Embed Size (px)
Citation preview

J Clin Pathol 1982:34;14-25
Immunoperoxidase study of the secretoryimmunoglobulin system in colonic neoplasiaPETER ISAACSON
From the Department ofPathology, Southampton Uniiversity Medical School, Southampton S09 4XY
SUMMARY The relation of the secretory immunoglobulin system in the colon to colorectal cancer
and dysplasia has been examined by staining routine formalin-fixed, paraffin-embedded sections fromcases of carcinoma, adenoma and ulcerative colitis for secretory component (SC), IgA and J chain.In carcinomas there was a close relation between SC synthesis and differentiation and a similarrelation was apparent between SC synthesis and degrees of dysplasia in adenomas. In both morpho-logical and functional (SC synthesis) terms degrees of dysplasia in adenomas resembled degrees ofdifferentiation in carcinomas suggesting that the essential "switch" in the progression towardsneoplasia may occur at the level of the adenoma and that invasive malignancy can arise fromdysplastic mucosa of varying severity. Actively regenerating mucosa in ulcerative colitis (UC)showed intense staining for SC as opposed to foci of precancerous dysplasia where, with one
exception, staining was markedly reduced or absent, suggesting staining for SC could be useful inidentifying foci of precancerous dysplasia in UC. In the absence of severe chronic inflammation, as inUC, the number of IgA-containing plasma cells was closely related to SC staining of neoplasticmucosa suggesting that SC may be important in the mechanism by which IgA lymphocytes hometo the lamina propria of the colon.
Immunohistochemistry, by permitting histologicalobservations relating structure and function, hasconsiderably widened the scope of diagnostic andinvestigative histopathology and the developmentof the immunoperoxidase technique has meant thatthe pathologist can now study material in thesetting with which he is most familiar and usestored material for retrospective studies. Notsurprisingly, when immunoperoxidase techniquesfirst became widely available, histopathologistsimmediately began to search for reliable immuno-histochemical markers that were indicative ofmalignant transformation. One such serologicalmarker, carcinoembryonic antigen (CEA), wasalready at hand and first reports of its value as animmunohistochemical marker of malignant changein colonic mucosa were encouraging.1 Subsequently,however, considerable doubt was cast over the valueof CEA as a tissue or serological marker of malig-nancy2 and the fate of many other immunohisto-chemical markers of malignancy has been similar.3A more logical approach to immunohistochemicalAccepted for publication 27 May 1981
changes in malignancy might be to attempt todemonstrate alterations in complex functions thatare carried out by normal cells and tissues. In theintestine the secretory immunoglobulin systemwould seem to be an ideal set of functions to studyin this way since it is well characterised4 and specificantisera to the three principal components of thissystem are available.
Immunoglobulin A (IgA) is secreted by intestinallamina propria plasma cells as a dimer, the twomolecules being linked by J (joining) chain. Thedimeric IgA becomes attached to secretory com-ponent (SC) which is synthesised by mucosalepithelial cells and the IgA-J-SC complex is thentransported to the lumenal surface of the gut mucosathrough the mucosal cells. This paper reports theresults of the immunohistochemical demonstrationof the three components of the secretory immuno-globulin system (SC, IgA and J chain) in normalrectal mucosa, in adenomas and in carcinomas andthe application of these results to the characterisationand diagnosis of premalignant change as it occurs inulcerative colitis.
14
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

Immunoperoxidase study of the secretory immunoglobulin system in colonic neoplasia
-4+
*-. '.L
7,-
7
.I .,47.+A~t
ai
0
4'.
1*
I)
.4+
.-$.298ici,; <' ;t
*. .. Jg a 4C2;N @ ,
' ---;; WN ru S '-' --' @-:.: M- s ,^
> 4-----; !, .,v5&
:. :: -g :. i.--
... 4 ... *
* S -.: o- e 5 ::- s : ,> vc' :- * + ' .- e -:--,¢D,v,
'., 4: '....
: g i- .E
,,- h .' e:-
,l1,- ----
Cb
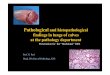
Fig. 1 Normal colonic mucosa stained for (a) SC, (b) IgA and (c) J chain. Immunoperoxidase x 100.
