Embed Size (px)
Citation preview

IIM - Epidemiology
• Rare, estimated annual incidence 5-10/million, estimated prevalence ~ 60/million.
• PM and DM peak in prevalence in childhood (5-15yrs) and mid-life (30-50yrs); IBM peaks after age 50.
• Females are preferentially affected (~2-3:1) in all forms except in IBM (female:male~1:3).
IIM - Epidemiology
• African-Americans may be at increased risk for IIM and poorer outcomes compared to Caucasians.
• All races on all continents are affected.• Anecdotal clustering of IIM onset in time and
space suggest strong environmental influences.
IIM – Systemic manifestations
• General manifestations:fatigue, fever, weight loss.
• Musculoskeletal: myalgia, muscle tenderness and weakness. Arthralgia, arthritis, contractures.
• Dermatologic:Photosensitive rashes and edema. Vasculitis with infarcts and ulceration. Subcutaneous inflammation (panniculitis) and calcification.
IIM – Systemic manifestations
• Gastrointestinal: oropharyngeal involvement with tongue weakness and voice changes; dysphagia and reflux.
• Pulmonary:Atelectasis, cough. Interstitial lung disease. Aspiration.
• Cardiovascular:Tachyrhythmias and other conduction abnormalities. Congestive heart failure from myocarditis or cor pulmonale. Raynaud.












IIM - Evaluation
• Careful history and physical examination to define:
1. The time\tempo of symptom onset and progression.
2. The exact nature of the problems and associated factors.
3. Medical and family history.4. Muscle bulk/strength, rashes, cardiac,
pulmonary, GI findings.5. Environmental exposures temporally associated.
IIM - Evaluation
• Laboratory evaluation directed by the above:
1. Muscle enzymes, serologies, tests to R/O other diseases.
2. Radiographic studies, muscle MRI.
3. EMG, biopsies of skin, muscle, possibly other tissues.
4. Special serologic or genetic studies depending upon results from the above.

IIM – Laboratory abnormalities
• Sarcoplasmic enzymes (CPK, LDH, ALT, AST, aldolase) – useful in assessing myositis activity.
• CPK MB fraction – correlates with diseases activity and is not usually indicative of cardiac involvement unless the ratio of CK-MB/total CK rapidly increases.
• ESR/CRP – elevated in <30% of pts.• ANA – positive in 60-90% of pts; best single lab
discriminator of IIM from other myopathies.
Causes of elevated serum CPK enzyme activity
• Physical trauma or muscle stress.1. Any muscle trauma – falls, EMG studies,
surgery, muscle bipsy, IM injection.2. Strenuous, prolonged exercise-marathon
running, forced marching.• Drug effects1. On muscle itself – clofibrate, ethanol,
amphetamines, heroin.2. On CK metabolism/clearance-phenobarbital,
morphine, diazepam.
Causes of elevated serum CPK enzyme activity
• Diseases1. Directly affecting muscle-non inflammatory
myopathies of all kinds, MI, malignant hyperthermia, infectious myopathies, IIM.
2. Affecting blood supply to muscle-emboli to muscle, vasculitis,prolonged immobilization.
3. Affecting the CNS-cerebral ischemia, trauma,infections.
• Possible familial cases in African-Americans.
Myositis –specific autoantibodies (MSA)
1. Anti-synthetases – Jo 1(anti histidyl tRNA synthetase).
2. Anti-signal recognition particle (SRP).
3. Anti-Mi-2.• They are directed at conserved conformational
epitopes on phosphorylated, cytoplasmic ribonucleoprotein particles involved in translation and present in all cells.
MSA
• They inhibit the function of the protein they target.• They appear to arise months prior to myositis
onset, are antigen driven, vary in titer with myositis disease activity and occasionally become negative after prolonged remission.
Associations of the MSA
• Anti-synthetases (Jo1):• Arthritis, interstitial lung disease, fevers,
mechanic’s hand, Raynaud’s.• Acute onset, severe disease.• Moderate response to therapy.• Prognosis poor; 70% 5-yrs survival.• Frequency in IIM 25-30%.
Associations of the MSA
• Anti-SRP:• Cardiac involvement, myalgias, mostly in black
females.• Very acute onset, very severe disease.• Poor response to therapy.• Poor prognosis – 25% 5 yrs survival.• Frequency in IIM – 5%.
Associations of the MSA
• Anti-Mi-2:• Classic dermatomyositis.• Acute onset. Mild disease.• Good response to therapy• Good prognosis. Nearly 100% 5 yrs survival/• Frequency in IIM 5-10%.
