Embed Size (px)
Citation preview

IL TRAPIANTO
DA CUORE NON BATTENTETeresa Rampino

11 Settembre 2008….. 2018
I° TRAPIANTO NHBD

TRAPIANTI DA DONATORE A CUORE NON BATTENTE O DOPO MORTE CIRCOLATORIA ( DCD) in Italia
Dati CNT 2018 parziale
107 TX RENE

Pavia
Milano
Padova
Bologna
FirenzeSiena
Verona
Palermo

Un rene di serie B?
DCD DBD

Donor after Circulatory Death
Permanent absence of circulation and respiration
Criteria for determination of death

Cardiac Arrest Loss of perfusion
ISCHEMIA
ANOXIA
Anoxic Injury
Irre
vers
ible
Inju
ry
>5’
Patient death
25-75’
15-120’
15-33’
24 h tissues
DONOR IN ASYSTOLE

Trends in Anaesthesia and Critical Care (2013); 72-76
Maximum tolerable warm ischaemia time in
transplantation from non-heart-beating-donors

PERIODO “NO TOUCH”
IL PERIODO IMPOSTO DALLA LEGGE PER LA DICHIARAZIONE DELLA MORTE CARDIACA
20 min

COUNTRYNO-TOUCH TIME
(MINUTES)
AUSTRIA 10
BELGIUM 5
CZECH REPUBLIC 10
FRANCE 5
ITALY 20
LATVIA 15
THE NETHERLANDS 5
UNITED KINGDOM 5
SPAIN 5
SWITZERLAND 10
Wind et al. Crical Care 2013, 17:R217
Variability of DCD protocols in Europe

AUTORESUSCITATIONE
«Lazarus phenomenon»
Ritorno spontaneo alla circolazione non assistita dopo l’arresto cardiaco

Homby K, Homby L, Shemie SD Crit Care Med 2010 (38), 5

Dopo un perioido“no-touch” di 20 minuti non esiste la possibilità di autoresuscitazione
Nel contesto italiano

CoordinamentoProtocollo ben definitoEsperienzaRisorse tecniche adeguate

Modified Thuong M et al, Transplant International 2016; 29: 749–759
(1995)The Maastricht categories of NHBD
Uncontrolled
Controlled
Partiallycontrolled

ACC
Heart activity
DCD Donor DEATH
ECMO
ADVANCED RESUSCITATION PROGRAM
Neurological
criteria
Cardiac
criteria
ECMO prior to death (EPD)

Class UNCONTROLLED
I Dead on arrival
II Unsuccessful resuscitation

150 min
TOTAL WARM ISCHEMIA TIME
1 – 4 hs (max 6)
ACLS
DECLARATION OF DEATH
CPR
EC
G20 min15 -20m
No flow
CardiacArrest
Organ Preservationin situ
Harvesting
Transp
lant
Cold Storage / Machine Perfusion
Low flow
DCD - UNCONTROLLED
ACLS Advanced CardiovascularLife Support
CPR CardiopulmonaryResuscitation


Class CONTROLLED
III Awaiting cardiac death
IV Cardiac death in a brain-dead donor