Material and methods
All the sections studied were from formalin-fixedparaffin-embedded tissue removed either at lapar-otomy or endoscopically. Sections of normalcolorectal mucosa were used to establish appropriatetitres of antisera and as a base line for comparisonwith diseased mucosa. These sections were takenfrom colectomy specimens well away from the siteof tumour or other localised disease-for example,diverticular disease. Adjacent normal mucosa wasalso included in most of the other sections studied.These included 25 cases (30 sections) of adenocar-cinoma and 25 cases (52 sections) of adenoma(12 tubular adenomas, 9 tubovillous adenomas,4 villous adenomas). In addition, 16 cases of ulcera-tive colitis were studied in eight of which precancer-ous dysplasia had been diagnosed. From these 16cases 20 sections of inflamed and regenerativemucosa were selected for study and compared to14 sections showing precancerous dysplasia.
Sections were stained by the PAP techniquefollowing trypsin digestion for IgA, J chain and SC.The details of the method used, sources of antiseraand specificity controls have been previouslydescribed.5-7 In all cases adjacent sections were
stained routinely with haematoxylin and eosinpermitting detailed comparison between con-ventional histology and immunohistochemistry.
NORMAL COLORECTAL MUCOSA (Fig. 1)Staining for SC was strongly positive along thelateral membranes of mucosal ce!ls and along theapical border of the crypts. No staining of mucingoblets was evident but cytoplasmic staining ofnon-mucin-containing columnar cells was present.The distribution of IgA and J chain matched that ofSC exactly with the exception that numerous plasmacells in the lamina propria showed strong cytoplasmicstaining for IgA and rather weaker staining for Jchain.
Relation ofSC staining to severity of dysplasia(differentiation)SC staining Mild dysplasia Mod dysplasia Severe dysplasia
(well differ'd) (mod differ'd) (poorly differ'd)
Carcinoma 25 casesnormal 6 1 -
reduced 2 16 1weak/absent - - 20
Adenomas 25 casesnormal 19 1 1reduced - 12 1weak/absent - 7
UC dysplasia 8 casesnormal Ireduced - - -
weak/absent - - 7
Results
15
.1 .:. J.: kik I, #A
I
.N
r*1-
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

.....:.;c v.1 A 4........>...
c.M g~~~~~~~~~~~', ... ..,,. i;
4w S .,........... .0*.X4,2:.X .+ +' <. ' :'A :.:: > Z.......... >St.
~~~~~~~~~~~4* e'.; ..;-A.:........., .,:.'j ,., ..;
os..... t ;|g'..4:Y
* .:~~~~~~'4 ;..S2.*@.......# .,:
2x * b ti X |6 S 5
.' .Zflb.
\4'at '.2
'a v
"4
I, p ii .
ii:.T...
C
* . .. a . ...... s. .:.:. 4
srirC) 4 5: e *
'S '4lr< @; ; o
b' # %.'A.r;
'4- 4,
'a
.4
it-4 -4.
5*-
.'1
$1
Fig. 2 Representative invasive ar-eas fiom the same sectiont of a colorectal carcinoma showing (a) uwelldifferentiated tumour with (b) strong staining for SC, (c) moderately differentiated tumolur with (d) reduced SCstaining, and (e) poorly differentiated tumour with (f) absent SC staining. a, c, e: haematoxYlin and eosini x 200;b, d, f immunoperoxidaise x 200.
COLORECTAL CARCINOMAS
The results of staining for SC are summarised in theTable. With the exception of some poorly differen-tiated tumours which showed uniform absence ofSC staining there was marked variation in initensity
of SC staining throughout the sections. It was there-fore impossible to grade the intensity of SC stainingin the section as a whole. With closer scrutiny itbecame clear that variation in SC staining was
regional and closely followed morphological changes
16 Isaacson
I 't44
P
:.I
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

Immunoperoxidase study of the secretory immunoglobulin system in colonic neoplasia
in both the cytology and architectural arrangement ofthe tumour cells (Fig. 2). Intensity of staining com-parable to normal mucosa was found only in areasof tumour that were well differentiated whilst veryweak or absent staining always correlated with poordifferentiation. Between these two extremes stainingwas always reduced in intensity and, although thedegree of reduction varied considerably, it againappeared to correlate closely with differentiation.It was not possible, however, to characterise thesemoderately differentiated foci into reproduciblesubgroups. Accordingly, representative areas of eachof the three degrees of differentiation were sought ineach tumour studied and the related intensity of SCstaining noted. The reverse procedure of correlatingintensity of SC staining with morphological differ-entiation was also carried out so that for each casestudied an assessment was reached correlatingintensity of SC staining with each degree of differ-entiation present. Thus, amongst the 25 cases ofcarcinoma studied, eight showed well differentiatedareas; in six of these SC staining was normal and intwo it was reduced in intensity. Poorly differentiatedareas were present in 21 cases and in 20 of thesestaining was very weak or absent, while in onereduced staining was noted. Areas of moderatedifferentiation were noted in 17 cases and SCstaining was reduced in intensity in 16 and normal inone. It was notable that cytological differentiationwas the critical factor in determining SC stainingrather than the overall architecture of the tumour-that is, gland formation, budding etc, although thetwo were usually related. With decreasing degrees ofdifferentiation there was increase in nuclear:cytoplasmic ratio, nuclear hyperchromatism andprominence of nucleoli. Stains of the malignant
X~~~9 x j
4 S> * 's i
epithelial cells for IgA and J chain paralleled SCstaining and there was striking correlation betweenmucosal SC and stromal IgA plasma cells. Thus,foci of decreased or absent SC staining were alwaysaccompanied by markedly decreased numbers ofIgA-containing plasma cells (Fig. 3).
