Embed Size (px)
Citation preview

Immunohistochemical Surrogate Markers ofBreast Cancer Molecular Classes PredictsResponse to Neoadjuvant ChemotherapyA Single Institutional Experience With 359 Cases
Rohit Bhargava, MD1; Sushil Beriwal, MD2; David J. Dabbs, MD1; Umut Ozbek, MS3; Atilla Soran, MD4;
Ronald R. Johnson, MD4; Adam M. Brufsky, MD5; Barry C. Lembersky, MD5; and Gretchen M. Ahrendt, MD4
BACKGROUND: Complete pathologic response to neoadjuvant chemotherapy (NACT) is predominantly seen in
‘‘ERBB2’’ and ‘‘basal-like’’ tumors using expression profiling. We hypothesize that a similar response could be pre-
dicted using semiquantitative immunohistochemistry for estrogen receptors (ER), progesterone receptors (PR), and
human epidermal growth factor receptor 2 (HER2). METHODS: ER, PR, and HER2 were used to classify 359 tumors
treated with NACT into 6 groups: luminal A (strong ERþ, HER2 negative), luminal B (weak to moderate ERþ, HER2
negative), triple negative (negative for ER, PR, and HER2), ERBB2 (negative for ER and PR, but HER2þ), luminal A-
HER2 hybrid (strong ERþ and HER2þ), and luminal B-HER2 hybrid (weak to moderate ERþ and HER2þ). Complete
pathologic response was defined as absence of invasive carcinoma in the breast and regional lymph nodes. RESULTS:
Thirteen percent (48 of 359) demonstrated complete pathologic response. The highest rate of complete pathologic
response was seen in ERBB2 (33%; 19 of 57) and triple negative (30%; 24 of 79) tumor classes. Among the ERþ ‘‘mo-
lecular’’ group, the highest rate of complete pathologic response was seen among luminal B-HER2 hybrid tumors, 8%
(2 of 24). Remainder of ERþ tumors demonstrated a very low rate of complete pathologic response, 1.5% (3 of 198).
The 5-year survival for patients achieving complete pathologic response was 96% compared with 75% in patients
that failed to achieve complete pathologic response. The overall survival was worse in the ER-negative group (ERBB2
and triple negative) compared with the ER-positive group. CONCLUSIONS: We confirm the recently defined ‘‘triple
negative paradox,’’ or rather ‘‘hormone receptor negative paradox,’’ that despite the best response to NACT, ERBB2
and triple negative tumors show the worst overall survival because of higher relapse among those with residual
disease. Cancer 2010;116:1431–9. VC 2010 American Cancer Society.
KEYWORDS: immunohistochemical surrogate markers, breast cancer molecular classes, neoadjuvant chemotherapy,
pathologic complete response, survival.
Traditionally, neoadjuvant chemotherapy (NACT) has been used in locally advanced breast cancers that aredeemed inoperable.1 More recently, it has been increasingly used for T2 and T3 tumors that are resectable, but the intentis to reduce the tumor size by NACT and subsequently remove a smaller portion of breast tissue than would otherwise beremoved at primary surgery.2-4 NACT followed by excision provides a unique opportunity to objectively assess in vivo tu-mor response to chemotherapeutic drugs. This information can be used for future patient treatment for further consolida-tion in case of complete response or trigger alternative therapeutic regimen in cases of minimal or no response.
Breast cancer is a heterogeneous disease at the morphologic, immunohistochemical (IHC), and even molecular level.Therefore, some breast carcinomas respond completely to NACT and others show minimal or no response.4,5 Apart fromthe breast tumor itself, other factors that may predict response include the number of cycles and type of chemotherapy
DOI: 10.1002/cncr.24876, Received: April 1, 2009; Revised: June 17, 2009; Accepted: July 10, 2009, Published online February 3, 2010 in Wiley InterScience
(www.interscience.wiley.com)
Corresponding author: Rohit Bhargava, MD, Department of Pathology, Magee-Womens Hospital, University of Pittsburgh Medical Center, 300 Halket Street,
Pittsburgh, PA 15213; Fax: (412) 641-1675; [email protected]
1Department of Pathology, Magee-Womens Hospital of UPMC, Pittsburgh, Pennsylvania; 2Department of Radiation Oncology, Magee-Womens Hospital of UPMC,
Pittsburgh, Pennsylvania; 3Department of Biostatistics, University of Pittsburgh, Pittsburgh, Pennsylvania; 4Department of Surgery, Magee-Womens Hospital of
UPMC, Pittsburgh, Pennsylvania; 5Department of Medical Oncology, Magee-Womens Hospital of UPMC, Pittsburgh, Pennsylvania
We thank Louise Mazur and Karen Baurle for clerical assistance.
