Embed Size (px)
Citation preview
REVIEW ARTICLE
Imaging Aspects of Pyogenic Infections of theCentral Nervous System
Nelson Paes Diniz Fortes Ferreira, MD,* Gilberto Miyazaki Otta, MD,*
Lazaro Luıs Faria do Amaral, MD,* and Antonio Jose da Rocha, MD†
Abstract: Although pyogenic infections of the central nervous
system are not a frequent group of diseases, their morbidity and
mortally are very high. For this reason they require prompt diagnosis
and treatment to avoid several complications that can lead to an
undesired outcome. In this article, we review the imaging findings of
these infections according to the anatomic site, their complications,
and their differential diagnosis. Special attention is given to the
different techniques of magnetic resonance imaging like perfusion,
spectroscopy, and diffusion, for each specific situation such as
meningitis, abscess, ventriculitis, purulent extra axial collections, and
vascular complications.
Key Words: brain, meningitis, MRI, pyogenic abscess
(Top Magn Reson Imaging 2005;16:145–154)
Central nervous system (CNS) infections constitute a groupof life-threatening diseases, which present themselves
with various clinical and imaging manifestations, forming aninteresting and challenging pattern for diagnosticians. Thebrain has some unique peculiarities like absence of lymphatics,lack of capillaries in the subarachnoid space, and presence ofcerebral spinal fluid (CSF), which is an excellent culture mediumfor dissemination of infectious processes, in the subarachnoidspace and into the ventricular system. Anatomically, pyogenicinfections can be divided into four main categories as follows:
1. Diffuse: meningitis2. Focal: cerebritis and abscess3. Extra-axial: empyema and subdural effusions4. Ventricular infections: ventriculitis.
Central nervous system infections are not frequent,accounting for 1% of primary hospital admissions and 2% ofnosocomially acquired infections1,2 and when encountered,require prompt diagnosis and initiation of specific treatment.
Pyogenic infections are one of the few curable categoriesof diseases affecting the CNS, where the untreated cases
rapidly progress to a fatal outcome and most of the deathsoccur within the first 24 hours of hospitalization.1,3
Acute bacterial meningitis can be caused by a range ofpathogens. Streptococcus pneumoniae is responsible forapproximately 47% of the cases, Neisseria meningitidis for25%, group B Streptococcus for 12%, and Listeria mono-cytogenes for 8%.4,5 The agents vary according to the age ofthe patient. In the Schuchat et al5 series, the main pathogen inthe neonatal group was group B Streptococcus; in infants (1 to23 months), S. pneumoniae caused 45% and N. meningitidiscaused 31% of the cases; through the ages 2 to 18 years, N.meningitidis was the main causative agent. Pneumococcus wasresponsible for 62% of cases in persons older than 19 yearsold.4,5
Focal suppurative process within the brain parenchymais frequently secondary to paranasal sinuses infections with25% of the cases occurring in pediatric patients, with peak ageoccurrence between 4 and 7 years. The most common caus-ative agents isolated are S. aureus, Enterobacteriaceae, S.pneumoniae, H. influenzae, streptococci of intermedius group,and Bacterioides.4,6
Significant improvements in imaging modalities, likemagnetic resonance imaging (MRI), making possible earlierdiagnoses and advances in the treatment of bacterial infections,have resulted in a decline in the incidence of complicationsand of the mortality rates.3 More recently, the advanced MRItechniques, such as proton MR spectroscopy (H-MRS), diffusion-weighted imaging (DWI), and perfusion-weighted imaging(PWI), have improved even more the detection and charac-terization of infectious lesion in the CNS.
DIFFUSE PYOGENICINFECTIONS (MENINGITIS)
Meningitis refers to an acute or chronic inflammatoryprocess of the pia-arachnoid (leptomeninges) and CSF. In-fectious meningitis is clinically classified into:
Acute pyogenicAseptic (usually viral), not discussed in this articleChronic (fungus, parasites) also not discussed in this article.
There are some routes of entry for infectious agents intothe CNS like hematogenous spread (more frequent), directinoculation (trauma, surgery), and local extension secondaryto an infection in the paranasal sinuses or in the mastoids.7
Pathologically the infectious process results in conges-tion and inflammation of meningeal vessels and cerebralcapillaries, increasing the permeability of the blood-brainbarrier and in distension of the subarachnoid space (SAS) by
From the *Department of Neuroradiology, Medimagem—Hospital Benefi-cencia Portuguesa de Sao Paulo, Sao Paulo, Brazil; †Department ofNeuroradiology—Santa Casa de Misericordia de Sao Paulo andLaboratorio Fleury, Sao Paulo, Brazil.
Reprints: Nelson Paes Diniz Fortes Ferreira, MD, Department of Neurora-diology, Medimagem—Hospital Beneficencia Portuguesa de Sao Paulo,Rua Maestro Cardim 769, Bela Vista, Sao Paulo, SP-Brazil 01323-000(e-mail: [email protected]).
Copyright � 2005 by Lippincott Williams & Wilkins
Top Magn Reson Imaging � Volume 16, Number 2, April 2005 145
exudates containing polymorphonuclear neutrophils, makingcerebrospinal fluid cloudy and sometimes purulent.1,8 Themeningeal exudates, containing leukocytes and fibrins, cansometimes result in block-age of CSF absorption in arachnoidsvilli leading to hydrocephaly. The progression of meningealinflammation can complicate with vasculitis and thrombosis ofthe superficial pial vessels leading to ischemia and infarction.
Patients initially present with headache and fever, fol-lowed by meningismus and decreased level of consciousness.Seizures and focal neurologic deficits may also occur.3 Thediagnosis is based in clinical and physical signs, and con-firmed by lumbar puncture and CSF analyses.
ROLE OF IMAGINGThe initial imaging study is cranial computed tomog-
raphy (CT) scanning to exclude conditions that contraindicatelumbar puncture, to detect possible complications and to ex-clude other conditions. Most of the CT scanning studies inpatients with uncomplicated meningitis are normal.9 CT andMRI scanning can demonstrate obliteration of SAS and basalcisterns, ventriculomegaly and meningeal enhancement.
