Embed Size (px)
Citation preview

Neoadjuvant Immunotherapy for NSCLCs
William N. William Jr., MD
Director of Oncology and Hematology, Hospital BP, a Beneficência Portuguesa de São Paulo
Adjunct Associate Professor, The University of Texas MD Anderson Cancer Center

Outline
• Background and rationale
• Neoadjuvant immunotherapy-based trials• IO monotherapy• IO combo• IO-chemo combo
• Challenges
• Future directions

Outline
• Background and rationale
• Neoadjuvant immunotherapy-based trials• IO monotherapy• IO combo• IO-chemo combo
• Challenges
• Future directions

The primary goal of adjuvant treatment is to eliminate micrometastatic disease
primary
micromets
Surgery
(primary)
Adjuvant
therapy
XX
Courtesy of Heymach JV, AACR 2018 (modified)

Neoadjuvant treatment can “downstage” the primary tumor
Neoadjuvant
therapy
X
surgery
X
XX
Courtesy of Heymach JV, AACR 2018 (modified)
Advantages of neoadjuvant therapy:• Downstage the tumor• Assess the biology of the disease• Impact micromets at an earlier
time point• Better tolerated before surgery
than after surgery • Assessment of response to
therapy• Translational analyses on tumors
at baseline and surgery • Evaluate potential surrogate
endpoints that may correlate with clinical benefit

Use of surrogate endpoints after induction therapy for neoadjuvant drug development in resectable NSCLC
• “FDA may grant traditional approval if a drug shows a direct clinical benefit or based on an improvement in an established surrogate”
• “The surrogate endpoint should be correlated with the clinical outcome, and should capture the complete net effect of the treatment on the clinical outcome”
Hellmann, ... William WN et al. Lancet Oncology 2014
Blumenthal G et al, J Thorac Oncol 2018 Pataer A, …, William WN et al., J Thorac Oncol, 2012

Major pathological response may represent a suitable surrogate for improved survival after neoadjuvant therapy
A. Overall Survival C.
D.
Overall Survival
Disease-Free Survival
Pataer A, William WN, … et al., J Thorac Oncol, 2012
MPR rate to neoadjuvant chemotherapy
in historical controls (MDACC): 19%
Recurrence-Free SurvivalB.
Cascone T, William WN, et al. Ann Thorac Surg, 2018

Chen L, Gibbons D et al, Nat Commun 2014
Genetic targeting of PD-L1 on cancer cells reverses the CD8+ TIL dysfunction and suppresses metastasis

Neoadjuvant IMT is superior to adjuvant in eradicating metastases in murine breast cancer model
Liu et al, Cancer Discovery 2016

Outline
• Background and rationale
• Neoadjuvant immunotherapy-based trials• IO monotherapy• IO combo• IO-chemo combo
• Challenges
• Future directions

Neoadjuvant anti-PD1 blockade is safe and
active in resectable NSCLC patients
Forde P et al, NEJM 2018
MPR (≤10% viable tumor cells) Rate: 45%

LCMC3 Study: Neoadjuvant Atezolizumab produces MPRs in 19% of resected NSCLC patients
Pathologic regression defined as % viable tumor cells – 100%. pCR, pathologic complete response. a 1 EGFR+ patient had aborted surgery. * Pathologic response could not be assessed. + EGFR+. + ALK+.
Patients in intended surgery population (n = 90)
• PR: 6 (7%); SD: 80 (89%); PD: 4 (4%)
• 3 of 8 EGFR/ALK+ had 40% to 50% pathological regression
Primary efficacy population (n = 77)
• MPR: 15 of 77 (19%; 95%CI: 11%, 30%)
• pCR: 4 of 77 (5%) patients
• 38 of 77 (49%) had ≥ 50% pathological regression
MPR
0% to −49% −50% to −89% −90% to −99% (MPR) −100% (MPR and pCR)
Kwiatkowski DJ, ASCO Annual Meeting 2019 Abstract 8503