Cancer March 15, 2010 1431
Original Article

used,6 tumor tissue microenvironment, and hostresponse. The latter factors are no doubt important, butthe current chemotherapeutic protocols are rather limitedand use a very similar type of chemotherapy (anthracy-cline or taxane based) except for human epidermal growthfactor receptor 2 (HER2)-positive patients who alsoreceive trastuzumab, and most patients receive 4-8 cyclesbefore surgical excision.7-9 The tumor tissue microenvir-onment and host response may also be important deter-minants of chemotherapeutic response but appears to betightly linked to tumor type itself.
On the basis of decades of morphologic data, it iswell-known that only a subset of ductal carcinomas showspathologic complete response to NACT. Recent geneexpression-based studies have shown complete pathologic
response in 45% of ERBB2 and basal-like breast carcino-mas compared with only 6% in luminal subtype.10
The primary aim of this study was to analyze theNACT database at our institution and identify the molec-ular classes (using IHC surrogate markers) that predictcomplete pathologic response to NACT. The molecularclasses, tumor grade, and complete pathologic responsewere correlated with disease-free survival (DFS) and over-all survival (OS).
MATERIALS AND METHODSThe institutional review board approved the study. Thepatient case list was obtained from the hospital tumorregistry, which represented consecutive cases treated withNACT at our institution. However, some cases did notmeet the criteria for inclusion in the study as explained inTable 1. Clinical information and pathology data wascarefully extracted from the clinical charts and reports toinclude a total of 359 cases for this study (Table 1).
IHC Surrogate Markers of MolecularClassification
Semiquantitative IHC results for hormone receptor andHER2 were obtained from pathology reports to classifytumors into molecular classes (Table 2). By using the cri-teria mentioned in Table 2, the tumors were classified asluminal A, luminal B, ERBB2, triple negative, luminal A-HER2 hybrid, and luminal B-HER2 hybrid. These crite-ria correspond to the initial gene expression profilingstudies and are similar (but not identical) to the priorstudies that used IHC as a surrogate for molecular classifi-cation.11-13 The criteria shown in Table 2 primarily
Table 1. Data Acquisition and Reasons for Case Deletion
Data acquisition: Late 1999 to early 2006
Total patients: 439
Total cases: 451
Cases deleted: 92
Total cases classified and examined for complete pathologic response:
359
Reasons for case deletion� Not a true neoadjuvant chemotherapy case, ie, excisional
biopsy performed that removed a large portion of the tumor
� Receptor study results not available
� Receptor results not semiquantitated
� HER2 results not available
� ERBB2(HER2) FISH not performed on HER2 IHC 21 case
� Suboptimal pathologic exam to determine complete patho-
logic response
Pretherapy biopsy slides were available for review on 191 cases (ie,
minus 168 cases)
HER2 indicates human epidermal growth factor receptor 2; FISH, fluores-
cence in situ hybridization; IHC, immunohistochemical.
Table 2. IHC Criteria Used for Molecular Classification
Molecular ClassBased on IntrinsicGene Set
IHC CategoriesUsed in theCurrent Study
Criteria Usedfor the IHCCategories
CorrespondingCategories (Cheang14)
Luminal A Luminal A ER score 200 or higher, HER2 negative Luminal
Luminal B Luminal B ER score 11-199 or PR score >10, HER2 negative Luminal
ERBB2 ERBB2 ER and PR score 10 or less, HER2 positive HER2þ/ER-/PR-
Basal-like Triple negativea ER and PR score 10 or less, HER2 negative Triple negative phenotype;
core basal if þ for CK5/6 or
EGFR; 5 negative phenotype if negative for
CK5/6 and EGFR
? Luminal C Luminal A-HER2 hybrid ER score 200 or higher, HER2 positive Luminal/HER2þ? Luminal C Luminal B-HER2 hybrid ER score 11-199 or PR score >10, HER2 positive Luminal/HER2þ
IHC indicates immunohistochemical; HER2, human epidermal growth factor receptor; ER, estrogen receptor; PR, progesterone receptors; HER2 indicates
human epidermal growth factor receptor 2; EGFR, epidermal growth factor receptor.
2ER/PR scored using H-score like method with a dynamic range of 0-300.
HER2 considered positive if 3þ by IHC or unequivocally amplified by FISH.aTriple negative tumors may be classified into basal and non-basal using basal phenotype markers, but further classification was not performed in the current study.
Original Article
1432 Cancer March 15, 2010

correspond to Cheang et al’s criteria,14 but we have subdi-vided the luminal category into luminal A, luminal B,luminal A-HER2 hybrid, and luminal B-HER2 hybridbased on hormone receptor expression level and HER2positivity. The subdivision was performed to study theimpact of semiquantitative hormone receptor analysis andcoexpression of hormone receptors and HER2 on chemo-therapeutic tumor response and survival. At our institu-tion, estrogen receptor (ER) and progesterone receptor(PR) results are reported using a semiquantitative score(previously described as ‘‘H-score’’), which details the per-centage of positive cells showing none, weak, moderate, orstrong staining.15,16 The score is given as the sum of thepercentage staining multiplied by an ordinal value corre-sponding to the intensity level (0 ¼ none, 1 ¼ weak, 2 ¼moderate, 3 ¼ strong). With 4 intensity levels, the result-ing score ranges from 0 (no staining in the tumor) to 300(diffuse intense staining of the tumor). HER2 protein wasanalyzed and scored using either HercepTest (1999-2003)or CB11 antibody (2004-2006) and basic DAB detectionon Benchmark XT (Ventana, Tucson, Ariz). HER2 wasconsidered positive with either 3þ immunoreactivity (dif-fuse strong reactivity in >10% of the tumor cells) orunequivocal amplification by fluorescence in situ hybrid-ization (FISH) (with a ratio of HER2 to chromosome 17centromeric region >2.2, using PathVysion Vysis dual-color FISHbyVysis Inc., Downers Grove, Ill). All 2þ cases(by immunohistochemistry) included in this study werefollowed by FISH. Equivocal FISH result (1.8: 2.2 ratio)was considered as negative for HER2 in this study.
