complained of recutr,~qt black-out spells. These episodes occurred within 30 sec of standing. They were a~vc,.'~_~.ed_ w,.'~_h ~erked impairment of consciousness, though not actual unconsciousne~. The severity of his symp- toms fluctuated. At times he was completely asymptomatic; at times he was inc-~paci~at,~d by orthostasis. His symptoms became severe about 20 years before. Eighteen years previously he was seen at the Jackson V.A. Hospital. His sitting blood pressure was 120/80 which fell to 83/75 afte:: a few minutes standing. Marked cardio-acceh:ration was noted, although the exact figures were not recorded. An adenocarcinoma of his lung had been removed 10 years previously. Another was removed 4 years previously. He had not been treated with immunosuppressi~e drugs for several ygars. During the last year symptom:; of dizziness had been quite distressing and because of ~;hese he was admiLted to the V.A. Hospital and then transferred to the University Hospital. On admission he was continuing his medication of 0.3 mg 9-a-flu- drocortisone acetate daffy and supplemental salt. Blood pressure was 140/80 supine with a pulse rate of 88. On standing blood pressure was 116/85 with a pulse rate of 130.
Protocol The blood pressures (3 measurements), pulse rates (3 measurements) and
venous blood sarnplez were taken for 3 days before each trial with a ph~.rma- cological agent under the following conditions: (1) after 1 h at rest in the supine position; (~) 5 min following postural challenge from supine to a 45 ° tilt [29] or standing [9], if possible, (data are all for 45* tilt); and (3) after sitting for 1 or 2 h following the postural challenge. In all cas~,s ~he blood samples were drawn into heparinized tubes using indwelling needles. The blood samples were immediately chilled on ice and transported to the labora- tory. After centrifugatiorL to remove red blood cells, the plasraa 'volume was measured, any bound caLecholamine released and the protein precipitated with 0.1 N perchloric acid followed by centrifugation. The resulting cate- cholamine-containing supernatant was stored at --85°C until purified and concentrated for analysis.
Noradrenaline extracts were purified and concentrated over activated alumina (Brockman activity I, neutral). Convenient sample volum,:s of the eluate were analyzed for noradrenaline by radioenzymatic methods [ 13,30]. Partially purified bovine phenylethavolamine.N-methyltran~ferase [.3,6] was used with [3H]S.adenosylmethionine as methyl" donor to produce tritiated adrenaline which was differentially extracted and counted by t3-scintillation. Internal standards of known amour~ts of noradrenaline were used to correct

209
for recovery and endogenous inhibitors. Standard curves were mn with each series of unknown samples, which were analyzed in duplica~ and repeated at least one time.
Pharmacological agents A number of potentially beneficial drugs acting by relatively specific
mechanisms can be considered in treating patients with symptoms of IOH. In the present study, certain agents were selected because they were known to exert some of their actions via the autonomic nervous system. Ephedrine, 25 mg i.v., was used for its indirect neurotransmitter releasing effect to test for noredrenergic vesicle stores of noradrenaline; it also has dLt'ect effects, especially on cardiac receptors [4,11]. Indomethacin, 25 mg p.o. 4 times daffy, was given as an inhibitor of prostaglandin synthesis [!6] mainly to block the inhibitory feedback action of prostaglandin-E presynapticaffy [12]. Cimetidine, 300 mg p.o. 4 times daffy, was chosen as a blocking agent of the type-2~ H2, histamine receptors, which can also have an inhibitory pre- synaptic function on sympathetic nerves [19].
Electron microscopy The electron microscopist (A.T-K) had no knowledge of the various
clinical signs observed in the patients other than they suffered from ortho- static hypotension at the time of the biopsy. Vena saphena magna has a par- ticularly rich innervation [1], is a pertinent capacitance vessel, and w.qs selected as an appropriate vessel to examine because it was accessible for biopsy with minimal trauma to the patient. Small portions were obtained from the ankles about one inch above the medial malleolus of the tibia after lidocaine hydrochloride (Xylocaine) had been applied as a local anesthetic. The excised tissue was rinsed free of blood, divided into small blocks and fixed by several methods for comparative purposes. These" included prefixa- tion in highly purified 2,5% glutaraldehyde in a 0.2 M potassium phosphate or cacodylate buffer or in Tyzode's solution followed by postfixation in 2% osmium tetroxide :~n the same buffer. Potassium permanganate 1.3% in the same buffer was ah o used. Some samples from each fixation were stained en bloc in aqueous 2% uranylacetate before dehydration and embedding. The segment of vein removed from one patient w~Ls sufficiently lorg to allow a portion to be incubated for 20 min at 30°C in 95% 02/5% C02 saturated Tyrode's solution containing 260 nmol/ml noradrenaline.
