Embed Size (px)
Citation preview

www.elsevier.com/locate/humpath
Cervical adenoid basal tumors comprised of adenoid basalepithelioma associated with various types of invasivecarcinoma: Clinicopathologic features, humanpapillomavirus DNA detection, and P16 expression
Anil V. Parwani MD, PhDa, Ann E. Smith Sehdev MDa,1, Robert J. Kurman MDa,b,Brigitte M. Ronnett MDa,b,*
aDepartment of Pathology, The Johns Hopkins University School of Medicine and Hospital, Baltimore, MD 21231, USAbDepartment of Gynecology and Obstetrics, The Johns Hopkins University School of Medicine and Hospital,
Baltimore, MD 21231, USA
Received 28 June 2004; accepted 25 August 2004
0046-8177/$ – see front matter D 2005
doi:10.1016/j.humpath.2004.08.015
Abbreviations: HPV, human papillom
* Corresponding author. Department
E-mail address: [email protected] Currently at Department of Patholo
Keywords:Adenoid basal tumor;
Adenoid basal carcinoma;
Cervical carcinoma;
Human papillomavirus
DNA;
p16 immunohisto-
chemistry
Summary Adenoid basal tumors are uncommon cervical lesions that some pathologists consider
invasive carcinomas but others consider bepitheliomasQ due to their low-grade histological appearance
and rarely documented malignant behavior. We report the clinicopathologic features of 10 tumors
comprised of both typical low-grade adenoid basal tumors (epitheliomas) intimately associated with
invasive carcinomas having infiltrative growth, increased cytological atypia and mitotic activity, and
various types of differentiation, including adenoid basal/squamous, pure squamous, adenoid cystic, and
small cell neuroendocrine. Tumors were evaluated for the presence of human papillomavirus (HPV)
DNA and immunohistochemical p16 expression. The patients in the study group ranged in age from 45
to 81 years (mean, 65 years). Most of the patients presented with abnormal cervicovaginal smears. The
initial diagnosis was made on specimens obtained by cervical biopsy, laser electrocautery excision
procedure (LEEP), or cone biopsy in 8 patients. Two 2 patients were incidentally diagnosed in
hysterectomy specimens. All 10 patients had squamous intraepithelial lesions (9 high-grade, 1 low-
grade). In all cases diagnosed in LEEP or cone biopsy specimens, the invasive carcinoma component
was present in the excisional specimen and extended to the margins. Seven patients diagnosed on
excisional or biopsy specimens who underwent hysterectomy had residual tumor in the cervix, ranging
from microscopic foci to deeply invasive. No lymph node metastases were identified in 4 patients who
were staged. Seven patients with follow-up were alive without evidence of disease after follow-up
intervals of 8 to 84 months (mean, 45 months; median, 29 months). One patient with a component of
small cell carcinoma died of other causes without evidence of disease at 18 months. HPV 16 DNAwas
detected in both the adenoid basal epithelioma and invasive carcinoma components in 9 tumors by in
Human Pathology (2005) 36, 82–90
Elsevier Inc. All rights reserved.
avirus; LEEP, laser electrocautery excision procedure; PCR, polymerase chain reaction.
of Pathology, Johns Hopkins Hospital, Weinberg Bldg., Room 2242, 401 N. Broadway, Baltimore, MD 21231.
(B.M. Ronnett).
gy, Good Samaritan Hospital, Portland, OR.

Cervical adenoid basal tumors 83
situ hybridization, and HPV 33 was detected by polymerase chain reaction in 1 tumor. All tumors
expressed p16 diffusely. Adenoid basal tumors are high-risk HPV-related tumors that can be comprised
of both a low-grade adenoid basal tumor, which can be designated as epithelioma, and invasive
carcinomas of various types. The invasive component is usually evident in the excisional biopsy
specimen, allowing for recognition of a tumor that needs further management.
D 2005 Elsevier Inc. All rights reserved.
1. Introduction
Adenoid basal tumors of the cervix have been designated
as badenoid basal carcinomasQ since their initial recognition,even though malignant behavior has rarely been observed
[1-8]. They are unusual cervical tumors composed of nests of
uniform cells displaying basaloid, squamous, and glandular
differentiation. The tumors are usually associated with
squamous intraepithelial lesions, most often high-grade.