Morphologic Examination
A detailed morphologic examination of pretherapy corebiopsy specimen was performed on 191 cases. Slides fromthe remaining 168 specimens were not available forreview. Several morphologic parameters were recorded asfollows: tumor type (ductal, lobular, other), tumor sub-type, tubule formation score (1-3), nuclear pleomorphismscore (1-3), mitotic activity score (1-3), total score (3-9),Nottingham grade (1-3), absolute mitoses count/10 high-power fields, tumor borders (infiltrative/pushing), sheet-like growth pattern, lobular-like growth, spindle cells,apocrine differentiation, nucleoli (visibility at �10),lymphoid infiltrate (10% or less/11%-50%/>50%), geo-graphic necrosis, apoptosis (visibility at �10), ductal car-cinoma in situ (type/grade/comedonecrosis), lobularcarcinoma in situ, and lymphovascular space invasion.These criteria were slightly modified from the publishedcriteria by Fulford and colleagues.17
Patient Treatment With NACT
NACT given to patients included compounds that aregenerally given as adjuvant chemotherapy.2 Because thiswas not a clinical trial, the patient population was diverseand the treatment received by patients was variable.NACT given to the patients was mainly based on clinicalstaging and physician discretion. The type of therapygiven can be broadly classified as anthracycline-basedtherapy, ie, doxorubicin (Adriamycin) plus cyclophospha-mide, 5-flurouracil, epirubicin, and cyclophosphamide, ortaxane-based therapy, ie, taxol plus carboplatinum, and incases of HER2-positive tumors, such as taxol, carboplati-num, and trastuzumab. In many cases a sequential combi-nation of anthracycline and taxane was given, ie,doxorubicin (Adriamycin) plus cyclophosphamide followedby taxane. The doses given were generally the recommendeddoses per unit body surface area. The total number of cyclesranged from 4-10 with an average total cycle number of 6.Trastuzumab was part of the NACT regimen in only 6ERBB2 tumors and 10 non-ERBB2, HER2-positivetumors. Trastuzumab was more often administered as adju-vant therapy inHER2-positive tumors.
Response Assessment
Complete pathologic response was defined as absence ofinvasive carcinoma in the post-therapy resection specimenand within regional lymph nodes. Percentage tumor sizereduction was also calculated based on pretherapy clinical tu-mor size and residual tumor size in the resection specimen.
Clinical Follow-Up
Disease-free survival (DFS) was calculated as the timefrom the date of diagnosis of the primary tumor to thedate of the development of distant or locoregional recur-rence. Overall survival (OS) was calculated as the timefrom the date of diagnosis of the primary tumor to thedate of death from any cause, or the date of last contact.The data were analyzed for DFS and OS separately forpatients with complete pathologic response and patientswithout complete pathologic response. Patient DFS andOS with respect to molecular classes and tumor grade wasalso analyzed.
Statistical Analysis
The chi-square (Monte Carlo method) test was used tocompare tumor stages among molecular classes andNACT given among molecular classes. The Kruskal-Wallis test was used to evaluate possible differences of agesamong molecular classes. Univariate logistic regression
IHC Criteria and Neoadjuvant Chemotherapy/Bhargava et al
Cancer March 15, 2010 1433

analyses were performed for each potential predictor vari-able of complete pathologic response to NACT. Variableswere included in the multivariate analysis if the univariateP-value was �.25. A stepwise selection procedure wasused to predict the probability of achieving completepathologic response. The survival experience was exam-ined with the 2 methods of time-to-event analyses: DFSand OS. The Kaplan-Meier survival curves were evaluatedfor difference among groups with the log-rank test. P-val-ues <.05 were considered statistically significant. Thedata analysis for this paper was generated using SAS soft-ware, Version 9.2 of the SAS System for Windows, prod-uct of SAS Institute Inc. (Cary, NC).