ADENOMASHere again intensity of SC staining was often notuniform and was dependent on the degree ofdysplasia within the adenoma be it tubular, tubulo-villous or villous. Adenomas were therefore assessedfollowing the same procedure as that used forcarcinomas with correlation of intensity of SCstaining with the degree of dysplasia (Table).Dysplasia in the adenomas was classified as mild,moderate, or severe according to the criteria ofMorson.8 Foci of mild dysplasia in adenomas(Fig. 4) stained strongly for SC while severelydysplastic foci showed very weak or negativestaining. Foci of moderate dysplasia showed reducedintensity of staining. Thus the pattern of staining wassimilar to that in carcinomas and when the cytologywas carefully evaluated the different degrees ofcytological differentiation paralleled those seen incarcinomas (Figs. 5, 6, 7). The mildly dysplastic cellsin adenomas were morphologically similar to thoseof well differentiated areas in carcinomas and stainedsimilarly for SC. Progressive increase in nuclearenlargement, loss of nuclear polarity and strati-fication of nuclei in both adenomas and carcinomaswas associated with decrease and, finally, loss of SCstaining. Staining for IgA and J chain producedresults similar to those found in carcinomas withmarked reduction of IgA-containing plasma cellsin areas where SC was decreased or absent (Fig. 8).
Fig. 3 Section ofpoorlydifferentiated carcinoma (right)adjacent to normal colorectalmucosa stainedfor IgA.Abundant positively stainingplasma cells are present betweennormal glands but virtuallyabsent within the tumour.Immunoperoxidase x 100.
17
i
11 .:.
1. eI I
.0 I -*f
1.
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

Isaacson
Q,/- N7
440
.00:~ ~I
/I o
Wh~~~~~~~~~~
'4+~~~~~~~~~~~~~~~~4
o4~ ~ ~
4?i
NNicY
1,55
....
1. N.
A4
p.~~~~~~~~~~~~~~4
I
Fig. 4 Representative areas from a single section of a colorectal adenoma showing (a) mild dysplasia with
(b) strong SC staining, (c) moderate dysplasia with (d) reduced SC staining and (e) severe dysplasia with
(f) absent SC staining, a, c, e: haematoxylln and eosin x 200; b, d, f: immunoperoxidase x 200.
ULCERATIVE COLITIS
Sections were selected to include quiescent and
highly active phases of the disease. Staining for SC
was strongly positive even in the presence of active
mucosal regeneration (Fig. 9). In 13 of 14 sections
from eight cases showing precancerous dysplasia
(Table) there was marked depletion and often total
absence of SC (Fig. 10). Amidst areas of intense
regeneration isolated dysplastic glands were high-
lighted by staining for SC (Fig. 1 1). One case showed
18
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

Immunoperoxidase study of the secretory immunoglobulin system in colonic neoplasia
A4,S h
[email protected]. t %~~~,WvtW < *%S^
Ds*+Sv... '
.A.l -- - -
1 11,
C
Fig. 5 Comparative histology of (a) mildly dysplastic adenoma and (b) well differentiated carcinomashowing marked similarity. SC staining intensity of (c) adenoma and (b) carcinoma, are also similar.a, b: haematoxylin and eosin x 400; c, d: immunoperoxidase x 400.