LCMC3 Study: Adverse Eventsa
TRAEs
With ≥ 5% Incidence, n (%)
Safety Population
(N = 101)
Fatigue 20 (20%)
Infusion-related reaction 11 (11%)
Pyrexia 10 (10%)
Decreased appetite 8 (8%)
AST increased 7 (7%)
Nausea 7 (7%)
Arthralgia 6 (6%)
Influenza-like illness 6 (6%)
Diarrhea 5 (5%)
Grade ≥ 3 TRAEs
Pneumonitis 3 (3%)
Nasal congestion 1 (1%)
Decreased lymphocyte count 1 (1%)
Anemia 1 (1%)
Adverse Events, n (%)Safety Population
(N = 101)
All-cause AEs 98 (97%)
Grade 3-4 29 (29%)
Grade 5b 2 (2%)
TRAEs 58 (57%)
Grade ≥ 3* 6 (6%)
Serious AE 30 (30%)
AE leading to treatment
withdrawal5 (5%)
AST, aspartate aminotransferase; TRAE, treatment-related adverse event. a AEs during neoadjuvant treatment. b 2 patients with Grade 5 AE not related to study treatment:
cardiac death post-surgical resection and death due to disease progression.
Data cutoff: September 5, 2018.
Kwiatkowski DJ, ASCO Annual Meeting 2019 Abstract 8503

Days after Cell Injection
Adjuvant vs. Neoadjuvant combo
Neoadjuvant superior
HR=0.33
P=.028
0 1 0 2 0 3 0 4 0 5 0 6 0
0
2 0
4 0
6 0
8 0
1 0 0
3 4 4 S Q O V A+-1 2 9 s v M ic e S u rv iv a l:
N e o a d ju v a n t IO -S u rg e ry A rm # 2
D a y s a fte r tu m o r c e ll in je c tio n
Pe
rc
en
t s
urv
iva
l
N e o a d ju v a n t a n t i-P D -1 +
a n t i-C T L A - 4
A d ju v a n t a n t i-P D -1 +
a n t i-C T L A - 4
Cascone, William WN et al, AACR 2018
**Microscopic lung mets
0
5
1 0
1 5
2 0
2 5
3 0
3 5
4 0
4 5
M ic ro s c o p ic L u n g M e ta s ta s e s
in 3 4 4 S Q -O V A+ N S C L C
Nu
mb
er o
f M
icro
sc
op
ic
Lu
ng
Me
tas
tas
es
/H&
E s
lid
e
N e o a d ju va n t IO -
S u rg e ry a rm
S u rg e ry -
A d ju v a n t IO a rm
IgG
a n ti-C T L A -4
a n t i-C T L A -4 +
a n ti-P D -1
a n ti-P D -1
0
5
1 0
1 5
2 0
2 5
3 0
3 5
4 0
4 5
M ic ro s c o p ic L u n g M e ta s ta s e s
in 3 4 4 S Q -O V A+ N S C L C
Nu
mb
er o
f M
ic
ro
sc
op
ic
Lu
ng
M
eta
sta
se
s/H
&E
s
lid
e
N e o a d ju va n t IO -
S u rg e ry a rm
S u rg e ry -
A d ju v a n t IO a rm
IgG
a n ti-C T L A -4
a n t i-C T L A -4 +
a n ti-P D -1
a n ti-P D -1* *
***
***
Neoadjuvant combined ICB prolongs survival and reduces mets vs. monotherapy or adjuvant combo in a preclinical model of NSCLC
CheckMate 012, a phase I study in stage
IIIB/IV NSCLC pts: higher ORRs and PFS
with combo nivo + ipi vs. nivo monotherapy
Hellmann MD et al, Lancet Oncol. 2017