RESULTSThe 359 tumors treated with NACT comprised 111(31%) luminal A, 73 (20%) luminal B, 57 (16%)ERBB2, 79 (22%) triple negative, 15 (4%) luminal A-HER2 hybrid, and 24 (7%) luminal B-HER2 hybrid. Asthese cases were considered for NACT, most were stage IIor higher at the time of diagnosis. There was no significantdifference in tumor stage among different molecularclasses (P ¼ .129). The patients with strong ERþ tumors(luminal A and luminal A-HER2 hybrid with median ageof 53 and 54 years) were 5-10 years older than weak/mod-erate ER-positive and ER-negative tumors (luminal B-HER2 hybrid, luminal B, ERBB2, triple negative withmedian ages of 44, 47, 48, 49 years, respectively), a differ-ence that was statistically significant (P ¼ .0002). Thepatient clinical data and tumor characteristics are shownin Table 3.
Molecular Class and Response to NACT
Of the 359 cases that could be classified using IHC surro-gate markers, 48 cases (13%) demonstrated completepathologic response. The highest rate of complete patho-logic response was seen in ERBB2 and triple-negative tu-mor classes with 33% (19 of 57) and 30% (24 of 79)showing complete pathologic response, respectively (Ta-ble 4). Among the ERþ ‘‘molecular’’ groups, the highest
Table 3. Patient Clinical Data and Tumor Characteristics for Each Molecular Class
LuminalA
LuminalB
ERBB2 TripleNegative
LuminalA-HER2 Hybrid
LuminalB-HER2 Hybrid
No. of Cases¼359 111 (31%) 73 (20%) 57 (16%) 79 (22%) 15 (4%) 24 (7%)
Median age (range) 53, y (24-87) 47, y (30-81) 48, y (25-76) 49, y (26-79) 54, y (43-80) 44, y (27-69)
Mean tumor size (median) 2.7 cm (2.1) 2.9 cm (2.6) 3.3 cm (2.9) 3.4 cm (3.0) 3.8 cm (3.0) 3.4 cm (3)
Tumor grade, data on 191 cases onlyGrade 1 7/60 (12%) 5/38 (13%) 0/29 (0%) 0/40 (0%) 0/9 (0%) 1/15 (7%)
Grade 2 48/60 (80%) 32/38 (84%) 19/29 (66%) 9/40 (22%) 9/9 (100%) 8/15 (53%)
Grade 3 5/60 (8%) 1/38 (3%) 10/29 (34%) 31/40 (78%) 0/9 (0%) 6/15 (40%)
Pretherapy tumor stageI 12 (11%) 6 (8%) 1 (2%) 4 (5%) 0 (0%) 0 (0%)
II 58 (52%) 49 (67%) 29 (51%) 45 (57%) 9 (60%) 14 (58%)
III 30 (27%) 11 (15%) 21 (37%) 27 (34%) 5 (33%) 9 (38%)
Indeterminate 11 (10%) 7 (10%) 6 (10%) 3 (4%) 1 (7%) 1 (4%)
NACT givenAnthracycline based (without taxane) 23 (20%) 15 (21%) 14 (24%) 24 (30%) 1 (7%) 6 (25%)
Taxane based (without anthracyclines) 12 (11%) 7 (10%) 21 (37%) 6 (8%) 4 (26%) 7 (29%)
Anthracycline 1 taxane 63 (57%) 47 (64%) 21 (37%) 49 (62%) 8 (53%) 11 (46%)
Trastuzumab as part of NACT 0 (0%) 0 (0%) 6/57 (11%) 0 (0%) 6/15 (40%) 4/24 (17%)
Other 2 (2%) 3 (4%) 0 (0%) 0 (0%) 1 (7%) 0 (0%)
Unknown 11 (10%) 1 (1%) 1 (2%) 0 (0%) 1 (7%) 0 (0%)
Average number of therapy cycles 6.4 6.8 6 6.7 6.6 6.1
HER2 indicates human epidermal growth factor receptor 2; NACT, neoadjuvant chemotherapy.
Table 4. Molecular Classes and Complete PathologicResponse
Molecular Class Absenceof CompletePathologicResponse
CompletePathologicResponse
Total
Luminal A 109 (98.2%) 2 (1.8%) 111
Luminal B 72 (98.6%) 1 (1.4%) 73
ERBB2 38 (66.7%) 19 (33.3%) 57
Triple negative 55 (69.6%) 24 (30.4%) 79
Luminal A-HER2 hybrid 15 (100%) 0 (0%) 15
Luminal B-HER2 hybrid 22 (91.7%) 2 (8.3%) 24
Total 311 (86.6%) 48 (13.4%) 359
Original Article
1434 Cancer March 15, 2010

rate of complete pathologic response was seen amongluminal B-HER2 hybrid tumors, 8% (2 of 24). The re-mainder of ERþ tumors demonstrated dismal rate ofcomplete pathologic response, 1.5% (3 of 198). Althoughcomplete pathologic response information was available onall 359 cases, tumor size reduction could not be analyzedon 30% of cases because of lack of information abouteither pretherapy tumor size or ambiguous reporting of thepost-therapy tumor size. The precise cellularity of the post-therapy residual tumor specimen was not available; there-fore, quantification (such as Miller-Payne scoring)9,18 ofresidual tumor was not feasible. Despite these shortcom-ings, the percentage tumor size reduction (available on70% of cases) deduced from gross and microscopicdescription provided a reasonable alternative to comparetumor size reduction in different tumor classes. The meantumor size reduction was higher in ERBB2 and triple-neg-ative tumors compared with other classes. The average per-centage tumor size reduction in descending order was asfollows: triple negative (75%), ERBB2 (68%), luminal B-HER2 hybrid (47%), luminal A-HER2 hybrid (33%),luminal B (30%), and luminal A (23%).