Comparing CT and MRI, obviously the latter is moresensitive, but its sensibility varies with the performedsequences.10–12
MAGNETIC RESONANCE IMAGINGT1 weight (T1WI) post-contrast images are more sen-
sitive than CT to demonstrate meningeal enhancement andthis finding is noted in approximately 55% to 70% of patientswith clinically proven meningitis.11,13,14 The literature is con-troversial if T1WI post contrast is more effective than FluidAttenuated Inversion Recovery (FLAIR) sequences with orwithout contrast material in the diagnoses of meningealdiseases. Some authors have reported that T1WI post contrastis superior to FLAIR15 and post-contrast FLAIR acquisitions.16
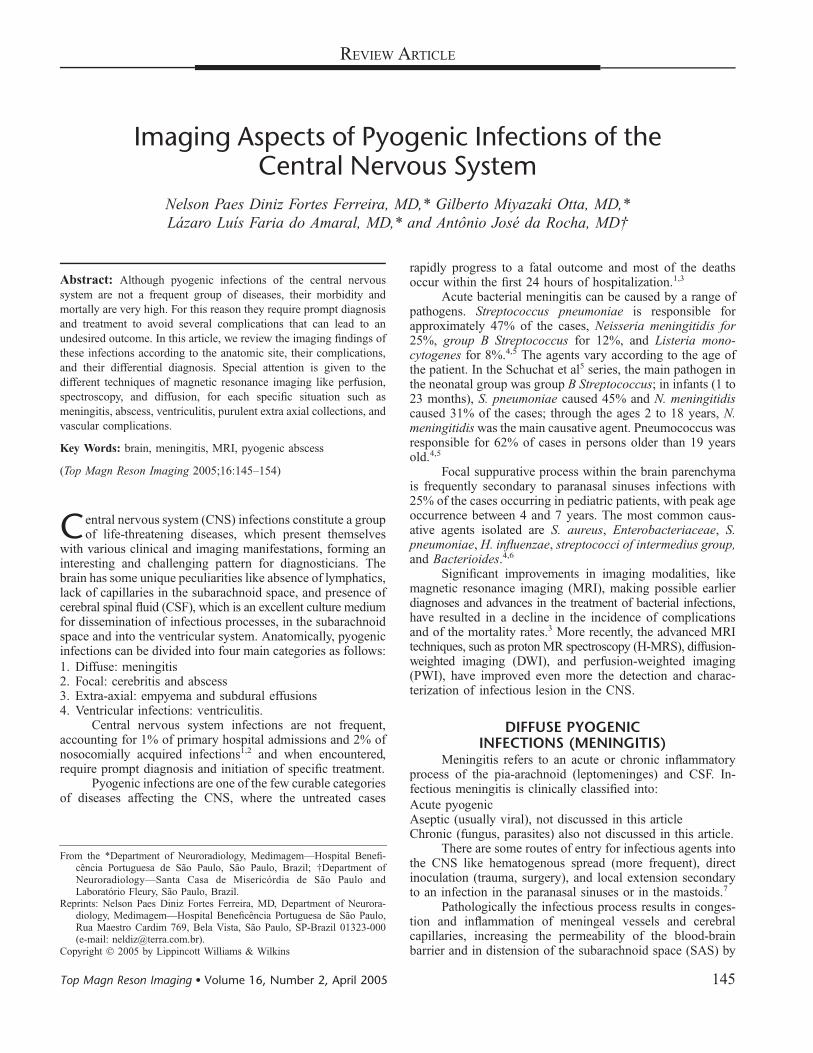
On the sequence FLAIR without contrast, the high signalof CSF is effectively nullified by an inversion recovery pulseafter an inversion time. Many authors have described thatFLAIR sequences are very sensitive to detect leptomeningealdiseases.11 This is explained by the elevation of protein levelsin SAS, causing a decrease in T1 relaxation time and resultingin hyperintensity (Fig. 1). Detection of nonhemorrhagic SASconditions has increased to approximately 88% with FLAIR
acquisitions.11 In spite of the high sensitivity of FLAIR imagesto detect hyperintensity within SAS, this finding is not specificfor meningitis and might be encountered in several diseasesand in normal conditions.10,17 For this reason one must keep inmind that several clinical conditions can occur with CSFhyperintensity on FLAIR images and some cautions should betaken, as follows:
After lumbar puncture the enhancement of the leptomeningesand the dura can persist over several weeks. For thisreason, in cases of suspected meningitis, the MR studyshould be performed before the lumbar puncture.10
The hyperintensity of the SAS on FLAIR images relatedto high levels of protein, is encountered in otherpathologies like subarachnoid hemorrhage, leptomenin-geal metastasis, and moyamoya disease.10
It has been recently described10,17 that slow arterial flow(arterial hyperintensity sign) and retrograde collateralslow flow in engorged pial arteries, via leptomeningealanastomosis (ivy sign), encountered in acute stroke andsevere arterial occlusive disease, may also causeleptomeningeal hyperintensity on FLAIR images.
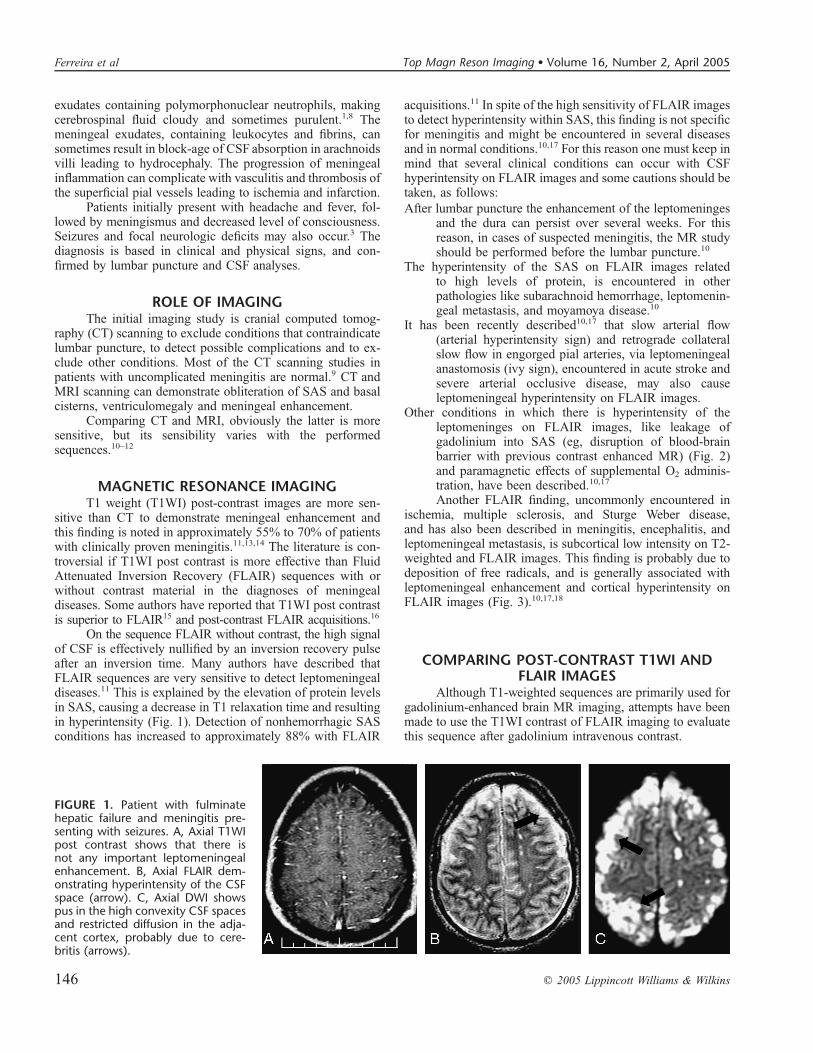
Other conditions in which there is hyperintensity of theleptomeninges on FLAIR images, like leakage ofgadolinium into SAS (eg, disruption of blood-brainbarrier with previous contrast enhanced MR) (Fig. 2)and paramagnetic effects of supplemental O2 adminis-tration, have been described.10,17
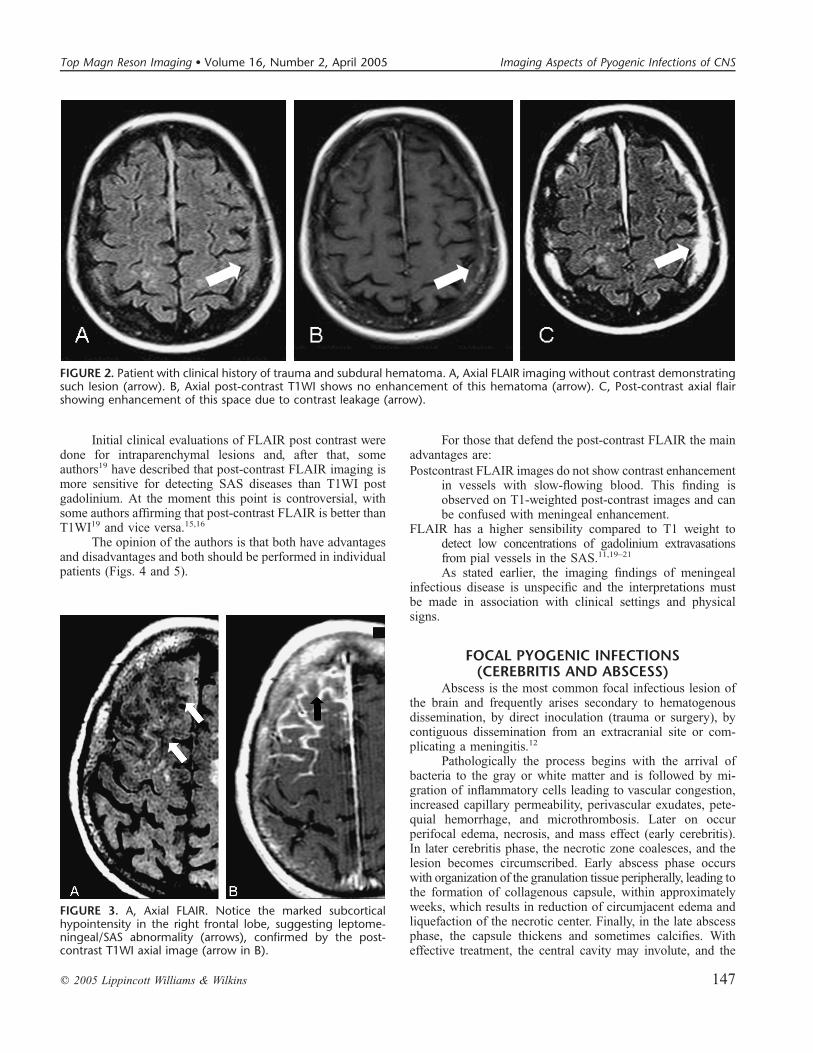
Another FLAIR finding, uncommonly encountered inischemia, multiple sclerosis, and Sturge Weber disease,and has also been described in meningitis, encephalitis, andleptomeningeal metastasis, is subcortical low intensity on T2-weighted and FLAIR images. This finding is probably due todeposition of free radicals, and is generally associated withleptomeningeal enhancement and cortical hyperintensity onFLAIR images (Fig. 3).10,17,18
COMPARING POST-CONTRAST T1WI ANDFLAIR IMAGES
Although T1-weighted sequences are primarily used forgadolinium-enhanced brain MR imaging, attempts have beenmade to use the T1WI contrast of FLAIR imaging to evaluatethis sequence after gadolinium intravenous contrast.