TOTAL WARM ISCHEMIA TIME
1 – 4 hs (max 6)
DECLARATION
OF DEATH
EC
G
20 min
No flow
Asystole
Organ Preservation
Harvesting
Tra
nsp
lan
t
Cold Storage/
Machine Perfusion
Low flow
DCD - CONTROLLED
withdrawal life
sustaining
treatment
Blood Pressure
Agonal phase
Functional WIT
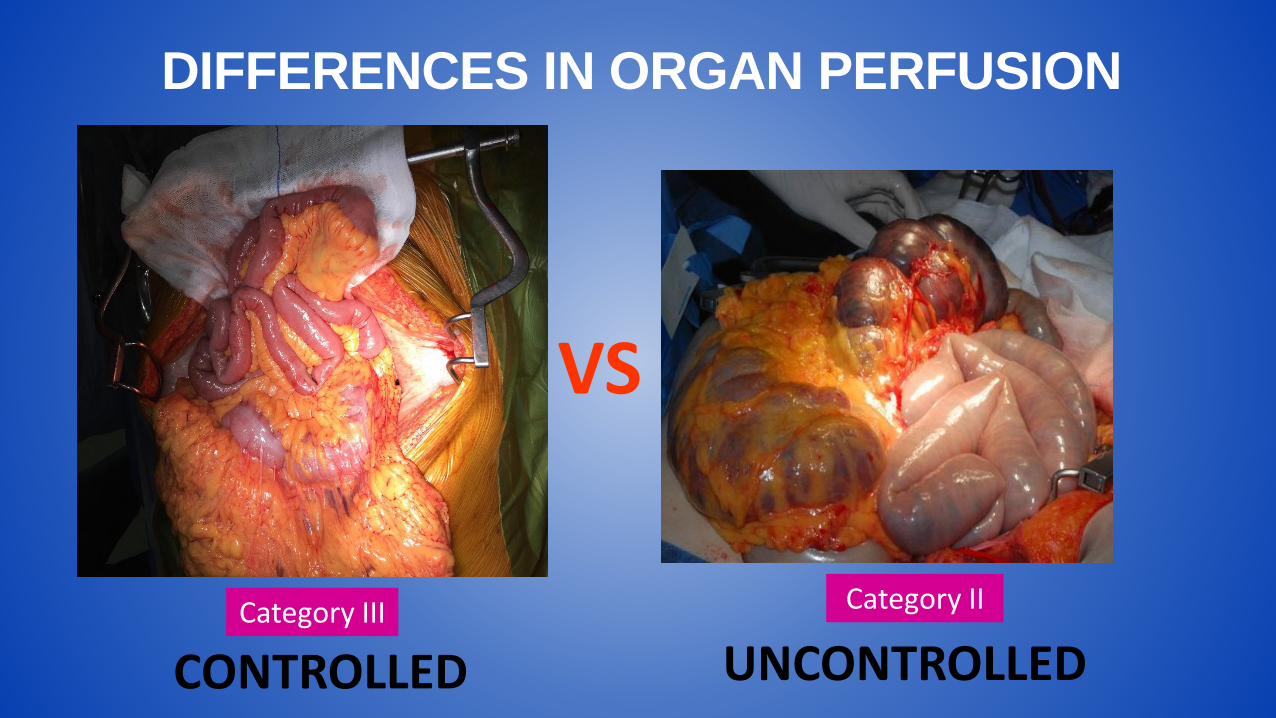
Category IICategory III
VS
DIFFERENCES IN ORGAN PERFUSION
CONTROLLED UNCONTROLLED


filmato

NORMOTERMIC REGIONAL PERFUSION
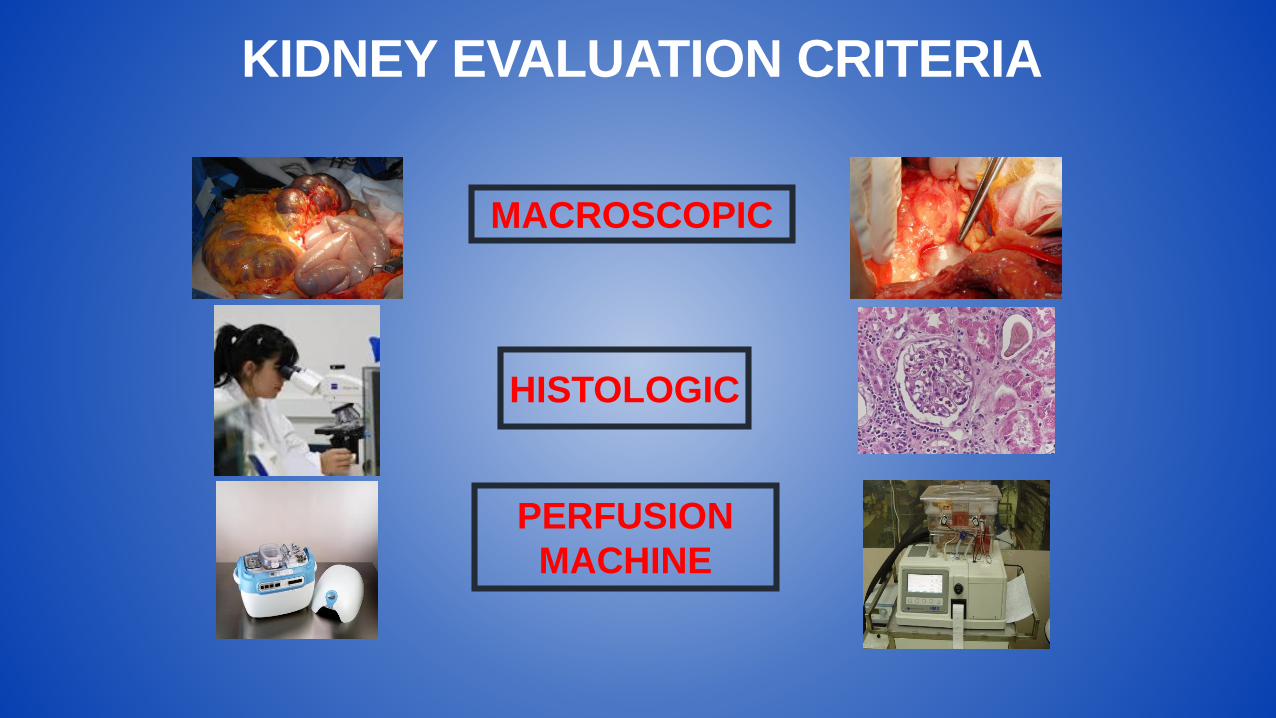
MACROSCOPIC
PERFUSION
MACHINE
HISTOLOGIC
KIDNEY EVALUATION CRITERIA