Most affected patients are asymptomatic postmenopausal
women who are diagnosed during follow-up of an abnormal
cervicovaginal smear. Pure, typical tumors appear to behave
in a benign fashion, leading the authors of one study to
recommend the term badenoid basal epitheliomaQ rather thanadenoid basal carcinoma [9]. Although the cases described in
that report were not associated with other types of invasive
carcinomas (except for 1 case of a microinvasive squamous
carcinoma), some other reports have described adenoid basal
tumors associated with invasive carcinomas and carcinosar-
comas [3,4,10-12]. In the present study we describe the
clinicopathologic features of a series of adenoid basal tumors
composed of a typical low-grade adenoid basal component
(bepitheliomaQ) intimately associated with invasive carcino-
mas displaying one or more types of differentiation. We
investigate the relationship between the adenoid basal
epitheliomas and invasive carcinomas by assessing for the
presence of HPV DNA and p16 expression in both tumor
components. We then present a proposal to subclassify these
tumors into adenoid basal epitheliomas and carcinomas.
2. Materials and methods
This study was approved by the Johns Hopkins Institu-
tional Review Board. The files of the Gynecologic Pathology
Consultation Service and Surgical Pathology Division, The
Johns Hopkins Hospital were searched for cases designated
as adenoid basal carcinoma, adenoid basal tumor, adenoid
basal and squamous carcinoma, or adenoid basal epithelioma
for the period 1984 to 2004. Of 14 potential cases of low-
grade adenoid basal tumor associated with additional types
of invasive carcinoma, 10 retrievable cases (9 consultation
cases and 1 routine case) were identified. Typical low-grade
adenoid basal tumors (n = 19) were excluded from the study.
2.1. Immunohistochemistry for p16
Formalin-fixed, paraffin-embedded tissue sections were
used. Immunoperoxidase labeling was done with an
automated BioTek-Tech Mate 1000 Staining System (Ven-
tana/Biotek Solutions, Tucson, AZ) at room temperature
with anti-p16(INK4a) (MTM Laboratories AG, Heidelberg,
Germany) at a dilution of 1:500.
2.2. Human papillomavirus DNA detection byin situ hybridization
Formalin-fixed, paraffin-embedded tissue sections were
used. Biotin-labeled HPV probe solutions (Dako, Carpin-
teria, CA) were applied to individual sections. These
included a wide spectrum probe (cocktail of HPV 6, 11,
16, 18, 31, 33, 45, and 51) and separate type-specific probes
for HPV 16 and HPV 18. Detection of hybridized probe was
done by tyramide-catalyzed signal amplification using the
Genpoint kit (Dako). Chromogenic detection was performed
with diaminobenzidine/H2O2. Controls included tissue
sections positive for HPV wide spectrum, the HeLa cell
line for HPV 18, and the SiHa cell line for HPV 16. Biotin-
labeled plasmid probes served as negative controls in each
case. Cases with a discrete punctate reaction product
specifically in tumor cell nuclei were interpreted as positive.
2.3. HPV DNA detection by polymerasechain reaction
To further analyze the tumors for the presence of HPV,
polymerase chain reaction (PCR) for HPV DNA was
performed on those specimens that were negative by in situ
hybridization. Tissue sections were deparaffinized with
xylene and resuspended and digested with buffer containing
proteinase K. Amplifications were performed for betaglobin
and for HPVs by the Roche line blot method [13]. This
method uses biotinylated pooled primers for HPV and for
betaglobin amplification. The amplified products are
screened against more than 35 HPV probes and betaglobin
probes immobilized on an extended filter strip. Specimens
that are negative for betaglobin and HPV are consid-
ered unsatisfactory.