RESULTS
Saphenoz; Jein ultra,ctructure: general observations
Saphenous vein biopsies from ccntrol patients had many norraal-appearing nerve axons and termin,-ls in the tunica media and adventitia in every tissue block sectioned, even though the innervat:'on appeared to be considerably less extensive than that previously observed in studies of human omental

210
• 2
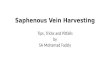
Fig. 1. Electron micrographs are from the saphenous vein biopsy of IOH pa~,ient CH. a: axons are partially ensheathed by Schwann cells located in the tunica advei~titia. Small vesicles (sv) with various electron densities often occar in clusters and are typical after

211
vein [28]. The vein biopsies from two of the IOH patients had relatively normal-appearing nerves and terminals {e.g. Fig. la, b). Three of the six patients with IOH showed nearly complete lack of nerve fibers (e.g. Fig. 2h) and one patient showed severe degeneration of most axons and terminals {e.g. Fig. 2d, e).
The typical hypoadrenergic type Based on the available data, three of the six patients were judged to be of
this type, which is exemplified by patient EG who was a 7S-year-old female with a 20-year history of IOH.
More than 50 grids covered with sections from different levels of i 0 tissue blocks were examined from her saphenous vein biopsy. No axons or termi- nals could be detected in the tunica media and only a few were present in the adventitia (Fig. 2b). These were difficult to identify with cel~ainty as being noradrenergic due to the sparsity of vesicles. In contrast to, the very few nerve fibers encountered, there occurred numerous mast celis along the adventitial-medial border (Fig. 2a--c). The high number of mast cells was unique in this patient compared to both controls and other IOH patients. Mast cells were easily identified by their oval shape, finger-like projections and many very large dense granules (Fig. 2a). Typical for human mast cells, there were scrolls [2,14] in some granules, while others appeared degranu- lated (Fig. 2c). In two instances, presumptive mast cells resembled the so-called fibroblastic type [ 14], which were much longer than the others and had irregular, thick projections. One such cell was located close to a bundle of axons ensheathed by a Schwann cell (F~g. 2b).
The resting level of plasma noradrenaline was very low in patient EG com- pared to normal controls in her age group [ 18,20,23,30], and this level did not change or fell slightly upon postur~l challenge (Fig. 3a). The sitting posi- tion could no*~ be maintained in order to obtain a subsequent blood sample after one hour. Upon postural challenge by 45 ° tilt, decreases in both mean blood pressure and pulse rate, a vasovagal response, were typical for this patient (Fig. 3b).
The ephedrine test for endogenous noradrenaline stores was negative in patient EG as evidenced by a very small increase in circulating noradrenaline
potassium permanganate fixation. Large vesic'es (iv) with less dense contents ,'ire al.~o preseat, b: a terminal portion o! an axon is shown adjacent to a smooth muscle cell (sin). Large vesicles (Iv) are filled with an electron dense matrix material but small vesicles (sv) contain very little dense matrix. An abundance of mitochondria (m) occurs. Glycogen has been extracted from this smooth muscle cell durir, g block-staining in uranylacetate. Preparation was fixed with glutaraldehyde followed by osmiura tetroxide, c: a portion of a mast cell contains large granules (g) with irregular shapes, d: glycogen (gly) occurs as beta particles and forms an abnormally large deposit in this smooth muscle cell. th.epara- tion was fixed with glutaraldehyde followed by osmium tetroxide without block-staining
m uranylacetate.