normal SC staining and in this case the dysplasticarea was macroscopically unusually well defined andhistologically bore a close resemblance to anadenoma with mild dysplasia (Fig. 12). Carefulcytological evaluation of the other cases showedappearances similar to those in severely dysplasticfoci of adenomas and poorly differentiated carci-nomas. Some of the sections of dysplasia werecharacterised by villous processes covered by mucin-containing cells (Fig. 13). The cells at the bases ofthese villi showed marked cytological dysplasia andstained negatively for SC. This negative stainingcontinued into the mucin-containing cells which,cytologically, showed little or no dysplasia. Stainingfor IgA and J chain revealed positively stainingplasma cells in the inflamed lamina propria ofregenerative and dysplastic areas in equal concen-tration.
Discussion
The results of this study showing progressive loss ofSC synthesis with increasing degrees of dysplasiaor dedifferentiation are in agreement with the twoprevious studies of Poger et a19 and Weisz-Carrington et al"' both reported from the samelaboratory. Using immunofluorescence on frozensections these workers noted diminished or absentSC synthesis in poorly differentiated colorectalcarcinomas and areas of severe dysplasia inadenomas. They did not, however, note the greatvariability of SC staining and differentiation withinthe same section of colorectal carcinoma, and eachtumour was simply classified as well, moderately, orpoorly differentiated. It is clear, from the results ofthe present study that few colorectal carcinomas arehomogeneous in their differentiation. A tumour may
19
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

Isaacson
Fig. 6 (a) Moderate dysplasia in an adenoma compared to (b) moderate differentiation in a carcinomashowing similar appearances. SC staining of (c) adenoma and (d) carcinoma, both show similar reduction inintensity. a, b: haematoxylin and eosin x 400; c, d: immunoperoxidase x 400.
superficially appear homogeneous in a routinelystained haematoxylin and eosin section but stainingfor SC often reveals marked differences in stainingintensity between groups of cells which on closerinspection are related to cytological differences.Studies relating differentiation of colorectal cancersto prognosis have not taken this lack of homogeneityinto account and their conclusions must be open todoubt.The results of staining adenomas for SC are of
great interest. The gradual loss of SC parallelingcytological (and usually architectural) dedifferentia-tion reinforces the validity of Morson's concept thatdysplasia is a spectrum of changes characterised bygraded degrees within adenomas.8 At first sight,however, it is difficult to reconcile absent SC stainingin severely dysplastic foci of adenomas with positivestaining in many carcinomas since the accepted viewis that adenomas pass through increasingly severegrades of dysplasia before transforming into carci-
nomas. This paradox is also apparent in the resultsof the studies of Poger et al and Weisz-Carringtonet al neither of whom commented on it, however. Itcan be explained by close examination of cytologicaldetail which shows that positively staining areas incarcinomas are cytologically markedly similar tothose in adenomas as are areas showing reduced andweak to absent staining. Thus, it would seem that,at the cytological level, differentiation in adenomasand carcinomas is similar and that the terms dysplasiaand differentiation are really synonymous. Morson'sconcept of dysplasia as a continous spectrum ofchanges in adenomas can, therefore, be extended toinclude invasive lesions. Does this mean that severedysplasia in adenomas is of no account? A glanceat the Table will show few well differentiated-thatis, mildly dysplastic, foci within carcinomas andlikewise few severely dysplastic-that is, poorlydifferentiated areas in adenomas. It should bestressed too, that well differentiated foci in carcino-
20
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

Immunoperoxidase study of the secretory immunoglobulin system in colonic neoplasia
4.fl; ,I y
~~~~~~~~
d 33. 43~d % a
Fig. 7 (a) Severe dysplasia in an adenoma showing similar appearances to (b) poorly differentiatedcarcinoma. There is absence ofSC staining in both (c) the adenoma and (d) the carcinoma.a, b: haematoxylin and eosin x 400; c, d: immunoperoxidase x 400.
fi A.
t a 42; <; s ;t '§!>'91 d; <> 5 w 0 Fmeca8 A Fecig. sainefdeoma
-~sec etor IgA ThrAatndplas mna cells in the
99i'.\i'0i;.'%wi. . $t ............i* ..\@4A'; . ...... 5.. 6 g;-.....mildly4--~~~~~~~~
3-0t - ~~~~~~~~~~~~~~~~~Fg. 8 A seto of an adeom
t ~~~~~~~~~~~~~~~~~(ae}Casreas Fi. 4) stainedfor
21
..
b0j4 i
.i
04
F 0 §F
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

' U
-4 r 4 8 '( ,§ e@'^*'F§
W a'~'*' It C;"''. 4'^¾" .a 4 ' . . .: e e * ...................... p$! 8 9>ts,
Fig. 9 (a) Actively regenerating inflamed mucosa fromt al case of ulcerative colitis .showing (b) strong staining forSC. a: haematoxylin atnd eosin x 100;, b: immunoperoxida.se x 100(.