N= 44
Eligibility NSCLC Stage I-IIIA
N2 single station
(AJCC7th)
Contralateral 2
and/or 4 node eval
to exclude N3
Surgical candidate
ECOG PS 0-1
Stratification Stage
R1:1
Arm B n=21:
Nivolumab
3 mg/kg
D1,15,29 +
Ipilimumab
1 mg/kg D1
D1 D15 D29
D1 D15 D29
Surgery
BIOMARKERS
EVALUATION
Arm A n=23:
Nivolumab
3 mg/kg
D1,15,29
CT
PET/CT
Blood
Stool
Tumor
Uninvolved
lung
CT, PET/CT
Tumor
(Archival/fresh)
Blood, Stool
SOC
Postop therapy
Primary endpoint:
≤10% viable tumor (MPR)
(within 3-6 weeks
after last dose)
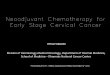
NEOSTAR: phase II study of induction checkpoint blockade for untreated stage I-IIIA NSCLC amenable for surgical resection
Cascone T, William WN, et al. ASCO Annual Meeting 2019 Abstract 8504
NCT03158129
PI: Cascone
co-PI: Sepesi
NCT03158129

Primary endpoint: MPR rate NI meets the pre-specified trial efficacy boundary
Overall ITT
Resected + not resected
Total
n = 44
N
n = 23
NI
n = 21
MPR + pCR 11 (25%)4 (17%)
(95% CI:5%,39%)
7 (33%)
(95% CI:15%,57%)
0% viable tumor (pCR) 8 (18%) 2 (9%) 6 (29%)
1-10% viable tumor 3 (7%) 2 (9%) 1 (5%)
% v
iab
le t
um
or
N (n = 21) NI (n = 16)
Evaluable
Resected on trial
Total
n = 37
N
n = 21
NI
n = 16
MPR + pCR 11 (30%) 4 (19%) 7 (44%)
0% viable tumor (pCR) 8 (22%) 2 (10%) 6 (38%)
1-10% viable tumor 3 (8%) 2 (10%) 1 (6%)
70
N (n = 23) NI (n = 21)
Pre-specified trial efficacy
boundary: ≥ 6 MPRs
Pa
tie
nt
co
un
t
MPR + pCR
>10 % viable tumor
1-10 % viable tumor
0 % viable tumor
20
Median (min, max)
70 (0,100)
Median (min, max)
20 (0,100)
Cascone T, William WN, et al. ASCO Annual Meeting 2019 Abstract 8504

Grade 1-2 TRAE*
N (23) NI (21)
n n/23 (%) n n/21 (%)
Fatigue 8 35% Rash acneiform 11 52%
Rash acneiform 6 26% Fatigue 7 33%
Anemia 3 13% Nausea 7 33%
Hyponatremia 3 13% Cough 6 29%
Diarrhea 2 9% Diarrhea 6 29%
Increased Alanine
Aminotransferase 2 9% Chills 3 14%
Flu like symptoms 2 9% Anemia 2 10%
Headache 2 9% Dyspnea 2 10%
Hypomagnesemia 2 9% Hyperthyroidism 2 10%
Pruritus 2 9% Pruritus 2 10%
Vomiting 2 10%
Grade 3-5 TRAE
N (23) NI (21)
n n/23 (%) n n/21 (%)
Hypermagnesemia (G3) 1 4% Diarrhea (G3) 1 4%
Hypoxia (G3) 1 4% Hyponatremia (G3) 1 4%
Pneumonia (G3)* 1 4%
Pneumonitis (G5)* 1 4%
* From the same patient
* The maximum grade of TRAE from a patient is considered
Median follow-up time after randomization: 8.4 months
Arm A: 1 pt (IIB) died of steroid-treated pneumonitis 4.1 months after randomization
Arm B: 1 pt (IIIA) had PD 2 months after randomization, and died of disease 17 months after randomization
Treatment-related adverse events (TRAEs) and follow up
Cascone T, William WN, et al. ASCO Annual Meeting 2019 Abstract 8504

Neoadjuvant chemotherapy increases expression of PD-L1 vs. untreated tumors
Parra ER, …, William WN et al, JITC 2018