FIGURE 1. Patient with fulminatehepatic failure and meningitis pre-senting with seizures. A, Axial T1WIpost contrast shows that there isnot any important leptomeningealenhancement. B, Axial FLAIR dem-onstrating hyperintensity of the CSFspace (arrow). C, Axial DWI showspus in the high convexity CSF spacesand restricted diffusion in the adja-cent cortex, probably due to cere-britis (arrows).
146 q 2005 Lippincott Williams & Wilkins
Ferreira et al Top Magn Reson Imaging � Volume 16, Number 2, April 2005
Initial clinical evaluations of FLAIR post contrast weredone for intraparenchymal lesions and, after that, someauthors19 have described that post-contrast FLAIR imaging ismore sensitive for detecting SAS diseases than T1WI postgadolinium. At the moment this point is controversial, withsome authors affirming that post-contrast FLAIR is better thanT1WI19 and vice versa.15,16
The opinion of the authors is that both have advantagesand disadvantages and both should be performed in individualpatients (Figs. 4 and 5).
For those that defend the post-contrast FLAIR the mainadvantages are:
Postcontrast FLAIR images do not show contrast enhancementin vessels with slow-flowing blood. This finding isobserved on T1-weighted post-contrast images and canbe confused with meningeal enhancement.
FLAIR has a higher sensibility compared to T1 weight todetect low concentrations of gadolinium extravasationsfrom pial vessels in the SAS.11,19–21
As stated earlier, the imaging findings of meningealinfectious disease is unspecific and the interpretations mustbe made in association with clinical settings and physicalsigns.
FOCAL PYOGENIC INFECTIONS(CEREBRITIS AND ABSCESS)
Abscess is the most common focal infectious lesion ofthe brain and frequently arises secondary to hematogenousdissemination, by direct inoculation (trauma or surgery), bycontiguous dissemination from an extracranial site or com-plicating a meningitis.12
Pathologically the process begins with the arrival ofbacteria to the gray or white matter and is followed by mi-gration of inflammatory cells leading to vascular congestion,increased capillary permeability, perivascular exudates, pete-quial hemorrhage, and microthrombosis. Later on occurperifocal edema, necrosis, and mass effect (early cerebritis).In later cerebritis phase, the necrotic zone coalesces, and thelesion becomes circumscribed. Early abscess phase occurswith organization of the granulation tissue peripherally, leading tothe formation of collagenous capsule, within approximatelyweeks, which results in reduction of circumjacent edema andliquefaction of the necrotic center. Finally, in the late abscessphase, the capsule thickens and sometimes calcifies. Witheffective treatment, the central cavity may involute, and the
FIGURE 3. A, Axial FLAIR. Notice the marked subcorticalhypointensity in the right frontal lobe, suggesting leptome-ningeal/SAS abnormality (arrows), confirmed by the post-contrast T1WI axial image (arrow in B).
FIGURE 2. Patient with clinical history of trauma and subdural hematoma. A, Axial FLAIR imaging without contrast demonstratingsuch lesion (arrow). B, Axial post-contrast T1WI shows no enhancement of this hematoma (arrow). C, Post-contrast axial flairshowing enhancement of this space due to contrast leakage (arrow).
q 2005 Lippincott Williams & Wilkins 147
Top Magn Reson Imaging � Volume 16, Number 2, April 2005 Imaging Aspects of Pyogenic Infections of CNS
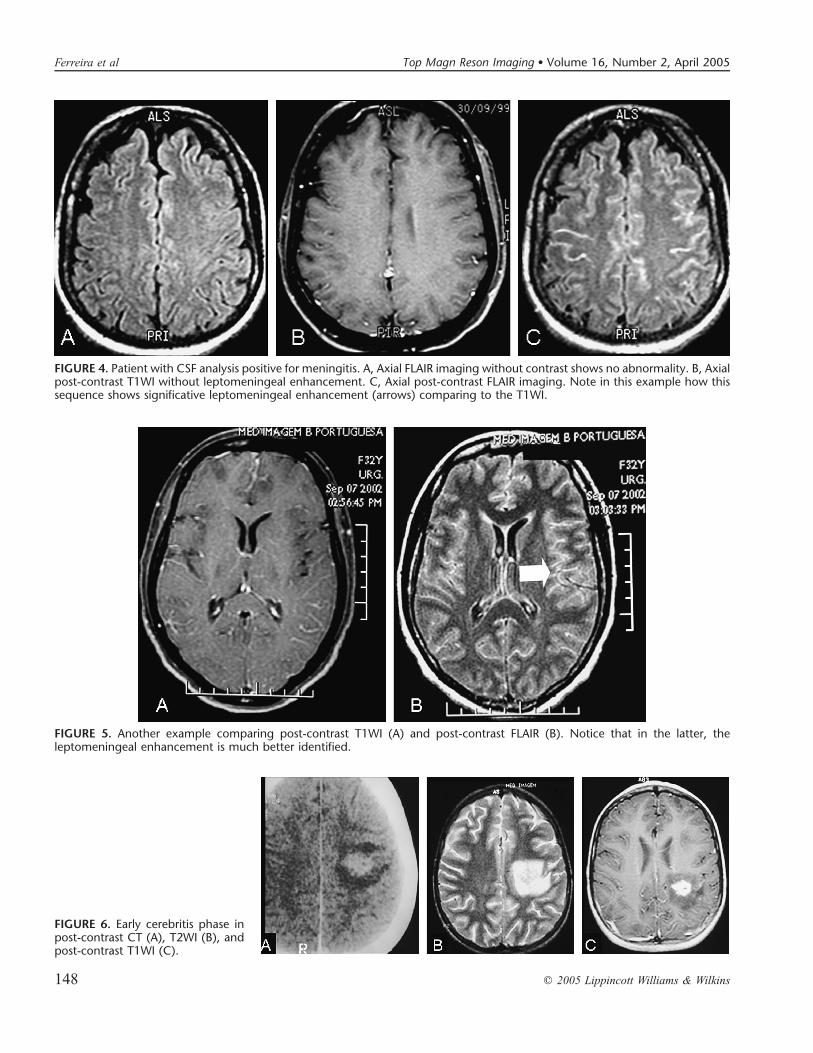
FIGURE 5. Another example comparing post-contrast T1WI (A) and post-contrast FLAIR (B). Notice that in the latter, theleptomeningeal enhancement is much better identified.