PRE -TRANSPLANT KIDNEY BIOPSY
ACUTE DAMAGE
CHRONIC DAMAGE
REMUZZI HISTOPATHOLOGICAL SCORE

CAPILLARY AND ARTERIOLAR TROMBOSIS
ACUTE DAMAGE
YES NO
TX
TUBULAR NECROSIS

DCD KIDNEY BIOPSY AT RETRIEVAL

RR 0,33
F 0,68 ml/min
DCD KIDNEY BIOPSY AFTER PULSATILE PERFUSION

Renal Resistance
(RR):
RR < 0,40
Perfusion Flow:
> 60 ml/min
Perfusional Criteria

RENAL RESISTENCE TREND DURING HYPOTHERMIC MACHINE PERFUSION IS PREDICTIVE OF GRAFT OUTCOME

RISORSE TECNOLOGICHE


PRESERVATION EX SITU
VS

HYPOTHERMIC
MACHINE PERFUSION
NORMOTHERMICSUBNORMOTHERMIC
4°C 20-25°C 32-36°C
+ O2 + O2

EX-VIVO MACHINE PERFUSION FOR KIDNEY PRESERVATION
Curr Opin Organ Transplant 2018, 23:369–374



Trapianto DCD: ne vale la pena?

Snoejis MG et al. JASN 2010
Kidneys from DCD provide survival benefit

Kidney International (2015)
Kidney donation after circulatory death (DCD) versus donation after brain death ( DBD)

Snoeijs MGJ et al. Transplantation 2010
Kidneys transplantation from DCD

DONOR IN ASYSTOLE

PRIMARY NON FUNCTION (PNF)perdita permanente della funzione del rene subito
dopo il Tx

PRIMARY NON FUNCTION (PNF)FREQUENCY ACCORDING TO TYPE OF DONATION

Rigetto iperacuto
CID
Sindrome Emolitica Uremica
Recidiva immediata di malattia di base
Ossaluria primaria
Trombosi
Emodinamica intraoperatoria
CAUSE PNF

Risk factors for primary non-functionin DCD
BMI > 25 kg/mq
Terminal creat.
Recipient age
Flow rate > 70
HLA mismatch
Resistive index > 0,4
Warm ischemia time>30 min
Donor category
Donor age>40y
Cause of death (CV)
Pre op sys BP<130 mmHg
Intra op sys BP<110mmHg
Central venous BP <4cmH2O

Post-operative graft functionAccording to average intra operative Central Venous Pressure
4
53 20
8 16

RENAL CORTICAL NECROSIS
TAC
ECOGRAFIA CON MDC
ISTOLOGIA

DELAYED GRAFT FUNCTION (DGF)Necessità di dialisi entro la prima settimana dopo
trapianto renale

DCD DBD ODDS p VALUE
DGF 72% 18% 10,3 < 0,001
DELAYED GRAFT FUNCTION in Kidney Transplantation From Donors After Cardiac Death
Transplantation, Volume 90, Number 10, November 27, 2010
0%
20%
40%
60%
80%
100%
DBD DCD
DG
F

Transplant International (2011) 676-686
ControlledDCD
UncontrolledDCD
DGF in Kidney Transplantation from controlledversus uncontrolled donation after circulatory death

Attivazione linfociti TDAMPs
Cellule dendriticheROS
Interleukines

DGF influenza la sopravvivenza di un trapianto da donatore a cuore non battente

Snoeijs et al..Transplantation • 90, 10-27, 2010
DCD GRAFT SURVIVAL
Delayed Graft FunctionImmediate Graft Function
Gra
ftsu
rviv
al
Time after transplantation (Yr)