Type and Amount of Chemotherapy
The patients received anthracycline-based or taxane-basedchemotherapy, with most receiving a sequential combina-tion of both (Table 3). However, there were slight differ-ences between chemotherapy given to patients dependingon receptor status, HER2 status, clinical stage, and physi-cian preference. Despite this variability, there was no sta-tistical difference for NACT given (for the most effectiveregimen doxorubicin plus cyclophosphamide followed byT) between patients that achieved complete pathologicresponse and patients that failed to achieve complete path-ologic response (P¼ .9108). Trastuzumab was part of theNACT regimen in 6 ERBB2 tumors, of which 5 (83%)achieved complete pathologic response. In contrast, 10patients with non-ERBB2, but HER2-positive tumors (ie,luminal A-HER2 hybrid and luminal B-HER2 hybridtumors) received trastuzumab, of which none achievedcomplete pathologic response.
Univariate Analysis of All the AnalyzedVariables for Complete Pathologic Response
In a univariate analysis, the following factors predictedcomplete pathologic response: higher Nottingham tumorgrade, ER-negative molecular class, HER2 status, apoc-rine differentiation, necrosis, apoptosis, and presence ofspindle cells. However, it should be noted that with
regards to morphologic features, data were available onlyon 191 cases. If one closely examines each of these mor-phologic parameters, then the correlation between tumor‘‘molecular’’ classes, morphology and tumor grade can beidentified as shown previously.19
Multivariate Analysis for CompletePathologic Response
The variables, HER2 status, Nottingham grade, spindlecells, apocrine differentiation, geographic necrosis, apo-ptosis, stage, and molecular class (ERþ vs ER negative),having P-values �.25 in univariate analyses, were used tobuild a model by using multivariate logistic regression.However, only molecular class was found as a statisticallysignificant predictor for complete pathologic response.The probability of complete pathologic response is lowerfor patients who have ERþ disease than the patients hav-ing ER-negative breast cancer molecular class (OR¼ 0.06with 95% confidence interval [CI] 0.02-0.18).
Morphologic Analysis
Microscopic examination of 191 cases revealed a correla-tion between higher tumor grade and complete pathologicresponse, as complete pathologic response was identifiedin 1 of 13 (7%) of grade 1, 14 of 125 (11%) grade 2, and14 of 53 (26%) of grade 3 tumors (P ¼ .0073 for grade 3vs others). The most high-grade tumors (Nottinghamgrade 3) were seen predominantly in the triple-negativegroup (58% cases), less commonly in the ERBB2 (18%cases) and luminal B-HER2 hybrid (11% cases) groups,and least commonly in other molecular groups (ie, 13%of combined luminal A, luminal B, and luminal A-HER2hybrid cases). However, once the tumors were assigned toone of the molecular classes, further division by Notting-ham grade did not add any other information that wouldhave predicted complete pathologic response. In addition,several morphologic features were associated with particu-lar molecular class, such as necrosis and spindle cells withtriple-negative tumors, and apocrine differentiation withERBB2 class. The association of apocrine differentiationwith ERBB2 tumor class was quite strong and was identi-fied in 26 of 29 (90%) ERBB2 tumors compared with 35of 162 (22%) of all other tumors combined (P¼ .0001).
Survival Analysis
An average of a 46-month follow-up period was availableon all cases. The average follow-up period was similar forcases that showed complete pathologic response (mean,46 months; median, 42 months; range, 21-99 months)and for cases that did not show complete pathologic
IHC Criteria and Neoadjuvant Chemotherapy/Bhargava et al
Cancer March 15, 2010 1435

response (mean: 46 months; median, 42 months; range,10-104 months).
Of the 48 patients that showed complete pathologicresponse, 5 patients recurred at an average of 27 monthsfrom initial diagnosis, of which 2 died, both of breast can-cer. Forty-six (including the 3 patients that recurred) of48 patients (ie, 96% patients) that showed complete path-ologic response were alive (please see Figs. 1A and 1B forDFS and OS).
Of the 311 patients that failed to show completepathologic response, 92 recurred at an average of 22months, 199 had no recurrence, and on 20 cases, recur-rence data were not available. In this group, 77 died (ie,75% patients were alive) in this relatively short follow-upperiod (please see Figs. 1A and 1B for DFS and OS).
Patient DFS and OS were also analyzed based on tu-mor grade. There was no difference in DFS among differ-
ent tumor grades, but OS was the worst for grade 3tumors (P¼ .0474).