Study design & Endpoints(Within 3 to 8 weeks after
surgical resection)
Mariano Provencio, Hospital Universitario Puerta de Hierro-Majadahonda, Madrid, Spain.
Primary Endpoint:
PFS at 24 months
Secondary Endpoints:
Down-staging rate,
complete resection rate,
ORR, safety, TTP, OS
at 3 years
Study start: April 2017
Enrollment completion: August 2018
Data analysis cut-off: 27th June 2019

1 Two patients were not resected due to their own decision, 3 patients did not fulfill resectability criteria according to the surgeons’ opinion2 Three patients did not receive adjuvant treatment due to toxicity, 1 patient exceeded the time per protocol to start adjuvant treatment
Patient Disposition
Mariano Provencio, Hospital Universitario Puerta de Hierro-Majadahonda, Madrid, Spain.
51 pts assessed for eligibility
46 eligible pts included and received neoadjuvant treatment (ITT)
5 pts did not meet all inclusion/exclusion
criteria
5 pts were not resected after neoadjuvant
treatment1
41 ptsunderwent surgery
37 pts receivedadjuvant treatment
4 pts did notreceive adjuvant treatment2
Patient baseline characteristics N=46 (ITT)
Age (median, range) 63(41-77)
Male, N (%) 34 (74 %)
ECOG PS
0 N (%)
1 N (%)
25 (54%)
21 (46%)
Smoking status, N (%)
Former/current 46 (100%)
Adenocarcinoma, N (%) 28 (61)
Co-morbidities, N (%) 43 (93,5)
N2 33 (89.2)
Multiple station 25 (75.8)

Pathological response
To identify factors influencing pathological response (complete and major) the following potential influencing factors were
considered:
• Comorbidities.
• Clinical stage.
• Tumor size mm
• Primary tumour site (right vs left).
• Histology (adenocarcinoma vs squamous).
• Node involvement (yes/no).
Each one of the factors were compared between the patients with a pathological response.
No statistically significant differences were observed
Mariano Provencio, Hospital Universitario Puerta de Hierro-Majadahonda, Madrid, Spain.
Pathologic response N=41 % (CI 95%)
Major Pathological Response (MPR)
Complete Response (CR)
34/41
24/41
83 (68-93)
59 (42-74)
> 10% residual viable tumor 7/41 17 (7-32)
• Age.
• Gender.
• Performance status.
• Smoking status.
• N2: Unique vs Multiple
• Toxicities
• Nodes N1 vs N2

Outline
• Background and rationale
• Neoadjuvant immunotherapy-based trials• IO monotherapy• IO combo• IO-chemo combo
• Challenges
• Future directions

The optimal cutoff percentage of viable tumor for predicting survival may differ between ADC and SCC in response to NAC
Qu, et al. J Thorac Onc 2019
65% VT correlated with survival in adenocarcinoma
≤10% VT correlated with survival in SCC

Weissferdt A and Pataer A 2019, under revisions
Strong Interobserver Agreement on MPR in NSCLC Patients Receiving Neoadjuvant Chemotherapy

A distinct pattern of immune-mediated tumor regression in NSCLC specimens with MPR to IO, with features of immune activation, tumor cell death, and tissue repair
Adapted from Cottrell TR et al. Ann Oncol. 2018

Neoadjuvant CT and IO are associated with similar histopathological changes compared to untreated resected tumors but result in lower proportions of viable tumor and higher degrees
of fibrosis
Parameter of PTR Untreated cohort
(mean values)
CT cohort(mean values)
IO cohort (mean values)
P value
Viable tumor 66.4% 40.9% 34% 0.0027
Fibrosis 27.4% 45.9% 59.2% 0.0033
Necrosis 6.2% 13.1% 6.6% 0.8817
Inflammation 2.32 1.50 1.85 0.2088
TLS 0.90 0.95 1.00 0.3552
Macrophages 0.10 0.66 0.81 0.0639
LVI 0.26 0.21 0.30 0.9113
Cholesterol clefts 0.083 0.87 0.91 0.0003
Giant cells 0.35 0.75 0.65 0.0300
Neovascularization 0.05 0 0.10 0.3679
Weissferdt A et al., ESMO Congress 2018