FIGURE 4. Patient with CSF analysis positive for meningitis. A, Axial FLAIR imaging without contrast shows no abnormality. B, Axialpost-contrast T1WI without leptomeningeal enhancement. C, Axial post-contrast FLAIR imaging. Note in this example how thissequence shows significative leptomeningeal enhancement (arrows) comparing to the T1WI.
FIGURE 6. Early cerebritis phase inpost-contrast CT (A), T2WI (B), andpost-contrast T1WI (C).
148 q 2005 Lippincott Williams & Wilkins
Ferreira et al Top Magn Reson Imaging � Volume 16, Number 2, April 2005
residual collapsed fibrotic capsule may remain indefinitely.Without treatment, the cavity may grow and the most seriouscomplication, including compartmental herniation and intra-ventricular rupture, may occur.3,22
Otitis media and mastoiditis are the most common originof cerebellar abscesses that constitute 2% to 14% of all brainabscesses. Chronic infections of the face and scalp, partic-ularly frontal sinusitis, may cause cerebritis or abscess in thefrontal lobe, which is the most common place of occurrence offocal infection. Due to these reasons, on encountering an ab-scess on imaging study it is important to search for a localcause, such as mastoiditis, otitis, sinusitis, or ectodermal defects.7
Patients may present with headache, nausea, ataxia, andpapilledema owing to increased intracranial pressure. Con-comitant fever, mental states changes, or focal neurologicdeficits are present in half of individuals. Seizures, visual, andspeech disturbances are less common manifestations.3
ROLE OF IMAGINGImaging diagnosis plays an important role in focal
pyogenic brain involvement. The advent of CT and MRimaging has allowed timely diagnosis and decreasing ofthe mortality rate.23 The imaging findings vary according tothe phase of the lesion and can be arbitrarily divided, for thebenefit of comprehension, into four phases.
Early Cerebritis PhaseThis phase is rarely imaged, and occurs between the
third to fifth days.24 CT demonstrates low attenuation, ill-defined area with subtle mass effect (Fig. 6). MR images offerhigher sensitivity for detection of the lesions than CTand showa hyperintense T2 weight and FLAIR lesion indistinguishableof edema and have isointense or hypointense T1-weightedsignal.25 In cerebritis there is no purulent fluid and the keydiagnostic sequence is the DWI. In this sequence there ismarked diffusion restriction, depicted by high signal (thatturns to low signal in apparent diffusion coefficients maps),which might be attributed to hypercellularity from abundantinfiltration of inflammatory cells, brain ischemia, or cytotoxicedema (Fig. 7).26 Contrast enhancement is minimal or absent.3
Late Cerebritis PhaseThis phase develops during the second week.24 The CT
is able to show that the central area becomes more hypodense,
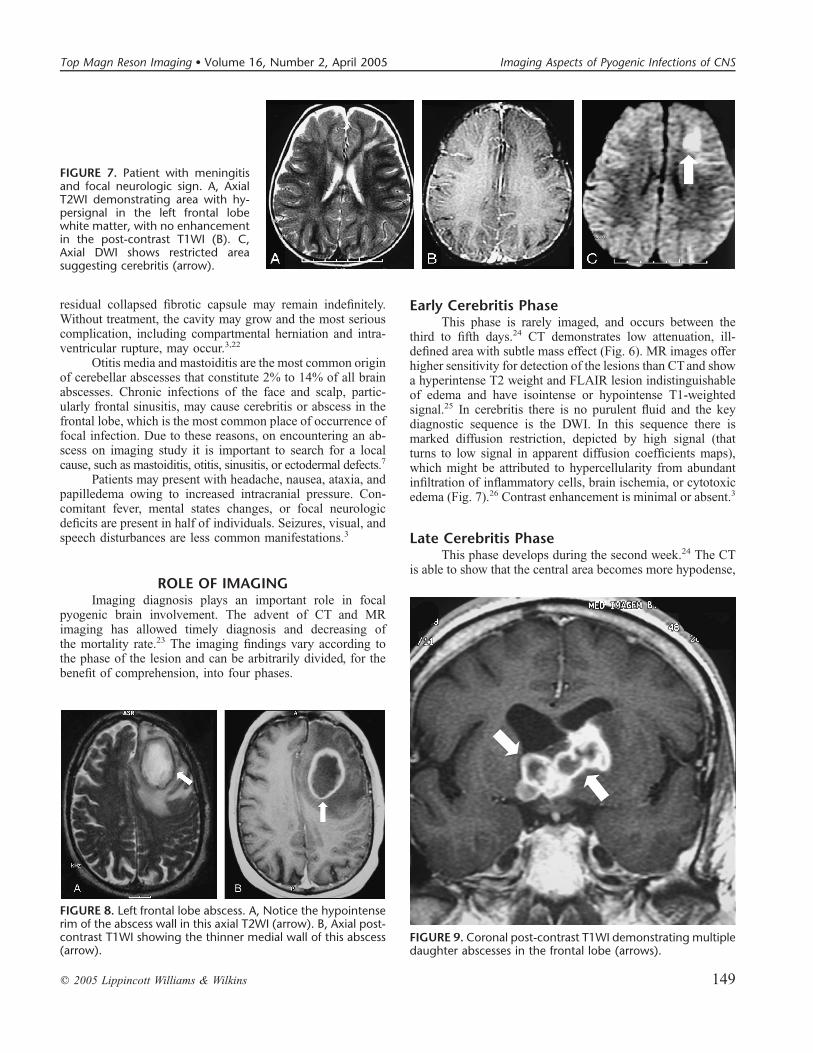
FIGURE 8. Left frontal lobe abscess. A, Notice the hypointenserim of the abscess wall in this axial T2WI (arrow). B, Axial post-contrast T1WI showing the thinner medial wall of this abscess(arrow).
FIGURE 9. Coronal post-contrast T1WI demonstrating multipledaughter abscesses in the frontal lobe (arrows).
FIGURE 7. Patient with meningitisand focal neurologic sign. A, AxialT2WI demonstrating area with hy-persignal in the left frontal lobewhite matter, with no enhancementin the post-contrast T1WI (B). C,Axial DWI shows restricted areasuggesting cerebritis (arrow).
q 2005 Lippincott Williams & Wilkins 149
Top Magn Reson Imaging � Volume 16, Number 2, April 2005 Imaging Aspects of Pyogenic Infections of CNS
due to necrosis, and continues to progress. The same aspectsare observed on T1WI, but the periphery may demonstrate anisointense or slight hyperintense rim. On T2WI the rim isisointense or hypointense and the central area is hyperintense;peripherally to the rim is noted hyperintense vasogenic area ofedema, (target lesion). The central area of necrosis hasrestricted water diffusion. After contrast administration, theenhancement is diffuse or nodular, progressing to thick,irregular-enhancing rim, according to the evolution of thecentral necrosis.3
Early Abscess PhaseClose to the second week,24 the capsule formation is
complete. CT demonstrates more demarcated isodense capsuleor slight hyperdense margin, interposed between the hypo-dense central area of necrosis and hypodense circumjacentedema. In relation to later cerebritis phase, MR demonstratesmore defined margins that are marked hypointense on T2WI,probably due to collagen or paramagnetic free radicals withinmacrophages and less probably due to hemorrhage, that willhave hyperintensity on T1 weight image and hypointensity onGradient-Echo images due to susceptibility effects of oxyhe-moglobin and ferritin/haemosiderin.3,27 The capsule of abscessin this phase may be less developed on its ventricular side thanon its cortical side, probably related to perfusion differencesbetween these areas (Fig. 8). The circumjacent edema reducesin relation to the cerebritis phase and the restriction to waterdiffusion persists. The postcontrast images reveal intense andwell-defined enhancement of the capsule. Daughter abscess(Fig. 9) becomes apparent in this phase.8 With the progressionof the abscess, the capsule becomes smoothest and thinnestwith edema reduction.