to
to

2]3
0 5
ncj N A / m l plasma
o
-"~o '1~" $o ,l_~,,,'Jr~s
Supine t i l t / SJthnq -'stand
I00 o ~ . meon BP, rnrnHcJ o - - - o pulse rote/rain
8O
40
1 b
2o_ ¢o" Ig do ~l M/NOTES
Supne t ~ o n d S~thn9
Fig. 3. Patient EG, data ± S.E.I~. a: baseline plasma noradrenaline (NA) level at rest immediately prior to 45 ° tilt and 5 rain after postural challenoe. The 60 rain sitt.ng sample was not available, h: mean blood pressure (BP) and pulse rate corresponding to times in (a).
at rest (Fig. 4a). Postural challenge did not increase plasma noradrenaline after ephedrine. Mean blood pressure and pulse rate were increased 5 rain after ephedrine was administered, pl'obably as the result of direct cardiac stimulation (Fig. 4b). Mear~ blood pressure which had become relatively low after 1 h at rest did not decrease further upon 45 ° tilt, but pulse rate dropped, typical of the vasovagal response.
Treatment with indomethacin (data not shown) had no effect on plasma noradrenaline before or after postural challenge, and there was a marked fall in mean blood pressure from 75 to 50 mm Hg while pulse ra~ increased only slightly upon 45 ° tilt.
Treatment with cimetidine was t eed with the intention of blocking any presynapUc H2-receptor feedback inhibition of neurotransmitter release. It
Fig. 2. Electron micrograph~ are from the saphenous vein biop.~ies of patier~t EG (a--c) and patien~ CW (d, e). a: a typical mast cell in the tunica adventitia has many finger-like projections and contains numerous large dense granules, b: a portion is shown of one of the few axon bundles encolmtered in this patient. Most axons (A) have little organelle content but occasionally a few vesicles are found. The axon bundle is located close to a mast cell containing dense gt'anu|es (g) . c: a portion of a mast cell is shown ;lnd some of the granules (g) are filled with scrolls which is typical for human mast cells. Several granules appear depleted of contents, d: a few, relatively normal appearinfi axons (A) are present among several abnorn al axons. Large accumulations of der, se amorphous material are typical in axons and Sc~wann cells of unmyelinated nerve fibers in this patient. Preparation was fix,,d with glutaraldehyde followed by osmium tetroxide ar, d block- stained with uranylacelate, e: portions of axons are from a specimen which was incubated with exogenous noradrenaline. Both the large vesicles (Iv) and small vesicles (sv) are intensely electron opaque. The axons are relatively close to smooth muscle cells (sin) in the tunica media. Preparation was fixed with potassium permanganate.

21~
ng NA/ml plosmo
I"
,' %
J & DRUG c] I I
- ' 5 6 0
Supine ~ t o n d Sitting
INr 6O ~
40 - ~ = meon BP, mmHg o---o pulse rote/mln
& DRUG b
- 6 0 INUT
Supine t~ fon d Sl~ting
Fig. 4. Patient EG, data ± S.E.M. a: baseline plasma noradrenaline (NA) level at rest, 5 rain after ephedrine i.v., 60 m m later at rest just prior to 45 ° tilt and 5 rain after postural challenge. The 60 min sitting sample was not available, b: mean blood pressure (BP) and pulse rate corresponding to t imes in (a).
h ~ been demons~zated in dog saphenous vein that such receptors may r e ~ a ~ ~ansmitter release [ 19]. Thus, it was of interest fo find out if mast ceUs were typically present in the human saphenous vein as a potential source of histgxnine. The drug was administered for acute effects as well as over a 15-day-period with and without salt-loading. There were no effects on the plasma noradrenaline. The resting mean blood pressure increased when c~metidine was combined with salt-loading but a vasova~al effect still resulted upon postural challenge. An excessive elevation in resting mean blood pressure to 140--160180--90 mm Hg developed and was accom- panied by dizziness and headache. A two-week course of salt-loading and cimetidine at a reduced dosage of 30() mg twice daily was also unsuccessful Note that although this patient had abnormally numerous mast cells in the blood vessel walls, she also had few noradrenergic terminals on which to determine the possible effects of feedback inhibition.
The hyperadre~ergic type Based on the available data, 2 of the 6 patients were judged to be of thi~
type as exemplified by patient CH, a 63-year-old female with a five-year histoIT of IOH.
