Embed Size (px)
Citation preview

Immunology 1984 52 181
Immunolocalization of complement component C9 on necrotic and non-necroticmuscle fibres in myositis using monoclonal antibodies: a primary role
of complement in autoimmune cell damage
B. P. MORGAN*, C. A. SEWRYt, K. SIDDLEI, J. P. LUZIOI & A. K. CAMPBELL* *Department ofMedical Biochemistry, Welsh National School of Medicine, Heath Park, Cardiff, tJerry Lewis Muscle ResearchCentre, Hammersmith Hospital, Ducane Road, London, and tDepartment of Clinical Biochemistry, Addenbrooke's
Hospital, Hills Road, Cambridge
Acceptedfor publication 25 November 1983
Summary. Monoclonal antibodies to human comple-ment component C9 were used to localise the mem-brane attack complex (MAC) of human complementon muscle fibres from patients with autoimmunemyositis. A pigeon erythrocyte 'model' system wasused to screen the available monoclonal antibodies fortheir ability to bind C9 after its insertion into theMAC. Three of the five antibodies tested were demon-strated, using radioiodine- or rhodamine-labelledsecond antibody, to bind. The antibody giving maxi-mum binding in this system was used to demonstratethat MACs were present on histologically normal aswell as on necrotic fibres in myositis. No binding wasseen in muscle from control subjects. These resultssuggest a primary role of complement in the patho-genesis of muscle fibre necrosis in myositis.
INTRODUCTION
Since the first description ofantibodies against thyrog-lobulin in the sera ofpatients with thyroiditis by Roittet al. (1956), autoantibodies to tissue antigens havebeen demonstrated in many diseases. Autoantibodiesto the cell membrane may fix complement (Bottazzo etal., 1980), causing cell damage. However, the investi-Correspondence: Dr B. P. Morgan, Dept. of Medical
Biochemistry, Welsh National School of Medicine, HeathPark, Cardiff CF4 4XN.
gation ofthe role ofcomplement in the pathogenesis ofthese diseases has been mainly limited to studies of theearly components. It has been proposed that themembrane attack complex (MAC) of complementmay cause morphological and chemical changes incells before or in the absence of lysis in autoimmunediseases (Campbell & Luzio, 1981). In order to test thishypothesis, it is necessary to establish that the MACoccurs on both non-necrotic and necrotic cells. To dothis, reagents which can identify the MAC in tissuesare required. Several studies have demonstrated thebinding of polyclonal antibodies to the terminalcomponent of human complement, C9, after itsinsertion into the MAC (Rauterberg, Ungemach &Gebest, 1979; Sahashi et al., 1980), but others havebeen unable to demonstrate binding (Rommel &Mayer, 1973; Boyle& Borsos, 1980). Using polyclonalantisera raised to neoantigens of the purified MAC,several groups have demonstrated MAC binding intissues in a variety of diseases, including systemiclupus erythematosus nephritis (Biesecker, Katz &Koffler, 1981), multiple sclerosis (Bozsik, 1983) andmuscle diseases (Engel & Biesecker, 1982). Sahashi etal. (1980) identified C9 at the motor end plate inacquired autoimmune myasthenia gravis, providingevidence of complement-mediated injury of the post-synaptic region in this disease. Engel & Biesecker(1982) demonstrated C9 binding to necrotic fibres in avariety of muscle diseases. However, they did not
181

B. P. Morgan et al.
demonstrate C9 or MAC binding to non-necroticfibres, and therefore concluded that complementbinding was a secondary event in muscle fibre necrosis.Thus the factors initiating necrosis and the subsequentevents leading to necrosis have yet to be determined.We have recently reported the production of
monoclonal antibodies to human C9 (Morgan et al.,1983b), and have used these antibodies to develop amethod for its immunopurification and a highlysensitive immunoradiometric assay (Morgan et al.,1983a). The aim of the work reported here was todemonstrate whether any of these monoclonal anti-bodies bound to C9 after its insertion into the MAC,and to use these antibodies for the immunolocaliza-tion of C9 in a pathological condition in whichcomplement activation is thought to occur. Thepigeon erythrocyte was used (Campbell, Daw &Luzio, 1979) to characterize antibody binding tomembrane-bound C9, and the antibody giving maxi-mum binding in this system was used for the immuno-localization of C9 in muscle from patients withautoimmune myositis.