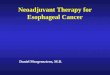
To test the validity of ‘‘triple-negative paradox,’’ theDFS and OS were compared between ER-negative(ERBB2 and triple negative) and ERþ (luminal A, lumi-nal B, luminal A-HER2 hybrid, and luminal B-HER2hybrid) molecular classes in patients that did not achievecomplete pathologic response. The DFS and OS wereworse for ER-negative molecular classes (P ¼ .0007 forDFS and <.0001 for OS; see Figs. 2A and 2B). The DFSand OS for ERþ versus ER-negative tumors was alsoexamined after stratifying by stage and the data remainedstatistically significant for each stage.
DISCUSSIONBreast cancer molecular classification using ‘‘intrinsic’’gene set demonstrated distinct molecular classeswith prognostic significance.20-22 As per our current
Figure 2. (A) Disease-free survival for estrogen receptor(ER)þ patients versus ER-negative patients that did notachieve complete pathologic response (P ¼ .0007). (B) Over-all survival for ERþ patients versus ER-negative patients thatdid not achieve complete pathologic response (P < .0001).
Figure 1. (A) Comparison of disease-free survival betweenpatients that achieved complete pathologic response versuspatients that failed to achieve complete pathologic response(P ¼ .0057). (B) Comparison of overall survival betweenpatients that achieved complete pathologic response versuspatients that failed to achieve complete pathologic response(P ¼ .0054).
Original Article
1436 Cancer March 15, 2010

understanding, these classes are luminal A, luminal B,ERBB2, and basal-like.23 The so-called ‘‘normal breast-like’’ group of tumors is now believed to be an artifact ofsampling and likely represented poorly sampled tumor tis-sue rather than a distinct, clinically important group.23,24
The initially described luminal C category was laterincluded along with luminal B tumors.21,22 Most IHCstudies that followed extrapolated the gene expressionfindings in less than optimal fashion. In a recent similarstudy, Carey et al classified the tumors based on IHC asluminal A (hormone receptorþ/HER2 negative), luminalB (hormone receptorþ/HER2þ), HER2 group (hor-mone receptor negative/HER2þ), and basal subtype(hormone receptor negative/HER negative). However,the authors clearly indicated in their study that ‘‘hormonereceptorþ/HER2þ tumors comprise only a minority ofluminal B tumors, so this method of subcategorizing theluminal subtype will necessarily misclassify a substantialfraction of luminal B tumors into the luminal A cate-gory.’’11 We have previously raised similar concerns aboutthis issue.25 Therefore, to faithfully reproduce the geneexpression profiling studies, we have used semiquantita-tive IHC (see Table 2). We believe this distinction is nec-essary to study the impact of semiquantitative IHChormone receptor analysis and coexpression of hormonereceptors and HER2 on chemotherapeutic tumorresponse and survival.
By using the simple IHC criteria shown in Table 2,the study findings suggest that routine hormone receptorand HER2 analysis can act as a substitute for expressionanalysis in predicting complete pathologic response toNACT. In one of the very first studies examining the rela-tionship between breast cancer molecular classes (usinggene expression analysis) and NACT tumor response,Rouzier et al demonstrated complete pathologic responsein 45% of ERBB2 and ‘‘basal-like’’ breast carcinomascompared with only 6% complete pathologic response inluminal tumors.10 Our results are very similar in the sensethat complete pathologic response was predominantly re-stricted to ERBB2 and triple-negative tumor classes; how-ever, the percentages of cases showing completepathologic response are slightly lower (30%-33% vs45%). This difference is likely explained by the larger andmore diverse study population in the current study and byslight differences in chemotherapeutic regimen betweenthe 2 studies. However, our findings are very similar tothe results obtained by Carey and colleagues,11 and webelieve the response rates observed in the current study aremore representative of the clinical experience.
Our semiquantitative hormone receptor analysisand IHC criteria for molecular classes were helpful in pre-dicting complete pathologic response and also showedsubtle differences in percentage tumor size reductionamong these classes. Average tumor size reduction appearsto be related to the amount of ER expression and presenceof HER2 overexpression. Surgeons and oncologists alikecan use this information in making better decisions aboutNACT. If the intent is to achieve complete pathologicresponse, only triple-negative and ERBB2 tumors shouldbe considered for NACT. The only other tumor type thatmay also be considered would be an luminal B-HER2hybrid tumor. If the intent is to reduce tumor size so thata smaller lumpectomy can be performed, then all tumorsmay be considered knowing that the tumor size reductionwould be lowest in strong ERþ, HER2-negative tumors.Because of short follow-up in the current study, the sur-vival differences were not apparent among the ERþtumors, but were significantly different between ERþ andER-negative ‘‘molecular’’ classes. Despite the bestresponse to NACT, ERBB2 tumors and triple-negativetumors showed the worst DFS and OS (5-year survival of65% for stage II and 45% for stage III). This worse sur-vival was seen only in the cases that did not achieve com-plete pathologic response, as cases that achieved completepathologic response had excellent survival irrespective ofthe molecular class (5-year survival of 96%). Our findingsare concordant with Carey et al, who called this phenom-enon ‘‘triple-negative paradox’’,11 ie, the good response toNACT, but poor survival rates because of higher relapseamong those with residual disease. Because both triple-negative and ERBB2 tumors demonstrate this phenom-enon, this triple-negative paradox should rather be called‘‘hormone receptor-negative paradox.’’