Later Abscess PhaseThis phase develops after the second week and may
persist for months.24 The central necrotic cavity decreases insize and the capsule looses the hypointensity on T2-weightedimages, unless calcification is present. Enhancement may per-sist and progressively decreases. Hypointense remnants of thecapsule may persist for years after resolution of the infection.3
DIFFERENTIAL DIAGNOSIS WITH OTHER RINGENHANCING LESIONS
Frequently, with conventional techniques, the imagingcharacteristics alone may not clearly distinguish a cerebral
abscess from other ring enhancing lesions, as for instancecystic/necrotic primary or secondary tumor, a resolving hema-toma or postoperative change. For this purpose we can use newtechniques, such as proton brain spectroscopy, DWI, and PWIin a tentative attempt to establish the correct diagnoses non-invasively.12
DIFFUSION WEIGHTED IMAGINGDiffusion weighted imaging (DWI) plays an important
role to differentiate pyogenic abscess from other ring en-hancing lesions. It is important to know that the pyogenicabscess has restricted diffusion as a main characteristic and itis the easiest way to diagnose this pathology. The reason forthis restriction, however, is poorly understood. For some authors,it might reflect high viscosity of inflammatory cells, but it is
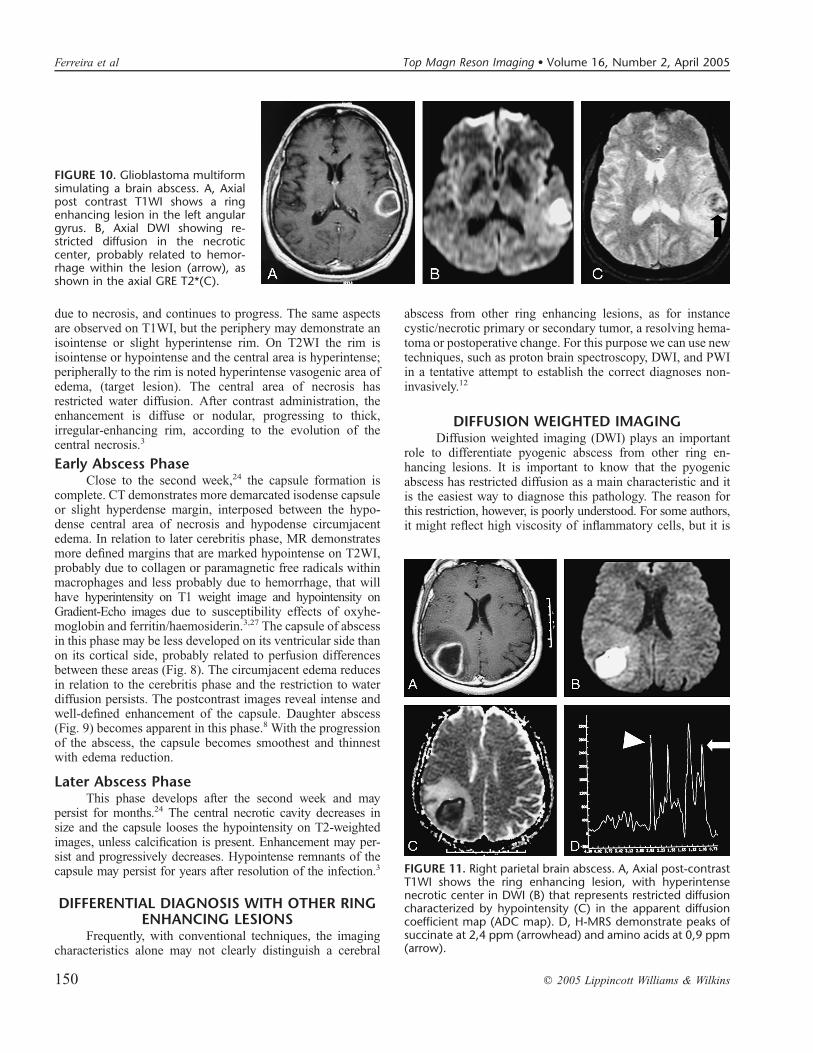
FIGURE 10. Glioblastoma multiformsimulating a brain abscess. A, Axialpost contrast T1WI shows a ringenhancing lesion in the left angulargyrus. B, Axial DWI showing re-stricted diffusion in the necroticcenter, probably related to hemor-rhage within the lesion (arrow), asshown in the axial GRE T2*(C).
FIGURE 11. Right parietal brain abscess. A, Axial post-contrastT1WI shows the ring enhancing lesion, with hyperintensenecrotic center in DWI (B) that represents restricted diffusioncharacterized by hypointensity (C) in the apparent diffusioncoefficient map (ADC map). D, H-MRS demonstrate peaks ofsuccinate at 2,4 ppm (arrowhead) and amino acids at 0,9 ppm(arrow).
150 q 2005 Lippincott Williams & Wilkins
Ferreira et al Top Magn Reson Imaging � Volume 16, Number 2, April 2005
known that these conditions are not confined to abscess andmight be present in various other brain diseases28–31 likehemorrhagic primary (Fig. 10) or secondary tumors andresolving hematomas.