IIM - pathogenesis
• Polymyositis and inclusion body myositis may be more cellularly mediated (CD8+ T cells).
• Dermatomyositis may be more humorally mediated (B cells).
IIM – Activity evaluation
1. Muscle strength – grading:• 5 – normal power resistance.• 4 – power decreased but muscle contraction
possible against resistance.• 3 – muscle contraction against gravity only.• 2 – muscle contraction possible only when
gravity is eliminated.• 1 – contraction without motion.• 0 – no contraction.
IIM – Activity evaluation
2. CPK levels.
3. EMG: fibrillations, positive sharp waves, short small polyphasic motor units, high frequency repetitive discharges, normal nerve conduction velocities.
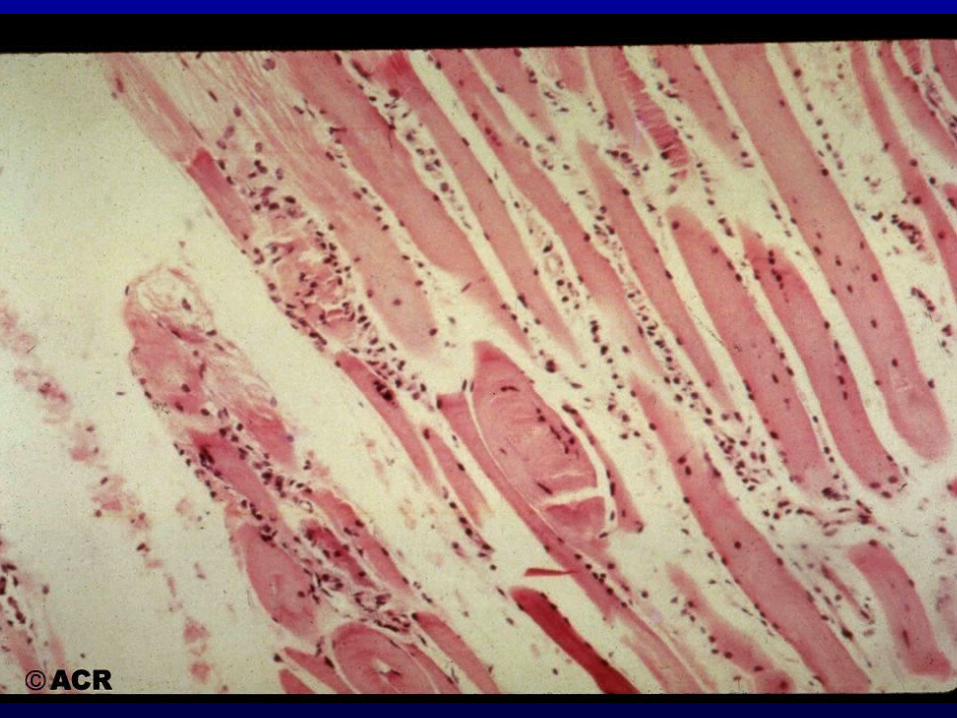