Graft survival of DCD and DBD kidney with DGF
DCD with DGFDBD with DGF

DONATION AFTER BRAIN DEATH
DONATION AFTER CIRCULATORY DEATH
ischemia
Necrosi tubulare
acuta
Catecholaminestorm
Cytokines
Peripheralischemia
IL 1TNFIL 6
Vasoconstriction
Activation of endothelium
Immune response
MHC
Organinflammation
IL 1
TNF
IL 6
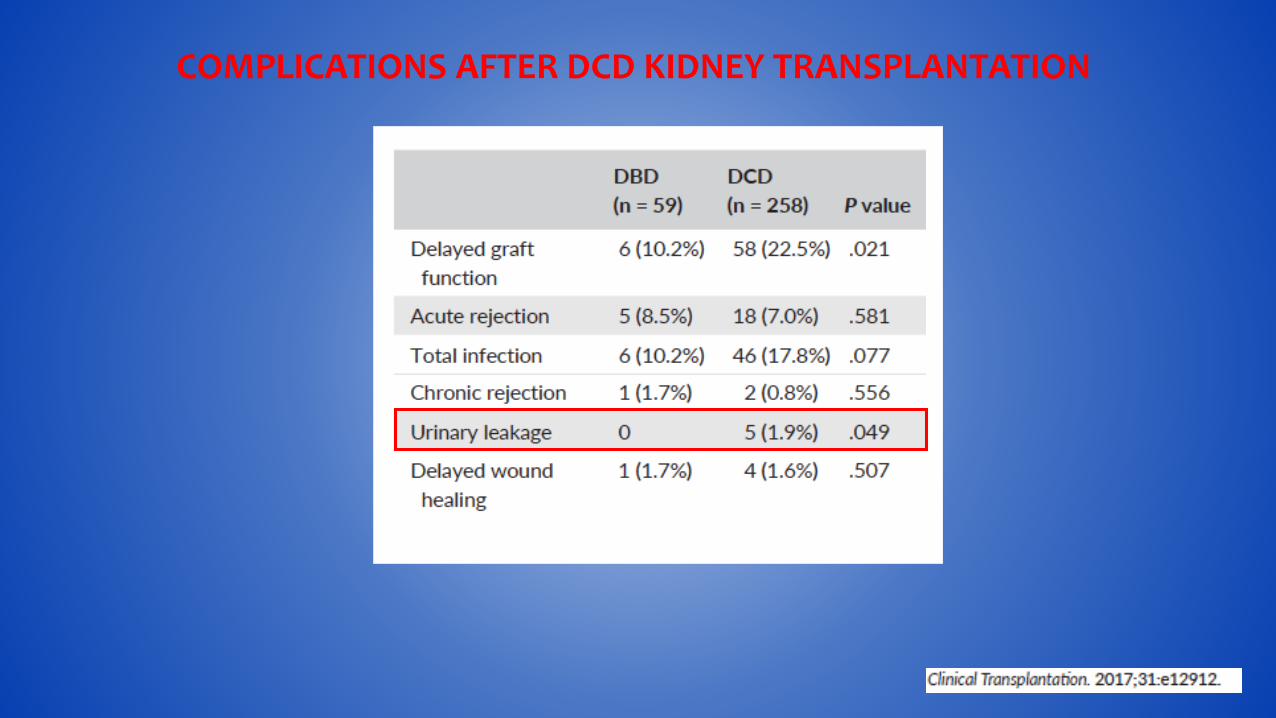
COMPLICATIONS AFTER DCD KIDNEY TRANSPLANTATION