3. Results
3.1. Clinicopathologic features
The clinicopathologic features of the 10 cases are
summarized in Table 1. The patients ranged in age from
45 to 81 years (mean, 65 years). Most of the patients
presented with abnormal cervicovaginal smears. The initial

A.V. Parwani et al.84
diagnosis was made on an excisional biopsy specimens
obtained by laser electrocautery excision procedure (LEEP)
or cone biopsy in 6 patients and in biopsy specimens in 2
patients. In 2 patients, the tumors were incidentally
diagnosed in hysterectomy specimens removed for pelvic
relaxation and uterine prolapse. The overlying cervical
squamous mucosa demonstrated a squamous intraepithelial
Table 1 Clinicopathologic Features of Cervical Adenoid Basal Tumo
Case Age Cervicovaginal
smear findings
Diagnostic
specimen
Invasiv
1 70 ASCUS, AGUS LEEP Adenoi
carcino
2 71 Abnormal* Cone biopsy Adenoi
carcino
3 79 HSIL Cone biopsy Adenoi
carcino
neuroe
4 81 Abnormal* Cone biopsy Squam
adenoid
5 61 HSIL Biopsy Adenoi
carcino
6 65 HSIL Cone biopsy Microi
carcino
7 45 HSIL Biopsy Adenoi
carcino
8 64 NA Hysterectomy Squam
9 49 HSIL LEEP Adenoi
carcino
10 65 NA Hysterectomy Adenoi
carcino
Tumor size, cm
(maximum dimension /
maximum depth)
Treatment
1 1.2 /0.3 Radical hysterectomy,
lymphadenectomy
2 0.6 /0.4 Total abdominal
hysterectomy, BSO;
Radiation therapy
3 At least 0.8 /0.5 Radiation therapy
4 2.5 /1.4 Radical hysterectomy,
BSO, lymphadenectomy
5 1.0 /0.8 Total vaginal
hysterectomy, RSO
6 0.4 /0.2 Radical hysterectomy,
lymphadenectomy
7 3.3 /1.4 Total abdominal
hysterectomy, BSO,
lymphadenectomy;
Radiation therapy
8 1.0 /0.6 Hysterectomy
9 1.3 /1.3 Radical hysterectomy,
BSO, lymphadenectomy
10 1.6 /0.8 Total vaginal hysterectomy
Abbreviations: ASCUS, atypical squamous cells of undetermined significance; AG
squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion;
ND, not done; NA, not available; NED, no evidence of disease; DOC/NED, died
* Pap smear reported as abnormal, not further specified.
lesion in all cases (9 high-grade, 1 low-grade). Each tumor
was comprised of typical low-grade adenoid basal tumor
intimately associated with invasive carcinoma. The low-
grade adenoid basal tumor components were characterized
by discrete nests of tumor in which the surrounding stroma
lacked a desmoplastic reaction. The epithelial nests dis-
played varying combinations of basaloid, squamous, and
rs
e carcinoma type Intraepithelial lesion Margin status
on excision
d basal/squamous
ma
HSIL Positive
d basal/squamous
ma
HSIL Positive
d basal/squamous
ma and small cell
ndocrine carcinoma
HSIL Positive
ous carcinoma and
cystic carcinoma
LSIL Positive
d basal/squamous
ma
HSIL –
nvasive squamous
ma
HSIL Positive
d basal/squamous
ma
HSIL –
ous carcinoma HSIL –
d basal/squamous
ma
HSIL Positive
d basal/squamous
ma
HSIL Negative
Margin status on
hysterectomy
Lymph node status
(positive/total)
Follow-up
status, months
Negative Negative (0/26) NED, 27
Positive ND NED, 72
ND ND DOC/NED, 18
Positive, with
tumor in parametria
Negative (0/19) NED, 18
Negative ND NED, 29
Negative Negative (0/45) NED, 78
Negative Negative (0/14) NED, 84
Negative ND NED, 8
Negative Negative (0/41) Recent case
Negative ND Recent case
US, atypical glandular cells of undetermined significance; HSIL, high-grade
BSO, bilateral salpingo-oophorectomy; RSO, right salpingo-oophorectomy;
of other causes with no evidence of disease.

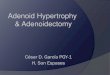
Fig. 1 Adenoid basal epithelioma (the associated invasive
carcinoma is not illustrated). The low-grade noninfiltrative compo-
nent is illustrated. Nests of tumor display basaloid, squamous, and
glandular differentiation. The stroma lacks a desmoplastic response.
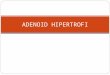
Fig. 2 Adenoid basal epithelioma (the associated invasive
carcinoma is not illustrated). The low-grade noninfiltrative compo-
nent associated with invasive carcinoma is illustrated. Nests of
tumor display basaloid and glandular differentiation. The stroma
lacks a desmoplastic response.