PROTON MAGNETICRESONANCE SPECTROSCOPY
The brain metabolites in pyogenic abscesses are dif-ferent from those found in normal brain and can help dif-ferentiate pyogenic brain abscesses from necrotic neoplasms.The predominant resonance peaks (N-acetylaspartate, choline,and creatine/phosphocreatine) that are usually observed in theparenchyma of the normal brain are hardly detectable in eithertumoral or abscess necrosis. Increases in lactate (1.3 ppm),acetate (1.92 ppm), and succinate (2.4 ppm) presumably orig-inate from the enhanced glycolysis and fermentation of theorganism. Amino acids, including valine and leucine (0.9ppm), are known to be the end products of proteolysis byenzymes released by neutrophils in pus (Fig. 11). Detection ofresonance peaks from acetate, succinate, and such amino acidsas valine and leucine has not been reported in proton MR
spectra of brain tumors. Discrimination between amino acids(ie, valine or leucine at 0.9 ppm) and lipid (at 0.8 to 1.2 ppm) isimportant, because lipid signals may exist in both brain tumorsand abscesses, whereas amino acids are not seen in proton MRspectra of brain tumors, suggesting that amino acids may bemarkers for brain abscesses. Therefore, if there are resonancepeaks at around 0.9 to 1.5 ppm on proton MR spectra obtainedwith an echo time of 270, an additional spectrum obtained atan echo time of 135 would be necessary to discriminate lactateor amino acids signals from lipid signal. It is known that withan echo time of 135, phase inversion occurs as a result of J-coupling in lactate and amino acids, but not in lipid.12,32–34 Ithas been reported that these spectral changes in brain abscessdisappear with effective antibiotic treatment, so the spectralmay be important to evaluate the treatment responses, and thespecificity of spectral is only valid for untreated infections.34
PERFUSION WEIGHTED IMAGING (PWI)More recently, some authors have reported the additional
information given by MRI perfusion with relative cerebralblood volume (rCBV) maps to distinguish abscess from otherring enhancement lesions. The utilization of perfusion to
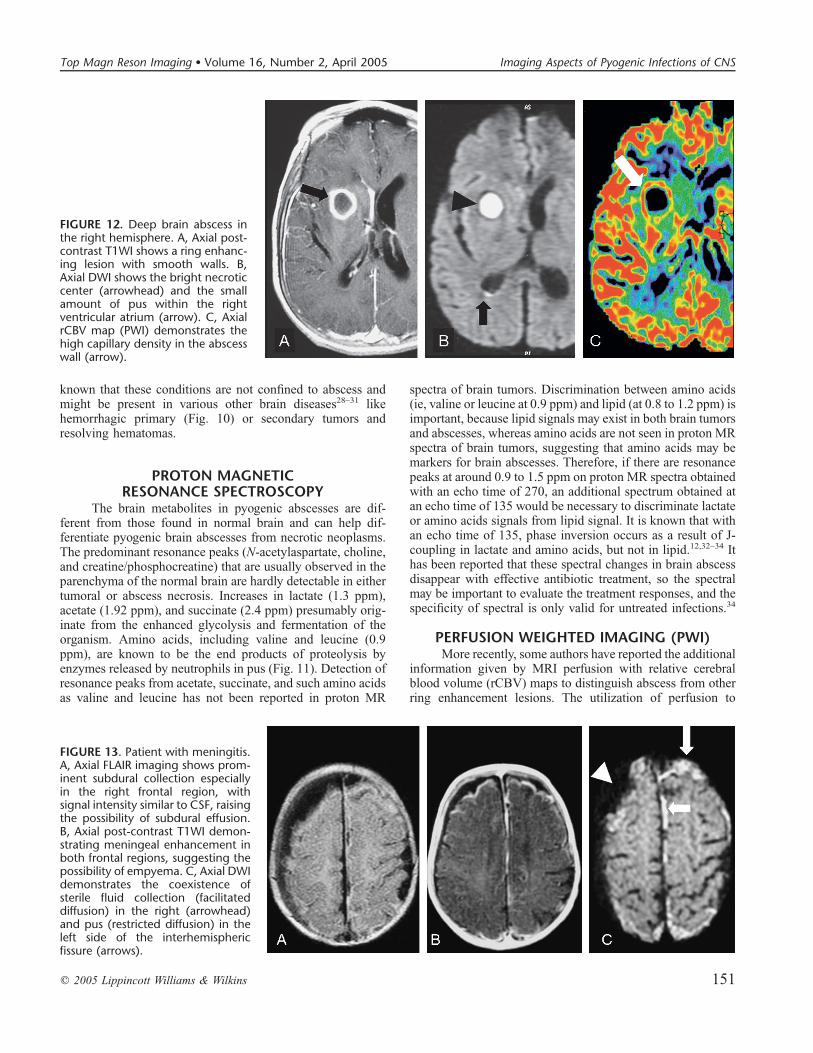
FIGURE 12. Deep brain abscess inthe right hemisphere. A, Axial post-contrast T1WI shows a ring enhanc-ing lesion with smooth walls. B,Axial DWI shows the bright necroticcenter (arrowhead) and the smallamount of pus within the rightventricular atrium (arrow). C, AxialrCBV map (PWI) demonstrates thehigh capillary density in the abscesswall (arrow).
FIGURE 13. Patient with meningitis.A, Axial FLAIR imaging shows prom-inent subdural collection especiallyin the right frontal region, withsignal intensity similar to CSF, raisingthe possibility of subdural effusion.B, Axial post-contrast T1WI demon-strating meningeal enhancement inboth frontal regions, suggesting thepossibility of empyema. C, Axial DWIdemonstrates the coexistence ofsterile fluid collection (facilitateddiffusion) in the right (arrowhead)and pus (restricted diffusion) in theleft side of the interhemisphericfissure (arrows).
q 2005 Lippincott Williams & Wilkins 151
Top Magn Reson Imaging � Volume 16, Number 2, April 2005 Imaging Aspects of Pyogenic Infections of CNS
distinguish low-grade from high-grade tumors has beenpreviously related with success. As low-grade tumors, abscessrim seems to have lower rCBV values than high-grade tumorsrim. In high-grade tumors the high rCBV values are probablydue to high capillary density of the neovascularity formation.The abscess collagen capsule theoretically is associated with
low capillary density and consecutively, low rCBV values.28 Inour anecdotal experience with perfusion in abscess, we havenoted that, in latter stages the abscess capsule might have highrCBV values, making the differential diagnoses (in individualpatients) with tumor impossible with this technique (Fig. 12).However further studies are requires to establish the perfusionrole in abscess.
EXTRA AXIAL FLUID AND PUS COLLECTIONSExtra axial fluid collections may occur in the subdural
and epidural spaces after meningitis. These collections can besterile fluids (effusions) or infected purulent fluids (empyema).Empyemas are uncommon collections frequently related tosinusitis, mastoiditis, infection secondary to previous crani-otomy, or post traumatic infection. Purulent meningitis in infantsis often related to both empyemas and subdural effusions.12
Subdural effusion is a collection secondary to irritationof the dura mater by infectious agents and its products orsecondary to subdural veins inflammation.
ROLE OF IMAGINGDifferentiating these situations (effusions and empyema)
is very important. In the former, CT and MR imaging dem-onstrate the same density and signal intensity of cerebrospinalfluid, and these collections generally do not require specific
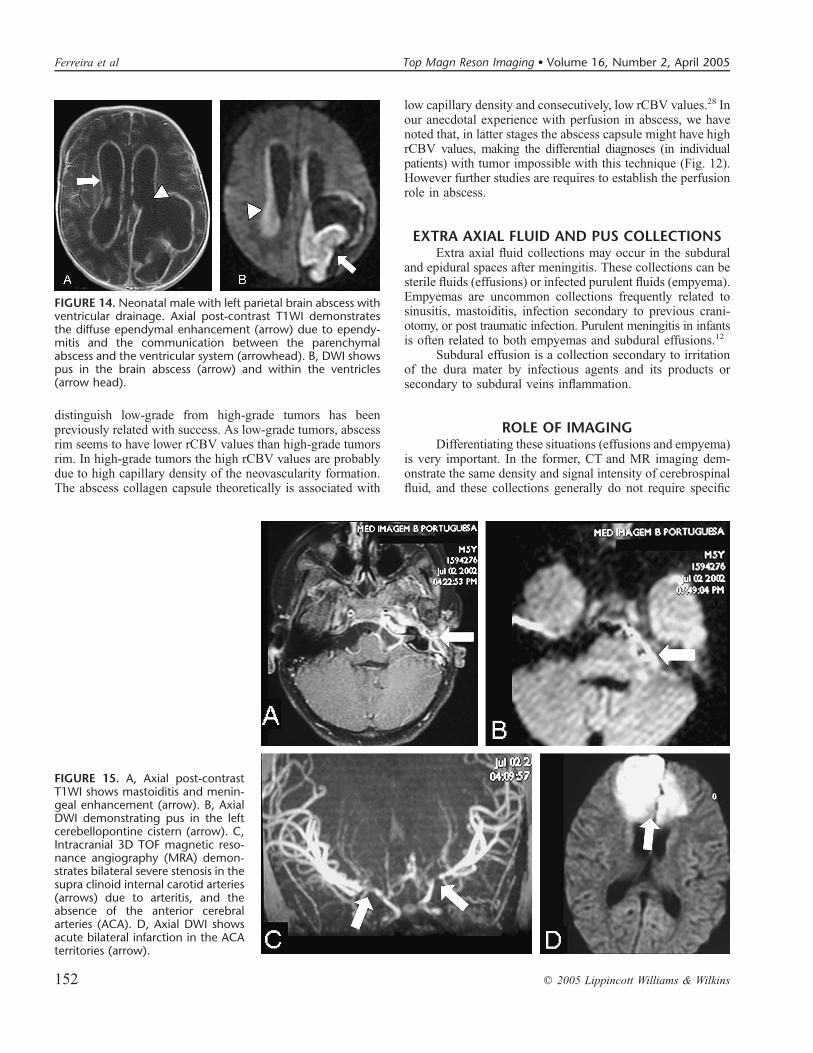
FIGURE 14. Neonatal male with left parietal brain abscess withventricular drainage. Axial post-contrast T1WI demonstratesthe diffuse ependymal enhancement (arrow) due to ependy-mitis and the communication between the parenchymalabscess and the ventricular system (arrowhead). B, DWI showspus in the brain abscess (arrow) and within the ventricles(arrow head).