.:p-. .....
F
* 8'. ?
o
.3 e.
i 8Sg. ; . ,. ,4ies4. .:
<, ,<e* ¢- > b *Fig. 10 (a) A case ofulcerative colitis showingprecancerous dysplasia onthe right. (b) Same fieldstainedfor SC showingabsent staining indysplastic mucosa. a:haematoxylin and eosinx 40; b:immunoper-oxidase x 40.
1'
'A
4'Ia
t:c: ...
I?....11
& t t'4;,ze
..
-1
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

Immunoperoxidase study of the secretory immunoglobulin system in colonic neoplasia
Fig. 11 (a) Active ulcerative colitis with a focus of dysplasia (arrow). (b) Same field
stained for SC which highlights the SC negative dysplastic focus in contrast to surroundintgpositively stainintg inflamed mucosa. a: haematoxylin and eosint x 40; b: immunoperoxidase
x 40.
*.3.e
Fig. 12 (a) A focus of dysplasia from a case ofulcerative colitis resembling a mildly dysplastic adenoma.(b) SC staining showing normal intensity.a: haematoxylin and eosin x 100; b: immunoperoxidasex 100.
mas were usually small in relation to the wholesection; likewise the severely dysplastic foci inadenomas. There is thus a greater tendency forseverely dysplastic foci to become invasive butsevere dysplasia is not a necessary precursor ofinvasion. Most pathologists will be familiar withexamples of well or moderately differentiated in-vasive carcinoma arising in large adenomas whichmay not show severe dysplasia. Thus, in terms of SCsynthesis and morphology there is no differencebetween cells comprising colorectal adenomas andcarcinomas and this suggests that the importantswitch in the progression towards invasive malig-nancy occurs at the level of the adenoma. Whetherinvasiveness requires a second fundamental changein the cell or is simply a matter of time is uncertain.When applied to examples of precancerous
dysplasia in ulcerative colitis the results of SCstaining are often dramatic but not unexpected. Thedysplasia in these cases is usually severe and cor-respondingly the invasive carcinomas that arise inUC are usually poorly differentiated. In five of theeight cases of precancerous dysplasia included in thisstudy there was an associated poorly differentiatedcarcinoma. All of these, which were not included inthe 25 cases of carcinoma described above werepoorly differentiated and stained negatively for SC.Again, to appreciate the severity of the dysplasia, itis the assessment of the cytology of individual cellsthat is important. The lack of SC staining in themucinous columnar cells covering villous processeswhich characterise some cases of precancerousdysplasia suggests that these cells are severelydysplastic although their morphological character-istics do not indicate this. The cells at the bases
23
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

Isaacson
4
4,
Fig. 13 (a) Precancerous dysplasia from a case of UC showing maturation of mucus-containing cells alongvillous structures. (b) High power view ofa base of a dysplastic crypt showing severe dysplasia. (c) Same fieldstained for SC showing absence of staining in the bases of the crypts and in mucus cells along the villousstructures. a, b: haematoxylin and eosin x 100 and x 400; c: immunoperoxidase x 100.