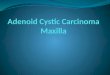
Fig. 3 Invasive squamous carcinoma associated with adenoid
basal epithelioma. Low magnification illustrates small nests of
adenoid basal epithelioma (top) associated with larger nests of
invasive squamous carcinoma.
Cervical adenoid basal tumors 85
glandular differentiation with minimal atypia and mitotic
activity (Figs. 1 and 2). The low-grade adenoid basal tumor
was connected to the overlying squamous intraepithelial
lesion in 3 cases. In all tumors, the low-grade adenoid basal
tumor component merged with areas of invasive carcinoma
(Fig. 3). These areas of invasive carcinoma were distinct
from the low-grade adenoid basal tumor components in that
the carcinomatous components exhibited greater nuclear
atypia and increased mitotic activity compared with the
low-grade components and had infiltrative patterns. Thus
there was little or no stromal response to the low-grade
components, but in the carcinomatous components the
surrounding stroma exhibited a more spindled or myxoid
appearance, often with inflammatory cells, consistent with
stromal desmoplasia (Fig. 4). The invasive carcinomatous
components in the tumors exhibited varying degrees of
adenoid basal and squamous differentiation. Adenoid basal
differentiation was characterized by cells in the nests with
scanty cytoplasm, peripheral palisading, and focal gland
formation (Figs. 4 and 5), and squamous differentiation was
manifested by increased amounts of dense eosinophilic
cytoplasm in cells within the central portions of these nests
(Fig. 6). Thus some invasive components had pure adenoid
basal differentiation, some displayed combined adenoid

Fig. 4 Invasive adenoid basal carcinoma. This deeply invasive
tumor displays predominantly basaloid and focal glandular
differentiation. A focus of tumor is present within a lymphatic
space (upper right).
Fig. 5 Invasive adenoid basal/squamous carcinoma. Basaloid
differentiation in the carcinoma is characterized by cells with
scanty cytoplasm and peripheral palisading. The smaller nest of
tumor at the top displays glandular (badenoidQ) differentiation.
There is nuclear atypia, and numerous mitotic figures are evident.
A.V. Parwani et al.86
basal and squamous differentiation, and some had pure
squamous differentiation (Figs. 3 to 6). A focus of
lymphatic invasion was identified in 1 case (Fig. 4). One
tumor also had a component of adenoid cystic carcinoma,
solid variant (Figs. 7 and 8). In another tumor, most of the
invasive component exhibited features of a high-grade
small cell neuroendocrine carcinoma, characterized by cells
with hyperchromatic nuclei, nuclear molding and stream-
ing, and minimal cytoplasm (Fig. 9). This component was
focally positive for cytokeratin and expressed neuroendo-
crine markers. In the 6 cases diagnosed on excisional
biopsy specimens, the invasive carcinoma extended to the
margins of those specimens (Fig. 7).
Most patients were treated with some form of hysterec-
tomy, often with bilateral salpingo-oophorectomy and
lymph node dissection. All those treated by surgery had
residual tumor in the cervix, ranging from just residual
adenoid basal tumor in the case with microinvasive
squamous carcinoma (in the excisional biopsy specimen)
to variable amounts of residual invasive carcinoma. The
amount of residual carcinoma ranged from microscopic foci
to deeply invasive tumor. For those cases in which
maximum dimensions could be obtained, the tumors ranged
in size from 0.4 to 3.3 cm in greatest dimension, with depth
of invasion ranging from 0.2 to 1.4 cm. Most cases had
negative margins on the hysterectomy specimens, and all
cases with lymph node dissections had no evidence of
lymph node metastases. However, 1 case had positive
margins with unknown lymph node status, and another case
had involvement of the parametria with a positive margin
but negative lymph nodes. Seven of 8 patients with
available follow-up were alive without evidence of disease
after follow-up intervals of 8 to 84 months (mean, 45
months; median, 29 months); 2 cases were recent, with very
limited follow-up. One patient with a component of small
cell carcinoma died of other causes, without evidence of
disease on imaging studies, at 18 months.
3.2. Immunohistochemical p16 expression and HPVdetection by in situ hybridization and PCR
All tumors exhibited diffuse expression of p16
(cytoplasmic, often with nuclear as well) in both the
adenoid basal epithelioma and invasive carcinoma com-
ponents (Fig. 10). HPV 16 DNA was detected in both the
adenoid basal epithelioma and invasive carcinoma com-
ponents in 9 tumors (Fig. 11). The positive reactions were
characterized by discrete punctate reactivity confined to

Fig. 6 Invasive adenoid basal/squamous carcinoma. Invasive
carcinoma exhibits mixed basaloid and squamous differentiation.