FIGURE 15. A, Axial post-contrastT1WI shows mastoiditis and menin-geal enhancement (arrow). B, AxialDWI demonstrating pus in the leftcerebellopontine cistern (arrow). C,Intracranial 3D TOF magnetic reso-nance angiography (MRA) demon-strates bilateral severe stenosis in thesupra clinoid internal carotid arteries(arrows) due to arteritis, and theabsence of the anterior cerebralarteries (ACA). D, Axial DWI showsacute bilateral infarction in the ACAterritories (arrow).
152 q 2005 Lippincott Williams & Wilkins
Ferreira et al Top Magn Reson Imaging � Volume 16, Number 2, April 2005
treatment and resolve spontaneously after treatment of themeningitis.
Subdural empyema is usually secondary to retrogradethrombophlebitis via the calvarial emissary veins from anadjacent infection. Subdural empyema requires urgent neuro-surgical treatment and the antibiotic therapy alone is notsufficient.12 Earlier diagnoses are necessary because thesubdural empyemas may cause complications such asthrombophlebitis and cerebritis. CT demonstrates a lentiformcollection slightly denser than cerebrospinal fluid. MRI is themodality of choice to differentiate subdural empyema fromsubdural effusion. Subdural empyemas present higher con-centrations of proteins and demonstrate higher signal thancerebrospinal fluid in T1-weighted and FLAIR images. Afterintravenous contrast administration, the membranes ofempyemas enhance. More recently this differentiation hasbeen easily done with DWI, where, like in abscess, theempyema shows higher signal and low ADC values, and theeffusion has facilitated diffusion (Fig. 13).12
In epidural empyemas, the purulent collection islocalized outside the dura mater, protecting brain parenchymafrom complications. Thus, patients with epidural abscess havemore insidious and benign course. This prolonged courseexplains the low or mixed signal intensity that may be en-countered in diffusion weighted images12 because the pusbecomes less viscous. The signal in T1- and T2-weightedimages and the density in CT are the same of subduralempyemas, and the contrast administration shows a thickerdura mater enhancement.
VENTRICULITISVentriculitis is an uncommon but serious complication
of meningitis or rupture of brain abscess into the ventricularsystem. CT shows ventricular enhancement after intravenouscontrast administration. MRI also shows this enhancement anddemonstrates, especially on FLAIR and DWI, increased signalof pus into the ventricular system. Ventriculomegaly is oftenpresent (Fig. 14). The most common finding in MRI is thepresence of ‘‘debris’’, and the best sequence and place to lookfor small amount of pus are respectively diffusion and theoccipital horn of the lateral ventricles.35
VASCULAR COMPLICATIONSCentral nervous system infarction associated with
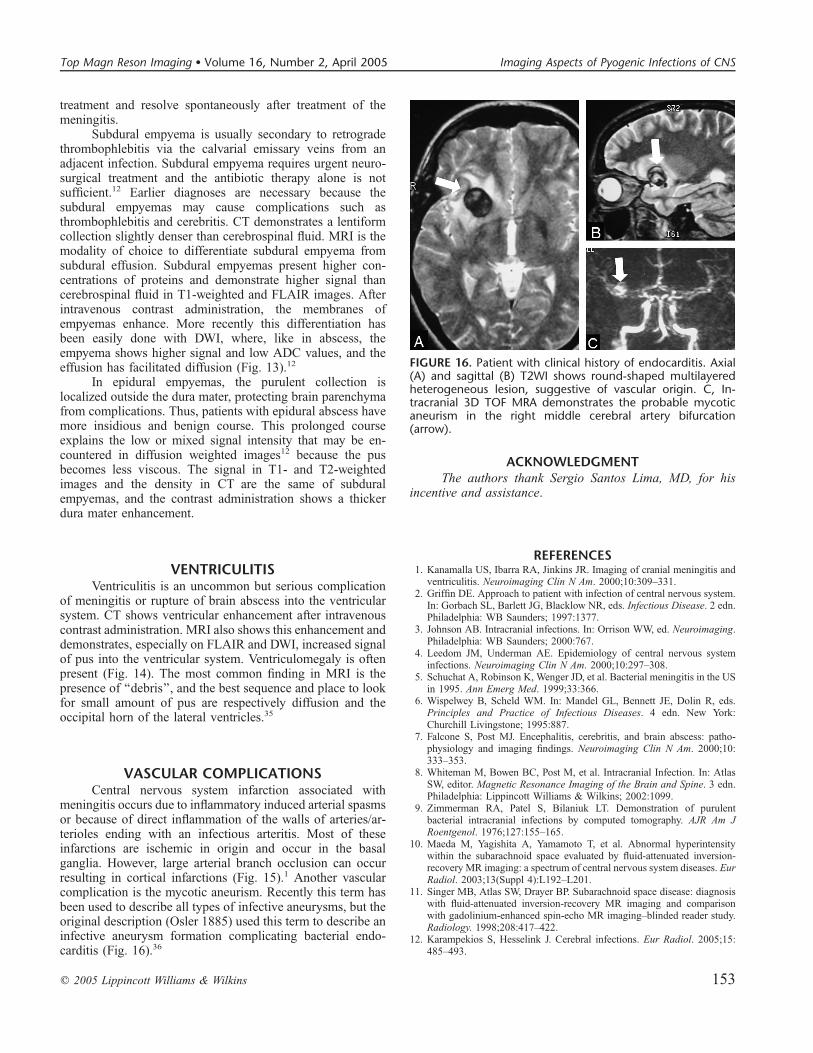
meningitis occurs due to inflammatory induced arterial spasmsor because of direct inflammation of the walls of arteries/ar-terioles ending with an infectious arteritis. Most of theseinfarctions are ischemic in origin and occur in the basalganglia. However, large arterial branch occlusion can occurresulting in cortical infarctions (Fig. 15).1 Another vascularcomplication is the mycotic aneurism. Recently this term hasbeen used to describe all types of infective aneurysms, but theoriginal description (Osler 1885) used this term to describe aninfective aneurysm formation complicating bacterial endo-carditis (Fig. 16).36
ACKNOWLEDGMENTThe authors thank Sergio Santos Lima, MD, for his
incentive and assistance.
REFERENCES1. Kanamalla US, Ibarra RA, Jinkins JR. Imaging of cranial meningitis and
ventriculitis. Neuroimaging Clin N Am. 2000;10:309–331.2. Griffin DE. Approach to patient with infection of central nervous system.
In: Gorbach SL, Barlett JG, Blacklow NR, eds. Infectious Disease. 2 edn.Philadelphia: WB Saunders; 1997:1377.