One unique feature of our study was review of thepretherapy tumor slides and detailed morphologic analy-sis on 191 cases. This examination showed that tumorgrades and molecular classes are not completely independ-ent of each other. It was not surprising to see that 3 tumorgrades distinctly showed different response to NACT andwere also prognostic. The tumor grades and molecularclasses (as identified by IHC) are closely interlinked. MostERBB2 and triple-negative tumors are Nottingham grade3, while luminal-type tumors are generally well-differenti-ated to moderately differentiated tumors. Although, bothERBB2 and triple-negative tumors responds equally toNACT, the morphologic examination suggested that themechanism of response is probably different. The triple-negative tumors are the most proliferative as was shown in
IHC Criteria and Neoadjuvant Chemotherapy/Bhargava et al
Cancer March 15, 2010 1437

the initial gene-expression profiling study20,21 and laterconfirmed with morphologic studies.26,27 The literaturealso suggests that ERBB2 tumors are high-grade, but moststudies fail to mention that ERBB2 tumors are not as pro-liferative as triple-negative tumors. In the current study, amitotic activity score of 3 was identified in 22 of 40(55%) triple-negative tumors in contrast to only 5 of 29(17%) ERBB2 tumors. This suggests that effect of NACTin triple-negative tumors is likely related to destruction ofrapidly proliferating cells but the effect of NACT inERBB2 tumors is related to mechanism other than inhibi-tion of cellular proliferation. Rouzier et al also reached atthe same conclusion as the genes responsible for completepathologic response in ERBB2 and ‘‘basal-like’’ tumors intheir study were distinct in each group.10
Another instructive feature of our study was the dif-ference in response rates among HER2þ tumors with theinclusion of trastuzumab in the NACT regimen. The useof trastuzumab in metastatic and adjuvant setting is nowwell-established. However, the use of trastuzumab in theneoadjuvant and adjuvant setting was mainly limited toclinical trials before 2005. This explains why only a totalof 16 (of 96) HER2þ patients received trastuzumab inour study. Despite these small numbers, the maximumbenefit was seen in ERBB2 (ERþ/PRþ/HER2þ) tumorscompared with luminal A-HER2 hybrid (strong ERþ/HER2þ) and luminal B-HER2 hybrid (weak to moderateERþ/HER2þ) tumors. Although none of the luminal A-HER2 hybrid or luminal B-HER2 hybrid tumors thatreceived trastuzumab showed complete pathologicresponse in this study, the percentage tumor size reduc-tion was far greater in luminal B-HER2 hybrid tumorsthan in luminal A-HER2 hybrid tumors, indicating extentof ER reactivity by IHC could influence tumor responseto trastuzumab. The effect of low ER expression on IHCcoupled with HER2 positivity was further exemplified by8% complete pathologic response rate in luminal B-HER2 hybrid tumors compared with only 1.5% completepathologic response rate in all other ERþ tumors.
In summary, we have shown that simple IHC-basedcategorization of breast tumors can help predict extent oftumor response to NACT. The predictive power of IHCcriteria appears to be similar to that of gene expressionanalysis. There are morphologic and immunohistologiccorrelates to molecular classes. Semiquantitative IHCanalyses of hormone receptors helps in better categoriza-tion of breast tumors than a mere positive or negativeresult. This information can be used toward improvedtherapeutic decisions.
CONFLICT OF INTEREST DISCLOSURESThe authors made no disclosures.
REFERENCES1. Kaufmann M, von Minckwitz G, Rody A. Preoperative
(neoadjuvant) systemic treatment of breast cancer. Breast.2005;14:576-581.
2. Gralow JR, Burstein HJ, Wood W, et al. Preoperative ther-apy in invasive breast cancer: pathologic assessment and sys-temic therapy issues in operable disease. J Clin Oncol. 2008;26:814-819.
3. Mieog JS, van der Hage JA, van de Velde CJ. Preoperativechemotherapy for women with operable breast cancer.Cochrane Database Syst Rev. 2007;CD005002.
4. Wolff AC, Davidson NE. Preoperative therapy in breastcancer: lessons from the treatment of locally advanced dis-ease. Oncologist. 2002;7:239-245.
5. Mauri D, Pavlidis N, Ioannidis JP. Neoadjuvant versus ad-juvant systemic treatment in breast cancer: a meta-analysis.J Natl Cancer Inst. 2005;97:188-194.
6. Gonzalez-Angulo AM, Morales-Vasquez F, Hortobagyi GN.Overview of resistance to systemic therapy in patients withbreast cancer. Adv Exp Med Biol. 2007;608:1-22.