Basaloid differentiation is seen at the periphery of the nests, where
palisading is evident. The central portion of the nest contains cells
with more abundant dense eosinophilic cytoplasm, indicating
squamous differentiation. There is nuclear atypia, and an abnormal
mitotic figure is present.
Cervical adenoid basal tumors 87
tumor nuclei. In 1 tumor (case 9), HPV DNA was not
detected by in situ hybridization, but PCR demonstrated
the presence of HPV 33.
Fig. 7 Mixed adenoid cystic carcinoma and squamous carcino-
ma associated with adenoid basal epithelioma. Low magnification
illustrates solid nests of adenoid cystic carcinoma (lower portion)
extending to the margin of the excisional specimen. Adjacent
tumor (upper portion) consists of small nests of adenoid basal
epithelioma (upper right) and slightly larger nests of squamous
carcinoma (upper left).
4. Discussion
Adenoid basal tumors are uncommon tumors of the
cervix that have been designated as badenoid basal
carcinomasQ in most reports [1-8]. More recently, the
designation badenoid basal epitheliomaQ has been suggested
as a more appropriate term, because most reported cases
have been associated with benign behavior [9]. Of 39 cases
reported in 7 studies, only 1 patient died of tumor [8], but it
appears that the tumor in that fatal case had unusual
histological features and may have been a high-grade
invasive basaloid carcinoma rather than a typical adenoid
basal tumor [1,2,6,8,9,14,15]. In addition, several studies
have emphasized the need to distinguish adenoid basal
tumors from adenoid cystic carcinomas of the cervix
because the latter are associated with a distinctly unfavor-
able prognosis [3,6,8,16].
Based on the collective experience in the literature, with
specific reference to points made in the study suggesting the
term bepitheliomaQ and the cases in the current study, several
observations can be made. First, based on the previous
studies, it appears that pure, typical adenoid basal tumors
(without malignant cytological features and unassociated
with other forms of invasive carcinoma) lack many of the
features of a malignant neoplasm and virtually always behave
in a benign fashion, even when present deep within the
cervical stroma [9]. Second, based on the cases in our study
and other reports in the literature, some typical adenoid basal
tumors can be associated with an unequivocal invasive
carcinoma displaying the microscopic features of carcinoma,
including increased cytological atypia, mitotic activity with
abnormal mitotic figures, and deeply infiltrative growth of
these cytologically malignant components. In addition, the
invasive components can display patterns of differentiation
indicating specific subtypes of invasive carcinoma with
established malignant behavior, including squamous, ade-
noid cystic, and small cell neuroendocrine carcinomas.
Although no lymph node metastases or tumor-related
deaths were observed in our study, all of the tumors
contained a carcinomatous component displaying malignant
cytological features; in addition, many deeply invaded the
cervical stroma, and some extended to margins or involved
the parametrial soft tissue. Notable cytological atypia and
deeply infiltrative growth are pathological features associ-

Fig. 8 Adenoid cystic carcinoma. Higher magnification of the
tumor in Fig. 7 illustrates the typical appearance of the solid form
of adenoid cystic carcinoma.
Fig. 9 Small cell neuroendocrine carcinoma associated with
adenoid basal epithelioma. Small cell carcinoma component (lower
portion) is composed of undifferentiated cells with scanty
cytoplasm and hyperchromatic nuclei displaying nuclear molding
and streaming. Small nests of adenoid basal epithelioma (upper
portion) are seen adjacent to the carcinoma.
A.V. Parwani et al.88
ated with carcinomas rather than benign tumors; hence, use
of the term bcarcinomaQ is appropriate for tumors exhibiting
these features despite the lack of documented malignant
behavior in the reported tumors.
We suggest the following approach to diagnosing the
spectrum of tumors exhibiting adenoid basal differentiation.