Ele-~en blocks of embedded saphenous ~'ein biopsy were sectioned at dif- ;~erent leve!s. Several noradrenergic nerve terminals were observed in 4 blocks, occasional terminals in 5 blocks and none in the remaining 2 blocks. ~,ll terminals appeared entirely normal and contained both small and large dense~ored vesicles which were evident with all fixa~iul~ methods tested. After potassium permanganate fixation, postulated to give a specific electron ,dense reactior, produc* in noradrenaline-cGntaining structures, many small vesicles of various electron densities could be observed together with larger vesicles of lower electron density (Fig. la). A few of the terminals contained

2 1 5
an abundance of mitochondria (Fig. Ib), but their vesk'le populations did not differ from terminals with few mitochondria. Occasionally the nerve terminals were located at a relatively short distance from adjacent smooth muscle ce~s (Fig. lb~, which would facilitate the interaction of released transmitter with effector cell receptors on the smooth muscle. A few myelinated axons were detected, but these were only i~resent in the tunica adventitia. This patient had a few mast cells in the tunica adventitia (Fig. lc) and these contained large dense granules which were often irregular in out- line. Most granules had a homogeneous smooth matrix, but typical mem- branous scrolls were present in some. There were no significant morphologi- cal differences in the structure of the mast cells and nerve t~rminals in this patient when compared to the control veins. However, in contrast to all of the other IOH and control patients, this patient's smooth muscle cells con- rained abnormrJly large accumulations of glycogen (Fig. ld) in all tissue blocks that had not been stained en bloc with uranylacetate, treatment with which extracts glycogen. Other IOH patients and controls had very little or only moderate amounts of glycogen in their smooth muscle cells.
Patient CH, like patient EG, also had a relatively low level of plasma nor- adrenaline ~-ompared to no,~-m~ individuals in her age group (Fig. 5a) and noradrenaline was barely detecta.ble in some samples. Following postural challenge, an exaggerated hyperadrenergic response occurred with a 10-fold increase in noradrenaline to 1.84 ng/ml plasma, which is much above the normal range. This returned towm'd the resting level after 1 h in the sitting position. At the same time both mean blood pressure and pulse rate fell, a vasovagM response, and these returned toward normal after 1 h sitting (Fig. 5b).
In pat ient CH the ephedrine test caused the low resting level of plasma noradrenaline to double to 0.29 ng/ml in 5 rain (Fig. 6a), After 1 h at rest, the value was dramatically increased to 4 times this, which is above the nor-
20
IO
0
no NA/ml plasma
I a
~1 ~jNUrES Supine ti~stond Sitting
I00
80
60
I
40 . ~ * mean BP, mmHg o---o pulse r0te/mln
b
2 O _ 6 o - ,LM'NUT~S
Supine t~.-/stan ~ Sithng
Fig. 5. Patient CH, data + S.E.M. a: b.~seh.le plasma noradrenaline (NA) level at rts: immediately prior to 45 ° tilt ~nd 5 rain after pastural challenge and after 60 rain sitting. b: mean blood pressure (BP) ax.d ~ulse rate corresponding to times in (a).

216
20
I0
0
ng NA/ml plosmo
~DRUG l
. / • (1 e
Supme tJ~stond Sitting
I00
so i 2
6(::
4C ~ " ~ " mean 9P, mmHg I. o---o pu~e rote/rnin I * oeuo
Supine ~ o n d Sitting
Fig. 6. Patient CH, data _- S.E.M. a: baseline plasma noradrenaline (NA) level a t rest, 5 min af ter ephedrine i.v., 60 rain later at rest just prior to 45 ° tilt and 5 rain af ter postural challenge. The 60 min sitt ing sample was not available, b: mean b lood pressure (BP) and tmlse rate corresponding to t imes in (a).
real rang~, ;~nd it nearly doubled again u p o n postural challenge. Thus, the presence of co,siderable noradrenaline stores was demonstrable in this patient in contrast to patient EG. Both mean blood pressure and pulse rate increased during the first 5 min after ephedrine (Fig. 6b), probably as a result of direct myocardial stimulation, and both returned close to the resting level after an hour at rest. Postural challenge still resulted in a drop in mean blood pressure but pulse rate was little changed. This pat ient was unable to maintain a sitting position, therefore, no sample was available after 60 rain.