7. Heys SD, Sarkar T, Hutcheon AW. Primary docetaxelchemotherapy in patients with breast cancer: impact onresponse and survival. Breast Cancer Res Treat. 2005;90:169-185.
8. Schwartz GF, Hortobagyi GN. Proceedings of the consensusconference on neoadjuvant chemotherapy in carcinoma ofthe breast, April 26-28, 2003, Philadelphia, Pennsylvania.Cancer. 2004;100:2512-2532.
9. Smith IC, Heys SD, Hutcheon AW, et al. Neoadjuvantchemotherapy in breast cancer: significantly enhancedresponse with docetaxel. J Clin Oncol. 2002;20:1456-1466.
10. Rouzier R, Perou CM, Symmans WF, et al. Breast cancermolecular subtypes respond differently to preoperativechemotherapy. Clin Cancer Res. 2005;11:5678-5685.
11. Carey LA, Dees EC, Sawyer L, et al. The triple negativeparadox: primary tumor chemosensitivity of breast cancersubtypes. Clin Cancer Res. 2007;13:2329-2334.
12. Carey LA, Perou CM, Livasy CA, et al. Race, breast cancersubtypes, and survival in the Carolina Breast Cancer Study.JAMA. 2006;295:2492-2502.
13. Nielsen TO, Hsu FD, Jensen K, et al. Immunohistochemi-cal and clinical characterization of the basal-like subtype ofinvasive breast carcinoma. Clin Cancer Res. 2004;10:5367-5374.
14. Cheang MC, Voduc D, Bajdik C, et al. Basal-like breastcancer defined by 5 biomarkers has superior prognosticvalue than triple-negative phenotype. Clin Cancer Res. 2008;14:1368-1376.
15. Flanagan MB, Dabbs DJ, Brufsky AM, Beriwal S, BhargavaR. Histopathologic variables predict Oncotype DX recur-rence score. Mod Pathol. 2008;21:1255-1261.
16. McCarty KS Jr, Miller LS, Cox EB, Konrath J, McCartyKS Sr. Estrogen receptor analyses. Correlation of biochemi-cal and immunohistochemical methods using monoclonalantireceptor antibodies. Arch Pathol Lab Med. 1985;109:716-721.
17. Fulford LG, Easton DF, Reis-Filho JS, et al. Specific mor-phological features predictive for the basal phenotype in
Original Article
1438 Cancer March 15, 2010

grade 3 invasive ductal carcinoma of breast. Histopathology.2006;49:22-34.
18. Ogston KN, Miller ID, Payne S, et al. A new histologicalgrading system to assess response of breast cancers to pri-mary chemotherapy: prognostic significance and survival.Breast. 2003;12:320-327.
19. Bhargava R, Striebel J, Beriwal S, et al. Prevalence, morpho-logic features and proliferation indices of breast carcinomamolecular classes using immunohistochemical surrogatemarkers. Int J Clin Exp Pathol. 2009;2:444-455.
20. Perou CM, Sorlie T, Eisen MB, et al. Molecular portraitsof human breast tumours. Nature. 2000;406:747-752.
21. Sorlie T, Perou CM, Tibshirani R, et al. Gene expression patternsof breast carcinomas distinguish tumor subclasses with clinicalimplications. Proc Natl Acad Sci U S A. 2001; 98:10869-10874.
22. Sorlie T, Tibshirani R, Parker J, et al. Repeated observationof breast tumor subtypes in independent gene expressiondata sets. Proc Natl Acad Sci U S A. 2003;100:8418-8423.
23. Sorlie T. Molecular classification of breast tumors: towardimproved diagnostics and treatments. Methods Mol Biol.2007;360:91-114.
24. Parker JS, Mullins M, Cheang MC, et al. Supervised riskpredictor of breast cancer based on intrinsic subtypes. J ClinOncol. 2009;27:1160-1167.
25. Bhargava R, Dabbs DJ. Luminal B breast tumors are notHER2 positive. Breast Cancer Res. 2008;10:404. Authorreply 405.
26. Lerma E, Peiro G, Ramon T, et al. Immunohistochemicalheterogeneity of breast carcinomas negative for estrogenreceptors, progesterone receptors and Her2/neu (basal-likebreast carcinomas). Mod Pathol. 2007;20:1200-1207.
27. Tan DS, Marchio C, Jones RL, et al. Triple negative breastcancer: molecular profiling and prognostic impact in adju-vant anthracycline-treated patients. Breast Cancer Res Treat.2008;111:27-44.
IHC Criteria and Neoadjuvant Chemotherapy/Bhargava et al
Cancer March 15, 2010 1439




![Immunohistochemical Biomarkers as a Surrogate of Molecular ... · grade 3 ENOC [18]. The adoption of prophylactic salpingo-oophorectomy in patients with BRCA muta-tion and extensive](https://img.pdfslide.net/doc/110x75/6123fe2a2913ad3c430eb813/immunohistochemical-biomarkers-as-a-surrogate-of-molecular-grade-3-enoc-18.jpg)