MATERIALS AND METHODS
ChemicalsNa['25I] (IMS 30) was obtained from AmershamInternational, Amersham, Bucks, U.K. lodogen wasobtained from Pierce and Warriner Ltd., Chester,U.K. All other chemicals were obtained from BDHChemicals, Poole, Dorset and were of the best gradeavailable.Medium A contained 0- 14 M sodium chloride, 0 005
M potassium chloride, 0-002 M magnesium chlorideand 0-01 M N-Tris-(Hydroxymethyl)-methyl-2-aminoethanesulphonic acid (TES), adjusted to pH 7-4with NaOH.
AntiseraAntiserum to pigeon erythrocytes was produced inguinea-pigs by immunization with pigeon erythro-cytes, as previously described (Campbell et al., 1979).A sheep antiserum to mouse immunoglobulins wasproduced by immunization of sheep by standardmethods. An IgG preparation was made from thisantiserum by sodium sulphate precipitation and waslabelled with 125I by the method of Fraker & Speck(1978). Goat anti-mouse immunoglobulin antibodylabelled with rhodamine was purchased from TagoInc. Immunodiagnostics, Burlingame, CA, U.S.A.
Monoclonal antibodiesMonoclonal antibodies to human C9 were producedas previously described (Morgan et al., 1983b). Fivemonoclonal antibodies were produced in quantity andstudied in detail, coded C9-8, C9-34, C9-36, C9-42 andC9-47. A monoclonal antibody produced at the sametime, but shown not to bind C9, was used as a controlin all experiments ('control' monoclonal antibody).
Purification of C9Human C9 was purified from plasma by immunoaf-finity chromatography as previously described (Mor-gan et al., 1983b).
Serum and C9-depleted serumSerum was obtained from normal volunteers andstored in aliquots at -70° prior to use. Serumspecifically depleted of C9 was produced by adsorp-tion of serum on a column of immobilized antibody toC9 as previously described (Morgan et al., 1983b).
Pigeon erythrocytes and intermediatesFresh pigeon blood anticoagulated with heparin wasobtained by bleeding pigeons from the wing vein. Theerythrocytes (E) were extensively washed in MediumA and stored on ice in Medium A at a cell concentra-tion of 1/10. Antibody-coated erythrocytes (EA) wereproduced by incubating the washed Es in Medium Awith a 1/100 dilution of heat-treated guinea-pig anti-pigeon E antiserum for 5 min at 37°. The EAs werewashed in Medium A, and stored on ice in MediumA+ 1 mm CaCl2. Erythrocyte intermediates coatedwith the complement components up to C8 (EA-C5-8)were produced by incubation of EAs with a 1/5dilution of C9-depleted serum (NHS-C9) for 3 min at37°. The EA-C5-8s were washed and stored on ice inMedium A. Erythrocyte intermediates coated with thecomplete sequence of complement components(EA-C5-9) were prepared by incubation of EA-C5-8swith pure C9 at a final dilution of 50 yg ml-' inMedium A at 0° for 5 min. Incubation was carried outat 0° to minimize the temperature-dependent lysis ofthe EA-C5-9 intermediates (Burakoff, Mantz & Bena-cerrof, 1975). The EA-C5-9s were washed in ice-coldMedium A and stored on ice. The completeness ofintermediate production was assessed at each stage byincubation of a portion of the intermediate with theappropriate complement source at 370 for 15 min andmeasuring the degree of haemolysis. Controls in-cluded incubation of Es with serum, and EAs withpure C9.
