Embed Size (px)
DESCRIPTION
Imatinib
Citation preview

Authors’ Disclosures of Potential Conflicts of Interest
Although all authors completed the disclosure declaration, the following authors or their immediate family membersindicated a financial interest. No conflict exists for drugs or devices used in a study if they are not being evaluated as part of theinvestigation. For a detailed description of the disclosure categories, or for more information about ASCO’s conflict of interestpolicy, please refer to the Author Disclosure Declaration and the Disclosures of Potential Conflicts of Interest section inInformation for Contributors.
Authors Employment Leadership Consultant Stock Honoraria Research Funds Testimony Other
T.G. Eisen Eli Lilly (A) Eli Lilly (A)
P.G. Harper Eli Lilly (A) Eli Lilly (A)
W.M.C. Martin Lilly (A)
Dollar Amount Codes (A) � $10,000 (B) $10,000-99,999 (C) � $100,000 (N/R) Not Required
REFERENCES1. Rudd RM, Gower NH, Spiro SG, et al: Gemcitabine plus carboplatin
versus mitomycin, ifosfamide, and cisplatin in patients with stage IIIB or IVnon-small-cell lung cancer: A phase III randomized study of the London LungCancer Group. J Clin Oncol 23:142-153, 2005
2. Cullen MH, Joshi R, Chetiyawardana AD, et al: Mitomycin, ifosfamideand cisplatin in non-small cell lung cancer: Treatment good enough tocompare. Br J Cancer 58:359-361, 1988
3. Cullen MH, Billingham LJ, Woodroffe CM, et al: Mitomycin, ifos-famide, and cisplatin in unresectable non-small-cell lung cancer: Effects onsurvival and quality of life. J Clin Oncol 17:3188-3194, 1999
4. Sculier JP, Paesmans M, Lafitte JJ, et al: A randomised phase III trialcomparing consolidation treatment with further chemotherapy to chestirradiation in patients with initially unresectable locoregional non-small-celllung cancer responding to induction chemotherapy: European Lung CancerWorking Party. Ann Oncol 10:295-303, 1999
5. Sculier JP, Lafitte JJ, Paesmans M, et al: Phase III randomized trialcomparing moderate-dose cisplatin to combined cisplatin and carboplatin inaddition to mitomycin and ifosfamide in patients with stage IV non-small-celllung cancer. Br J Cancer 83:1128-1135, 2000
6. Sculier JP, Lafitte JJ, Berghmans T, et al: A phase III randomised studycomparing two different dose-intensity regimens as induction chemother-apy followed by thoracic irradiation in patients with advanced locoregionalnon-small-cell lung cancer. Ann Oncol 15:399-409, 2004
DOI: 10.1200/JCO.2005.01.7640
Imatinib Mesylate Can InduceObjective Response in Progressing,Highly Expressing KIT AdenoidCystic Carcinoma of theSalivary Glands
TO THE EDITOR: KIT expression appears as a commonfeature in 80% to 100% of adenoid cystic carcinoma of thesalivary glands arising from the head and neck.1-3 Imatinibmesylate to prevent the activation of KIT has been recentlyreported by Hotte et al as having limited or no activity in amulticenter phase II trial in 15 patients with unresectable ormetastatic salivary adenoid cystic carcinoma.4
We are currently conducting a multicenter phase IItrial in patients with recurrent or metastatic adenoid cysticcarcinoma strongly overexpressing KIT using CD117 im-
munohistochemistry (50% to 100% staining in tumorcells). In our study, patients were required to display docu-mented tumor progression on two consecutive computedtomography and/or magnetic resonance imaging scans per-formed 3 to 4 months apart before study entry and to haveat least one measurable target lesion � 2 cm. Imatinibmesylate was administered at 400 mg orally bid (800 mg/d).The primary end point of our study is the assessment oftime to tumor progression given the low proliferative frac-tion characterizing this disease making the observation ofobjective tumor shrinkage with any previously used anti-cancer agent unusual.
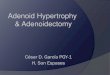
To date, eight patients (one male, seven females) haveentered the study. Target lesions were pulmonary metasta-sis in all patients, with one patient also displaying locore-gional recurrence. Median age was 45 years (range, 37 to71), performance status was 0 in seven patients and 1 in onepatient. Previous treatment with chemotherapy was re-ported in four patients. Toxicity was mild to moderate in allbut one patient, who presented grade 3 neutropenia andanemia requiring transfusion and dose reduction, and an-other who experienced severe fatigue requiring treatmentdiscontinuation. The latter patient, who was withdrawnearly on for toxicity, was not assessable for efficacy. Amongsix assessable patients, three patients were stable after 3months of treatment and one patient displayed a partialresponse of 42% according to the Response EvaluationCriteria in Solid Tumors Group criteria. This response wasobserved in a 41-year old woman who previously receivedcisplatin-FU combination with no objective response. Base-line grade 1 dyspnea completely resolved within the firsttwo months of treatment. This clinical benefit correlatedwith a significant improvement in imaging as measured by acomputed tomography scan performed after 3 months oftreatment showing objective response on multiple pulmo-nary target lesions (Fig 1). The patient is still under treat-ment at 800 mg/d.