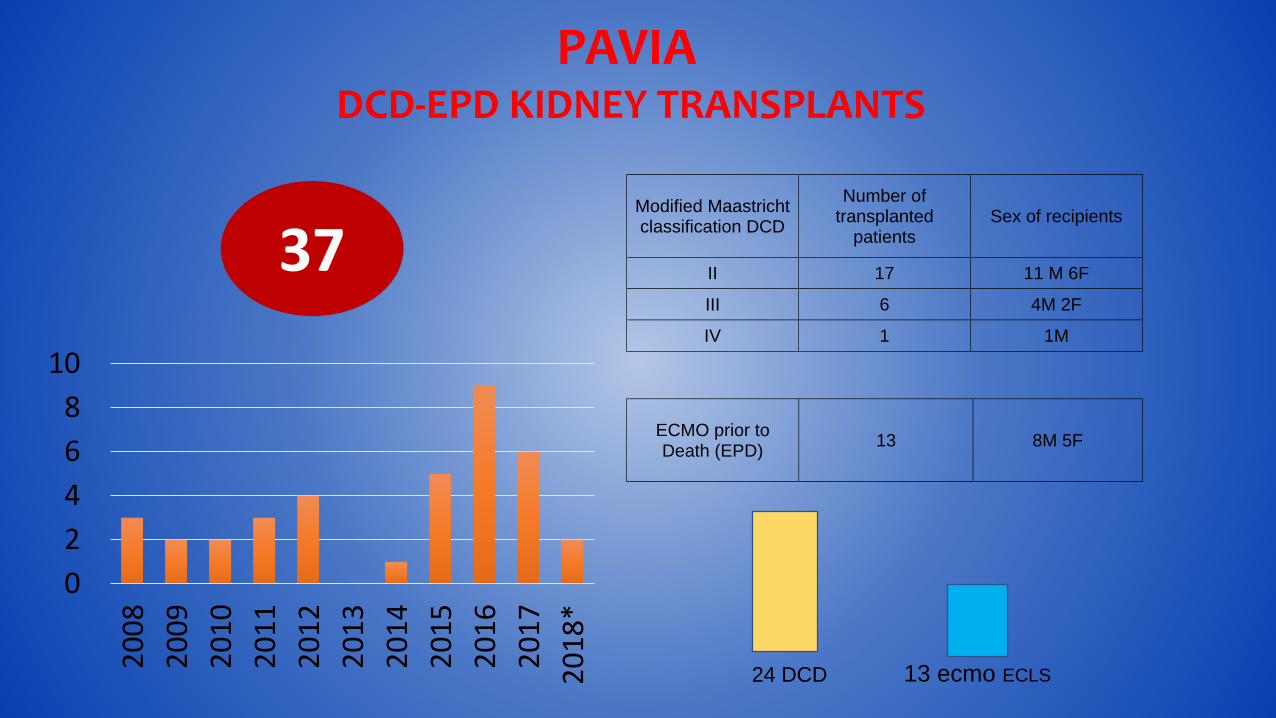
PAVIADCD-EPD KIDNEY TRANSPLANTS
Modified Maastricht classification DCD
Number of transplanted
patients Sex of recipients
II 17 11 M 6F
III 6 4M 2F
IV 1 1M
ECMO prior to Death (EPD)
13 8M 5F
37
24 DCD 13 ecmo ECLS
0
2
4
6
8
10
20
08
20
09
20
10
20
11
20
12
20
13
20
14
20
15
20
16
20
17
20
18
*

Donor Age (years) ( mean and sd) DCD group 51± 8.3
Recipient Age (years) ( mean and sd) DCD group 53.8±11.2
Sex of donor M/F DCD group 20/3
Sex of recipient M/F DCD group 16/7
DEMOGRAPHIC CHARACTERISTICS

VARIABLE MEDIAN IQR
DAYS OF DGF 11.5 8.25-17.5
NUMBER OF
DIALYSIS
6 4--9
DCD Group
VARIABLE MEDIAN IQR
DAYS OF DGF 4 1-9.5
NUMBER OF DIALYSIS 2 0--5
EPD Group
DGF 53% DGF 90%
Delayed Graft Function

GRAFT SURVIVAL
87%
13%
graft survival
graft loss
Trombosi vena renalePNF
Sepsi severa
DCD EPD
92%
8%
graft survival
graft loss
PNF

PATIENT SURVIVAL
69%
31%
surviving patients
dead patients
DCD EPD
87%
13%
surviving patients
dead patients
CancroComplicanze cardiovascolari
CancroComplicanze cerebrovascolari

DBD w
eek 1
DCD w
eek 1
EPD w
eek 1
DBDye
ar 1
DCD y
ear 1
EPD yea
r 1
DBD yea
r 3
DCD y
ear 3
EPD yea
r 3
0
5
10
15
*
*p<0.001 vs DBD and EPD week 1
° °p<0.001 vs DBD, DCD, EPD year 1,3
se
rum
cre
atin
ine
mg
%
RENAL FUNCTION in DCD, EPD and DBD

Induction Immunosuppressive therapyPAVIA
Thymoglobuline
2017
2016
2015
2014
2013
2012
2011
Thymoglobuline[iperimmune/diabetic patients]
Basiliximab
+ steroid, CNI inhibitors and MMF

DGF; 85%
THYMOGLOBULINE
DGF 76%
PNF; 9%
BASILIXIMAB
DGF and PNF
9 days(Median)
11 days(Median)
IR 15% IR 15%

DCDDBDSTESSO PROGRAMMA VISITE FOLLOW UP
STESSE TERAPIA IMMUNOSOPPRESSIVA
STESSO PROGRAMMA BIOPSIE PROTOCOLLARI

THE FUTURE
Stem cellsPharmaco therapyAnti inflammatory reagentsGene transferOxygenation
Kidney conditioning with

Rampino T et al.
Rene umano

Un rene di serie B?
DCD DBD






