182

C9 on necrotic and non-necrotic musclefibres
Assessment of binding ofmonoclonal antibodiesEach intermediate was incubated on ice for 15 minwith each monoclonal antibody at equivalent dilutions(about 1O pg ml-I in Medium A). The intermediateswere washed in Medium A at 0° and a dilution of125I-labelled sheep anti-mouse immunoglobulin anti-body sufficient to give about 105 d.p.m. per tube wasadded. After a further 15 min incubation at 00, theintermediates were washed and the radioactivity in thewashed cell pellet measured in a Nuclear EnterprisesNE1600 Gamma Spectrometer. Intermediates simi-larly incubated with monoclonal antibody and washedwere incubated at 00 for 15 min with rhodamine-labelled goat anti-mouse immunoglobulin antibodydiluted 1/20 in Medium A. After washing, boundfluorescence was assessed using a fluorescence micro-scope. Smears of intermediates were also made onmicroscope slides and fixed by immersion in methanolfor 15 sec. Enough of a dilution of monoclonalantibody (10 pg ml-' in phosphate-buffered saline[PBS]) to cover the smear was then placed on the slideand incubated at room temperature for 15 min. Theslides were washed extensively in PBS and enough of a1/50 dilution of rhodamine-labelled goat anti-mouseimmunoglobulin antibody to cover the smear placedon the slide. After a further 15 min incubation, theslides were again washed extensively and boundfluorescence assessed using a fluorescence microscope.
Controls in each case included the preincubation ofthe primary antibody with C9 and the omission ofeither the primary or secondary antibody. The dilu-tions and incubation times used were selected inpreliminary experiments.
Muscle biopsiesMuscle biopsies were obtained from four patients withmyositis, aged 8, 9, 25 and 66 years. Two ofthese (aged8 and 25 years) had dermatomyositis, and the othertwo had polymyositis. All patients had clinical andhistopathological features of myositis, and elevatedserum creatine kinase. Biopsies were also obtainedfrom two control subjects with histochemically andhistologically normal muscle. All biopsies wereobtained from the quadriceps muscle under localanaesthesia using the Bergstrom needle technique asdescribed by Edwards (1973). All samples were rapidlyfrozen in 'Arcton 12' (ICI) at - 150° in preparation forhistological and immunochemical examination. Cryo-stat sections (10 pm) were cut at - 20° and placed oncoverslips.
Preliminary studies involved testing binding of each
of the monoclonal antibodies at varying dilutions tothe sections, using rhodamine-labelled or biotin-labelled second antibody to detect binding. Monoc-lonal antibody C9-47 at a dilution of 1/200 (10 pgml-') gave the best binding in C9-positive sections,and was thus chosen for the remainder of the study.Enough of this antibody to cover the section wasplaced on the coverslip and incubated at room tem-perature for 45-60 min. After extensive washing inPBS, enough of a 1/50 dilution of rhodamine-labelledgoat anti-mouse immunoglobulin antibody to coverthe section was placed on the coverslip and incubatedfor a further 45-60 min at room temperature. Thecoverslips were then washed in PBS and mounted inUVinert (Gurr). Bound fluorescence was detectedusing a fluorescence microscope (Zeiss).
Controls included the substitution of 'control'monoclonal antibody for C9-47: pretreatment ofC9-47 with C9: and omission of either the primary orsecondary antibody.
Localization ofC9 in sections ofmuscle using C9-47was also attempted using a biotin-avidin-peroxidasesystem. The second antibody used was a biotinulatedgoat anti-mouse immunoglobulin antibody and bind-ing of second antibody was detected using an avidin-peroxidase complex and diaminobenzidine (Hsu,Raine & Fanger, 1981).
Serial sections of each biopsy were stained with avariety of techniques to demonstrate histological andhistochemical features (Dubowitz & Brooke, 1973).
RESULTS
Monoclonal antibody binding to the MAC on pigeonerythrocytesIn order to discover which monoclonal antibodieswere capable of binding to membrane-bound C9, theMAC was formed on pigeon erythrocytes underconditions which inhibited lysis (< 20%), and a doub-le-antibody technique used to quantify C9 binding.Using an 'l25-labelled sheep anti-mouse immunog-
lobulin second antibody it was demonstrated, asshown in Table 1, that of the five monoclonalantibodies to C9, three bound strongly to the MAC.Of the remaining two antibodies, C9-8 bound weaklyto the MAC, and only C9-34 failed to bind. None ofthe antibodies bound significantly to any of the otherintermediates. Preincubation of pigeon erythrocyteswith serum, or antibody-coated pigeon erythrocytes(EA) with pure C9, produced no binding of monoc-
183

B. P. Morgan et al.
Table 1. Monoclonal antibody binding to pigeonerythrocyte intermediates
Antibody
Intermediate C9-8 C9-34 C9-36 C9-42 C9-47
E 147 154 99 129 151EA 132 153 121 209 221EA-C5-8 108 215 219 112 97EA-C5-9 854 212 4378 5720 7987
A double-antibody technique was used, usingC9-47 as first antibody and 1251-labelled sheepanti-mouse antibody as second antibody, as detailedin the text. The counts bound in the washed cellpellet were measured. Results are expressed ascounts bound in each case (mean of triplicatedeterminations).