Results of the study by Hotte et al recently published inthe Journal of Clinical Oncology have appeared rather dis-appointing with no evidence of objective response among15 treated patients.4 Based on their results, the authors
Correspondence
www.jco.org 6271
67.99.175.226Information downloaded from jco.ascopubs.org and provided by at ROSWELL PARK CANCER INST on March 4, 2015 from
Copyright © 2005 American Society of Clinical Oncology. All rights reserved.

conclude that evaluation of imatinib mesylate is no longerwarranted in this population. However, based on encour-aging preliminary results in our phase II trial and otherrecent case reports,5 we would like to modulate this state-ment and suggest that imatimib mesylate may have, at leastin a limited subset of patients, antitumor activity in adenoidcystic carcinoma. Interestingly, responses have been re-ported both in irradiated areas and in patients failing priortherapy with platinum.5
The natural history of this disease appears to be associ-ated with a prolonged chronic phase during which theproliferation index as measured by flow cytometry in ourexperience was lower than 1%. A switch phase with acceler-ation of tumor progression is known to occur in mostadvanced disease. As physicians involved in early drug de-velopment trials, we usually require documented tumorprogression as an essential eligibility criteria. Hence, in ourtrial and few case reports of objective responses,5 patientshad clear documented tumor progression at study entry.Antitumor activity was preceded by early evidence of clini-cal benefit (disappearance of trismus, dysphagia or bleedingfor locoregional relapse,5 complete resolution of dyspneafor pulmonary metastasis in our experience) after a fewweeks of treatment. Therefore, discrepancies in results byHotte et al and others might be, at least in part, explained bythe nonrequirement for documented tumor progression at
baseline in the Hotte et al study, suggesting that most oftheir patients might have been treated during nonaccelera-tion phases of the disease. Therefore, the absence of cellularproliferation might have limited the potential of imatinibmesylate to induce tumor regression.
In addition, treatment parameters may also have im-pacted the likelihood of efficacy. In the study by Hotte et althe median duration of treatment was � 2 months, which ina nonaccelerated phase might have been insufficient tomaximize the duration of exposure and optimize the poten-tial benefit of treatment. In our study, the first tumor eval-uation was performed only after 3 months of treatment thatwas further maintained in the absence of tumor progres-sion. Response to imatinib mesylate is known to sometimesoccur only after several months of treatment and be pre-ceded by sustained tumor stabilization. This has beenobserved in gastrointestinal stromal tumors, and slow re-sponses according to Response Evaluation Criteria in SolidTumors Group criteria have been supported by the use ofpositron emission tomography scans showing evidence ofmetabolic inactivation of the tumor. Similar observationswere reported in patients with glioblastoma in whom re-sponses occurred sometime after 6 months of tumor stabi-lization.6 Thus, the median duration of treatment in thestudy by Hotte et al might be regarded as insufficient to
Fig 1. Baseline (A)-(C) and evidence ofobjective response (B)-(D) in a patient withmultiple pulmonary metastasis of an ade-noid cystic carcinoma after 3 months ofdaily oral 800 mg imatinib mesylate.
Correspondence
6272 JOURNAL OF CLINICAL ONCOLOGY
67.99.175.226Information downloaded from jco.ascopubs.org and provided by at ROSWELL PARK CANCER INST on March 4, 2015 from
Copyright © 2005 American Society of Clinical Oncology. All rights reserved.

draw definitive conclusions on imatinib mesylate efficacy inadenoid cystic carcinoma.
Finally, the level of KIT overexpression might play arole in imatinib mesylate sensitivity. Interestingly, a strongoverexpression of KIT by tumor cells was a prerequisite toenter our study. The above-described patient who re-sponded exhibited strong CD117 immunostaining. Con-versely, only four of 16 patients were reported to displaystrong KIT expression in the study by Hotte et al. In theabsence of overexpression and/or KIT mutations, responseto imatinib mesylate is likely to be low and might accountfor the absence of drug activity in the study by Hotte et al.We are currently investigating the type of KIT mutationharbored by our responding patient.