30
2.0
I0
no NA/ml Plosmo
/
- 60 _ inure
iOOr
..° .... K ,
60 t1- o-" """" •
/
40 [ . ~ e Meon 8P, mmHg O----O Pulse Rail, I)14ts/r:lm
b 20 ' ' - ' - - ~
-60 _ 15minu,e 60
supine- ,,I/t/ston d sitting supine - ,il~tond sitting
F~K. 7. Patient CH, data ± S.E.M. a: ph~sma noradrenaline (NA) levels after 24 h treat- ment with indomethacin at rest, 5 min af ter 45 ° tilt and af ter 60 rain sitting, b: mear blood pressure (BP) and pulse, rate corresponding to t imes in (a).

217
Patient CH subsequently was treated with indomethaein with the inten- tion of preventing the normal prostaglandin feedback inhibition of neuro- txarmn;itter release. After 24 h of treatment, a positive response was ob- served. The resting level of plasma noradrenaline had increased to the high normal range (Fig. 7a) and this was more than doubled 5 ~ i n after postural challenge by 45 ° tilt. The noradrenaline continued to rise to very high levels after an hour in the sitting position. Concomitantly, the resting mean blood pressure of 90 mm Hg was maintained upon postural challenge but decreased considerably within an hour in the sitting position (Fig. 7b). Pulse rate also slightly increased upon postural challenge and continued to elevate as blood pressure dropped after an hour in the sitting position.
An intermediate type Patient CW was a 50-year-old male with a 32-year history of intermit tent
[OH. Exam~a t ion of numerous grids filled with sections from 12 blocks of embedded saphenous vein biopsy revealed abnormalities not encountered in any of the other IOH patients. Many axons, both unmyelinated and myeli- nated, and terminals were present in the adventitia and media. Some un- myelinated axons and terminals appeared to be structurally normal even though their vesicle content was reduced. However, the majority of un- myelinated axons contained amorphous electron dense material (Fig. 2d). Many terminals among the smooth muscle cell:~ in the media were almost completely filled with large dense bodies of similar electron density regard- less of the type of fixation used. In fact, their appearance resembled that after chemical sympathectomy with 6-hydroxydopamine. Similar pathology was not evident in the myel, inated axons, however, myelin lamellae were frequently separated into two layers.
A portion of the saphenous vein incubated in the presence of exogenous
• ng NA/ml plasma
I0 / [
/ Q
O. o 6 0 , 2 0 MINUTES
Supine til~stand S=thng
I00
80
60
40
20
a ~.,
"'IS
* ~ = me(m BP, n'.nHg o---o pulse rote/rain
b
j . | /dINUTE$ Supine t~stand Sitting
Fig. 8. Patient CW, data + S.E.M. a: baseline plasma noradrenaline (NA) level at rest immediately prior to 45 ° tilt, 5 min after postural challenge and after 120 min sitting, b: mean blood pressure (BP) and pulse rate corresponding to times in (a).

218
1.0
ng NA/ml plasma
&ORUG a
0"6C) I' " " " 5 60 120 MINUTES
- . , ]m
Supine - fstatiltj nd Sitting
8 0 .
60
40 o ~ o mean 8P, mmHg o- --o pulse rate/rain
40RUO b I~ "°°'= 20-60 60 120
- MINUTES. Supine ti~stand Sitting
Fig. 9. Patient CW, data ± S.E.M. a: baseline plasma noradrenal ine (NA) level at rest, 60 rain af ter ephedrine at rest just pr ior to 45 ° tilt, 5 min af ter postural challenge and af ter 60 rain sitting. Ephedrine was administered s.c. inadvertent ly , therefore no 5 min sample was taken at rest. :): mean blood pressure (BP) and pulse rate corresponding to t imes in (a).
noradrenaline (see Me~ods) had small and large dense-cored vesicles with intensely electron dense matrices in the few normal appearing axons (Fig. 2e), but still only a few ~ esicles were present.