lonal antibody. Thus, the MAC components up to C8were necessary for C9 binding, indicating that C9 wasincorporated into the MAC, and not non-specificallybound to the cell. Preincubation of the monoclonalantibody with pure C9 abolished monoclonal anti-body binding to C9-positive intermediates.An identical pattern of uptake of monoclonal
antibody was demonstrated using a rhodamine-labelled second antibody. Cell-surface fluorescencewas only detectable when antibodies C9-36, C9-42 andC9-47 were incubated with EA C5-9 intermediates.C9-47 appeared to give the best labelling in thissystem. Figure 1 shows the labelling obtained usingC9-47 as first antibody, with EA C5-8 or EA C5-9intermediates. Preincubation of the monoclonal anti-body with C9, or omission of first antibody, abolishedfluorescence uptake. Fixation of intermediates withmethanol prior to incubation with the monoclonalantibody reduced, but did not abolish, uptake ofantibody and subsequent fluorescent labelling.
*:
....... . . .:.
.. .... ..... . ;.N, . ...
0B
.. .. ..* .:. :: ::
.... .. ...t S. ..... .... :... ^ i }. .} .tB 3 X w
:. :.X*es : .... : . . *er
8. : :::
X
......
.. :>:
Figure 1. Pigeon erythrocytes coated with the complement components up to C8 (EA-C5-8) or with the complete sequence ofcomplement components (EA-C5-9) were used in a double-antibody immunofluorescence study, using C9-47 as first antibody,and rhodamine-labelled goat anti-mouse immunoglobulin antibody as second antibody. (a) and (b) show EA-C5-9s viewed byphase contrast, and fluorescence microscopy respectively. (c) and (d) show EA-C5-8s viewed in the same way.
184

C9 on necrotic and non-necrotic muscle fibres
Monoclonal antibody binding to human muscle
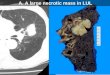
Initial screening of the monoclonal antibodiesrevealed that, as with the pigeon erythrocyte, monoc-lonal antibodies C9-36, C9-42 and C9-47 bound toC9-positive muscle sections. The best staining andlowest background was obtained using C9-47 at adilution of 1/200 (10 ug ml- '). Using this antibody C9was detected in all sections of muscle from patientswith myositis. Three distinct types ofC9 binding wereseen. Firstly, C9 was detected in small necrotic fibres,the whole fibre straining vividly (Fig. 2a). These'bright fibres' occurred singly and in groups through-out the sections. Histological examination of serialsections confirmed the necrotic nature of these fibres.Necrotic fibres were identified by the clumping of
myofibrils, loss of eosin and trichrome staining, andsometimes invasion by macrophages. Secondly, C9was demonstrated as a bright rim at the periphery oflarge fibres (Fig. 2b; N). These fibres showed patchystaining with haematoxylin and eosin (Fig. 2c; N) andwere probably hypercontracted fibres in theearly stagesof necrosis. The third type of C9 binding was demon-strated as discrete patches on the surface ofsome fibreswhich did not appear to be necrotic and showed nogross histological abnormality (Fig. 2d, f; *).No C9 binding was demonstrated in undiseased
muscle, and preincubation of muscle sections with C9caused no increase in staining. Preincubation ofC9-47with pure C9 abolished staining (Fig. 2e). Omission offirst or second antibody, or substitution of the controlantibody for C9-47 also abolished staining. C9-speci-
Figure 2. Cryostat sections ofmuscle from a patient with myositis stained with a double-antibody immunofluorescence method(a, b, d and e) and with haematoxylin and oesin (c and f). (a) C9 in a small necrotic fibre ('bright fibre') (magnification x 255). (b)C9 localized to the periphery of a large fibre (N) (magnification x 255). (c) Serial section to (c) stained with haematoxylin andeosin, showing variation in staining intensity in fibre (N), suggesting that it is in the early stages of necrosis (magnificationx 170). (d) C9 in discrete patches (arrowed) on the surfaces of four fibres (*) (magnification x 255). (e) Serial section to (d)stained with C9-47 preincubated with C9, demonstrating the loss of rhodamine labelling on these fibres (*) (magnificationx 255). (f) Serial section to (d) and (e) stained with haematoxylin and eosin, showing the non-necrotic appearance of the samefibres (*) (magnification x 170).