Pure low-grade adenoid basal tumors lacking appreciable
cytological atypia, mitotic activity, and an infiltrative pattern
in a desmoplastic stroma (ie, without evidence of invasive
carcinoma of adenoid basal/squamous, pure squamous,
adenoid cystic, or other type) that are confined to an
excisional specimen with clearly negative margins can be
designated as badenoid basal epitheliomas.QThis terminology
has been recommended by other investigators and is more
appropriate than the term badenoid basal hyperplasia,Qbecause it acknowledges that these lesions are neoplasms
that may be precursors of the associated invasive carcinomas
occasionally encountered [9,17]. Tumors composed of both
typical low-grade adenoid basal tumor (epithelioma) and an
invasive, cytologically malignant component exhibiting
adenoid basal/squamous, pure squamous, and/or adenoid
cystic differentiation can be diagnosed as invasive carcino-
mas based on their morphological features. Those with mixed
differentiation can be subclassified according to the patterns
of differentiation (such as mixed adenoid basal/squamous
carcinoma, or mixed squamous and adenoid cystic carcino-
ma). Many tumors with the features of carcinoma may well
behave in a benign fashion after complete excision based on
the experience in the literature and this study, but the
designation bcarcinomaQ is appropriate in view of their
morphological features. Thus most adenoid basal tumors
can be classified as either epithelioma or carcinoma when
either the entire lesion is available for evaluation or the
microscopic features of malignancy are present.
Tumors extending to the margins of an excisional
specimen but lacking cytological features of malignancy
and the histological features of typical invasive squamous,
adenoid basal, or adenoid cystic carcinoma pose some
difficulty, in that adequacy of treatment cannot be deter-
mined. Accordingly, in practice such tumors can be
designated as adenoid basal epithelioma with a comment
that the possibility of an invasive carcinomatous component
cannot be excluded due to incomplete evaluation in the
setting of a positive margin. In such cases another excisional
specimen or hysterectomy is required to exclude an invasive
component and assure adequate treatment.
Other investigators have demonstrated by both in situ
hybridization and PCR that cervical adenoid basal carcino-
mas, adenoid cystic carcinomas, and small cell carcinomas
contain HPV DNA (most often HPV 16) [4,5,7,18,19]. Our

Cervical adenoid basal tumors 89
study confirms these observations and demonstrates that
both the adenoid basal epithelioma and invasive carcinoma
components contain high-risk HPV. In addition, the finding
of high-risk HPV DNA in both components suggests that
the carcinomas arose from the adenoid basal epitheliomas
and lends further support to the concept that the epithelio-
mas are neoplastic precursor lesions [17]. Immunohisto-
chemical detection of p16 expression is associated with
high-risk HPV infection in cervical intraepithelial lesions
and invasive carcinomas and can serve as a surrogate
marker of high-risk HPV infection in the appropriate
pathological setting [20,21]. The diffuse expression of p16
in all tumors in our study, including 1 tumor in which HPV
DNA was not detected by in situ hybridization, indicates
that immunohistochemical expression of p16 can be used as
a surrogate marker of high-risk HPV infection in these
tumors when in situ hybridization reactions do not detect
HPV due to technical reasons or when in situ hybridization
and PCR techniques are not available in the laboratory. The
finding of various subtypes of high-risk HPV-related
invasive cervical carcinomas intimately associated with
adenoid basal epitheliomas in our cases lends support to
the concept that adenoid basal tumors are of putative reserve
Fig. 10 Mixed adenoid cystic carcinoma and squamous carci-
noma associated with adenoid basal epithelioma. Diffuse expres-
sion of p16 is evident in all components of the tumor illustrated
in Fig. 7.
Fig. 11 Mixed adenoid cystic carcinoma and squamous carci-
noma associated with adenoid basal epithelioma. Adenoid basal
epithelioma component contains HPV 16 DNA as demonstrated by
a punctate nuclear reaction product in the in situ hybridization
preparation. The carcinomatous components were similarly posi-
tive (not shown).
cell origin, by demonstrating the potential of these invasive
components to undergo divergent differentiation [3,4].
Acknowledgments
The authors thank Keerti V. Shah, MD, DrPH, Depart-
ment of Molecular Microbiology and Immunology, Johns
Hopkins Bloomberg School of Public Health, for providing
the PCR analysis.
References
[1] Baggish MS, Woodruff JD. Adenoid basal lesions of the cervix.
Obstet Gynecol 1971;37:807-19.
[2] Baggish MS, Woodruff JD. Adenoid-basal carcinoma of the cervix.