The resting level of pEsma noradrenaline in patient CW was low to average, depending on the time of testing, compared to r~ormals in his age group (Figs. 8, 9). The response to postuml challenge w;ts not normal and some- what L-',t~rmediate between the examples of hypoadrenergic and hyper- a(renergic types given above. Thus, plasma noradrenaline did not increase in,mediately after postural challenge by 45 ° tilt, but rose during the next 2 h in th~ sitting position (Fig. 8a). Although this patient had an extended history of precipitous falls in blood presmtre on an i~termediate bvsis and a typical fall in blood pressure and incre&~e in pulse rate was noted immedi. ately prior at the V.A. Hospital and upon admission to the Clinical Research Center for this study, he demonstrated a relatively nomml response to main- tain mean blood pressure and to increase pulse rate (Fig. 8b) at the time of sampling for noradrenaline levels.
When the ephedrine test for noradrenaline stores wa~ p~rformed, the i-ti- tia]ly Io w resting level of noradrenaline was increased about 3-fold within 1 h (Fig. 9;i), confirming the presence of considerable noradrenaline stores. Because ephedrine was inadvertently administered subcut~meously, which was unlmown until after the analysis samples were received, no responses wef.e avdlable at 5 min. Upon 45 ° tilt, plasma noradrenaline fell and eventu- ally returned to the relatively low initial value after 2 h in the sitting posi- tion. Again at the time of testing, mean blood pressure and pulse rate respons:s contitm~ to be relatively normal during postural challenge and thereafter (Fig. 9b).

219
DISCUSSION
The morphological, biochemical and physiological findings indicate that patients who can be cJ/nically classified as having IOI-I of a peripheral type are heterogeneous. Of the 6 patients diagnosed with IOH from which saphenous vein biopsies were studied under the electron microscope, at least 3 general categories of abnormalities were indicated. This information helped to explain the clinical sigrls and the physiological and pharmacological responses of the patients.
The patients could not all be classified according to the recent criteria [32] by which IOH patients of the peripheral type had low levels of circulat- ing noradrenaline which did not increase upon postural challenge. In general, 3 of the 6 patients in this study appeared to fit these criteria with low levels of circulating plasma noradrenaline and a typical hypoadrenergic response to postural challenge. A marked depletion of noradrenaline stores was apparent as the result of physiological and pharmacological tests. Correspondingly, ultrastructural examination of saphenous vein biopsies from these patients revealed very few noradrenergic axons a~d terrriinals with sparse vesicles.
However, two of the 9atients in this study also had low levels of circulat- ing plasma noradrenaline but were best characterized by a hyperadrenergic response. Saphenous vein biopsies showed these patients to have relatively normal appearing noraclrenergic innervation with small and large dense- cored vesicles in the terrainals. Noradrenaline stores could be demonstrated pharmacologically and physiologically. There was an exaggerated response to release transmitter, as if attempting to compensate for a blunted or absent effector cell respon~. ~lhat is, ~-receptor stimulation of smooth muscle con- traction was ineffective. Thi:~ type of response was not reported in the recent classification of IOH patient~ based on circulating noradrenaline levels [32].
One patient appeared to be intermediate between the hypoadrenergic and hyperadrenergic types in certain respects. Theft is, circulating levels of nor- adrenaline were low to average for the age group and an abnormally slow release of neurotransmitter followed postural challenge. Although many axons and terminals were found h~ the saphenous vein biopsy, a large major- ity of these were filled with de~se amorphous material as if undergoing degeneration. An intermediate type was also not described in the recent study on noradrenaline lew.~ls [32].
In some respects, the findings in the present study of IOH can be clearly analogized to recent data [7] reporting on 26% of diabetic patients with adrenergic nervous system abnormalities. Among these were the typical hypoadrenergic group, but in addition the newly recognized clinical syn- drome of hyperadrenergic postural hypotension with apparent vascular resistance to noradrenaline was reported. In fact, nearly any combination of circulating noradrenaline and physiological responses of blood pressure and pulse rate could be found.