TMB and PD-L1 correlations with MPR and pathological regression in neoadjuvant ICI studies
n = 68
ρ = −0.24a
P = 0.04
Kwiatkowski DJ, ASCO 2019 Abstract 8503
(n = 40) (n = 10)
P =
0.48a
TMB by MPR (n = 50)
Forde P et al, NEJM 2018

Elevated baseline tumor PD-L1 expression is associated with radiographic and pathologic responses in NEOSTAR
Tina Cascone, MD, PhD
Ba
se
lin
e %
PD
-L1
CR/PR SD/PD
60
80
40
20
0
P = 0.015
Baseline % PD-L1 and RECIST responses
% v
iab
le t
um
or
<1% >1%
60
80
100
40
20
0
Baseline % PD-L1
P = 0.046
Baseline % PD-L1 and % viable tumor
Baselin
e %
PD
-L1
MPR No MPR
60
80
40
20
0
P = 0.015
Baseline % PD-L1 and MPR
Cascone T, William WN, et al. ASCO Annual Meeting 2019 Abstract 8504

Nivo plus Ipi combo is associated with increased T cell repertoire diversity and reactivity in the tumor at surgery
Reuben A. et al, ASCO 2019 Abstract 8532
Tu
mo
r rich
ne
ss s
urg
ery
Blood richness baseline
R = 0.82
P = 0.023
10000 30000 50000 70000
0
5000
10000
15000
G0
Tum
or S
N
NI
Uninvolved
lung
Resected
tumor
Clo
na
lity
Ric
hn
ess
Uninvolved
lung
Resected
tumor
Div
ers
ity
Reacti
vit
y
Ric
hn
ess
Pre-
therapy
Pre-
therapy
Surgery Surgery
N NI
Pre-
therapy
Pre-
therapy
Surgery SurgeryC
lon
alit
y
N NI
Div
ers
ity
Re
ac
tivit
y
Cascone T, ASCO Annual Meeting 2019 Abstract 8504

Early ctDNA clearance is associated with pathologic response to anti-PD1 therapy in early-stage NSCLC
Anagnostou V, Forde P et al, Cancer Res 2019
Updated long-term follow up following neoadjuvant nivolumab:• At median follow up of 30 m, 15/20 pts are
disease-free and alive. 2 pts have died, 1 of disease relapse.
• Median RFS unreached. The 24m RFS rate is 69% (95% CI: 51-93).
• Presence of ctDNA at diagnosis and MPR do not associate with RFS.
Reuss JE et al, J Clin Oncol 37, no. 15_suppl, 2019 Abstract 8524

Outline
• Background and rationale
• Neoadjuvant immunotherapy-based trials• IO monotherapy• IO combo• IO-chemo combo
• Challenges
• Future directions

NEOSTAR: a platform phase II study to test induction checkpoint blockade-based strategies for untreated and resectable stage I-IIIA NSCLC
NCT03158129
N total = 44
Eligibility
NSCLC Stage I-
IIIA (AJCC7th)
Surgical
Candidate
Stratification
Stage
Surgery
R1:1
Arm B:
Nivolumab
3 mg/kg
D1,15,29 +
Ipilimumab
1 mg/kg D1
D1 D15 D29
D1 D15 D29
SurgeryWithin 8 weeks
post surgery
Within 8 weeks
post surgery
Arm A:
Nivolumab
3 mg/kg
D1,15,29
SOC
Postop therapy
SOC
Postop therapy
Primary endpoint:
≤10% viable tumor (MPR)Arm C:
Nivolumab
360 mg IV +
Chemotherapy
IV q3 weeks
X 3 cycles
D1 D22 D43
SurgeryWithin 8 weeks
post surgery
SOC
Postop therapy
N = 22
Eligibility
NSCLC
Stage IB (≥4cm)-
IIIA (AJCC 7th)
Surgical
Candidate PI: Cascone
co-PI: Sepesi
Primary endpoint:
≤10% viable tumor (MPR)