185

B. P. Morgan et al.
fic fluorescence was easily distinguishable from theautofluorescence apparent in all muscle sections, asthe latter persisted on removal of the rhodamine filter.
Perioxidase staining using C9-47 as first antibodygave similar results, though interpretation was compli-cated by the high level ofendogenous peroxidase in thesection.
DISCUSSION
We have demonstrated that C9 can be identified oncells using monoclonal antibodies raised to nativehuman C9. Incubation of erythrocytes with C9 in theabsence of the early components of the MAC, orincubation of muscle sections with C9, caused nobinding of monoclonal antibody, indicating that theC9 identified in this study is incorporated into theMAC, and not non-specifically bound to the cellsurface.Of five monoclonal antibodies produced to native
C9, three have been demonstrated to interact withmembrane-bound C9. This finding is surprising inview of the problems encountered by other groups indemonstrating interaction of polyclonal anti-C9 anti-body with C9 once cell-bound (Boyle & Borsos, 1980).The inability of these workers to demonstrate anti-body binding led to the proposal that C9 was insertedinto the membrane, thereby masking most of theantigenic determinants. Our findings do not necess-arily contradict this proposal, as we have merelydemonstrated that at least some of the antigenicdeterminants of native C9 are still accessible toantibodies after C9 incorporation in the MAC. Thedemonstration that only about 25% of the C9 mole-cule is inaccessible to enzymatic digestion after inser-tion into the MAC supports this view (Hammer et al.,1977).
It has previously been reported, using polyclonalantisera to C9 or to neo-antigens of the MAC, that theMAC is present only on severely necrotic fibres inmuscle diseases (Engel & Biesecker, 1982). This led tothe proposal that MAC binding merely acts as apropagator, and not as an initiator of necrosis. Using amonoclonal antibody which interacts with cell-boundC9 we have demonstrated the presence of MACs onhistologically normal fibres and fibres in the earlystages of necrosis, as well as on severely necrotic fibresin autoimmune myositis (Fig. 2). This implies that, inthis condition, complement may be the primary factor
initiating muscle necrosis. It is likely that the improvedsensitivity and specificity afforded by monoclonalantibodies is responsible for this difference in findings.
In all disorders involving muscle fibre necrosis,necrotic fibres are denuded of plasma membrane(Schmalbruch, 1975; Carpenter & Karpati, 1979) andit has been suggested that, in Duchenne musculardystrophy, plasma membrane loss is the basic abnor-mality (Mokri & Engel, 1975). Complement is knownto cause an increase in lipid turnover in nucleated cells(Schlager, Ohanian & Borsos, 1978) and it has beensuggested that these cells have the capacity to recoverfrom complement attack by endocytosis or exocytosisof membrane regions bearing MACs (Richardson &Luzio, 1980; Campbell & Luzio, 1981; Ramm et al.,1983). Thus, in muscle disease, complement may beresponsible for the plasma membrane loss observed,necrosis occurring when membrane loss exceeds thecapacity of the fibre to replace it.We have previously demonstrated that the earliest
detectable event on binding of the MAC is a rapid risein intracellular free calcium (Campbell et al., 1979).Thus, the changes in intracellular calcium observed inboth necrotic and non-necrotic fibres in muscle dis-eases (Oberc& Engel, 1977; Bodsteiner& Engel, 1978)could be mediated by the MAC. The increasedintracellular calcium may be important in propagatingevents leading to fibre necrosis (Busch et al., 1972)by inhibition of mitochondrial respiratory activity(Wrogemann, Blanchaer & Jacobson, 1979), acti-vation of proteases (Azana, Raymond & Robin,1979), depolymerization of microtubules (Schliwa,1976) and saturation ofthe calcium uptake capacity ofthe sarcoplasmic reticulum (for review, see Campbell,1983).In summary, we have demonstrated, using a monoc-
lonal antibody to C9 which interacts with C9 after itsincorporation into the MAC, that C9 is present onboth necrotic and non-necrotic fibres in myositis. Wetherefore propose that the MAC is a primary factor inthe causation of muscle fibre necrosis in myositis.