3. Johnson AB. Intracranial infections. In: Orrison WW, ed. Neuroimaging.Philadelphia: WB Saunders; 2000:767.
4. Leedom JM, Underman AE. Epidemiology of central nervous systeminfections. Neuroimaging Clin N Am. 2000;10:297–308.
5. Schuchat A, Robinson K, Wenger JD, et al. Bacterial meningitis in the USin 1995. Ann Emerg Med. 1999;33:366.
6. Wispelwey B, Scheld WM. In: Mandel GL, Bennett JE, Dolin R, eds.Principles and Practice of Infectious Diseases. 4 edn. New York:Churchill Livingstone; 1995:887.
7. Falcone S, Post MJ. Encephalitis, cerebritis, and brain abscess: patho-physiology and imaging findings. Neuroimaging Clin N Am. 2000;10:333–353.
8. Whiteman M, Bowen BC, Post M, et al. Intracranial Infection. In: AtlasSW, editor. Magnetic Resonance Imaging of the Brain and Spine. 3 edn.Philadelphia: Lippincott Williams & Wilkins; 2002:1099.
9. Zimmerman RA, Patel S, Bilaniuk LT. Demonstration of purulentbacterial intracranial infections by computed tomography. AJR Am JRoentgenol. 1976;127:155–165.
10. Maeda M, Yagishita A, Yamamoto T, et al. Abnormal hyperintensitywithin the subarachnoid space evaluated by fluid-attenuated inversion-recovery MR imaging: a spectrum of central nervous system diseases. EurRadiol. 2003;13(Suppl 4):L192–L201.
11. Singer MB, Atlas SW, Drayer BP. Subarachnoid space disease: diagnosiswith fluid-attenuated inversion-recovery MR imaging and comparisonwith gadolinium-enhanced spin-echo MR imaging–blinded reader study.Radiology. 1998;208:417–422.
12. Karampekios S, Hesselink J. Cerebral infections. Eur Radiol. 2005;15:485–493.
FIGURE 16. Patient with clinical history of endocarditis. Axial(A) and sagittal (B) T2WI shows round-shaped multilayeredheterogeneous lesion, suggestive of vascular origin. C, In-tracranial 3D TOF MRA demonstrates the probable mycoticaneurism in the right middle cerebral artery bifurcation(arrow).
q 2005 Lippincott Williams & Wilkins 153
Top Magn Reson Imaging � Volume 16, Number 2, April 2005 Imaging Aspects of Pyogenic Infections of CNS

13. Chang KH, Han MH, Roh JK, et al. Gd-DTPA-enhanced MR imaging ofthe brain in patients with meningitis: comparison with CT. AJNR Am JNeuroradiol. 1990;11:69–76.
14. Ginsberg LE. Contrast enhancement in meningeal and extra-axial disease.Neuroimaging Clin N Am. 1994;4:133–152.
15. Kamran S, Bener AB, Alper D, et al. Role of fluid-attenuated inversionrecovery in the diagnosis of meningitis: comparison with contrast-enhanced magnetic resonance imaging. J Comput Assist Tomogr. 2004;28:68–72.
16. Galassi W, Phuttharak W, Hesselink JR, et al. Intracranial meningealdisease: comparison of contrast-enhanced MR imaging with fluid-attenuated inversion recovery and fat-suppressed T1-weighted sequences.AJNR Am J Neuroradiol. 2005;26:553–559.
17. Taoka T, Yuh WT, White ML, et al. Sulcal hyperintensity on fluid-attenuated inversion recovery MR images in patients without apparentcerebrospinal fluid abnormality. AJR Am J Roentgenol. 2001;176:519–524.
18. Lee JH, Na DG, Choi KH, et al. Subcortical low intensity on MR imagesof meningitis, viral encephalitis, and leptomeningeal metastasis. AJNR AmJ Neuroradiol. 2002;23:535–542.
19. Mathews VP, Caldemeyer KS, Lowe MJ, et al. Brain: gadolinium-enhanced fast fluid-attenuated inversion-recovery MR imaging. Radiol-ogy. 1999;211:257–263.
20. Mamourian AC, Hoopes PJ, Lewis LD. Visualization of intravenouslyadministered contrast material in the CSF on fluid-attenuated inversion-recovery MR images: an in vitro and animal-model investigation. AJNRAm J Neuroradiol. 2000;21:105–111.
21. Jackson EF, Hayman LA. Meningeal enhancement on fast FLAIR images.Radiology. 2000;215:922–924.
22. Kamra P, Vatsal DK, Husain M, et al. MRI demonstration of unsuspectedintraventricular rupture of pyogenic cerebral abscesses in patients beingtreated for meningitis. Neuroradiology. 2002;44:114–117.
23. Rana S, Albayram S, Lin DD, et al. Diffusion-weighted imaging andapparent diffusion coefficient maps in a case of intracerebral abscess withventricular extension. AJNR Am J Neuroradiol. 2002;23:109–112.
24. Salzman KL. Meningitis. In: Osborn AG, ed. Diagnostic Imaging—Brain.Salt Lake City: Amirsys; 2004:I-8-24.
25. Zimmenrman RA, Bilaniuk LT, Sze G. Intracranial Infection. In:Zanawadski B ND, ed. Magnetic Resonance Imaging of Central NervousSystem. New York: Raven Press; 1987:235.
26. Tung GA, Rogg JM. Diffusion-weighted imaging of cerebritis. AJNR AmJ Neuroradiol. 2003;24:1110–1113.
27. Sudhakar KV, Agrawal S, Rashid MR, et al. MRI demonstration ofhaemorrhage in the wall of a brain abscess: possible implications fordiagnosis and management. Neuroradiology. 2001;43:218–222.
28. Holmes TM, Petrella JR, Provenzale JM. Distinction between cerebralabscesses and high-grade neoplasms by dynamic susceptibility contrastperfusion MRI. AJR Am J Roentgenol. 2004;183:1247–1252.
29. Guo AC, Provenzale JM, Cruz LC Jr, et al. Cerebral abscesses:investigation using apparent diffusion coefficient maps. Neuroradiology.2001;43:370–374.
30. Camacho DL, Smith JK, Castillo M. Differentiation of toxoplasmosis andlymphoma in AIDS patients by using apparent diffusion coefficients.AJNR Am J Neuroradiol. 2003;24:633–637.
31. Hartmann M, Jansen O, Heiland S, et al. Restricted diffusion within ringenhancement is not pathognomonic for brain abscess. AJNR Am JNeuroradiol. 2001;22:1738–1742.
32. Chang KH, Song IC, Kim SH, et al. In vivo single-voxel proton MRspectroscopy in intracranial cystic masses. AJNR Am J Neuroradiol. 1998;19:401–405.
33. Lai PH, Li KT, Hsu SS, et al. Pyogenic brain abscess: findings fromin vivo 1.5-T and 11.7-T in vitro proton MR spectroscopy. AJNR Am JNeuroradiol. 2005;26:279–288.
34. Burtscher IM, Holtas S. In vivo proton MR spectroscopy of untreatedand treated brain abscesses. AJNR Am J Neuroradiol. 1999;20:1049–1053.
35. Fukui MB, Williams RL, Mudigonda S. CT and MR imaging features ofpyogenic ventriculitis. AJNR Am J Neuroradiol. 2001;22:1510–1516.
36. Cloud GC, Rich PM, Markus HS. Serial MRI of a mycotic aneurysm ofthe cavernous carotid artery. Neuroradiology. 2003;45:546–549.
154 q 2005 Lippincott Williams & Wilkins
Ferreira et al Top Magn Reson Imaging � Volume 16, Number 2, April 2005

![Annals of Clinical Case Reports Case Report - anncaserep.com · pyogenic granuloma was described [5]. The Term Pyogenic granuloma is a misnomer because the The Term Pyogenic granuloma](https://img.pdfslide.net/doc/110x75/5d0a41bb88c993cf0c8b7f5f/annals-of-clinical-case-reports-case-report-pyogenic-granuloma-was-described.jpg)


