of these villi appear to differentiate morphologicallybut not functionally as they progress up the villousstalks. Poger et al thought that they could relateSC synthesis to the presence of mucin but as em-phasised by the findings in precancerous dysplasiathis study does not confirm this.The question naturally arises as to the diagnostic
value of staining for SC to detect precancerousdysplasia. In active ulcerative colitis differentiationbetween regeneration and precancerous dysplasiacan be extremely difficult. Some success in differen-tiating these two conditions can be achieved bystaining immunohistochemically for CEA." Thisrests,however, on careful adjustments of the titre ofthe antiserum to achieve a quantitative rather thanqualitative distinction between CEA synthesis in thetwo conditions and this, coupled with the variationin specificity of different antiCEA sera, meant thatthe technique was not suitable for routine use.Provided that antiSC serum is titred out to givecrisp specific staining on normal colon there is littleeffect on differential staining between normal anddysplastic mucosa by a shift in titre of one or twodilutions in either direction and antisera from twodifferent sources and species have given identicalresults. Foci of mild dysplasia which bear a strongresemblance to mildly dysplastic adenomas asoccurred in one case in this study will not be
distinguished by SC staining. Although dysplasia,when it occurs in ulcerative colitis, tends to be severedistinction from inflamed regenerative mucosa canstill be difficult, and here SC staining could be helpfulas shown in Fig. 11. Further prospective studies onbiopsy specimens are needed to fully evaluate theusefulness of SC staining as a diagnostic tool.The relation of lamina propria IgA plasma
cells to the SC status of the mucosa is intriguing. Asreported by Weisz-Carrington et al, in the absenceof overt inflammation there is an extremely closerelationship between absence of SC and absence ofIgA-containing plasma cells and this relationshipholds true within a single microscopic field. Thissuggests a role for SC in the homing mechanismof IgA lymphocytes to the lamina propriaof the gut;a hypothesis originally put forward by Guy-Grandet al12 but later refuted by Brandtzaeg et al.13Alternatively, IgA may be necessary to induce SCproduction by mucosal cells. The presence ofabundant IgA-containing plasma cells in the SCnegative inflamed dysplastic mucosa of ulcerativecolitis is against this suggestion however.
References
Isaacson P, Le Vann HP. The demonstration of carcino-embryonic antigen in colorectal carcinoma and colonic
24
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from

Immunoperoxidase study of the secretory immunoglobulin system in colonic neoplasia
poiyps using an immunoperoxidase technique. Cancer1976;38:1348-56.
2 Isaacson P, Judd MA. Immunohistochemistry of carcino-embryonic antigen in the small intestine. Cancer 1978;42:1554-9.
3Neville AM, Laurence DJR. Tumour markers and thegastrointestinal tract. In: Wright R, ed. Recent advancesin gastrointestinal pathology. London: WB Saunders,1980 :255-66.
4Brown WR. Relationships between immunoglobulins andthe intestinal epithelium. Gastroenterology 1978;75:129-38.
5 Mepham BL, Frater W, Mitchell BS. The use of proteo-lytic enzymes to improve immunoglobulin stainingby the PAP technique. Histochem J 1979;11:345-57.
6 Isaacson P. Immunochemical demonstration of J chain:a marker of B-cell malignancy. J Clin Pathol 1979;32:802-7.
7Isaacson P. Crypt cell carcinoma of the appendix-so-called adenocarcinoid tumour. Am J Surg Pathol 1981;5:213-24.
8 Morson BC, Konishi F. Dysplasia in the colorectum.In: Wright R, ed. Recent advances in gastrointestinal
pathology. London: WB Saunders, 1980:331-43.9 Poger ME, Hirsch BR, Lamm ME. Synthesis of secretory
component by colonic neoplasms. Am J Pathol 1976;82:327-34.
'0 Weisz-Carrington P, Poger ME, Lamm ME. Secretoryimmunoglobulins in colonic neoplasms. Am J Pathol1976 ;85 :303-14.
Isaacson P. Tissue demonstration of carcinoembryonicantigen (CEA) in ulcerative colitis. Gut 1976;17:561-7.
12 Guy-Grand D, Griscelli C, Vassalli P. Gut-associatedlymphoblasts and intestinal IgA plasma cells. Adv ExpMed Biol 1974;45:41.
3 Brandtzaeg P, Gjeruldsen ST, Korsrud F, Baklien K,Berdal P, Ek J. The human secretory immune systemshows striking heterogeneity with regard to involvementof J chain-positive IgD immunocytes. J Immunol 1979;122:503-10.
Requests for reprints to: Dr P Isaacson, Department ofPathology, Level E, South Laboratory Block, GeneralHospital, Southampton S09 4XY, England.
.5
copyright. on S
eptember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.35.1.14 on 1 January 1982. Dow
nloaded from





![[12 septembre 2005 ] CRI UHP – NANCY2 1 Base de lien BALI Université Henri Poincaré et Université Nancy 2 UNIRE](https://img.pdfslide.net/doc/110x75/551d9d80497959293b8b9aaf/12-septembre-2005-cri-uhp-nancy2-1-base-de-lien-bali-universite-henri-poincare-et-universite-nancy-2-unire.jpg)