It is now necessary to investigate whether C9binding is demonstrable on non-necrotic fibres inother muscle diseases where changes in intracellular ornuclear calcium have been implicated (Maunder-Sewry & Dubowitz, 1979), but the primary lesion hasnot been demonstrated. Finally, investigation of C9binding to non-necrotic, but morphologically or func-tionally abnormal, cells in other autoimmune diseases(Goudie, 1980) may identify the MAC as a primaryfactor in pathogenesis.
186

C9 on necrotic and non-necrotic muscle fibres 187
ACKNOWLEDGMENTS
B.P.M. is an MRC training fellow; C.A.S. is funded bythe Muscular Dystrophy Group of Great Britain. Wethank the Arthritis and Rheumatism Council for agrant to J.P.L. for the preparation of monoclonalantibodies to C9, and a project grant to A.K.C. K.S. isa Wellcome Trust Senior Lecturer.
REFERENCES
AZANA J.L., RAYMOND J. & ROBIN J.M. (1979) Purificationand some physiochemical and enzymatic properties of acalcium ion-activated neutral proteinase from rabbitskeletal muscle. Biochem. J. 183, 339.
BIESECKER G., KATZ S. & KOFFLER D. (1981) Renal localisa-tion of the membrane attack complex in systemic lupuserythematosus nephritis. J. exp. Med. 154, 1779.
BODSTEINER J.B. & ENGEL A.G. (1978) Intracellular calciumin Duchenne dystrophy and other myopathies: a study of567000 muscle fibres in 114 biopsies. Neurology, 28, 439.
BorrAzzo G.F., DEAN B.M., GORSUCH A.M., CUDWORTHA.G. & DONIACH D. (1980) Complement-fixing islet-cellautoantibodies in Type I diabetes: possible monitors ofactive beta-cell damage. Lancet, i, 668.
BOYLE M.D.P. & BoRsos T. (1980) The terminal stages ofimmune haemolysis: a brief review. Molec. Immunol. 17,425.
BoZSIK B.P. (1983) Demonstration of an autoantibodybinding to human membrane attack complex. Immuno-biology, 164, 215.
BURAKOFF S.J., MANTZ E. & BANACERROF S. (1975) Is theprimary complement lesion insufficient for lysis? Failureof cells damaged under osmotic protection to lyse inEDTA or at low temperatures after removal of osmoticprotection. Clin. Immunol. Immunopath. 4, 108.
BUSCH W.A., STROMER M.H., GOLL D.E. & SUZUKI A. (1972)A Ca2+-specific removal of Z-lines from rabbit skeletalmuscle. J. Cell Biol. 52, 367.
CAMPBELL A.K. (1983) Intracellular Calcium: its UniversalRole as Regulator. John Wiley, Chichester.
CAMPBELL A.K., DAW R.A. & Luzio J.P. (1979) Rapidincrease in intracellular free Ca2+ induced by antibodyplus complement. FEBS Lett. 107, 55.
CAMPBELL A.K. & LUZIO J.P. (1981) Intracellular calcium asa pathogen in cell damage initiated by the immunesystem. Experientia, 37, 1110.
CARPENTER S. & KARPATI G. (1979) Duchenne musculardystrophy: plasma membrane loss initiates cell necrosisunless it is repaired. Brain, 102, 147.
DUBOWITZ V. & BROOKE M.H. (1973) Muscle Biopsy: aModern Approach. Saunders, London.
EDWARDS R.H.T., MAUNDER C.A., LEWIS P.D. & PEARSEA.G.E. (1973) Percutaneous needle biopsy in the diag-nosis of muscle diseases. Lancet, ii, 1070.
ENGEL A.G. & BIESECKER G. (1982) Universal involvement ofcomplement in muscle fibre necrosis. In: Disorders of theMotor Unit, (ed. D. L. Schotland), p. 535. Wiley Medical.