In the present study, indomethacitl was tried in patient CH who was of the hyperadrenergic--vasovagal type with an apparent blunted receptor cell

220
response. This inhibitor of prostaglandin synthesis has been used to treat patients with IOH of ~ e central neurogenic type (Shy--Drager), based on the belief that an endogenous vasodilating prostaglandin was inhibited [16]. However, another effect of pro~taglandin-E (to cause vasodilatation) involves the feedback inhibition of noradrenaline release from sympathetic nerve terminals [12]. It has" been demonstrated that prostaglandin-E effectively inhibits transmitter release from vasoconstrictor nec~es in humans [26]. This feedback inhibition is reversed when drugs like indomethacin are admin- istered. In accordance with this possibility, patient "CH responded to indo- methacin treatment by a significant increase in the resting level of plasma noradrenaline and in response to postural challenge, and a transient correc- tion of the orthostatic hypo~nsion.
In considering the possible intermediate type of IOH exemplified by patient CW, it should be recalled that he had undergone surgery for car- cinoma of the lung on two prior occasions, 10 and 4 years previously, but had not been treated with immunosuppressiv,~ drugs in the last few years. This patient's orthostasis had been treated for 20 yeats and, therefore, was presumed to be unrelated to his more recent carcinomas. However, there have been reports of severe orthostatic hypotension in patients with bronchogenic carcinoma; in one case the orthostasis was believed to be asso- ciated with the malignancy [25], but in the two others there appeared to be no relationship [4,9].
From the results of the present study, it is evident that in certain patients with IOH of the peripheral type an ultrastructural investigation of blood vessel innervation can be helpful in explaining the variations in respc.nse to physiological and ph~.w, acological tests. This knowledge may be be~eficial when ind ivi,~lual regimens of therapy are designed. It is suggested tha~ IOH, like diabetes with noradrenergic abnormalities, includes a category of individuals who are hyperadrenergic in that they secrete exaggerated amounts of neurotransmitter in ~sponse to stimulus, but have a blunted effector cell response. Further, intermediate types and responses should also be anticipated.
ACKNOWLEDGEMENTS
This research was supported in part by Research (}rant GM15490, Train- ing Grant GM00359, CRC Grant RR-00626 from the NIH, the American Heart Association - Mississippi Affiliate, and NSF Grant BNS-20220. J. McC. B. i,,;a postdoctoral fellow, American Heart Association - Mississippi Affiliate.
REFERENCES
1 Abraham, A., Microscopic Innervation of the Heart and Blood Vessels in Vertebrates including Man, Pergamon Press, Oxford, 1969.
2 Asboe-Hansen, G., The mast cell in health and disease, Aeta Dermatovener, Suppl., 73 (1973) 139--148.

221
3 Axelrod, J., Purification and properties of phenylethanolamine-N-methyl transferase, J. Biol. Chem., 237 (1962) 1657--I660.
4 Bannister, R., Ardill, L. and Fentem, P., An assessment of various methods of treat ment of idiopathic orthostatic hypotension, Quart. J. Med. New Series, XXXVIII, 152 (1969) 377--395.
5 Bradbury, S. and Eggleston, C., Postural hypotension: a report of three cases, Amer. Heart J., I (1925) 73--86.
6 Connett, R.J. and Kirshner, N., Purification and properties of bovine phenylethanol- amine-N-methyl transferase, J. biol. Chem., 245 (1970) 329--334.
7 Cryer, P.E., Silverberg, A.B., Santiago, J.V. and Shah, S.D., Plasma cat~ cholamines iN diabetes. The syndromes of hypoadrenergic and hyperadrenergic po~ural hypoten sion, Amer. J. Med., 64 (1978) 407--416.
8 Demanet, J.C., Usefulness of noradrenaline and tyramine infusion test in the diagnosi~ of orthostatic hypotension, Cardiology, 61, Suppl. 1 (1976) 213--224.
9 Drischel, H., Fanter, H., Gurtler, H., Labitzke, H. and Priegnitz, F., Das Verhalten der Herzfrequenz gesunder Menschen beim iJbergang vom Liegen zum Stehen, Arch. Kreislaufforsch., 40 (1963) 135.
10 Goodall, M., Harlan, W.R., Jr. and Alton, H., Noradrenaline release and metabolism in orthostatic (postural) hypoten~,~ion, Circulation, 36 (1967) 489--496.