In summary, considering the few possible alternativesgiven to patients with recurrent or metastatic progressiveadenoid cystic carcinoma, we consider that, although spo-radic, evidence of antitumor activity deserves further clini-cal investigation. Translational research that could help toidentify patients who would respond to imatinib mesylate iswarranted before rejecting this drug for the treatment ofpatients with adenoid cystic carcinoma.
Sandrine Faivre, Eric Raymond, Odile Casiraghi,Stéphane Temam, and Patrice BerthaudBeaujon University Hospital, Clichy; Institut Gustave-Roussy, Villejuif;Novartis Pharma; France
■ ■ ■
Authors’ Disclosures of Potential Conflicts of Interest
Although all authors completed the disclosure declaration, the following author or immediate family members indicateda financial interest. No conflict exists for drugs or devices used in a study if they are not being evaluated as part of theinvestigation. For a detailed description of the disclosure categories, or for more information about ASCO’s conflict of interestpolicy, please refer to the Author Disclosure Declaration and the Disclosures of Potential Conflicts of Interest section inInformation for Contributors.
Authors Employment Leadership Consultant Stock Honoraria Research Funds Testimony Other
Patrice Berthaud Novartis Pharma
Dollar Amount Codes (A) � $10,000 (B) $10,000-99,999 (C) � $100,000 (N/R) Not Required
REFERENCES1. Holst VA, Marshall CE, Moskaluk CA, et al: KIT protein expression and
analysis of c-kit gene mutation in adenoid cystic carcinoma. Mod Pathol12:956-960, 1999
2. Jeng YM, Lin CY, Hsu HC: Expression of the c-kit protein is associatedwith certain subtypes of salivary gland carcinoma. Cancer Lett 154:107-111,2000
3. Edwards PC, Bhuiya T, Kelsch RD: C-kit expression in the salivary glandneoplasms adenoid cystic carcinoma, polymorphous low-grade adenocarci-noma, and monomorphic adenoma. Oral Surg Oral Med Oral Pathol OralRadiol Endod 95:586-593, 2003
4. Hotte SJ, Winquist EW, Lamont E, et al: Imatinib mesylate in patientswith adenoid cystic cancers of the salivary glands expressing c-kit: APrincess Margaret Hospital phase II consortium Study. J Clin Oncol 23:585-590, 2005
5. Alcedo JC, Fabrega JM, Arosemena JR, et al: Imatinib mesylate astreatment for adenoid cystic carcinoma of the salivary glands: Report of twosuccessfully treated cases. Head Neck 26:829-831, 2004
6. Raymond E, Brandes A, Van Oosterom A, et al. Multicentre phase IIstudy of imatinib mesylate in patients with recurrent glioblastoma: AnEORTC: NDDG/BTG Intergroup Study. Proc Am Assoc Clin Oncol 22:107s,2004 (abstr (1501)
DOI: 10.1200/JCO.2005.01.6055
IN REPLY: We would first like to congratulate Dr Faivreand colleagues for conducting their innovative and interest-ing study, and we thank them for sharing their preliminarydata. We will address their concerns related to our study1
and its conclusions.Faivre et al state that one objective response has been
seen on their study, and that at least two other responseshave been observed by others and published as a case re-port.2 Although promising, the response seen in the study
of Faivre et al has not yet been confirmed to our knowledge.Furthermore, the anecdotal responses observed in the casereport were not part of a study protocol and should beinterpreted with caution. Slevin et al recently published inabstract form their preliminary results of a phase II studywith imatinib mesylate and cisplatin in patients with ade-noid cystic carcinoma (ACC).3 One of 12 assessable patientshad a documented partial response, which may be attribut-able to the combination of agents, but may also have beensecondary to cisplatin alone. Our conclusion that imatinibmesylate did not warrant further evaluation in this patientpopulation was not based on the premise that the agent hadno activity whatsoever. It was based on the finding that, atthe end of the first stage, the observed level of activity waslower than our predetermined assumption that imatinibmesylate would be worthy of further evaluation if the re-sponse rate was at least 5%.4 This was not observed in ourstudy, and early termination occurred after completion ofthe first stage. Faivre et al also postulate that the patientsenrolled in our study might have had limited potential torespond to imatinib mesylate because some of them mayhave been entered during a nonacceleration phase. Al-though interesting, we do not believe that this hypothesishas been supported by published scientific observations. Inactuality, studies have suggested that patients in an acceler-ated phase of any type of cancer may not respond as well tothese agents because of the development of multiple alter-native mechanisms of progression. An example of this is the
Correspondence
www.jco.org 6273
67.99.175.226Information downloaded from jco.ascopubs.org and provided by at ROSWELL PARK CANCER INST on March 4, 2015 from
Copyright © 2005 American Society of Clinical Oncology. All rights reserved.