Surgical
resection
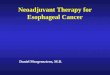
Arm D: Durvalumab 1500 mg IV + danvatirsen
200 mg IV
Arm A: Durvalumab 1500 mg IV monotherapy
Patients stratified by
lymph node
involvementR
an
do
miz
e 1
:1:1
:1
(up
to
40
pa
tie
nts
pe
r a
rm)
Week 0 Week 1 Week 2 Week 3 Week 4
ECOG PS, Eastern Cooperative Oncology Group performance
status; NSCLC, non-small-cell lung cancer
Days 29 to
42
Follow-up
Day 105
Durv
alu
mab
Durv
alu
mab
Danvatirs
en
Danvatirs
en
Danvatirs
en
Danvatirs
en
Danvatirs
en
Danvatirs
en
Danvatirs
en
Arm B: Durvalumab 1500 mg IV +
oleclumab 3000 mg IV
Durv
alu
mab
Ole
clu
mab
Ole
clu
mab
Arm C: Durvalumab 1500 mg IV + monalizumab
750 mg IV
Durv
alu
mab
Monaliz
um
ab
Monaliz
um
ab
Tumor sample obtained
prior to treatment
Resectable, early
stage
(I [> 2 cm] to IIIA)
NSCLC
ECOG PS 0/1
NeoCOAST: Platform study testing the safety and activity of neoadjuvant Durvalumab with or without novel immunotherapies
Primary endpoint
MPR rate
Secondary endpoints
Feasibility of surgery within planned window
Safety: AEs, SAEs etc.
pCR rate, PK, ADAs
Garcia Campelo R, Cascone T et al, WCLC 2019, P2.04-28

Trial identifier Phase Sponsor Stage Intervention/Disease space Primary endpoint
NCT02259621 (NA_00092076) 2 Sidney Kimmel Comprehensive Cancer Center
IB–IIIA Nivo with or without ipi Safety and feasibility
NCT02818920 (TOP 1501) 2 Duke University Medical Center IB–IIIA Pembrolizumab (neoadjuvant and adjuvant) Surgical feasibility rate
NCT02927301 (LCMC-3) 2 Genentech IB–IIIA Atezolizumab (neoadjuvant and adjuvant) MPR
NCT02572843 2 Swiss Group for Clinical Cancer Research
IIIA (N2) Durvalumab (neoadjuvant, following chemotherapy, and adjuvant)
EFS
NCT03794544 (NeoCOAST) 2 MedImmune I [> 2 cm]-IIIA Durvalumab with or without novel I-O agents MPR
NCT03158129 (NEOSTAR) 2 MD Anderson Cancer Center I–IIIA Nivo with or without ipi or chemo MPR
NCT03197467 (NEOMUN) 2 AIO-Studien-gGmbH II-IIIA Pembrolizumab (neoadjuvant) Feasibility, safety, clinical, path responses
NCT03081689 (NADIM) 2 Spanish Lung Cancer Group IIIA (N2) Nivolumab, carboplatin, paclitaxel PFS
NCT03838159(NADIM II)
2 Fundación GECP IIIA/IIIB (T3N2) Neoadjuvant Nivo, Paclitaxel, Carbo and adjuvant Nivo vs. neoadj Paclitaxel, Carbo
pCR
NCT02716038 2 Columbia University IB-IIIA Neoadjuvant Atezo, Carbo, Nab-paclitaxel MPR
NCT03237377 2 Sidney Kimmel Comprehensive Cancer Center
IIIA Neoadjuvant Durvalumab/RT or Durvalumab/Tremelimumab/RT
Toxicities, Feasibility of Preoperative ImmunoRT
NCT02904954* 2 Weill Medical College of Cornell University
I-IIIA Durvalumab With or Without SBRT DFS
NCT02998528 (CheckMATE 816) 3 Bristol-Myers Squibb IB-IIIA Nivo plus ipi or chemotherapy vs. chemo EFS and pCR rate
Selected ICI trials in the neoadjuvant/perioperative space for resectable NSCLC
https://clinicaltrials.gov/
*Altorki et al., IASLC 2019, P2.04-92: 34 pts randomized to Durva vs. Durva+SBRT: Grade 3/4 AEs: 11%. Resectability rate: 88% (30/34; 28R-0:87%). Grade 3/4 perioperative AEs: 31% (10/32). MPR Arm-2: 47% (8/17) vs. 0 in Arm-1. Excluding 4 EGFR mutant pts, MPR 61.5% (8/13%) in Arm-2.