11 Goodman, L.S. and Gilman, A., The Pharmacological Basis of Therapeutics, Mac- Milland, New York, 1975.
12 Hedqvist, P., Basic mechanisms of prostaglandin action on autonomic neurotransmis- sion, Ann. Rev. Pharmacol. To'_~ic.~l., 17 (1978) 259--279.
13 Henry, D.P., Starman, B.J., Johnson, D.G. and Williams, R.H., A sensitive radio- enzymatic assay for norepinephrine in tissues and plasma, Life Sci., 16 (19'75)375-- 384.
14 Hibbs, R.C., Burch, G.E. and Phillips, J.H., Electron-microscopic observations on the human mast cell, Amer. Heart J., 60 (1960) 121--127.
15 Johnson, R.H., Orthostatic hypotension in neurological disease, Csrdiology, 61, Suppl. 1 (1976) 150--167.
16 Kochar, M.S. and Itskovitz, H.D., Treatment of idiopathic hypotension (Shy--Drager syndrome) with indomethacin, Lancet, 1 (1978) 1011--1014.
17 Kontos, H.A., Richardson, D.W. and Norvell, J.E., Norepinephrme depletion in idio- pathic orthostatic hypotension, Ann. intern. Med., 82 (1975) 336--341.
18 Lake, C.R., Zeigler, M.G., Coleman, M.D. and Kopin, I.J., Age-adjusted plasma nor- epinephrine levels are similar in normotensive and hypertensive subjects, New Engl. J. Med., 296 (197 ]) 208--209.
19 McGrath, M.A. and Shepherd, J.T., Inhibition of adrenergic neurotransmission in canine smooth muscle by histamine: mediation by H2 receptors, Circulat. Res., 39 (1976) 566--573.
20 Pedersen, E.B. and Christensen, N.J., Catecholamines in plasma and urine in patients with essential hypertension determined by double-isotope derivative techniques, Acta med. scand., 198 (1975) 373--377.
21 Roessmann, U., van den Noort, S. and McFarland, D.E., Idiopathic orthostatic hypo- tension, Arch. Neurol. (Chic.), 24 (1971) 503--510.
22 Schirger, A. and Thomas, J.E., Idiopathic orthostatic hypotension: clinical spectrum and prognosis, Cardiology, 61, Suppl. 1 (1976) 144--149.
23 Sever, P.S., Catecholamines in essential hypertension: the present controversy. In W.H. Birkenhager and H.E. Falke (Eds.), Circulating C~techolamines and Blood Pres- sure, University Park Press, Baltimore, 1978, pp. 1--10.
24 Shy, G.M. and Drager, G.A., A neurological syndrome associated with orthostatic hypotension, Arch. Neurol. (Chic.), 2 (1960) 511--527.
25 Siemsen, J.K. and Meister, L., Bronchogenic carcinoma associated with severe ortho- static bypotension, Ann. intern. Med., 58 (1963) 669--676.

222,
26 Stjtirne, L. ar.d Gripe, K., Pmstaglandin-dependent and -independent feedback control of noradrenaline secretion in vasoconstrictor nerves of normotensive human subjects: a preliminary report, Naunyn-Schmiedeberg~ Arch. exp. Path. Pharmak., 280(1973) 441--446.
27 Thulesius, O., Pathophysiological classification and diagnosis of orthostatic hypoten- sion, Cardiology, 61, Suppl. 1 (1976) 180--190.
28 Thureson-Klein,/t,., Stjiirne, L. and Brundin, J., Uitrastructure of the nerves in veins fror~ human omentum, Neumseience, 1 (1976) 333--337.
29 Tuekman, ,J. and Shillingford, J., Effect of different degrees of tilt on cardiac output, heart rate and blood pressure in normal man, Brit. Heart J., 28 (1966) 32.
30 Weise, V.K. and Kopin, l.J., Assay of cateeholamines in.human plasma: studies of a single i.~otope radioenzymatie procedure, Life Sci., 19 (1976) 1673--1G86.
31 Ziegler, M.G., Lake, C.R. and Kopin, l.J., Plasma noradrenaline increases with age, Nature (Lond.), 261 (1976) 333--335.
32 Zeigler, M.G., Lake, C.R. and Kopin, l.J., The sympathetic nervous system defect in primary orthostatie hypotension, New Engi. J. Med., 296 (1977) 293--297.