FRAKER P.J. & SPECK J.C. (1978) Protein and cell membraneiodination with a sparingly soluble chloramide, 1, 3, 4,6-tetrachloro-3a, 6a diphenylglycouril. Biochem. biophys.Res. Commun. 80, 849.
GOUDIE R.B. (1980) Autoimmune thyroiditis. In: Muir'sTextbook of Pathology (ed. J. R. Anderson), 1022.Arnold.
HAMMER C.H., SHIN M.L., ABRAMOVITZ A.S. & MAYERM.M. (1977) On the mechanism of cell membranedamage by complement: evidence on insertion of poly-peptide chains from C8 and C9 into the lipid bilayer oferythrocytes. J. Immunol. 119, 1.
Hsu S-M., RAINE L. & FANGER H. (1981) Use of avidin-bio-tin-peroxidase complex (ABC) in immunoperoxidasetechniques. J. Histochem. Cytochem. 29, 577.
MAUNDER-SEWRY C.A. & DUBOWITZ V. (1979) Myonuclearcalcium in carriers of Duchenne muscular dystrophy: anX-ray microanalysis study. J. neurol. Sci. 33, 323.
MOKRi B. & ENGEL A.G. (1975) Duchenne dystrophy:electron microscopic findings pointing to a basic or earlyabnormality in the plasma membrane of the muscle fibre.Neurology, 25, 1111.
MORGAN B.P., CAMPBELL A.K., Luzio J.P. & SIDDLE K.(1983a) Immunoradiometric assay for human comple-ment component C9 utilising monoclonal antibodies.Clin. chim. Acta, 134, 85.
MORGAN B.P., DAW R.A., Luzio J.P., SIDDLE K. & CAMP-BELL A.K. (1983b) Immunoaffinity purification ofhumancomplement component C9 using monoclonal anti-bodies. J. immunol. Meth. 64, 269.
OBERC M.A. & ENGEL W.K. (1977) Ultrastructural localisa-tion of calcium in normal and abnormal skeletal muscle.Lab. Invest. 36, 566.
RAMM L.E., WHITLOW M.B., KOSKI C.L., SHIN M.L. &MAYER M.M. (1983) Elimination of complement chan-nels from the plasma membranes of U937: a nucleatedmammalian cell line. J. Immunol. 131, 1411.
RAUTERBERG E.W., UNGEMACH B. & GEBEST H.J. (1979)Quantitative measurement of C9 sites and their associ-ation to the ring-like 'lesions' on complement-lysedmembranes. J. Immunol. 122, 355.
RICHARDSON P.J. & LuzioJ.P. (1980) Complement-mediatedproduction of plasma-membrane vesicles from rat fat-cells. Biochem. J. 186, 897.
RoITT I.M., DONIACH D., CAMPBELL P.N. & HUDSON R.V.(1956) Autoantibodies in Hashimoto's disease (lympha-denoid goitre). Lancet, ii, 820.
ROMMEL F.A. & MAYER M.M. (1973) Studies of guinea-pigcomplement component C9: reaction kinetics and evi-dence that lysis of EAC1-8 results from a single membranelesion caused by one molecule of C9. J. Immunol. 110,637.
SAHASHI K., ENGEL A.G., LAMBERT F.H. & HOWARD F.M.(1980) Untrastructural localisation of the terminal andlytic ninth complement component (C9) at the motorend-plate in Myasthenia Gravis. J. Neuropathol. exp.Neurol. 39, 160.
SCHLAGER S.I., OHANIAN S.H. & BORSOS T. (1978) Stimula-tion of the synthesis and release of lipids in tumour cellsunder attack by antibody and C. J. Immunol. 120, 895.
SCHLIWA M. (1976) The role of divalent cations in theregulation of microtubule assembly. J. Cell Biol. 70, 527.

188 B. P. Morgan et al.
SCHMALBURCH H. (1975) Segmental fibre breakdown anddefects of the plasmalemma in diseased human muscles.Acta Neuropathol. 33, 129.
WROGEMANN K., BLANCHAER M.C. & JACOBSON S.E. (1979)
Calcium-associated magnesium-responsive defect of oxi-dative phosphorylation by skeletal muscle mitochondriaof B 10 14.6 dystrophic hamsters. Life Sci. 9, 1167.