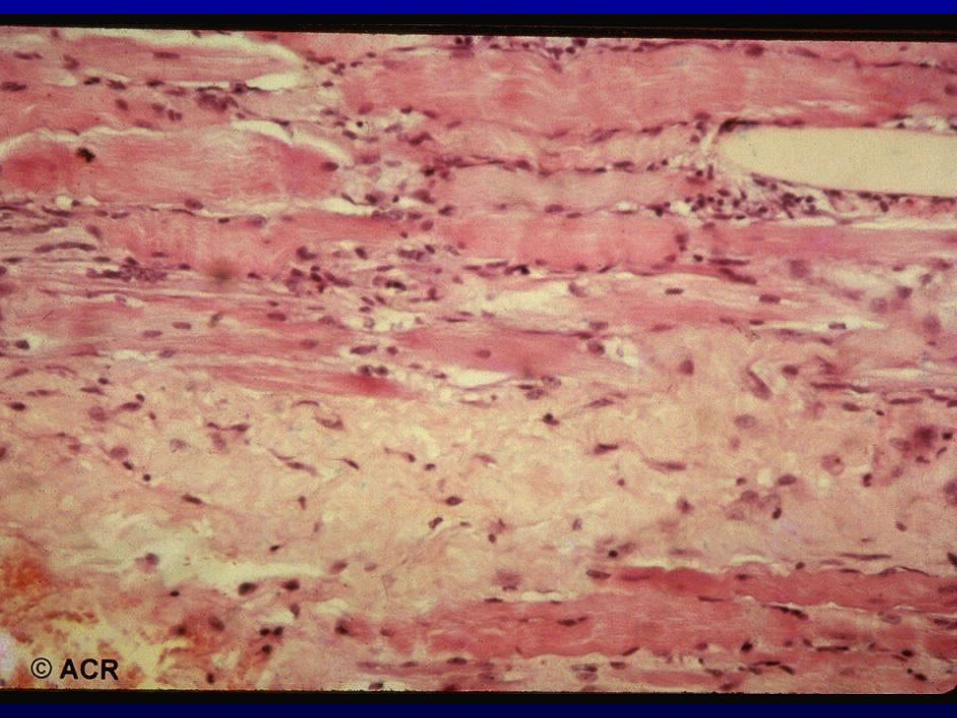
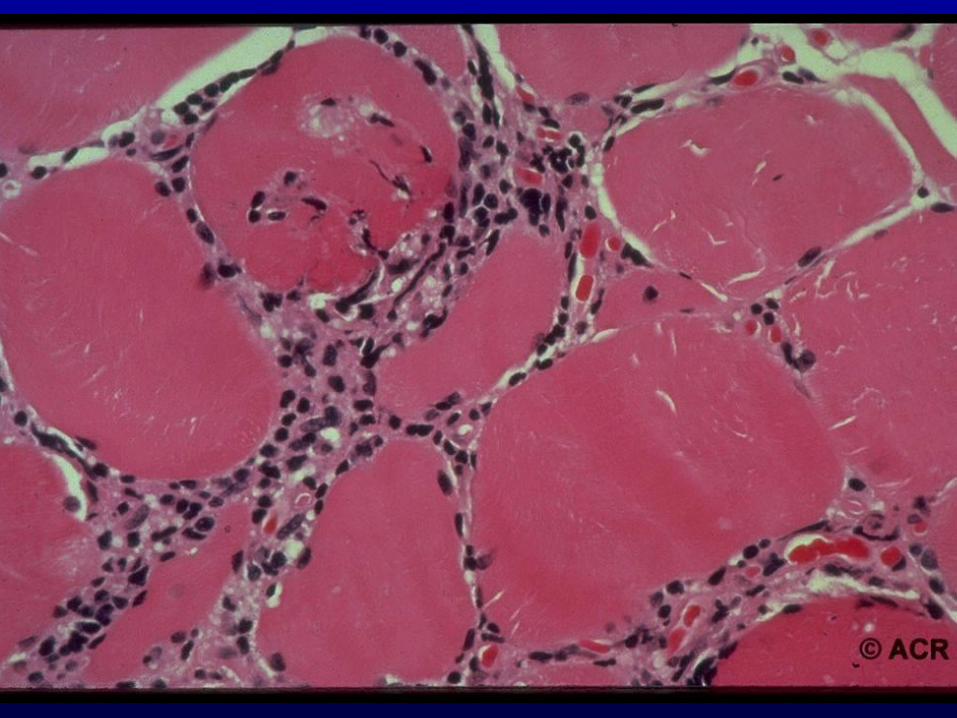
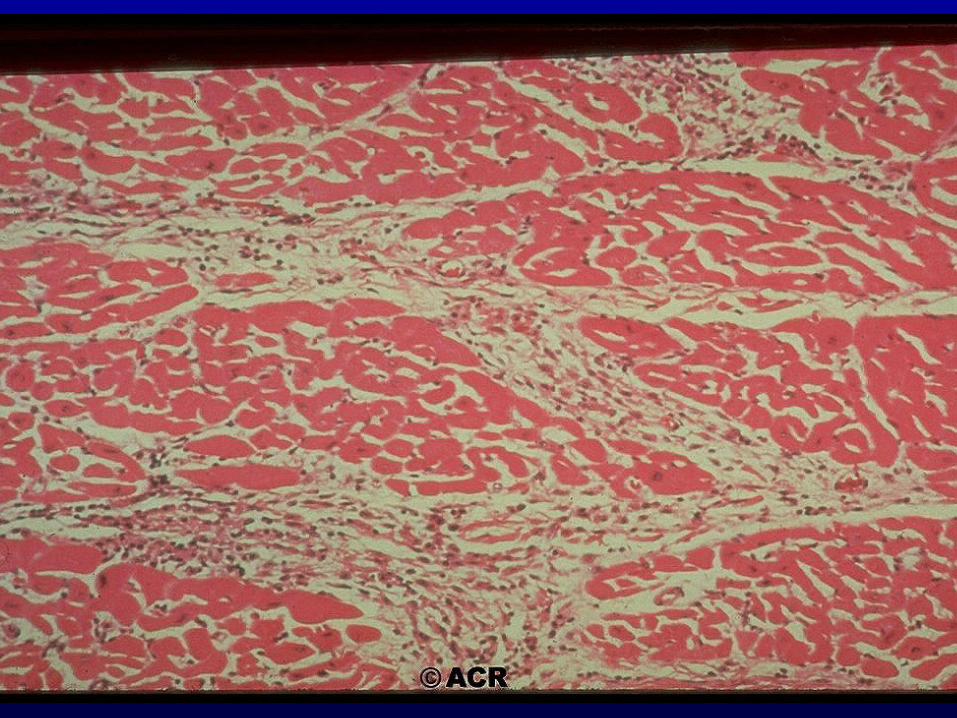
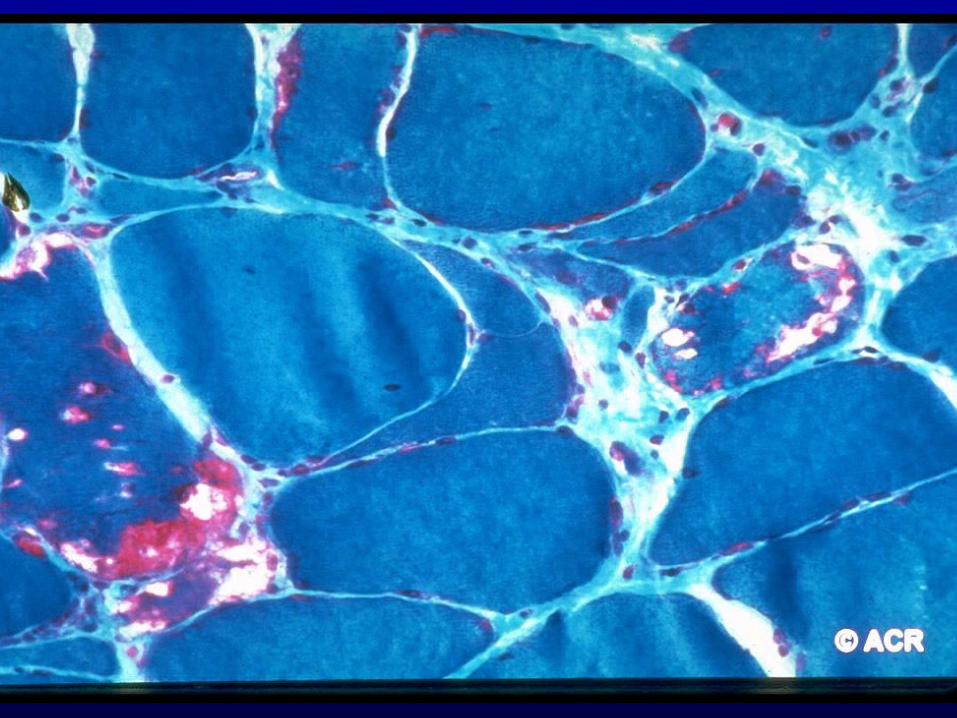
4. Muscle biopsy: myofiber degeneration/regenaration, MNC infiltrates, perifascicular atrophy.
IIM – Activity evaluation
4. MRI: T1-weighted images – chronic changes in muscles, atrophy.
T2 – weighted and STIR images – active inflammation.
• Biopsy is taken from a weak muscle, without atrophy, not damaged by EMG, injection, etc.
Poor prognostic factors in Myositis
• Based on demographic features:1. Age : older.2. Gender: female.3. Race: black.• Based on signs-symptoms:1. Fever, dysphagia, severe myositis.2. Cardiac, pulmonary or GI involvement.3. Delay to diagnosis and treatment.4. Failure to induce remissin.
Poor prognostic factors in Myositis
• Based on clinical or serologic group:
1. Clinical groups: polymyositis, cancer-associated or inclusion body myositis.
2. Serologic groups: anti-synthetases or anti-SRP autoantibodies.
Therapy
• Steroids 1-2mg/kg/d.• Cytotoxic: MTX, AZT, cytoxan• IVIG• Plaquenil (rash).• Rehabilitation and physical therapy.





![Prevalence of Children with Severe Fetal Alcohol Spectrum ...FAS prevalence of 3.7 to 7.4 per 1,000. Overall FASD was estimated as 35 per 1,000 (3.5%) [38], Overall FASD was estimated](https://img.pdfslide.net/doc/110x75/5fa3fe3b02308246357b1359/prevalence-of-children-with-severe-fetal-alcohol-spectrum-fas-prevalence-of.jpg)