Ongoing phase 3 periadjuvant studies with I-O in resectable NSCLC
Key Eligibility Criteria
• Stage II-III* resectableNSCLC
• ECOG PS 0–1
I-O +Chemotherapy
4 cycles†
I-O
13-16 cycles†
Chemotherapy† Placebo/BSC
Surgery
R
Surgery
Checkmate 77T1 KEYNOTE-6712 IMpower0303 AEGEAN4,5
I-O agent Nivolumab Pembrolizumab Atezolizumab Durvalumab
Primary endpoint(s) EFS EFS, OS MPR, EFS MPR
PCD May 2023 Jan 2024 March 2025 July 2020
Stages II-IIIB‡ II-IIIB‡ II-IIIB‡ IIA-IIIB‡
Target enrollment 452 786 374 300
*Stages included differ between trials. †Dosage, timing, duration, and chemotherapy backbones differ between trials; information not available for Checkmate 77T or AEGEAN. ‡Includes stages IIIB patients with N2 disease that is considered resectable.1. Clinicaltrials.gov. NCT04025879. Accessed August 7, 2019. 2. Clinicaltrials.gov. NCT03425643. Accessed August 7, 2019. 3. Clinicaltrials.gov. NCT034056063. Accessed August 7, 2019. 4. Clinicaltrials.gov. NCT03800134. Accessed August 7, 2019. 5. Heymach JV et al. Poster presentation at WCLC 2019. P1.18-02.

Trial identifier Phase Sponsor Stage Intervention Primary endpoint
NCT02595944(ANVIL)
3 National Cancer Institute (NCI)
IB–IIIA Nivolumab DFS, OS
NCT02486718(IMpower010)
3 Hoffmann-La Roche IB–IIIA Atezolizumab DFS
NCT02273375 (BR31)
3 Canadian Cancers Trials Group
IB-IIIA Durvalumab DFS
NCT02504372 (KEYNOTE-091) (PEARLS)
3 EORTC, Merck IB–IIIA Pembrolizumab DFS
NCT03053856 2 Samsung Medical Center
IIIA (N2) Pembrolizumab DFS
NCT03447769CANOPY-A
3 Novartis Pharmaceuticals
IIA-IIIA and IIIB (T > 5cm N2) completely resected
Canakinumab or placebo
DFS
Selected ICI trials in the adjuvant space for operable NSCLC
https://clinicaltrials.gov/

ALCHEMIST Adjuvant ICI trial post ANVIL
Study Chair: Jacob Sands - ALLIANCE
Courtesy of Jacob Sands

ICI trials in the perioperative space: what we have learned and future directions
Role of neoadjuvant/perioperative ICIs for stage I-III resectable NSCLC
Best therapy timing, # doses, sequence vs combination, spatiotemporal modulation of the immune TME by therapy are under investigation (preclinical models as platform)
Investigate safety/feasibility and activity of novel neoadjuvant IO-based combinations: STING agonists, intratumoral IOs, anti-CTLA-4-based combos?
Biomarker discovery/patient selection in neoadjuvant studies: PD-L1, TMB, scRNA-seq, ctDNA, microbiome, oncogenic drivers, TCR/neoantigen repertoire, sex/age, radiomics
Validation of surrogate clinical endpoints in phase 3 studies
Harmonization/standardization of methods for path response assessment (tumor, nodes) Does type of therapy matter? Does histology matter? Guidelines being developed by IASLC Interobserver agreement on path responses: IASLC efforts; industry-academia collaboration; FDA input/guidance MPR in IIT population vs. resected patients only, exclusion of oncogenic drivers
Surgical challenges after neoadjuvant therapies