Obstet Gynecol 1966;28:213-8.
[3] Grayson W, Taylor LF, Cooper K. Adenoid cystic and adenoid basal
carcinoma of the uterine cervix: comparative morphologic, mucin, and
immunohistochemical profile of two rare neoplasms of putative
breserve cellQ origin. Am J Surg Pathol 1999;23:448-58.

A.V. Parwani et al.90
[4] Grayson W, Taylor LF, Cooper K. Adenoid basal carcinoma of the
uterine cervix: detection of integrated human papillomavirus in a rare
tumor of putative breserve cellQ origin. Int J Gynecol Pathol
1997;16:307-12.
[5] Jones MW, Kounelis S, Papadaki H, et al. The origin and molecular
characterization of adenoid basal carcinoma of the uterine cervix. Int J
Gynecol Pathol 1997;16:301 -6.
[6] Van Dinh T, Woodruff JD. Adenoid cystic and adenoid basal
carcinomas of the cervix. Obstet Gynecol 1985;65:705 -9.
[7] Cviko A, Briem B, Granter SR, et al. Adenoid basal carcinomas of the
cervix: a unique morphological evolution with cell cycle correlates.
Hum Pathol 2000;31:740 -4.
[8] Ferry JA, Scully RE. bAdenoid cysticQ carcinoma and adenoid basal
carcinoma of the uterine cervix. A study of 28 cases. Am J Surg
Pathol 1988;12:134-44.
[9] Brainard JA, Hart WR. Adenoid basal epitheliomas of the uterine
cervix. A reevaluation of distinctive cervical basaloid lesions currently
classified as adenoid basal carcinoma and adenoid basal hyperplasia.
Am J Surg Pathol 1998;22:965 -75.
[10] Clement PB, Zubovits JT, Young RH, et al. Malignant mullerian
mixed tumors of the uterine cervix: a report of nine cases of a
neoplasm with morphology often different from its counterpart in the
corpus. Int J Gynecol Pathol 1998;17:211-22.
[11] Grayson W, Taylor LF, Cooper K. Carcinosarcoma of the uterine
cervix: a report of eight cases with immunohistochemical analysis and
evaluation of human papillomavirus status. Am J Surg Pathol
2001;25:338 -47.
[12] Takeshima Y, Amatya VJ, Nakayori F, et al. Co-existent carcinosar-
coma and adenoid basal carcinoma of the uterine cervix and
correlation with human papillomavirus infection. Int J Gynecol Pathol
2002;21:186 -90.
[13] Gravitt PE, Peyton CL, Alessi TQ, et al. Improved amplification
of genital human papillomaviruses. J Clin Microbiol 2000;38:
357-61.
[14] Daroca Jr PJ, Dhurandhar HN. Basaloid carcinoma of uterine cervix.
Am J Surg Pathol 1980;4:235-9.
[15] Samaratunga H, Beresford A, Davison A. Squamous cell carcinoma in
situ involving mesonephric remnants. A potential diagnostic pitfall.
Am J Surg Pathol 1994;18:1265-9.
[16] Albores-Saavedra J, Manivel C, Mora A, et al. The solid variant of
adenoid cystic carcinoma of the cervix. Int J Gynecol Pathol
1992;11:2 -10.
[17] Grayson W, Cooper K. Adenoid basal epithelioma versus adenoid
basal carcinoma. Am J Surg Pathol 2000;24:313-4.
[18] Grayson W, Taylor L, Cooper K. Detection of integrated high-risk
human papillomavirus in adenoid cystic carcinoma of the uterine
cervix. J Clin Pathol 1996;49:805-9.
[19] Masumoto N, Fujii T, Ishikawa M, et al. P16 overexpression and
human papillomavirus infection in small cell carcinoma of the uterine
cervix. Hum Pathol 2003;34:778 -83.
[20] Klaes R, Friedrich T, Spitkovsky D, et al. Overexpression of
p16(INK4A) as a specific marker for dysplastic and neoplas-
tic epithelial cells of the cervix uteri. Int J Cancer 2001;92:
276-84.
[21] Sano T, Oyama T, Kashiwabara K, et al. Expression status of p16
protein is associated with human papillomavirus oncogenic
potential in cervical and genital lesions. Am J Pathol 1998;153:
1741-8.